")
Back to Journals » Journal of Inflammation Research » Volume 17
Predictive Factors for Poor Outcomes Associated with COVID-19 in a Retrospective Cohort of Myasthenia Gravis Patients
Authors Bi Z , Gao H, Lin J, Gui M, Li Y, Li Z, Bu B
Received 26 April 2024
Accepted for publication 19 August 2024
Published 29 August 2024 Volume 2024:17 Pages 5807—5820
DOI https://doi.org/10.2147/JIR.S475729
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Zhuajin Bi,1,2 Huajie Gao,1,2 Jing Lin,1,2 Mengcui Gui,1,2 Yue Li,1,2 Zhijun Li,1,2 Bitao Bu1,2
1Department of Neurology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei Province, People’s Republic of China; 2Hubei Key Laboratory of Neural Injury and Functional Reconstruction, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Zhijun Li, Department of Neurology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei Province, People’s Republic of China, Email [email protected] Bitao Bu, Email [email protected]
Purpose: To investigate the predictors for poor outcomes (including disease exacerbation, hospitalization and myasthenic crisis) in patients with pre-existing myasthenia gravis (MG) following Coronavirus disease 2019 (COVID-19), and to explore the potential effects of COVID-19 on inflammatory and immune responses in MG patients.
Patients and Methods: This retrospective cohort study analyzed medical records of 845 MG patients who were diagnosed with COVID-19 between January 2020 to March 2023 at a single medical center.
Results: Generalized MG at onset and comorbidities (chronic kidney disease and malignancy) were independent risk factors of poor outcomes. Patients achieving minimal manifestation or better status before COVID-19 had a significantly reduced risk for poor outcomes. Furthermore, patients with older onset age or anti-acetylcholine receptor antibody had a higher risk of exacerbation and hospitalization than those without. Prednisone or immunosuppressant treatment had the potential to reduce the occurrence of poor outcomes, while the duration of prednisone or immunosuppressant usage was associated with a higher risk of poor outcomes. Of the 376 MG patients with blood results available, patients with COVID-19 tended to have higher levels of leukocyte counts, neutrophil-lymphocyte-ratio, hypersensitive C-reactive protein, and Interleukin-6, as well as lower percentages of lymphocytes and regulatory T cells compared to patients without COVID-19.
Conclusion: Disease severity at onset, comorbidities, and unsatisfactory control of myasthenic symptoms predicted the occurrence of poor outcomes in MG patients following COVID-19. The risk of poor outcomes was reduced in patients controlled by short-term immunosuppressive therapy. Novel coronavirus might affect inflammatory and immune responses in MG patients, particularly in altering interleukin-6 and regulatory T cell levels.
Keywords: myasthenia gravis, COVID‐19, poor outcomes, immunosuppressive treatment, immune responses
Introduction
Myasthenia gravis (MG) is an acquired autoimmune disorder of the neuromuscular junction mediated by pathogenic antibodies targeting acetylcholine receptors (AChR), muscle-specific kinase (MuSK), or lipoprotein-related protein 4 (LRP4).1,2 Clinically, it is characterized by fluctuating weakness and fatigability of skeletal muscles. The disease course of MG is highly variable, ranging from complete stable remission to relapse and even death. Despite therapeutic advances for the management of MG, approximately 34–69% of patients may experience recurrent exacerbations or even myasthenic crisis (MC) requiring repeated rescue with short-term intravenous immunoglobulin or plasma exchange treatments.1–3 Importantly, infection (particularly respiratory ones) is thought to be the main contributor to MG exacerbations, accounting for 15–40% of cases and a 3–8% mortality rate.4–6
Coronavirus Disease 2019 (COVID-19) is a contagious disorder caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.7–9 It has been reported that patients with MG are more susceptible to COVID-19 due to the weakened immune system and immunosuppressive treatments.9,10 In addition, several case reports demonstrated that patients with MG might face a particularly severe course of COVID-19 since infections could trigger MG exacerbation and even MC, which imposed a high disease burden on affected patients.11,12 Currently, although the therapeutic management of MG patients during the COVID-19 pandemic has been guided by expert consensus, predictors for poor outcomes (including disease exacerbation, hospitalization and MC) in MG patients following COVID-19 remain incompletely identified.13,14 Prognostic factors for poor outcomes can be useful for clinicians to predict which patients are at risk for a more severe and debilitating disease course during the COVID-19 pandemic. Therefore, we conducted a retrospective analysis of 845 MG patients with COVID-19 to identify risk factors for disease exacerbation, hospitalization, and MC.
