")
Back to Journals » Journal of Inflammation Research » Volume 18
Prediction of Clinical Bronchiectasis from Asymptomatic Radiological Bronchiectasis
Authors Fan Y, Li Z, Jiang N, Zhou Y, Song J, Yu F, Zhang J, Wang X
Received 19 November 2024
Accepted for publication 1 April 2025
Published 12 April 2025 Volume 2025:18 Pages 4995—5009
DOI https://doi.org/10.2147/JIR.S505235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yamin Fan,1,* Zhuanyun Li,2,* Nanchuan Jiang,3,* Yaya Zhou,1,* Jianping Song,1 Fan Yu,1 Jianchu Zhang,1,* Xiaorong Wang1,*
1Department of Respiratory and Critical Care Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 2Department of Emergency Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 3Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianchu Zhang, Department of Respiratory and Critical Care Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, 430022, People’s Republic of China, Email [email protected] Xiaorong Wang, Department of Respiratory and Critical Care Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, 430022, People’s Republic of China, Email [email protected]
Background: Under persistent inflammation, asymptomatic radiological bronchiectasis (ARB) may develop into clinical bronchiectasis (CB). Although CB has been extensively studied, the potential for ARB to evolve into CB remains largely unexplored. Whether the ARB could progress to CB and the risk factors to speed up the process are poorly understood.
Methods: This was an observational cohort study. 370 patients with radiological bronchiectasis were included in Wuhan Union Hospital in 2018. 296 ARB patients were followed up in 2022 to verify if they progressed to CB and divided the development and validation of clinical prediction models into a training set (n=207) and a validation set (n=89) by the ratio of 7:3. LASSO algorithm and multivariable logistic regression analysis were performed to construct a new nomogram model. ROC, a calibration and decision curve were used to assess the predictive performance of our new prediction model.
Results: 370 patients (74, 20% with CB) were finally included. Compared with ARB, CB had lower BMI, Bhalla score, FEV1% predicted, greater extent and degree of bronchodilation, more lobes with mucus plugs, greater thickness of bronchodilation, greater likelihood of pulmonary heart disease and chronic obstructive pulmonary disease (COPD), and lower likelihood of hypertension and coronary artery disease (P< 0.05). In 2022, 60 out of 296 ARB patients progressed to CB. Age, FEV1% predicted, COPD, heart failure (HF), degree of bronchiectasis, number of lobes with bronchiectasis and number of lung segments with mucus plugs were risk factors. The AUCs of the prediction model were 0.866 (95% CI, 0.802– 0.931) in the training set and 0.860 (95% CI, 0.770– 0.949) in the validation set.
Conclusion: ARB may progress to CB under the risk factors, including age, FEV1% predicted, COPD, HF and CT images including degree of bronchiectasis, number of lobes with bronchiectasis and number of lung segments with mucus plugs), based on which the nomogram model is a convenient and efficient tool for follow-up management and preventing CB in patients with ARB.
Keywords: asymptomatic radiological bronchiectasis, clinical bronchiectasis, nomogram, predictive model
Introduction
Bronchiectasis is a clinical syndrome characterized by chronic cough and sputum production in the presence of abnormal thickening and dilatation of the bronchial wall visible on lung imaging.1 However, some patients with bronchiectasis on lung computed tomography (CT) do not have cough, sputum or other clinical symptoms associated with bronchiectasis, which is named asymptomatic radiological bronchiectasis. The relationship between asymptomatic radiological bronchiectasis (ARB) and clinical bronchiectasis (CB) (radiological bronchiectasis associated with chronic syndromes) is unclear. Furthermore, given the incomplete understanding of the natural history of the bronchiectasis process, the long-term prognostic significance of asymptomatic radiological bronchiectasis is unknown. Asymptomatic radiological emphysema may develop into typical chronic obstructive pulmonary disease (COPD) symptoms under the influence of risk factors such as smoking or low FVC1,2 which is considered early stages of COPD. However, whether the asymptomatic radiological bronchiectasis could progress to clinical bronchiectasis and the risk factors to speed up the process are poorly understood. Just as COPD and emphysema are the results of inflammation destruction,3 both radiological bronchiectasis and clinical bronchiectasis result from airway tissue destruction caused by pulmonary infection, immunodeficiency, autoimmune disease and mucus obstruction, which are associated with inflammation of the airway.4–6 We hypothesize that asymptomatic radiological bronchiectasis may develop into clinical bronchiectasis in case of persistent inflammation. Here, we conducted a cohort study to investigate the long-term outcomes of asymptomatic radiological bronchiectasis after 4 years of follow-up, to explore the risk factors and construct a nomogram model to predict the occurrence of symptoms in radiological bronchiectasis patients. It could identify high-risk individuals who will develop clinical bronchiectasis and provide a reference for formulating treatment plans for patients with radiological bronchiectasis.
