")
Back to Journals » Journal of Inflammation Research » Volume 17
Predictive Efficacy of the Advanced Lung Cancer Inflammation Index in Hepatocellular Carcinoma After Hepatectomy
Authors Qiu X, Shen S , Lu D, Jiang N , Feng Y, Li J, Yang C, Xiang B
Received 12 March 2024
Accepted for publication 16 July 2024
Published 1 August 2024 Volume 2024:17 Pages 5197—5210
DOI https://doi.org/10.2147/JIR.S468215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Xin Qiu,1,2,* Shuang Shen,1,* Donghong Lu,2 Nizhen Jiang,3 Yifei Feng,3 Jindu Li,1 Chenglei Yang,1 Bangde Xiang1,4,5
1Department of Hepatobiliary Surgery, Guangxi Medical University Cancer Hospital, Nanning, People’s Republic of China; 2Department of Gastroenterology, The First Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China; 3Guangxi Medical University Cancer Hospital, Nanning, People’s Republic of China; 4Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor, Ministry of Education, Nanning, People’s Republic of China; 5Guangxi Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor, Nanning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bangde Xiang; Chenglei Yang, Email [email protected]; [email protected]
Background: Hepatocellular carcinoma (HCC) presents a significant global health challenge due to its poor prognosis and high recurrence rates post-surgery. This study examines the predictive efficacy of the Advanced Lung Cancer Inflammation Index (ALI) in assessing the post-hepatectomy prognosis of patients with HCC.
Methods: A cohort comprising 1654 HCC patients who underwent hepatectomy at Guangxi Medical University Cancer Hospital from 2013 to 2019 was enrolled. Patients were stratified into two groups according to the median ALI level, and then subjected to propensity score matching (PSM) in a 1:1 ratio. Kaplan-Meier survival curves, the traditional Cox proportional hazards (CPH) model, and machine learning (ML) models were employed to analyze and evaluate ALI’s prognostic significance. Furthermore, ALI’s prognostic value in digestive system tumors was validated via analysis of the National Health and Nutrition Examination Survey (NHANES) database.
Results: After applying PSM, a final cohort of 1284 patients, categorized into high and low ALI groups, revealed a significantly reduced survival time in the low ALI cohort. Univariate and multivariate Cox analyses identified ALI, BCLC stage, CK19, Hepatitis B virus (HBV) DNA, lymph node metastasis, and microvascular invasion (MVI) as independent predictors of prognosis. Both traditional CPH and ML models incorporating ALI demonstrated excellent predictive accuracy, validated through calibration curves, time-dependent ROC curves, and decision curve analysis. Furthermore, the prognostic value of ALI in digestive tumors was confirmed in the NHANES database.
Conclusion: The ALI exhibits potential as a prognostic predictor in patients with HCC following hepatectomy, providing valuable insights into postoperative survival.
Keywords: advanced lung cancer inflammatory index, ALI, hepatocellular carcinoma, HCC, prognosis, Cox regression, machine learning, ML
Introduction
Primary liver cancer ranks as the sixth most prevalent cancer globally,1 with a 5-year survival rate as low as 21%.2 Hepatocellular carcinoma (HCC) constitutes 80% of these cases3 and surgical resection remains the optimal treatment. However, due to challenges in early diagnosis, approximately 9% and 55% of HCC cases in China were initially diagnosed at intermediate and advanced stages, respectively, missing the window for surgery.4 Furthermore, approximately 60–80% of patients experience recurrence or distant metastasis within 5 years post-surgery.5 Current approaches for advanced HCC treatment involve radiotherapy, chemotherapy, immunotherapy, etc. Yet, owing to the considerable heterogeneity of HCC, the efficacy is generally suboptimal.6 Consequently, improving the prognosis of HCC patients stands as a pressing challenge.
Recent evidence highlights the pivotal role of systemic inflammation and malnutrition in the onset and progression of cancers.7 Systemic inflammation may occur in response to malignant neoplasia, mediated by immune proteins, cytokines, and immune cells.8 Simultaneously, malnutrition significantly affects all aspects of cancer management and prognosis by diminishing treatment effectiveness, exacerbating treatment-related side effects, and decreasing patients’ quality of life.8,9 Inflammation- or nutrition-based indices such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and C-reactive protein-to-albumin ratio (CAR) are widely employed for early prognosis assessment in various tumors.10–12 The Advanced Lung Cancer Inflammation Index (ALI), initially proposed by Syed H. Jafri et al in 2013,13 has proven to be an excellent prognostic predictor in lung cancer. Subsequently, ALI has demonstrated prognostic value in various tumors, such as colorectal cancer, gastric cancer, and myeloma14–17 and correlated with a better prognosis. In liver cancer, ALI may predict the efficacy of immunotherapy in advanced HCC patients5,18 and predict the overall survival and cancer-specific survival after hepatectomy.17 However, research on the role of ALI in patients undergoing hepatectomy for HCC is limited because of the imbalance of the clinicopathological data and hindered by small sample sizes. Therefore, the value of ALI in HCC patients after surgery requires further investigation.
This study aims to investigate the prognostic significance of ALI in HCC patients post-hepatectomy. We evaluated the significance of ALI in predicting overall survival (OS) and constructed both traditional Cox proportional hazards (CPH) models and machine learning (ML) models. Subsequently, we validated their effectiveness in a separate validation set. We anticipate that these findings may contribute to identifying effective prognostic biomarkers and ultimately improving the prognosis for HCC patients.