Materials and Methods
Patients and Study Design
This study was based on a retrospective observational analysis of a single center cohort from January 2020 to March 2023, examining clinical records of all in- and out-patients with MG who were diagnosed with COVID-19 and treated at the Tongji Hospital, one of the largest comprehensive medical treatment center of central China. The diagnosis of MG was based on the clinical history of fluctuating muscle weakness and the presence of one or more of the following: a positive test for anti-AChR and/or anti-MuSK antibodies, a decrement of greater than 10% on repetitive nerve stimulation (RNS), or an unequivocally positive response to cholinesterase inhibitors.3,15 All patients in our cohort were confirmed with COVID-19 by nasopharyngeal swab specimens through SARS-CoV-2-PCR positive nasopharyngeal swab.16 Suspected cases without established diagnosis (n = 873), with insufficient case documentation (less than 6 months of longitudinal documentation) (n = 285), or with insufficient baseline data (n = 146) were excluded. In addition, patients with negative COVID-19 (n = 1164) or new-onset MG within 14 days after COVID-19 (n = 15) were excluded. After that, a total of 845 MG patients with confirmed COVID-19 were enrolled in this study. Figure 1 depicts the selection procedure.
 |
Figure 1 Study flowchart. Abbreviations: Jan, January; Mar, March; MC, myasthenic crisis; MG, myasthenia gravis; COVID-19, coronavirus disease-2019; RT-PCR, reverse transcription-polymerase chain reaction. |
Data Acquisition
Demographics and clinical information were collected including age, sex, disease duration, concomitant diseases, signs and symptoms of COVID-19, the status of antibody (anti-AChR-ab, anti-MuSK-ab, anti-Titin-ab and anti-LRP4-ab) evaluated as previously described,3 results of RNS test, thymus type, the Myasthenia Gravis Foundation of America (MGFA) classification and MGFA postintervention status (MGFA-PIS),17 and MG specific medications (pyridostigmine, prednisone and/or immunosuppressant) before COVID-19. To be specific, the age ranges of disease onset for juvenile MG (JMG), early-onset MG (EOMG), and late-onset MG (LOMG) were less than 18 years, 18–49 years, and 50 years or older, respectively.18 The MGFA is graded 1–5 based on an overall assessment of the severity of symptoms and signs.3,17,19 Minimal manifestation status (MMS) was defined as no symptoms of functional limitations of MG but weakness of extraocular muscles only detectable by examination.20 The thymus status was assessed and classified as normal (including atrophy, fatty and cystic), hyperplastic, or thymoma based on chest computed tomography scan and/or magnetic resonance imaging in non-thymectomized patients, and histologic examination in thymectomized patients.3 All chest images were reviewed by two senior radiologists. The cutoff between low‐dose prednisone and high-dose prednisone was set at 0.25 mg/kg/d prednisone or equivalent methylprednisolone/prednisolone as previously defined.21 Patients who received prednisone or immunosuppressant treatment less than 1 year after diagnosis were classified as early prednisone or immunosuppressant, and those treated with prednisone or immunosuppressants for 1 year or more were classified as late prednisone or immunosuppressant.19 The vaccinated status was classified as “unvaccinated” or ‘one or more vaccinations’ before COVID-19.22
In addition, laboratory results of blood routine, infection-related biomarkers, inflammatory cytokines, immunoglobulins, complement proteins, and lymphocyte subsets were collected from MG patients with and without COVID-19 who were treated at our center between January 2020 and March 2023. All laboratory tests were conducted on admission and completed by the clinical laboratory of Tongji Hospital.
Definitions of Outcomes
The primary outcome was exacerbation and secondary outcomes were hospitalization and MC. The exacerbation associated with COVID-19 was defined as the reappearance or worsening of one or more MG symptoms or signs of muscle weakness within 2 weeks following a positive PCR test, with a minimum increase of QMG scores ≥ 3 points from the previous visit, which lasted for more than 24 hours.3,5,23 Hospitalization to the medical center for exacerbation within 2 weeks following a positive PCR test was also considered a poor outcome. The MC was characterized by a rapid exacerbation of muscle weakness leading to respiratory failure requiring intubation and noninvasive ventilation.17
Statistical Analysis
Descriptive data are presented as mean ± standard deviation (SD) or median (interquartile range, IQR) for continuous variables, and as absolute numbers and percentages (%) for categorical variables. Categorical variables were analyzed using chi-square or Fisher’s exact test, while continuous variables using the Mann–Whitney-U-test or or unpaired t-test. To evaluate clinical factors that might affect the poor outcomes (including disease exacerbation, hospitalization, and MC), we performed univariate and multivariate logistic regression analyses with outcome measures and adjusted odds ratios (OR), and their 95% confidence intervals (CI) were calculated. Furthermore, logistic regression analysis was used to investigate the differences in serum markers between MG patients with and without SARS-CoV-2 infection, adjusting for age, sex, disease duration, MGFA classification, comorbidities, thymoma, COVID-19 vaccination, prednisone, and immunosuppressant treatment. All statistical analyses were performed with SPSS version 22.0 (SPSS Inc. Chicago, IL, USA) and R version 4.0.4, and two-tailed p < 0.05 was considered significant.