Materials and Methods
Subjects and Data Collection
This was an observational cohort study in which hospitalized patients with radiological bronchiectasis were included in Wuhan Union Hospital in 2018. We assigned patients to one of two groups: an asymptomatic radiological bronchiectasis group and a clinical bronchiectasis group. Patients in the asymptomatic radiological bronchiectasis group were followed up by telephone in 2022 and some of them had their lung CTs reviewed. The project followed the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Union Hospital of Tongji Medical College, Huazhong University of Science and Technology, without the need for written informed consent, as informed consent was waived by our Institutional Review Board due to the retrospective nature of our study (2022–0389).
Data collected included age, sex, BMI, smoking history, cause of bronchiectasis, comorbidities, imaging manifestations and severity of bronchiectasis, and lung function (FEV1% predicted). In this study, the (25-Bhalla score) was used instead of the total score of lung CT manifestations. For ease of writing, all references to the (25-Bhalla score) below are replaced by the Bhalla score. CT images were independently assessed by two independent observers and differences were resolved by consensus. The comorbidities of bronchiectasis were investigated according to the Spanish guidelines program.7 The primary observation of the telephone interviews was the presence or absence of clinical bronchiectasis.
The study flow chart of this study was shown in Figure 1.
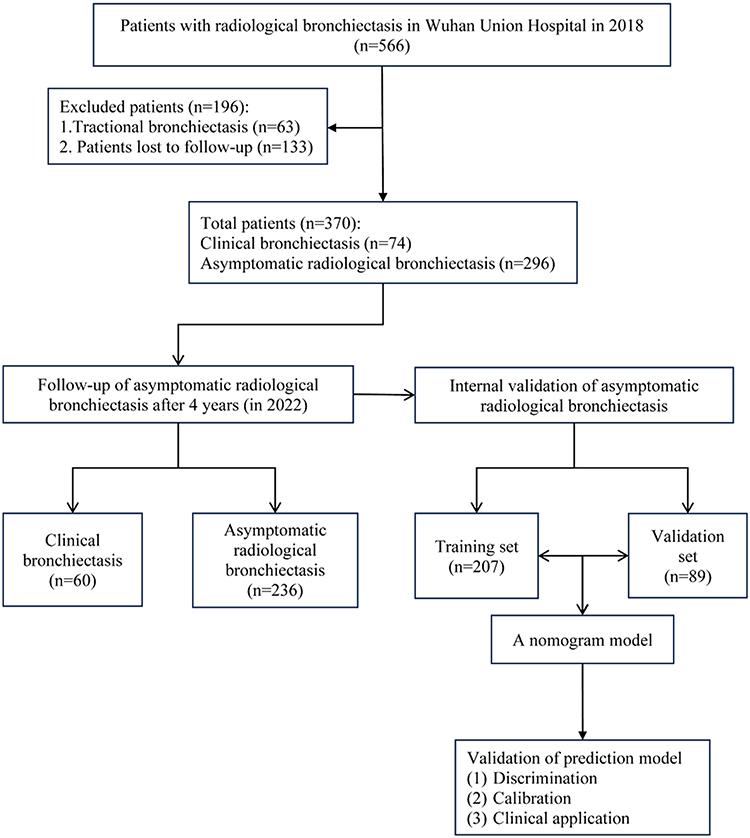 |
Figure 1 The flowchart of the development and validation of the prediction model. |
Identification of Radiological Bronchiectasis and Clinical Bronchiectasis
According to the international consensus recommendations for the radiological and clinical diagnosis of bronchiectasis, 1 the British Thoracic Society (BTS) guidelines for non-cystic fibrosis(NCF) bronchiectasis 8 and the International Expert Consensus on Clinical Symptoms of Bronchiectasis in Adults for Use in Clinical Trials, 1 the following three criteria are used to define the radiological bronchiectasis: an inner or outer airway–artery diameter ratio (the ratio of airway diameter to their adjacent artery diameter) of 1. 0 or more, a lack of tapering of the airways, and visibility of airways in the periphery. Radiological bronchiectasis is diagnosed when one of these criteria is met. The criteria for clinical bronchiectasis include at least two of the following must be met: (1) a cough most days of the week; (2) sputum production most days of the week; (3) a history of exacerbations.