Methods
Patient Selection
Over the period spanning December 2013 to December 2019, a total of 2198 consecutive adult patients, aged 18 years or older, underwent surgical interventions at Guangxi Medical University Cancer Hospital. These individuals underwent validation for HCC through a combination of radiological and histological methodologies. The patients underwent a thorough evaluation. Inclusion criteria comprised individuals who (1) underwent R0 resection, characterized by complete tumor removal with a negative microscopic margin; (2) were postoperatively confirmed to have HCC through pathology; and (3) had no history of prior anti-cancer treatments, including radiation, transcatheter arterial chemoembolization (TACE), or targeted therapy. Exclusion criteria were applied to patients with (1) incomplete clinical data, (2) a follow-up duration of less than 30 days, or (3) concurrent presence of other malignancies. The study followed the principles outlined in the Declaration of Helsinki (2013 revision) and obtained approval from the Ethics Committee of Guangxi Medical University Cancer Hospital (Approval No. KY2024017). Written informed consent was obtained from all eligible participants enrolled in the study. The investigators were aware of both the outcome and predictor variables as blinding was not implemented.
Mortality outcomes and survival analysis data from individuals participating in National Health and Nutrition Examination Survey (NHANES)19 between 1999 and 2020 were correlated to demonstrate the effectiveness of ALI in an external dataset. The NHANES, conducted by the Centers for Disease Control and Prevention (CDC), is a biennial cross-sectional survey. Its primary objective is to assess the nutritional and health status of children and adults in the United States. NHANES employs a complex multistage probability sampling design20 to select a representative sample of the US population. The survey includes interviews covering demographic, dietary, health-related, and socio-economic factors, supplemented by laboratory tests conducted by trained medical personnel. All NHANES protocols obtained ethical approval from the National Center for Health Statistics Board, and participants provided written informed consent.
Clinicopathological Characteristics
Within 24 hours before surgery, clinical characteristics and biochemical data, including age, gender, height, weight, albumin (ALB), absolute neutrophil count, absolute lymphocyte count, platelet (PLT) count, total bilirubin (TBIL), HBV DNA load, HBsAg, ascites, alpha-fetoprotein (AFP), BCLC (Barcelona Clinic Liver Cancer) staging, Child-Pugh classification, intrahepatic bile duct dilation (IHBD), cirrhosis, splenomegaly, and alcohol history, were collected. Postoperatively, pathological details, such as microvascular invasion (MVI), Edmondson-Steiner grading, lymph node metastasis, tumor quantity, and cytokeratin 19 (CK19), were documented.
Follow-Up and Survival
Following hepatectomy, examinations were performed bi-monthly during the initial two years, transitioning to a three-month frequency thereafter. Clinical monitoring, including physical examinations, liver function tests, blood routine assessments, AFP level evaluations, and at least one imaging technique (eg, abdominal ultrasonography, enhanced computed tomography, or magnetic resonance imaging), was implemented. Patient follow-ups extended from admission until either death or September 2023. Overall survival (OS) was defined as the duration between hepatectomy and the occurrence of death or the conclusion of the follow-up period.
ALI Calculations
ALI was computed using the following formulas: ALI = Body Mass Index (BMI) * ALB / NLR. BMI is determined by the weight (in kilograms) divided by the square of height (in meters). ALB represents the serum albumin level (in g/dL), and NLR is calculated as the absolute neutrophil count divided by the absolute lymphocyte count.
The Construction of the Traditional CPH Model and ML Model
Patients were categorized into high and low ALI groups based on the median ALI level. To minimize potential confounding factors in prognostic assessment, we employed 1:1 propensity score matching (PSM) with a tolerance of 0.05 (12, 13). The traditional CPH model was developed using univariate and multivariate analysis, predicting patient survival outcomes with significant independent predictor variables (P < 0.05). The model evaluation consists of assessing the area under the receiver operating characteristic (ROC) curve, Harrell’s C-index, and time-based decision curve analysis (DCA).
To explore and validate ALI’s role in the postoperative prognosis of HCC patients, we incorporated a variety of ML algorithms and combinations, such as Elastic Net (Enet), CoxBoost, Random Survival Forest (RsF), and Survival Support Vector Machine (SVM). After PSM processing, outliers were initially trimmed based on quartiles, and pairwise Pearson correlation matrices were employed to assess collinearity among variables (with a threshold of r > 0.8). Then, stepwise Cox and Least Absolute Shrinkage and Selection Operator (LASSO) algorithms were employed for feature selection. The data were randomly divided into training and testing sets at a 7:3 ratio, followed by grid search for five-fold cross-validation to ascertain the optimal model hyperparameters. For each model obtained, the C-index was computed on the test set, and the model with the highest average C-index was chosen as the best model.
The chi-square test was utilized for analyzing categorical variables. All analyses were conducted using R software version 4.3.2 (http://www.r-project.org/) and Python software version 3.10 (https://www.python.org/). The following R packages were utilized: “readxl”, “survminer”, “survival”, “ggplot2”, “compareGroups”, “tableone”, “MatchIt”, “plyr”, “car”, “rms”, “pROC”, “timeROC”, “caret”, “PredictABEL”, “ggDCA”, “tidyverse”, “reshape2”, “ggcorrplot”, “cormtcars”, “DynNom”, “foreign”, and “rsconnect”. A P-value < 0.05 was deemed statistically significant.