Results
Baseline Characteristics and clinical Features of Participants
A total of 845 patients (median [IQR] age at onset: 40.0 [16.4, 54.9] years; 56.4% female) had received an MG diagnosis before being infected with COVID-19 (Table 1). Among these patients, 817 patients (96.7%) exhibited symptoms of COVID-19 at the time of diagnosis. The common symptoms of COVID-19 were fever in 704 patients (83.3%), cough in 464 patients (54.9%), vomiting or diarrhea in 165 patients (19.5%), and myalgia in 156 patients (18.5%). COVID-19 vaccination status was available for 669 patients, and the total vaccination rate was 69.7%. The median (IQR) disease duration between disease onset and infection was 4.0 (1.8, 9.3) years. At the initial stage, 548 patients (64.9%) showed only ocular symptoms (MGFA class I), and 297 patients (35.1%) presented with generalized muscle weakness (MGFA class II–V). Before contracting COVID-19, the maximum disease severity was classified as ocular MG (MGFA class I) in 409 patients (48.4%), mild MG (MGFA class II) in 273 patients (32.3%), and moderate to severe MG (MGFA class III–V) in 163 patients (19.3%). The percentage of patients with anti-AChR-ab positivity, anti-MuSK-ab positivity, anti-Titin-ab positivity, and anti-LRP4-ab positivity was 77.5%, 2.3%, 18.9%, and 0.0%, respectively.
 |
Table 1 Demographics and Clinical Features of the Patients |
More than half of the patients received immunosuppressive treatments before COVID‐19, most commonly oral prednisone and tacrolimus. 549 patients (65.0%) received prednisone following diagnosis with a median (IQR) dosage of 10.0 (5.0, 10.0) mg. 443 patients (52.4%) received standard immunosuppressant treatment, including tacrolimus (n = 322), azathioprine (n = 40), mycophenolate mofetil (n = 50), methotrexate (n = 24) and rituximab (n = 7). The median (IQR) time between diagnosis and the start of the prednisone and IS was 1.0 (0.2, 5.7) and 2.2 (0.5, 7.6) years, respectively. Furthermore, there were 268 (48.8%) and 148 (33.4%) patients who received their first prednisone and IS less than 1 year after diagnosis and were classified as early prednisone or IS, respectively, while 281 (51.2%) and 295 (66.6%) patients who received prednisone and IS after 1 year or more and were considered as late prednisone or IS, respectively.
Predictors for Disease Exacerbation, Hospitalization and MC
Overall, 153 patients (18.1%) experienced a disease exacerbation of MG symptoms after COVID-19, of which 80 patients (9.5%) required hospitalization and 30 patients (3.6%) developed MC. The QMG scores for patients with acute exacerbations were significantly increased at the time of SARS-CoV-2 infection, with a mean QMG score of 11.2 ± 7.8 points (range = 3–24 points). To evaluate the potential risk factors for poor outcomes (including disease exacerbation, hospitalization, and MC), we first performed a binary logistic regression (seen in Supplementary Table S1). After that, we entered variables with p-value < 0.05 in univariate analysis into the multivariate logistic regression analysis to identify independent risk factors. The results showed that age at onset (OR = 1.013, 95% CI 1.002–1.026, p = 0.026), concomitant chronic kidney disease (OR = 4.576, 95% CI 1.320–15.868, p = 0.017), concomitant malignancy other than thymoma (OR = 3.006, 95% CI 1.199–7.541, p = 0.019), generalized disease at onset (OR = 1.683, 95% CI 1.037–2.733, p = 0.035), MMS or better status (OR = 0.130, 95% CI 0.082–0.206, p < 0.001), anti-AChR-ab (OR = 2.470, 95% CI 1.219–5.007, p = 0.012) and anti-MuSK-ab (OR = 5.077, 95% CI 1.405–18.347, p = 0.013) were independent predictors for disease exacerbation (Table 2). Multivariate analysis of independent predictors for hospitalization identified that age at onset (OR = 1.025, 95% CI 1.009–1.041, p = 0.002), concomitant chronic kidney disease (OR = 5.768, 95% CI 1.635–20.344, p = 0.006), concomitant malignancy other than thymoma (OR = 3.412, 95% CI 1.202–9.686, p = 0.021), generalized disease at onset (OR = 2.005, 95% CI 1.124–3.575, p = 0.018), MMS or better status (OR = 0.142, 95% CI 0.083–0.246, p < 0.001) and anti-AChR-ab (OR = 2.346, 95% CI 1.008–5.464, p = 0.048) as independent risk factors. Furthermore, multivariate analysis revealed concomitant chronic kidney disease (OR = 5.964, 95% CI 1.314–27.070, p = 0.021), concomitant malignancy other than thymoma (OR = 4.944, 95% CI 1.227–19.921, p = 0.025), generalized disease at onset (OR = 2.957, 95% CI 1.175–7.443, p = 0.021), and MMS or better status (OR = 0.217, 95% CI 0.096–0.488, p < 0.001) predicted the occurrence of MC as independent risk factors (Table 2).