Telephone Follow-up
The questionnaires designed for use in CB are the Quality of Life-Bronchiectasis questionnaire, Bronchiectasis Health Questionnaire, St. George’s Respiratory Questionnaire and the Leicester Cough Questionnaire. With reference to diagnostic criteria and appeal-relevant questionnaires of CB, we developed the follow-up visit content. Follow-up visits included symptoms and severity of cough, sputum, hemoptysis, dyspnea, sputum purulence, exacerbations and quality of life. Each patient and all family members who were aware of the patient’s condition were followed up twice at different times by two independent researchers in strict accordance with the follow up protocol. The investigators recorded the results of the follow-up and separately determined whether the follow-up ARB population met the diagnosis of CB. Disagreements, if any, were resolved by consensus.
Development and Validation of the Nomogram
The clinical data of ARB was compiled in R language, and by randomly splitting the patient data into the training set (n = 207) and the validation set (n = 89) by the ratio of 7:3. The training set was used to select predictors and construct the prediction model, while the validation set was used to verify the performance of the prediction model. In our study, the LASSO binary logistic regression model was used to select risk factors, and factors with non-zero coefficients were selected. Multivariate logistic regression analysis assessed the association between risk factors and CB and created a model based on the selected variables, depicted in the form of a nomogram. For a specific real case, each point of a variable was assigned to a score (Points axis). Sumed the achieved points of 7 variables to obtain a total score. The total score on the Total Points axis corresponds to a predicted risk value on the Risk axis. In our study, the accuracy of the nomogram model was assessed by internal validation. Area under the ROC curve (AUC) was used to assess the discrimination of the model, and the calibration plot was used to assess how close the actual results of the nomogram were to the predicted results. Decision curve analysis (DCA) shows the standardized net benefit relative to the risk threshold probability9 and was used to assess the clinical utility of the model. The clinical impact curves showed the number of high-risk and true-positive patients at different threshold probabilities. Kaplan-Meier curves and Log rank tests were used for the survival analysis.
Statistical Analysis
The baseline information of the study population was analyzed using descriptive statistics. The Kolmogorov–Smirnov test was used to test the normality of the distribution of continuous variables. Normally distributed continuous variables were expressed as mean and standard deviation and vice versa as median and interquartile range. For categorical variables, frequencies and percentages are the best way to present them.
Given the high number of lost patients, in order to test the robustness of the results, we preformed 2 sensitivity analyses to generate data of primary end point for patients lost to follow-up: (1) all patients lost to follow-up were considered to have developed CB in 2022; (2) all patients lost to follow-up were considered to have not developed CB in 2022. In sensitivity analysis, we compared the baseline characteristics between the CB group and the ARB group.
Statistical analysis was performed using SPSS (IBM SPSS Statistics 26.0, SPSS Inc., Chicago, IL, United States) and R language (version 4.1.3). All statistical tests were two-sided, and statistical significance was set at 0.05.
Results
Characteristics of the Cohort
A total of 566 hospitalized patients with radiological bronchiectasis in Wuhan Union Hospital in 2018. A total of 370 patients (190 (51.35%) males and 180 (48.65%) females) were finally included after excluding 63 patients with tractional bronchiectasis and 133 lost patients (49 of whom died of other diseases). 74 (20.0%) had clinical bronchiectasis and 296 (80.0%) had asymptomatic radiological bronchiectasis. The causes for hospitalization of these patients were shown in Supplementary Table 1. In our study, hospitalized patients underwent chest CT scanning because of different clinical symptoms (fever, cough, sputum, hemoptysis, dyspnea, chest pain, etc), lung disease (eg, lung cancer and tuberculosis, etc.) and/or a certain disease that required clarification of the presence of pulmonary complications (eg, interstitial pneumonitis in patients with rheumatic system diseases, etc).
In 2022, the asymptomatic radiological bronchiectasis group was subdivided into a follow-up clinical bronchiectasis group (60, 20.27%) and a consistently asymptomatic radiological bronchiectasis group (236, 79.73%).