Results
Baseline Characteristics
A total of 2198 patients underwent screening, and ultimately, 1654 patients met the inclusion criteria (Figure 1). In this cohort, 86.28% of the patients were female, with a mean age of 52.99 years. Approximately 85.49% of the patients tested positive for HBsAg. Based on the median ALI, patients were categorized into high ALI (n=827) and low ALI (n=827). There were no differences in gender, HBV DNA, and liver cirrhosis between these two groups (Supplementary Table 1). However, significant disparities were observed in age, AFP, HBsAg, BCLC stage, and MVI between the high and low ALI groups (P<0.05), which may confound ALI’s predictive ability. Then, we performed PSM to balance these unequal factors. As a result, 1282 patients (641 per group) were obtained through PSM, and their characteristics are detailed in Table 1. The mean age was 52.84 ± 11.11 years in the low ALI group and 53.52 ± 11.90 years in the high ALI group. The proportions of males were 85.65% and 85.96%, respectively, indicating similarity between the two groups. No significant disparities were observed in various clinical and postoperative pathological characteristics.
 |
Table 1 Characteristics of PSM HCC Patients |
 |
Figure 1 Patient Selection Flowchart. |
Survival Benefits for Patients with High ALI
The median OS for low ALI patients was 44 months, whereas high ALI patients experienced an extended survival period of 49 months. High ALI patients exhibited a significantly prolonged OS (P=0.002), with higher OS rates (Figure 2A). The 1-year, 3-year, and 5-year survival rates were 90.04%, 74.94%, and 66.66% for patients in the high ALI group, respectively, compared to 83.30%, 66.87%, and 59.54% for those in the low ALI group. The hazard ratio (HR) for ALI was 0.75, with a 95% confidence interval (CI) ranging from 0.62 to 0.90. These findings suggest that ALI may serve as an outstanding prognostic factor for postoperative survival in HCC patients.
 |
Figure 2 OS and Variable Correlation of ALI. (A) OS analysis for patients categorized by low or high ALI. (B) Heat map illustrating the correlation between variables, with color depth indicating the value. (C) OS analysis for patients in both training and validation datasets. |
Selection of Independent Prognostic Factors
To explore the potential correlations among the included study variables, we calculated the Pearson correlation and presented it in a heatmap (Figure 2B). Consistent with clinical knowledge, splenomegaly exhibited a close association with liver cirrhosis and platelet count, while Child-Pugh grade was correlated with TBIL and ascites. However, ALI showed no significant relationship with other variables, indicating its potential as an independent biomarker.
We then performed univariate and multivariate Cox analyses to identify potential risk factors for OS. ALI, splenomegaly, BCLC stage, CK19, HBV DNA, lymph node metastasis, and MVI were identified as independent prognostic factors influencing OS (Table 2).
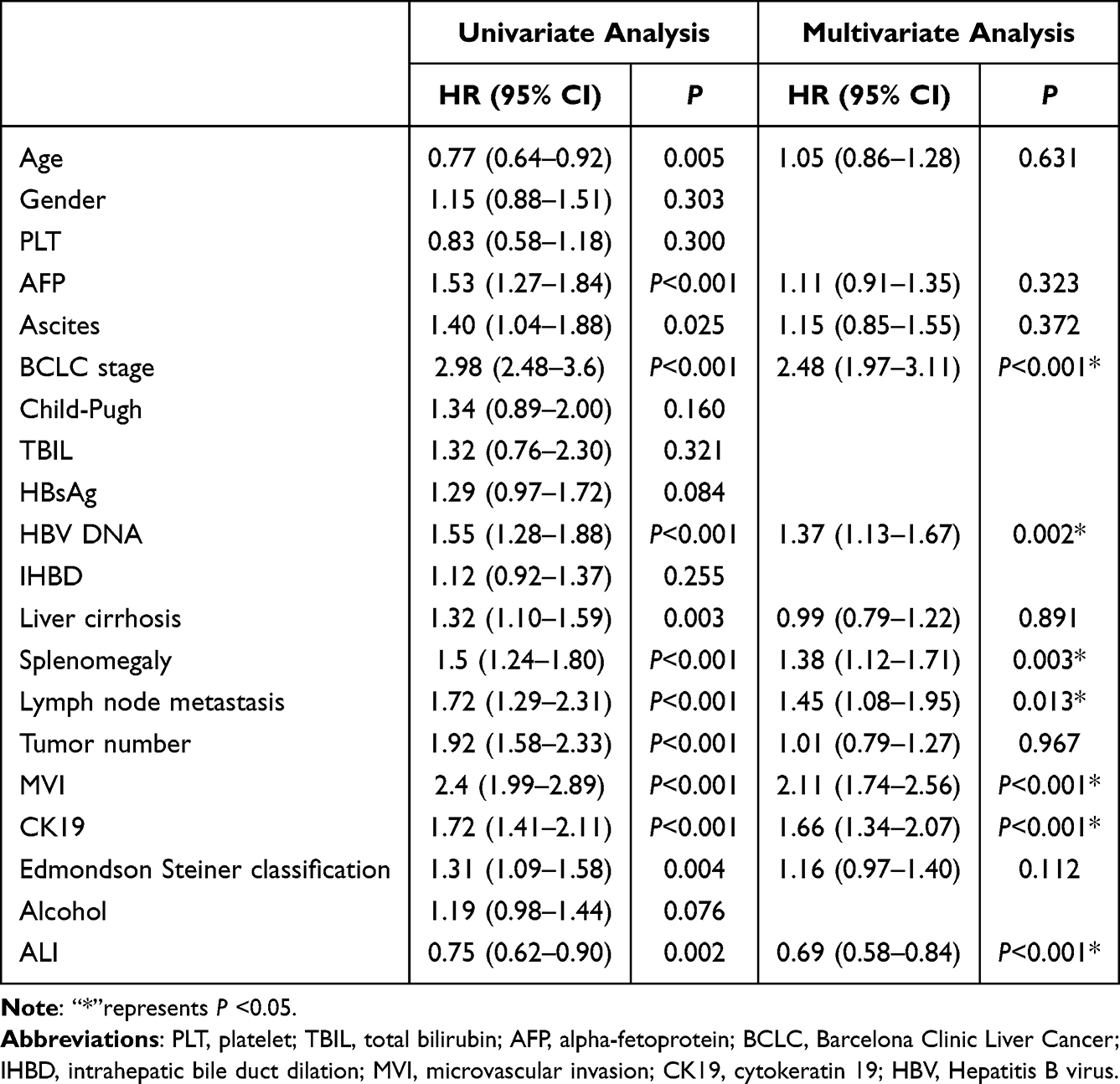 |
Table 2 Univariate and Multivariate Analysis for OS |
Construction, Evaluation, and Validation of the CPH Model and ML Model
The patients were randomly divided into a training dataset (n=898) and a validation dataset (n=384) at a 7:3 ratio. There were no differences in basic clinicopathologic characteristics (see Supplementary Table 2) and survival (Figure 2C) between the two groups. To enhance the predictive accuracy for OS, we developed a diagnostic nomogram incorporating the aforementioned independent variables (Figure 3) which is available on the website: https://aliqiuxin.shinyapps.io/DynNomapp/. The calibration curves demonstrated exceptional consistency in the OS rates between the model’s