 |
Table 2 Multivariate Logistic Regression Analysis for the Risk Factors for Disease Exacerbation, Hospitalization, and MC |
In addition, we investigated whether therapeutic management of MG influences poor outcomes during SARS-CoV-2 infection. We first tested the effects of different treatment modalities (none medication, pyridoxamine alone, and a combination of pyridostigmine, low-dose/high-dose prednisone, and IS) on the occurrence of exacerbation, hospitalization, and MC. After adjusting for confounding factors, including age at onset, sex, chronic comorbidities, symptoms at onset, MGFA classification, MGFA-PIS, the status of anti-AChR-ab and anti-MuSK-ab, our data showed that none medication (OR = 13.717, 95% CI 4.824–39.003, p < 0.001) was an independent risk factor for exacerbation, while pyridostigmine alone was an independent risk factor for exacerbation and hospitalization (exacerbation: OR = 2.144, 95% CI 1.228–3.743, p = 0.007, hospitalization: OR = 2.525, 95% CI 1.197–5.325, p = 0.015) (Figure 2 and Supplementary Table S2). However, the risk for exacerbation (OR = 0.410, 95% CI 0.190–0.885, p = 0.023) and hospitalization (OR = 0.245, 95% CI 0.067–0.888, p = 0.032) were reduced for patients receiving pyridostigmine and IS compared with those who did not. To further dissect the importance of therapeutic management, we analyzed the effects of prednisone or IS dosage, duration of drug maintenance, and the timespan between disease onset and drug administration on poor outcomes. In the group of prednisone-treated patients, the use of prednisone had the potential to reduce the occurrence of exacerbation (OR = 0.635, 95% CI 0.410–0.982, p = 0.041), while the duration of prednisone usage was associated with a higher risk of exacerbation (OR = 1.236, 95% CI 1.102–1.388, p < 0.001) and hospitalization (OR = 1.287, 95% CI 1.123–1.474, p < 0.001). Similarly, the use of IS predicted the reduction of the risk of exacerbation (OR = 0.443, 95% CI 0.278–0.705, p = 0.001), hospitalization (OR = 0.387, 95% CI 0.209–0.715, p = 0.002) and MC (OR = 0.379, 95% CI 0.149–0.965, p = 0.042), while the duration of IS usage was associated with a higher risk of exacerbation (OR = 1.391, 95% CI 1.179–1.643, p < 0.001), hospitalization (OR = 1.498, 95% CI 1.191–1.883, p = 0.001) and MC (OR = 1.433, 95% CI 1.021–2.011, p = 0.037).
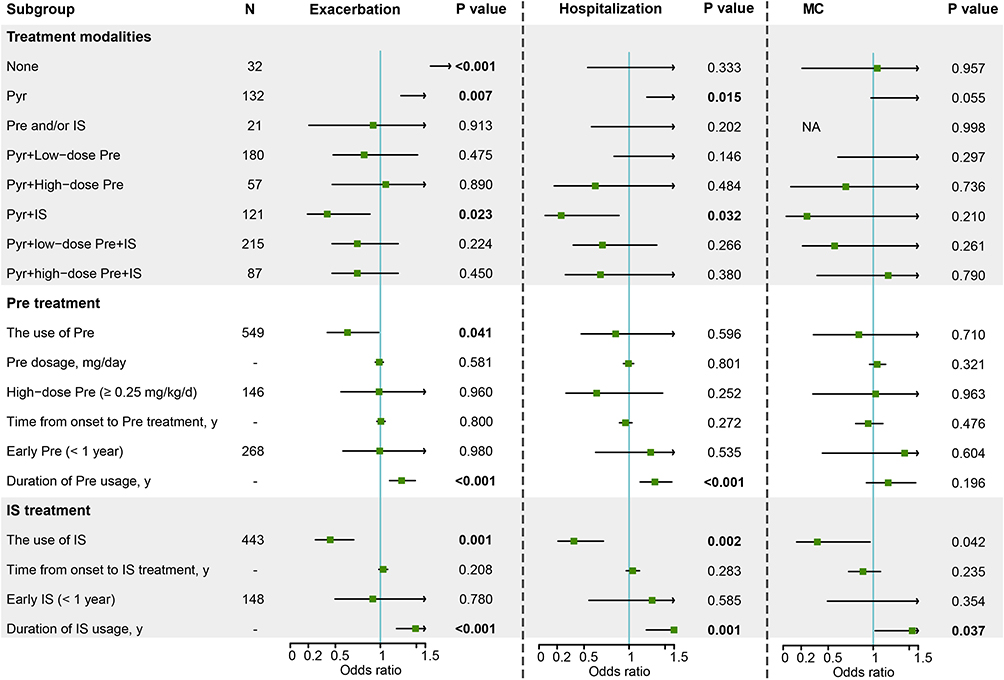 |
Figure 2 Adjusted odds ratio of therapeutic management for poor outcomes following COVID-19 infection in patients with MG. Notes: The likelihood ratio test was used for statistical analysis of possible risk factors in logistic regression. OR and 95% CI were adjusted for sex, age at onset, hypertension, diabetes, cardiovascular disease, cerebrovascular disease, chronic kidney disease, malignancy other than thymoma, symptoms at onset, MGFA classification, MGFA-PIS before COVID-19, anti-AChR and anti-MuSK-ab status. A p-value below 0.05 was considered statistically significant. Statistically significant results are bold. NA: Estimates are unreliable due to the small number of observations. |
Dysregulation of Inflammatory and Immune Response in MG Patients with COVID-19