In 2018, compared with the ARB, CB had lower BMI, Bhalla score and FEV1% predicted, more quantities in the number of lung segments with bronchiectasis and mucus plug involvement, greater degree of bronchodilation and mucus plugs, greater thickness of bronchodilation, greater likelihood of pulmonary heart disease and chronic obstructive pulmonary disease (COPD), and lower likelihood of hypertension and coronary artery disease (P< 0. 05). In 2022, compared with the consistently ARB, the follow-up CB had older age, lower Bhalla score and FEV1% predicted, more quantities in the number of lung segments with bronchiectasis and mucus plug involvement, greater degree of bronchodilation and mucus plugs, greater likelihood of COPD (P< 0. 05) (Table 1 and Supplementary Table 2).
 |
Table 1 Comparison of Baseline Characteristics Between Clinical Bronchiectasis Group and Asymptomatic Radiological Bronchiectasis Group |
The results of the 2 sensitivity analyses we conducted were generally consistent with the results of the main analysis (Supplementary Tables 3 and 4), indicating the robustness of the results of the main analysis.
The Construction of Predictive Model Based on Risk Factors
The 296 patients with asymptomatic radiological bronchiectasis at baseline were divided into a training set (207, approximately 70%) and a validation set (89, approximately 30%) for internal validation. There were no significant differences in any of the variables we included between the training set and the validation set, suggesting that the training set could be used for internal validation (Supplementary Table 5). The training set (including 42 cases that progressed to clinical bronchiectasis) was then analyzed. The follow-up clinical bronchiectasis group in the training set appeared to be older and to had lower Bhalla scores, worse FEV1% predicted, a higher degree of bronchiectasis, a greater extent of bronchiectasis, a greater extent of mucus plugs, and a greater likelihood of COPD and heart failure (HF) comorbidities (P<0.05) (Table 2).
 |
Table 2 Comparison of the Characteristics Between Consistently Asymptomatic Radiological Bronchiectasis Group and Follow-up Clinical Bronchiectasis Group in the Training Set |
We screened 39 variables in the training cohort using the LASSO binary logistic regression model, which selected 7 variables with non-zero coefficients (Supplementary Figure 1A, B and Supplementary Table 6). After multivariate logistic regression analysis, age, COPD, HF, number of lobes with bronchiectasis, number of lung segments with mucus plugs, degree of bronchiectasis, and FEV1% predicted were independent risk factors for clinical bronchiectasis (Figure 2). We weighted the regression coefficients of the risk factors in multivariate logistic regression and developed a risk score formula to predict the occurrence of clinical bronchiectasis. Risk score = −4.690 + 0.051 (age) + 1.235 (if COPD is positive) + 0.883 (if HF is positive) + 1.147 (degree of bronchiectasis) + 0.380 (number of lobes with bronchiectasis) + 0.191 (number of lung segments with mucus plugs) - 0.057 (FEV1% predicted) (Supplementary Table 7). The nomogram model for predicting the likelihood of asymptomatic radiological bronchiectasis to clinical bronchiectasis was developed based on the above risk factors. A real case is shown in Figure 3.
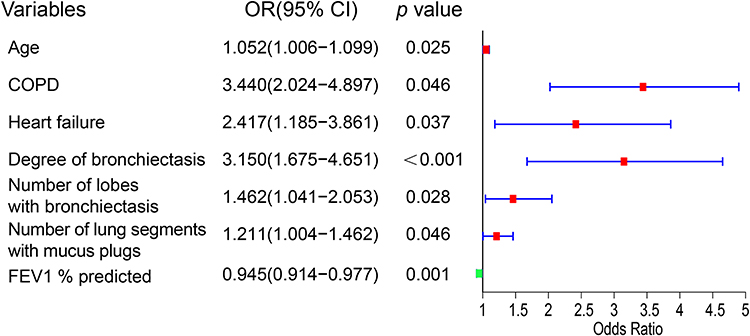 |
Figure 2 Forest plot showing the relationship between the risk factors and the progression from asymptomatic radiological bronchiectasis to clinical bronchiectasis. |
 |
Figure 3 Nomogram for predicting the risk of the progression from asymptomatic radiological bronchiectasis to clinical bronchiectasis. A 67-year-old patient with asymptomatic radiological bronchiectasis, a history of COPD and no history of HF. FEV1% predicted was 66%, the degree of bronchiectasis was 3, the number of lung lobes with bronchiectasis was 2, and the number of lung segments with mucus plugs was 2. This patient had a total score of 345 and an 84.6% risk of clinical bronchiectasis. |
Validation and Evaluation of the Nomogram
The validation of the nomogram in this study was performed by internal validation. The calibration curve of the nomogram was used to show the agreement between the predicted and observed results. The agreement between the two results performed well in the training cohort and the validation cohort (Figure 4A and B). The Hosmer-Lemeshow results showed no significant difference, indicating a good fit in the training cohort. The predictive performance of the nomogram was assessed by the ROC curve, which had an AUC of 0.866 (95% CI, 0.802–0.931) in the training set and an AUC of 0.860 (95% CI, 0.770–0.949) in the validation set. The predictive performance of the nomogram was comparable to combine 1 (combining age, COPD, HF, FEV1% predicted and Bhalla score) (0.861 (95% CI, 0.774–0.948)), but higher than the Bhalla score (0.653 (95% CI, 0.559–0.747)). The predictive value of combine 2 (combining the degree of bronchiectasis, the number of lung lobes with bronchiectasis and the number of lung segments with mucus plugs) (0.815 (95% CI, 0.698–0.932)) was also significantly higher than the Bhalla score, suggesting the importance of the three imaging parameters in predicting the development of clinical bronchiectasis (Figure 4C and D, Table 3 and Supplementary Tables 8 and 9).