predictions and actual observations. The standard lines in both the training and validation sets closely matched the calibration curves, regardless of the 1-year, 3-year, or 5-year timeframes. (Figure 4A and B). Furthermore, we evaluated the model’s accuracy through 1000 bootstrapped resamples, resulting a C-index of 0.714 (95% CI, 0.682, 0.738) for the training set and 0.706 (95% CI, 0.658, 0.741) for the validation set. Subsequently, time-dependent ROC curves were generated to validate the model’s predictive capability. The AUCs for the 1-, 3-, and 5-year survival rates in the training set were 0.805, 0.751, and 0.749, respectively (Figure 4C). Similarly, the AUCs for the 1-, 3-, and 5-year survival rates in the validation set were 0.783, 0.728, and 0.724, respectively (Figure 4D). Then, we compared our nomogram with traditional predictive methods, such as BCLC,21 China liver cancer staging (CNLC),22 Albumin-Bilirubin (ALBI),23 Okuda,24 and Tumor-Node-Metastasis (TNM)25 stages. The AUC values of the nomogram were significantly higher than those of the traditional methods in both the training and validation datasets (Figure 4E and F). Additionally, DCA curves were constructed to further assess the nomogram (4 G, H). DCA is a method used to evaluate the clinical value of predictive models by considering the net benefit across different risk thresholds. If the model curve is above the baseline lines (ALL and None) in most or all risk thresholds, it indicates that the model has higher utility and net benefit in prediction. In our study, the nomograms for 1-, 3-, and 5-year predictions were all above the ALL and None lines in the training dataset, and mostly above these baselines in the validation dataset, suggesting that the nomogram model formulated in this investigation demonstrates robust predictive consistency, offering enhanced accuracy in forecasting the prognosis of HCC patients with hepatectomy.
 |
Figure 3 Nomogram for OS Forecast in HCC Patients Post-Hepatectomy. |
 |
Figure 4 Nomogram Assessment at 1-, 3-, and 5-Year OS. (A) Calibration curves in the training dataset. (B) Calibration curves in the validation dataset. (C) ROC curves in the training dataset. (D) ROC curves in the validation dataset. (E) ROC curves of nomogram and traditional predictive methods in 1-year OS of training database. (F) ROC curves of nomogram and traditional predictive methods in 1-year OS of validation database. (G) DCA curves in the training dataset. (H) DCA curves in the validation dataset. |
To enhance our understanding of whether ALI exhibits consistent predictive abilities for postoperative HCC patients across different models, we utilized various ALI-based ML methods and ensemble validations. Utilizing 9 different algorithms, we constructed predictive models on our dataset and calculated the C-index and ROC curves for each model and presented these values of the test dataset in Figure 5A. The specific values of AUC for the training and validation datasets are shown in Supplementary Table 3, while the ROC curves for each dataset are presented in Supplementary Figure 1. The results showed that the combination of the Survival-SVM model was optimal, achieving the highest average C-index (0.7138). Compared to the actual survival outcomes in the same dataset, the combined model performed excellently in predicting 1-year, 3-year, and 5-year OS (represented as 0.8052, 0.7432, and 0.7644, respectively). Interestingly, we observed that the C-index for the other 8 models based on ALI exceeded 0.7, demonstrating remarkable accuracy in predicting OS at 1, 3, and 5 years. This underscores the fact that even after adjusting for available algorithms and clinical features, ALI still retains favorable predictive efficacy.