A total of 376 MG patients with blood routine results available were divided into the uninfected group (n=273) and the infected group (n=103). It is important to note that this sample was different from the original sample as it consisted of older patients with more comorbidities (Supplementary Table S3). Compared with the uninfected group, most of the patients in the infected group tended to have higher leukocyte (7.4 vs 6.5 ×109, p = 0.001) and neutrophil (4.9 vs 3.8 ×109, p < 0.001) counts, higher neutrophil-to-lymphocyte ratio (NLR) (3.0 vs 2.1, p < 0.001), lower lymphocytes counts (1.5 vs 1.8 ×109, p < 0.001), as well as lower percentages eosinophils (0.6 vs 1.5%, p < 0.001) and basophils (0.2 vs 0.3%, p < 0.001) (Supplementary Table S4), which was further confirmed by logistic regression models (Table 3). Infection-related biomarkers and inflammatory cytokines were also elevated in infected patients than the uninfected ones, including hypersensitive C-reactive protein (hs-CRP) (3.0 vs 0.8 mg/mL, p < 0.001), procalcitonin (0.1 vs 0.05 ng/mL, p = 0.004), erythrocyte sedimentation rate (11.0 vs 6.0 mL/h, p = 0.006), interleukin (IL)-2β (434.0 vs 343.0 U/mL, p = 0.004), and IL-6 (3.6 vs 2.0 pg/mL, p = 0.003). Furthermore, immunoglobulin M decreased significantly in the infected patients compared to the uninfected patients (0.9 vs 1.1 g/L, p = 0.042). Among patients who underwent lymphocyte subsets test on admission, the total percentage of T cells, B cells, NK cells, and the percentage of regulatory T (Treg) cells (CD3+CD4+CD25+CD127low+) in the infected group were significantly lower than those in the uninfected group. Moreover, both naïve (CD45RA+ CD3+CD4+CD25+CD127low+) and induced Treg cells (CD45RO+ CD3+CD4+CD25+CD127low+) decreased significantly in the infected group compared with the uninfected group. In logistic regression models, inflammatory and immune markers, including hs-CRP (OR = 1.017, 95% CI 1.003–1.032, p = 0.020), IL-6 (OR = 1.148, 95% CI 1.046–1.259, p = 0.001), and the percentage of Treg cells (OR = 0.279, 95% CI 0.117–0.664, p = 0.004) were significantly associated with SARS-CoV-2 infection in patients with MG after adjusting for confounding factors.
 |
Table 3 Adjusted Odds Ratio and 95% Confidence Interval of Laboratory Factors for COVID-19 Infection |
Discussion
Previously many studies have focused on the therapeutic management of MG during the COVID-19 pandemic, however, the aggravating effects of COVID-19 on the disease course of MG have not been well addressed.10,13,24 This study aimed to identify patients at risk for poor outcomes (exacerbation, hospitalization, and MC) during COVID-19 through analysis of the large cohort of 845 MG patients with COVID-19. In previous observational studies,7,10,11 COVID-19 was noted to be more benign in the majority of MG patients, and a possible reason for the more benign course in the majority of MG patients is that the MG symptoms of most MG patients at the time of SARS-CoV-2 infection are well controlled. Our results indicated that nearly 18.1% of MG patients with COVID-19 experienced disease exacerbations, slightly higher than the 10–15% reported in the previous literature.9–11 We also revealed that patients achieving MMS or better status were at a reduced risk for poor outcomes than those who did not. In addition, disease severity at onset was identified as an important predictive factor for poor outcomes in our cohort. Based on our observations, treatment strategies should be tailored to the disease status and severity of initial symptoms potentially reducing the likelihood for poor outcomes.