 |
Table 3 Comparison of AUC Results From Nomogram Models |
 |
Figure 4 Discrimination and calibration of the nomogram prediction models in the training and validation cohorts. (A) Calibration plot in the training cohort. (B) Calibration plot in the validation cohort. (C) ROC curve in the training cohorts. (D) ROC curve in the validation cohorts. |
Clinical Usefulness
DCA is a method of assessing the benefit of a diagnostic test by quantifying the net benefit at different threshold probabilities to determine the clinical utility of the nomogram. DCA was used in this study to assess the clinical utility of the nomogram. Both the training and validation cohorts showed a higher net clinical benefit compared to the two thresholds of “no intervention” and “intervention for all” (Supplementary Figure 2A).The clinical impact curves showed a convergence between the number of patients considered at high risk of asymptomatic radiological bronchiectasis developing into clinical bronchiectasis and those with asymptomatic radiological bronchiectasis developing into clinical bronchiectasis event within this risk threshold (Supplementary Figure 2B and C). The prediction model had good clinical applicability.
Imaging Follow-up
Due to patients’ inattention to asymptomatic imaging bronchiectasis, poor health status and change of hospital of attendance, in 2022, a total of 53 patients underwent lung CT review (11 patients in the clinical bronchiectasis group, 12 patients in the follow-up clinical bronchiectasis group and 30 patients in the consistently asymptomatic radiological bronchiectasis group). There were no significant changes in CT imaging characteristics in 2022 compared with lung CT in 2018 (Table 4). These indicated that the progression of CT imaging was slow, and that studies of this progression would require longer follow-up. However, due to the small number of patients who had a follow-up lung CT at 4 years, the above conclusions may not be entirely correct and we need to be cautious. The number of lung CTs reviewed in subsequent studies still needs to be expanded in order to draw reliable conclusions.
 |
Table 4 Comparison of CT Imaging Characteristics of the Lungs in 2018 and 2022 |
Discussion
In the current cohort study, we demonstrated that asymptomatic radiological bronchiectasis may progress to clinical bronchiectasis after 4 years of follow-up. To the best of our knowledge, this is the first study to develop and validate a predictive model for new-onset symptoms of bronchiectasis based on simple radiological features and clinical factors. Using this predictive model, people with asymptomatic radiological bronchiectasis at the risk of clinical bronchiectasis can be quickly identified at the first consultation.
Asymptomatic radiological bronchiectasis is commonly encountered in patients with early CF10 and has been documented in the clinic.11 However, asymptomatic radiological bronchiectasis in non-CF individuals is often overlooked. Our study is the first to demonstrate that the asymptomatic radiological bronchiectasis could develop into clinical bronchiectasis under the influence of risk factors including advanced age, low FEV1, comorbid COPD and/or HF, the degree of bronchiectasis, the number of lobes with bronchiectasis as well as the number of lobes with mucus plugs. This was consistent with two multidimensional severity indices of bronchiectasis, the FACED score12 and the Bronchiectasis Severity Index (BSI),13 both of which emphasized the important role of age, FEV1, and radiological extension in bronchiectasis. This implied that asymptomatic radiological bronchiectasis may be as part of the natural earlier history disease process of clinical bronchiectasis and could develop clinical bronchiectasis under the influence of various risk factors, which may be delayed and even modified by earlier intervention. Thus, the predictive model in our study could help to early identify and timely prevent the progression of asymptomatic radiological bronchiectasis to clinical bronchiectasis.