 |
Figure 5 Predictive Performance of Machine Learning Models and OS in NHANES. (A) Evaluation of machine learning models using the C-index and ROC curves in the validation dataset. (B) OS analysis for patients with digestive cancers in the NHANES database. |
Significance of ALI in Digestive Tumors
To further investigate the significance of ALI in predicting the prognosis of cancers, particularly digestive system tumors (including HCC), we investigated its role in NHANES database. From 1999 to 2020, a total of 111,066 individuals were investigated, among them, 5769 (5.19%) were diagnosed with cancer, and 522 (0.47%) were patients with digestive neoplasms. Among these digestive cancer patients, 343 patients with complete survival and clinical data were enrolled for further analysis. After calculating the ALI value of each patient, we divided them into low and high group according to the median (ALI=53.70) in a similar manner. The clinical data in each group were comparable (Table 3), and patients with a high ALI value had significantly prolonged survival time (Figure 5B). The median survival times for the high and low ALI groups were 160 and 87 months, respectively. The 1-year, 3-year, and 5-year survival rates for patients in the high ALI group were 97.08%, 88.91%, and 82.14%, respectively, compared to 97.09%, 82.46%, and 69.27% for those in the low ALI group. These findings suggest that ALI serves as an excellent predictor not only in HCC patients who underwent surgery but also in patients with digestive cancers.
 |
Table 3 Characteristics of NHANES Patients |
Discussion
Malnutrition and inflammation are closely related with the survival state of cancer patients, leading to immune deficiencies and metabolic disorders.26 However, few markers can effectively combine inflammation and nutrition. Therefore, it is crucial to explore an efficient indicator that can seamlessly integrate these factors. ALI, characterized by the amalgamation of BMI, albumin, and NLR, proficiently accomplishes this task, representing the simultaneous state of nutritional well-being and inflammatory response. In colorectal cancer patients undergoing surgery, a lower ALI was associated with an increased occurrence of postoperative complications and poorer OS.14 Likewise, ALI serves as a proficient predictor for both postoperative complications and the long-term outcomes in individuals diagnosed with gastrointestinal cancer.27 In HCC, ALI is also a prognostic marker in patients receiving immunotherapy.5,18 However, the value of ALI in HCC patients received surgery was rarely explored. In this study, we collected clinical data of 1654 HCC patients who underwent hepatectomy to explore the significance of ALI. To mitigate the influence of confounding factors, we employed PSM and found no difference between low and high ALI after matching. Consistent with previous studies, the patients with higher ALI showed obviously prolonged survival, establishing ALI as a standalone risk determinant for OS. Furthermore, the COX model based on ALI, along with various ML algorithm models, exhibited excellent AUC values and predictive capabilities, indicating ALI as an outstanding prognostic factor for the survival of HCC patients after liver resection.
To further validate ALI’s prognostic predictor function, we explored its role in the NHANES database, a nationally representative cross-sectional survey. Due to the low incidence of HCC in the United States, we attempted to explore ALI’s function in digestive cancer sufferers. Surprisingly, ALI was also strongly associated with the prognosis in digestive tumors. Patients with high ALI showed significantly lengthened OS compared to those with low ALI. These data provide robust external evidence for the prognostic value of ALI.
The significance of ALI in HCC patients post-surgery was first discussed by Wen YZ et al.17 They found that ALI had robust predictive value and constructed a nomogram incorporating ALI, age, and TNM stage. However, the study’s sample size of 425 patients was relatively small, which limited its reliability. In this study, the sample size surpasses 1000 cases, this substantial sample volume significantly bolsters statistical power, ensuring robust stability and consistency. Furthermore, Wen YZ et al only compared some clinical data between the high and low ALI groups, without discussing common biochemical markers and pathological results. In our study, beyond the variables necessary for calculating ALI, we incorporated 20 additional variables, comprehensively covering all crucial indicators for HCC patients both before and after surgery. The baseline data is exceptionally comprehensive; therefore, the ALI value derived from this study possesses greater persuasiveness.
Confounding variables pose significant challenges in retrospective studies, often difficult to mitigate. For example, in a study assessing the prognostic nutritional index (PNI) in HCC, differences in age, BMI, CNLC stage, and tumor number between low and high PNI groups substantially undermine the confidence in PNI’s prognostic value.28 Similarly, in a study examining C-reactive protein (CRP) as a predictor of response to PD-1 inhibitors in HCC patients, inconsistencies in AFP level, NLR, and tumor size across high and low CRP groups greatly diminish result credibility.29 However, the clinicopathological data in the low and high ALI groups in our study underwent PSM, which excluded 372 cases to ensure baseline data balance. All variables across these two groups showed no discrepancies, maximizing control over confounding factors, bolstering the credibility of causal inference, and enhancing internal validity, thus strengthening the convincingness of our results.