Our data showed that fever and cough were the most common presenting symptoms in patients with MG following SARS-CoV-2 infection, similar to those reported in non-myasthenic patients.8,16,25 Furthermore, the symptoms of COVID‐19 did not dramatically influence the MG course in our cohort. Meanwhile, available data implicate that there is no association between COVID-19 severity and risk of MG worsening, as even mild or subclinical COVID-19 cases may trigger exacerbation of MG.6,26 Data regarding the effect and safety of COVID-19 vaccines in the context of MG is debated.6,27,28 Many studies indicated vaccines against SARS-CoV-2 showed good short-term safety and could prevent severe COVID-19 in vulnerable patients.27,28 Our results indicated a relatively low vaccination coverage rate of 69.7%, which might contribute to an increase in the occurrence of poor outcomes in MG patients following COVID-19. In addition, patients with MC in our cohort had a lower vaccination rate than those without (50.0% vs 70.5%, χ2 test, P = 0.026), which was similar to the study by Lupica A et al, suggesting that MC was more common in unvaccinated patients.28 We also aimed to assess the effect of pre-COVID-19 vaccination status on poor outcomes of MG disease following SARS-CoV-2 infection. However, we did not find a significant association between COVID-19 vaccination status and poor outcomes, which required further validation in prospective cohort studies. More importantly, we identified anti-AChR-ab positivity as an independent risk factor for poor outcomes of disease exacerbation, which was consistent with previous studies.19,29 This can be interpreted as the possibility that antibodies against the SARS-CoV-2 protein may cross-react with AChR subunits due to epitope homology.30
It has been reported that COVID-19 is more likely to influence the disease course in the elderly and those with underlying comorbidities and immunologic deficiencies.16,31 Corroborating previous studies,10 age at onset was identified as a easily accessible and reliable predictor for poor outcomes of disease exacerbation and hospitalization following COVID-19. Of all comorbidities observed in our cohort, the comorbidities renal and oncologic were identified to be the risk factors for poor outcomes in MG patients with COVID-19, suggesting that more severe immune dysregulation and prolonged inflammation in this fragile subgroup of patients.5,25 Similar findings have also been published in non-myasthenic patients.25 A recent study by Di Stefano et al suggested that respiratory disorders and thymoma were more common in MG patients with more severe disease.32 These results suggest that comorbidities may be associated with the worsening course of MG, regardless of the presence or absence of COVID-19. Therefore, myasthenic patients with more comorbidities should receive intensified disease monitoring to recognize and prevent the occurrence of poor outcomes.
Currently, the role of immunosuppressive therapy on the course of MG disease during the COVID-19 pandemic remains controversial.9 Some reports have suggested that immunotherapy may exert a protective effect in MG patients by reducing the dramatic upregulation of inflammatory cytokines during COVID-19,8,10 while others suggested that corticosteroid treatment before the diagnosis of COVID-19 or during COVID-19 was associated with a higher risk of mortality in MG patients.33 Our data revealed that the use of prednisone or immunosuppressants before COVID-19 was effective in reducing the occurrence of disease exacerbation in MG during COVID‐19 infection, while the prednisone dosage displayed no association with the outcomes. It is important to note that while prednisone may be safe and effective in the beginning, it should be tapered off in combination with immunosuppressants during long-term follow-up to avoid adverse reactions.1,17,21 In line with Jakubíková et al,5 we found the duration of prednisone or immunosuppressant usage was associated with a higher risk of poor outcomes, which might be related to the immune instability of these patients requiring maintenance of immunotherapy. Taken together, we do not recommend reducing or even discontinuing these immunosuppressive agents in MG patients well-controlled by short-term immunotherapy.
Infections have been documented to stimulate the immune system, potentially triggering autoimmune responses or exacerbating the course of MG.34 For example, Epstein-Barr virus has the capacity to promote abnormal activation and survival of B-lymphocytes to induce MG disease.35 With the emergence of COVID-19, the relationship between infections and MG has gained renewed attention. In this study, a significantly elevated neutrophil count and decreased lymphocyte count (ie the increase of NLR) were found in the infected group compared to the uninfected group. Furthermore, MG patients with COVID-19 had a significantly higher level of serum IL-6 than those without. These findings have been similarly observed in the general population infected with COVID-19.16,36,37 It is worth noting that pro-inflammatory cytokine IL-6 might also play an important role in the pathophysiology of MG.38 In addition, T lymphocyte damage is involved in the pathological process of COVID-19.16,37 In our cohort, although the number of peripheral blood CD3+CD4+ T lymphocytes in infected patients tended to be lower than that in uninfected patients, the difference did not reach statistical significance (P = 0.076). More importantly, we noted a significantly lower percentage of Treg cells (including naïve and induced Treg cells) in MG patients with COVID-19 than those without. It is well-known that Treg plays an important role maintenance of self-tolerance and immune homeostasis, and Treg deficiency is involved in the development of MG.3 Overall, these findings suggest that infections may regulate lymphocytes and their cytokine signaling to induce pro-inflammatory and dysregulated immune responses, thereby mediating the pathological process of MG disease.24,34 Further researches are essential to deepen our understanding of how various infections, including but not limited to COVID-19, affect the course of MG.