Bronchiectasis has been demonstrated as an age-associated disease.14,15 In addition to the physiological decline in respiratory muscle function, age-related immunosenescence may play an important role. Excessive inflammation, loss of control of persistent infections and the potential microbiome dysbiosis due to immunosenescence16–19 play an important role in the occurrence of clinical bronchiectasis and worsening the clinical syndrome.20 Not surprisingly, FEV1 and coexisting COPD were independent predictors of clinical bronchiectasis. Persistent deregulated chronic inflammation is strongly associated with COPD, leading to poorly reversible airflow limitation, mucus hypersecretion and airway wall thickening.21–23 Luminal obstruction, mucus plugging and thickened airway walls lead to a reduction in FEV1 over time. In addition, respiratory hypoxia due to lower FEV1 could be a potential driver of sterile neutrophilic inflammation to accelerate the progression of clinical bronchiectasis.24 Our study also confirmed that the presence of HF was also associated with the progression of clinical bronchiectasis. Systemic inflammation may be a possible explanation for the mechanistic pathway linking bronchiectasis and HF.25,26 It should be noted that symptoms such as cough and sputum production may be related to HF itself rather than clinical bronchiectasis, and there were a few cases of HF in our study. Whether HF plays an important role in disease progression needs further confirmation in multicenter, large-sample studies. In terms of other comorbidities, our study found that ARB was more likely to be comorbid with hypertension and coronary artery disease compared with CB. However, no such difference was found between follow-up CB and consistent ARB. This may be related to selection bias in our study. After all, our study population consisted of inpatients, most of whom were hospitalized for other conditions.
Computed tomography (CT) is a minimally invasive imaging modality that provides both high-contrast and high-resolution images of the lungs and airways. Due to its close correlation with airway inflammation, clinical manifestations and disease activity, CT has proven to be the most important test in the diagnosis of bronchiectasis and a most essential component in determining the prognosis and risk of chronic respiratory diseases such as COPD27,28 and bronchiectasis.29,30 Greater degree and extent of bronchodilation and mucus plugs on CT indicate destruction and impaired mucociliary clearance and/or mucus hypersecretion due to airway inflammation, leading to susceptibility to infection, airflow obstruction and damage, all of which accelerate the progression of clinical bronchiectasis.31–33 Therefore, it is logical to use the and the number of lung segments with mucus plugs as key determinants in predicting the occurrence of clinical bronchiectasis in patients with bronchiectasis. Furthermore, they are simpler than the Bhalla score and are available to the clinician at the time of the patient’s initial radiological diagnosis of bronchiectasis. Therefore, imaging findings of the above three radiological parameters are important because they allow a rapid assessment of the likelihood that the patient will progress to clinical bronchiectasis.
The overall score of nomogram we built (refer to Figure 3) ranged from 150 to 400, with the associated risk level varying between 0.002 and 0.96. Essentially, an elevated total score indicated an increased risk of CB among ARB patients. The real case illustrated by Figure 3 was selected from among ARB (n=296). This patient has 345 total points (Statistical analysis and Figure 3 for details), which corresponds 84.6% risk of CB. The nomogram could be used for patient-specific risk screening, as the real case mentioned by Figure 3 proving its effectiveness in forecasting the risk of CB in ARB patients.
This study has some limitations that should be mentioned. First, the sample size was insufficient to draw firm conclusions. Second, the data for the nomogram were obtained from a single center and selection bias could not be avoided. The follow-up was performed by telephone call, which may have a recall bias in terms of symptoms. Third, the generalization of our nomogram should be interpreted with caution due to the lack of external validation. So, we would require multicenter prospective studies to further investigate the clinical practice of our nomogram. Fourthly, the study was conducted in inpatients and there was a possibility of selection bias. Perhaps in future studies, selecting a healthy population for the study would give more representative results. In addition, the influence of radiological manifestations of different etiologies and microbial colonization on the occurrence of clinical bronchiectasis were not studied and discussed by us. Finally, we could not estimate the impact of asymptomatic bronchiectasis on clinical outcomes, such as mortality, hospitalization, exacerbations and quality of life, due to the short follow-up.
Conclusion
Asymptomatic radiological bronchiectasis may progress to clinical bronchiectasis, which can be identified by age, FEV1% predicted, COPD, HF, the degree and extent of bronchial dilatation and the extent of mucus plugs. The model constructed from the above risk factors can help clinicians address the controversial issues of when and in which patients therapeutic intervention should be initiated.