In the present era, numerous novel biomarkers and methods predict the survival of cancer patients after surgery, including results from bulk transcriptomics and single-cell sequencing analysis,30,31 MR features,32 and the expression of specific genes in the tumor.33,34 However, the costs of these methods are generally high and pose a considerable economic burden for patients and are difficult to apply in clinical practice. In contrast, ALI is derived from BMI, blood routine, and liver function results, which are all common clinical indexes. These indicators are easily accessible, and calculating the value of ALI is straightforward. While for the common existing prognostic measures, such as the BCLC and CNLC stages, generally have low specificity and sensitivity, resulting in smaller AUC values and difficulties in accurately predicting survival outcomes for HCC patients post-surgery. By incorporating ALI into routine clinical assessments, healthcare providers can more accurately stratify patients into different risk categories. This stratification enables clinicians to tailor treatment plans more effectively, ensuring that high-risk patients receive more aggressive and timely interventions while low-risk patients can be managed with less intensive approaches. Moreover, traditional nomograms are cumbersome to calculate; therefore, we developed a web-based nomogram to overcome this limitation. Serving as a network or mobile-based clinical decision tool, it enables clinicians to effortlessly input seven clinical data points, significantly enhancing convenience. This model holds significant promise for widespread adoption and application.
BMI, a fundamental metric for assessing body obesity, frequently functions as a broad indicator reflecting overall nutritional status. A low BMI value is an important diagnostic standard of cachexia,35 generally associated with a poor prognosis. Conversely, an appropriate BMI may indicate better nutritional condition and boost immune function to fight against cancer.36 Albumin, the richest protein in the body, is mainly synthesized by the liver and maintains colloid osmotic pressure.37 Additionally, albumin mediates inflammation by binding and transporting inflammatory substances,38 protecting tissues against inflammatory injury.39 Low albumin is related to malnutrition, weaker systemic inflammatory reactions, and poorer survival.40 In normal individuals, neutrophil may swallow bacteria and exert anti-inflammatory function. In the tumor patients, neutrophil may produce reactive oxygen species and nitric oxide with a potential ability to inhibit T-cell differentiation,41 playing a role in promoting cancer. While Lymphocytes, mainly including T cells, B cells, and Natural killer cells, play a crucial role in the adaptive response of the immune system and act as key mediators of humoral and cellular immunity.42 The ratio of neutrophils and lymphocytes, namely NLR, has been reported to predict outcomes in many cancers, such as non-small cell lung cancer, gastric cancer, and rectal cancer.43–45 Therefore, maintaining a suitable BMI, an elevated albumin level, and a reduced NLR can result in an increased ALI level, ultimately contributing to an improved prognosis.
Our study has certain limitations. Firstly, it was conducted in a single center, which may pose challenges to internal validity. The generalizability of our study outcomes might be limited by specific geographic locations, patient demographics, or treatment modalities. Despite utilizing the NHANES database for external validation, it is not exclusive to HCC patients and lacks sufficient externally matched clinical-pathological data to validate the efficacy of ALI and the nomogram. Therefore, our primary objective was to anchor our findings in authentic scenarios using extensive sample data, aiming to address these limitations and highlight potential avenues for model improvement. Secondly, although the study addressed potential confounding factors like age and gender, it inadequately considered other variables such as socioeconomic status, necessitating further investigation. In subsequent research phases, we intend to perform external validation across diverse cohorts and conduct prospective investigations both locally and internationally to enhance the accuracy of our findings. Thirdly, while we introduced an outstanding index and model for predicting post-hepatectomy survival in HCC patients, specific strategies to improve OS were not delineated. Nevertheless, given the rapid advancements in targeted immunotherapy for HCC, we contend that our model establishes a foundation for further analyses in this field and may facilitate the integration of innovative therapeutics in the future.
Conclusion
ALI is an effective prognostic predictor for HCC patients post-surgery. The nomogram and ML models based on ALI provide clinicians with valuable insights into patient survival outcomes. This study may enhance comprehensive treatment strategies and improve survival rates for HCC patients after surgery.
Acknowledgments
We express our gratitude to all the staff contributing to this study.
Funding
This work was supported by grants from the National Natural Science Foundation of China (82260573), National Major Special Science and Technology Project (2017ZX10203207), High-level innovation team and outstanding scholar program in Guangxi Colleges and Universities, “139” projects for training high-level medical science talents from Guangxi (G201903001), The Key Research and Development Project of Guangxi (AB20297009, AA18221001, AB18050020), The Key Laboratory of Early Prevention and Treatment for Regional High-Frequency Tumor, Ministry of Education/Guangxi, Independent Research Project (GKE2017-ZZ02, GKE2018-KF02, GKE2019-ZZ07), Development and application of medical and health appropriate technology in Guangxi (S2019039), and Youth Science Foundation of Guangxi Medical University (GXMUYSF202321 and GXMUYSF202407).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
2. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA. 2023;73(1):17–48. doi:10.3322/caac.21763
3. Ladd AD, Duarte S, Sahin I, Zarrinpar A. Mechanisms of drug resistance in HCC. Hepatology. 2023;79(4):926–940. doi:10.1097/HEP.0000000000000237
4. Park JW, Chen M, Colombo M, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Int. 2015;35(9):2155–2166. doi:10.1111/liv.12818
5. Li Q, Ma F, Wang J. Advanced lung cancer inflammation index predicts survival outcomes of hepatocellular carcinoma patients receiving immunotherapy. Front Oncol. 2023;13:997314.