There were several limitations to our study that should be acknowledged. Firstly, the study was limited to a single-center and retrospective design. Nevertheless, our cohort represents one of the largest case series of MG patients with COVID-19 and provides interesting results. Second, although accurate and objective information was obtained through interviews with professional neurologists, the effect of COVID-19 on the course of MG patients may be exaggerated because some asymptomatic or mild cases may not attend hospitals. Third, given the difficulty in distinguishing between the effects of the infection and the MG worsening in severely ill patients with respiratory failure,24,39 it is more likely in these cases that the predictors of MC will be used to predict a life-threatening condition requiring intensive care and respiratory support in MG patients with COVID-19. Finally, co-infection with bacteria or superinfection might potentially affect the results of the immune response in MG patients with COVID-19, a larger cohort would be better to assess the temporal change in immune response after SARS-CoV-2 infection.
Conclusion
In conclusion, our study suggests COVID-19 did not dramatically influence the course of MG disease in the majority of patients with MG, especially in those with few comorbidities, ocular MG at onset, and satisfactory control of MG before infection. MC was more frequent among unvaccinated patients with MG. However, being unvaccinated was not significantly associated with poor outcomes after adjusting for confounding factors. Myasthenic patients should continue their immunosuppressive therapy in the current pandemic. SARS-CoV-2 may mediate inflammatory and immune responses in MG patients, particularly in regulating the levels of interleukin-6 and Treg cells.
Abbreviations
anti-AChR-ab, anti-acetylcholine receptor antibody; anti-LRP4-ab, anti-lipoprotein-related protein 4 antibody; anti-MuSK-ab, anti-muscle-specific kinase-ab; CI, confidence intervals; COVID-19, Coronavirus Disease 2019; ESR, Erythrocyte sedimentation rate; hs-CRP, hypersensitive C-reactive protein; IL, interleukin; IQR, interquartile range; LDH, lactate dehydrogenase; MC, myasthenic crisis; MG, myasthenia gravis; MGFA, myasthenia gravis foundation of America classification; MMS, minimal manifestation status; NK, natural killer; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratios; PCT, procalcitonin; PIS, postintervention status; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; Treg, regulatory T.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Committee of Clinical Investigation at Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan China (NO. TJ-IRB202404125), and the protocol was conducted in accordance with the Declaration of Helsinki. A waiver of informed consent was granted by the ethics committees due to a retrospective design of deidentified data and a minimal risk involved. The data presented in this study do not allow for the identification of individuals. We are committed to ensuring the privacy and confidentiality of the subjects, or their anonymity, throughout the entire research process.
Acknowledgments
The authors cordially thank the participants and their families, as well as the support from Hangzhou Zhongmei Huadong Pharmaceutical Co., Ltd.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gilhus NE, Verschuuren JJ. Myasthenia gravis: Subgroup classification and therapeutic strategies. Lancet Neurol. 2015;14(10):1023–1036. doi:10.1016/S1474-4422(15)00145-3
2. Mao ZF, Mo XA, Qin C, Lai YR, Olde Hartman TC. Course and prognosis of myasthenia gravis: A systematic review. Eur J Neurol. 2010;17(7):913–921.
3. Bi Z, Zhan J, Zhang Q, et al. Clinical and immune-related factors associated with exacerbation in adults with well-controlled generalized myasthenia gravis. Front Immunol. 2023;14:1177249. doi:10.3389/fimmu.2023.1177249
4. Gummi RR, Kukulka NA, Deroche CB, Govindarajan R. Factors associated with acute exacerbations of myasthenia gravis. Muscle Nerve. 2019;60(6):693–699. doi:10.1002/mus.26689
5. Jakubíková M, Týblová M, Tesař A, et al. Predictive factors for a severe course of COVID-19 infection in myasthenia gravis patients with an overall impact on myasthenic outcome status and survival. Eur J Neurol. 2021;28(10):3418–3425. doi:10.1111/ene.14951
6. Sansone G, Bonifati DM. Vaccines and myasthenia gravis: A comprehensive review and retrospective study of SARS-CoV-2 vaccination in a large cohort of myasthenic patients. J Neurol. 2022;269(8):3965–3981. doi:10.1007/s00415-022-11140-9