Patient Data Confidentiality Statement
The data and personal information of the research subjects were kept confidential and the identifying information of the research subjects in the study was digitally identified with a study number. All study members and the study sponsors were asked to keep the information about the study subjects confidential and not disclose any information about the study subjects.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No.82270021).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aliberti S, Goeminne PC, O’Donnell AE, et al. Criteria and definitions for the radiological and clinical diagnosis of bronchiectasis in adults for use in clinical trials: international consensus recommendations. Lancet Respir Med. 2022;3:298–306. doi:10.1016/S2213-2600(21)00277-0
2. Soriano JB, Polverino F, Cosio BG. What is early COPD and why is it important? Europ Respir J. 2018;6.
3. Hogg JC, Senior RM. Chronic obstructive pulmonary disease - part 2: pathology and biochemistry of emphysema. Thorax. 2002;57(9):830–834. doi:10.1136/thorax.57.9.830
4. Schäfer J, Griese M, Chandrasekaran R, Chotirmall SH, Hartl D. Pathogenesis, imaging and clinical characteristics of CF and non-CF bronchiectasis. BMC Pulm Med. 2018;18(1):79. doi:10.1186/s12890-018-0630-8
5. Keir HR, Chalmers JD. Pathophysiology of bronchiectasis. Semin Respir Crit Care Med. 2021;4:499–512.
6. José RJ, Loebinger MR. Clinical and radiological phenotypes and endotypes. Semin Respir Crit Care Med. 2021;4:549–555.
7. Vendrell M, de Gracia J, Olveira C, et al. [Diagnosis and treatment of bronchiectasis. Spanish Society of Pneumology and Thoracic Surgery]. Archivos de Bronconeumologia. 2008;11:629–640.
8. Pasteur MC, Bilton D, Hill AT. British Thoracic Society guideline for non-CF bronchiectasis. Thorax. 2010;65(Suppl 1):i1–58. doi:10.1136/thx.2010.136119
9. Fitzgerald M, Saville BR, Lewis RJ. Decision curve analysis. JAMA. 2015;4:409–410. doi:10.1001/jama.2015.37
10. Schultz A, Stick S. Early pulmonary inflammation and lung damage in children with cystic fibrosis. Respirology. 2015;4:569–578. doi:10.1111/resp.12521
11. Winter DH, Manzini M, Salge JM, et al. Aging of the lungs in asymptomatic lifelong nonsmokers: findings on HRCT. Lung. 2015;2:283–290. doi:10.1007/s00408-015-9700-3
12. Martínez-García M, de Gracia J, Vendrell Relat M, et al. Multidimensional approach to non-cystic fibrosis bronchiectasis: the FACED score. Europ Respir J. 2014;5:1357–1367. doi:10.1183/09031936.00026313
13. Chalmers JD, Goeminne P, Aliberti S, et al. The bronchiectasis severity index. An international derivation and validation study. Am J Respir Crit Care Med. 2014;5:576–585. doi:10.1164/rccm.201309-1575OC
14. Zhou YM, Wang C, Yao WZ, et al. [The prevalence and risk factors of bronchiectasis in residents aged 40 years old and above in seven cities in China]. Zhonghua Nei Ke Za Zhi. 2013;5:379–382.
15. Derbyshire EJ, Calder PC. Bronchiectasis-could immunonutrition have a role to play in future management? Frontiers in Nutrition. 2021;652410. doi:10.3389/fnut.2021.652410
16. Santoro A, Bientinesi E, Monti D. Immunosenescence and inflammaging in the aging process: age-related diseases or longevity? Ageing Res Rev. 2021;71:101422. doi:10.1016/j.arr.2021.101422
17. Soma T, Nagata M. Immunosenescence, inflammaging, and lung senescence in asthma in the elderly. Biomolecules. 2022;10.
18. Fülöp T, Dupuis G, Witkowski JM, Larbi A. The role of immunosenescence in the development of age-related diseases. Revista de Investigacion Clinica; Organo Del Hospital de Enfermedades de la Nutricion. 2016;2:84–91.