6. Shi Y, Wang Y, Niu K, Zhang W, Lv Q, Zhang Y. How CLSPN could demystify its prognostic value and potential molecular mechanism for hepatocellular carcinoma: a crosstalk study. Comput Biol Med. 2024;172:108260. doi:10.1016/j.compbiomed.2024.108260
7. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013
8. Gavriilidis P, Pawlik TM. Inflammatory indicators such as systemic immune inflammation index (SIII), systemic inflammatory response index (SIRI), neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) as prognostic factors of curative hepatic resections for hepatocellular carcinoma. Hepatobiliary Surg Nutr. 2024;13(3):509–511. doi:10.21037/hbsn-23-631
9. Xie H, Wei L, Ruan G, et al. Performance of anthropometry-based and bio-electrical impedance-based muscle-mass indicators in the Global Leadership Initiative on Malnutrition criteria for predicting prognosis in patients with cancer. Clin Nutr. 2024;43(7):1791–1799. doi:10.1016/j.clnu.2024.05.039
10. Asaka S, Shimakawa T, Nishiguchi R, et al. Preoperative and postoperative c-reactive protein to albumin ratio (CAR) as a prognostic marker for survival of esophageal squamous cell carcinoma patients after surgery. Anticancer Res. 2023;43(11):5139–5147. doi:10.21873/anticanres.16714
11. Ruan GT, Xie HL, Yuan KT, et al. Prognostic value of systemic inflammation and for patients with colorectal cancer cachexia. J Cachexia Sarcopenia Muscle. 2023;14(6):2813–2823. doi:10.1002/jcsm.13358
12. Sonehara K, Ozawa R, Hama M, et al. Predictive factors associated with long-term response to combination immunotherapy in patients with untreated advanced non-small-cell lung cancer: a multicenter retrospective study. Oncology. 2023;101(7):425–434. doi:10.1159/000531324
13. Huang X, Liu Y, Liang W, et al. A new model of preoperative systemic inflammatory markers predicting overall survival of osteosarcoma: a multicenter retrospective study. BMC Cancer. 2022;22(1):1370. doi:10.1186/s12885-022-10477-8
14. Zhang B, Li ZW, Tong Y, et al. The predictive value of advanced lung cancer inflammation index for short-term outcomes and prognosis of colorectal cancer patients who underwent radical surgery. Int J Clin Oncol. 2023;28(12):1616–1624. doi:10.1007/s10147-023-02410-1
15. Huo C, Liu Y, Xie F, Zhao L, Huang H, Feng Q. Advanced lung cancer inflammation index predicts the outcomes of patients with non-metastatic gastric cancer after radical surgical resection. J Gastrointest Oncol. 2023;14(3):1653–1654. doi:10.21037/jgo-23-315
16. Cheng J, Li Q, Xiao S, et al. The advanced lung cancer inflammation index predicts chemotherapy response and infection risk in multiple myeloma patients receiving induction chemotherapy. Front Genetics. 2022;13:1047326. doi:10.3389/fgene.2022.1047326
17. Wen YZ, Liu GM, Liao JP, Xu JW. Advanced lung cancer inflammation index predicts overall survival of hepatocellular carcinoma after hepatectomy. Front Oncol. 2024;14:1294253. doi:10.3389/fonc.2024.1294253
18. Liu C, Zhao H, Zhang R, Guo Z, Wang P, Qu Z. Prognostic value of nutritional and inflammatory markers in patients with hepatocellular carcinoma who receive immune checkpoint inhibitors. Oncol Lett. 2023;26(4):437. doi:10.3892/ol.2023.14024
19. Centers for Disease Control and Prevention. National health and nutrition examination survey. Available from: https://www.cdc.gov/nchs/nhanes/index.htm.
20. Ahluwalia N, Dwyer J, Terry A, Moshfegh A, Johnson C. Update on NHANES dietary data: focus on collection, release, analytical considerations, and uses to inform public policy. Adv Nutr. 2016;7(1):121–134. doi:10.3945/an.115.009258
21. Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Disease. 1999;19(3):329–338. doi:10.1055/s-2007-1007122
22. Zhou J, Sun H, Wang Z, et al. Guidelines for the diagnosis and treatment of primary liver cancer (2022 Edition). Liver Cancer. 2023;12(5):405–444. doi:10.1159/000530495
23. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach—The ALBI Grade. J clin oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
24. Okuda K, Ohtsuki T, Obata H, et al. Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 patients. Cancer. 1985;56(4):918–928. doi:10.1002/1097-0142(19850815)56:4<918::AID-CNCR2820560437>3.0.CO;2-E
25. Vauthey JN, Lauwers GY, Esnaola NF, et al. Simplified staging for hepatocellular carcinoma. J Clin Oncol. 2002;20(6):1527–1536. doi:10.1200/JCO.2002.20.6.1527
26. Arends J. Struggling with nutrition in patients with advanced cancer: nutrition and nourishment-focusing on metabolism and supportive care. Ann Oncol. 2018;29(Suppl 2):ii27–ii34. doi:10.1093/annonc/mdy093
27. Pang HY, Chen XF, Yan MH, et al. Clinical significance of the advanced lung cancer inflammation index in gastrointestinal cancer patients: a systematic review and meta-analysis. Front Oncol. 2023;13:1021672. doi:10.3389/fonc.2023.1021672
28. Hu Y, Cai Y, Ma W, et al. The prognostic nutritional index and tumor pathological characteristics predict the prognosis of elderly patients with early-stage hepatocellular carcinoma after surgery. Biosci Trends. 2023;17(5):369–380. doi:10.5582/bst.2023.01212
29. Zhang Y, Lu L, He Z, et al. C-reactive protein levels predict responses to PD-1 inhibitors in hepatocellular carcinoma patients. Front Immunol. 2022;13:808101. doi:10.3389/fimmu.2022.808101
30. Qu C, Wu Q, Lu J, Li F. Prognostic value and potential mechanism of cellular senescence and tumor microenvironment in hepatocellular carcinoma: insights from bulk transcriptomics and single-cell sequencing analysis. Environ Toxicol. 2024;39(5):2512–2527. doi:10.1002/tox.24121
31. Liu Y, Li H, Zeng T, et al. Integrated bulk and single-cell transcriptomes reveal pyroptotic signature in prognosis and therapeutic options of hepatocellular carcinoma by combining deep learning. Briefings Bioinf. 2023;25(1). doi:10.1093/bib/bbad487
32. Yang Y, Li L, Xu Y, et al. The GRAPHS-CRAFITY score: a novel efficacy predictive tool for unresectable hepatocellular carcinoma treated with immunotherapy. La Radiol Med. 2024. doi:10.1007/s11547-023-01753-z
33. Wang J, Che F, Zhao Y, et al. The prognostic and therapeutic roles of ARL-6 gene in hepatocellular carcinoma. Int J Med Sci. 2024;21(2):207–218. doi:10.7150/ijms.88039
34. Jia X, Wang Y, Yang Y, Fu Y, Liu Y. Constructed Risk Prognosis Model Associated with Disulfidptosis lncRNAs in HCC. Int J Mol Sci. 2023;24(24):17626. doi:10.3390/ijms242417626
35. McGovern J, Dolan RD, Skipworth RJ, Laird BJ, McMillan DC. Cancer cachexia: a nutritional or a systemic inflammatory syndrome? Br J Cancer. 2022;127(3):379–382. doi:10.1038/s41416-022-01826-2
36. Tajan M, Vousden KH. Dietary approaches to cancer therapy. Cancer Cell. 2020;37(6):767–785. doi:10.1016/j.ccell.2020.04.005
37. Wu B, Wang J, Chen Y, Fu Y. Inflammation-targeted drug delivery strategies via albumin-based systems. ACS Biomater Sci Eng. 2024;10(2):743–761.
38. Zhang C, Yang K, Yang G. Design strategies for enhancing antitumor efficacy through tumor microenvironment exploitation using albumin-based nanosystems: a review. Int J Biol Macromol. 2023;258(Pt 2):129070. doi:10.1016/j.ijbiomac.2023.129070
39. Duran-Güell M, Flores-Costa R, Casulleras M, et al. Albumin protects the liver from tumor necrosis factor α-induced immunopathology. FASEB J. 2021;35(2):e21365. doi:10.1096/fj.202001615RRR
40. Almasaudi AS, Dolan RD, Edwards CA, McMillan DC. Hypoalbuminemia reflects nutritional risk, body composition and systemic inflammation and is independently associated with survival in patients with colorectal cancer. Cancers. 2020;12(7):1986. doi:10.3390/cancers12071986
41. Mosca M, Nigro MC, Pagani R, De Giglio A, Di Federico A. Neutrophil-to-lymphocyte ratio (NLR) in NSCLC, gastrointestinal, and other solid tumors: immunotherapy and beyond. Biomolecules. 2023;13(12):1803. doi:10.3390/biom13121803
42. Klobuch S, Seijkens TTP, Schumacher TN, Haanen J. Tumour-infiltrating lymphocyte therapy for patients with advanced-stage melanoma. Nat Rev Clin Oncol. 2024;21(3):173–184. doi:10.1038/s41571-023-00848-w
43. Nindra U, Shahnam A, Stevens S, et al. Elevated neutrophil-to-lymphocyte ratio (NLR) is associated with poorer progression-free survival in unresectable stage III NSCLC treated with consolidation durvalumab. Thoracic Cancer. 2022;13(21):3058–3062. doi:10.1111/1759-7714.14646
44. Wang W, Tong Y, Sun S, et al. Predictive value of NLR and PLR in response to preoperative chemotherapy and prognosis in locally advanced gastric cancer. Front Oncol. 2022;12:936206. doi:10.3389/fonc.2022.936206
45. Polk N, Budai B, Hitre E, Patócs A, Mersich T. High neutrophil-to-lymphocyte ratio (NLR) and systemic immune-inflammation index (SII) are markers of longer survival after metastasectomy of patients with liver-only metastasis of rectal cancer. Pathol Oncol Res. 2022;28:1610315. doi:10.3389/pore.2022.1610315
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.