19. Murray MA, Chotirmall SH. The impact of immunosenescence on pulmonary disease. Mediators Inflammation. 2015;2015:692546. doi:10.1155/2015/692546
20. Whitters D, Stockley R. Immunity and bacterial colonisation in bronchiectasis. Thorax. 2012;11:1006–1013. doi:10.1136/thoraxjnl-2011-200206
21. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;1:16–27. doi:10.1016/j.jaci.2016.05.011
22. Rovina N, Koutsoukou A, Koulouris NG. Inflammation and immune response in COPD: where do we stand? Mediators Inflammation. 2013;2013:413735. doi:10.1155/2013/413735
23. Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. New Engl J Med. 2004;350(26):2645–2653. doi:10.1056/NEJMoa032158
24. Montgomery ST, Mall MA, Kicic A, Stick SM. Hypoxia and sterile inflammation in cystic fibrosis airways: mechanisms and potential therapies. Europ Respir J. 2017;49(1):1600903. doi:10.1183/13993003.00903-2016
25. Murphy SP, Kakkar R, McCarthy CP, Januzzi JL. Inflammation in Heart Failure: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(11):1324–1340. doi:10.1016/j.jacc.2020.01.014
26. Dick SA, Epelman S. Chronic heart failure and inflammation: what do we really know? Circ Res. 2016;119(1):159–176. doi:10.1161/CIRCRESAHA.116.308030
27. Bakker JT, Klooster K, Vliegenthart R, Slebos DJ. Measuring pulmonary function in COPD using quantitative chest computed tomography analysis. Eur Respir Revi. 2021;161.
28. Wang Y, Xu J, Meng Y, Adcock IM, Yao X. Role of inflammatory cells in airway remodeling in COPD. Int J Chron Obstruct Pulmon Dis. 2018;Volume 13:3341–3348. doi:10.2147/COPD.S176122
29. Ooi GC, Khong PL, Chan-Yeung M, et al. High-resolution CT quantification of bronchiectasis: clinical and functional correlation. Radiology. 2002;225(3):663–672. doi:10.1148/radiol.2253011575
30. Wu FJ, Qi Q, Hu Q, Xu LS. [Correlation between chest CT features and clinical characteristics of patients with bronchiectasis]. Zhonghua Yi xue Za Zhi. 2019;38:2982–2988.
31. Zhou-Suckow Z, Duerr J, Hagner M, Agrawal R, Mall MA. Airway mucus, inflammation and remodeling: emerging links in the pathogenesis of chronic lung diseases. Cell Tissue Res. 2017;367(3):537–550. doi:10.1007/s00441-016-2562-z
32. Vidaillac C, Chotirmall SH. Pseudomonas aeruginosa in bronchiectasis: infection, inflammation, and therapies. Exp Rev Respir Med. 2021;15(5):649–662. doi:10.1080/17476348.2021.1906225
33. Brightling C, Greening N. Airway inflammation in COPD: progress to precision medicine. Europ Respir J. 2019;2.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Predictive Nomogram with Age and Laboratory Findings for Severe COVID-19 in Hunan Province, China
Jiang J, Zhong W, Huang W, Gao Y, He Y, Li X, Liu Z, Zhou H, Fu Y, Liu R, Zhang W
Therapeutics and Clinical Risk Management 2022, 18:579-591
Published Date: 17 May 2022
Establishment and Validation of a Predictive Nomogram for Hallux Valgus with Pain Under the Second Metatarsal
Bai Z, Cao X, Yang Y, Sun X, Dong Y, Wen J, Sun W
Journal of Pain Research 2022, 15:3523-3536
Published Date: 7 November 2022
Establishment and Validation of a Model for Disease-Free Survival Rate Prediction Using the Combination of microRNA-381 and Clinical Indicators in Patients with Breast Cancer
Shen J, Wang M, Li F, Yan H, Wang R, Zhou J
Breast Cancer: Targets and Therapy 2022, 14:375-389
Published Date: 30 November 2022
A Visualized Mortality Prediction Score Model in Hematological Malignancies Patients with Carbapenem-Resistant Organisms Bloodstream Infection
Qian C, Wu Q, Ruan Z, Liu F, Li W, Shi W, Ma L, Peng D, Yin H, Yao L, Li Z, Hong M, Xia L
Infection and Drug Resistance 2023, 16:201-215
Published Date: 7 January 2023
Establishment and Validation of a Predictive Model for Post-Treatment Anxiety Based on Patient Attributes and Pre-Treatment Anxiety Scores
Sun W, Shen J, Sun R, Zhou D, Li H
Psychology Research and Behavior Management 2023, 16:3883-3894
Published Date: 19 September 2023