7. Gungor Tuncer O, Deymeer F. Clinical course and outcome of an outpatient clinic population with myasthenia gravis and COVID-19. Muscle Nerve. 2022;65(4):447–452. doi:10.1002/mus.27497
8. Emmi G, Bettiol A, Mattioli I, et al. SARS-CoV-2 infection among patients with systemic autoimmune diseases. Autoimmun Rev. 2020;19(7):102575. doi:10.1016/j.autrev.2020.102575
9. Morawiec N, Adamczyk B, Adamczyk-Sowa M. COVID-19 and autoimmune diseases of the nervous system - an update. Neurol Neurochir Pol. 2023;57(1):77–89. doi:10.5603/PJNNS.a2023.0008
10. Businaro P, Vaghi G, Marchioni E, et al. COVID-19 in patients with myasthenia gravis: Epidemiology and disease course. Muscle Nerve. 2021;64(2):206–211. doi:10.1002/mus.27324
11. Rodrigues CL, de Freitas HC, Lima PRO, et al. Myasthenia gravis exacerbation and myasthenic crisis associated with COVID-19: Case series and literature review. Neurol Sci. 2022;43(4):2271–2276. doi:10.1007/s10072-021-05823-w
12. Singh S, Govindarajan R. COVID-19 and generalized Myasthenia Gravis exacerbation: A case report. Clin Neurol Neurosurg. 2020;196:106045. doi:10.1016/j.clineuro.2020.106045
13. Jacob S, Muppidi S. International MG/COVID-19 Working Group, Guidance for the management of myasthenia gravis (MG) and Lambert-Eaton myasthenic syndrome (LEMS) during the COVID-19 pandemic. J Neurol Sci. 412;2020:116803. doi:10.1016/j.jns.2020.116803
14. Costamagna G, Abati E, Bresolin N, Comi GP, Corti S. Management of patients with neuromuscular disorders at the time of the SARS-CoV-2 pandemic. J Neurol. 2021;268(5):1580–1591. doi:10.1007/s00415-020-10149-2
15. Bi Z, Cao Y, Liu C, et al. Remission and relapses of myasthenia gravis on long-term tacrolimus: A retrospective cross-sectional study of a Chinese cohort. Ther Adv Chronic Dis. 2022;13:20406223221122538. doi:10.1177/20406223221122538
16. Qin C, Zhou L, Hu Z, et al. Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clin Infect Dis. 2020;71(15):762–768. doi:10.1093/cid/ciaa248
17. Sanders DB, Wolfe GI, Benatar M, et al. International consensus guidance for management of myasthenia gravis: Executive summary. Neurology. 2016;87(4):419–425. doi:10.1212/WNL.0000000000002790
18. Verwijst J, Westerberg E, Punga AR. Cancer in myasthenia gravis subtypes in relation to immunosuppressive treatment and acetylcholine receptor antibodies: A Swedish nationwide register study. Eur J Neurol. 2021;28(5):1706–1715. doi:10.1111/ene.14730
19. Nelke C, Stascheit F, Eckert C, et al. Independent risk factors for myasthenic crisis and disease exacerbation in a retrospective cohort of myasthenia gravis patients. J Neuroinflammation. 2022;19(1):89. doi:10.1186/s12974-022-02448-4
20. Jaretzki A 3rd, Barohn RJ, Ernstoff RM, et al. Myasthenia gravis: recommendations for clinical research standards. task force of the medical scientific advisory board of the myasthenia gravis foundation of America task force of the medical scientific advisory board of the myasthenia gravis foundation of America. Neurology. 2000;55(1):16–23. doi:10.1212/wnl.55.1.16
21. Zhang C, Bu B, Yang H, et al. Immunotherapy choice and maintenance for generalized myasthenia gravis in China. CNS Neurosci Ther. 2020;26(12):1241–1254. doi:10.1111/cns.13468
22. Cheng WJ, Shih HM, Su KP, Hsueh PR. Risk factors for poor COVID-19 outcomes in patients with psychiatric disorders. Brain Behav Immun. 2023;114:255–261. doi:10.1016/j.bbi.2023.08.024
23. Rzepiński Ł, Zawadka-Kunikowska M. COVID-19 pandemic year in a sample of Polish myasthenia gravis patients: An observational study. Neurol Neurochir Pol. 2022;56(1):61–67. doi:10.5603/PJNNS.a2021.0054
24. Delly F, Syed MJ, Lisak RP, Zutshi D. Myasthenic crisis in COVID-19. J Neurol Sci. 2020;414:116888. doi:10.1016/j.jns.2020.116888
25. Guan WJ, Liang WH, Zhao Y, et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur Respir J. 2020;55(5):2000547. doi:10.1183/13993003.00547-2020
26. Finsterer J, Scorza FA. Perspectives of Neuro-COVID: Myasthenia. Front Neurol. 2021;12:635747. doi:10.3389/fneur.2021.635747
27. Farina A, Falso S, Cornacchini S, et al. Safety and tolerability of SARS-Cov-2 vaccination in patients with myasthenia gravis: A multicenter experience. Eur. J Neurol. 2022;29(8):2505–2510.
28. Lupica A, Di Stefano V, Iacono S, et al. Impact of COVID-19 in AChR myasthenia gravis and the safety of vaccines: Data from an Italian cohort. Neurol Int. 2022;14(2):406–416. doi:10.3390/neurolint14020033
29. König N, Stetefeld HR, Dohmen C, et al. MuSK-antibodies are associated with worse outcome in myasthenic crisis requiring mechanical ventilation. J Neurol. 2021;268(12):4824–4833. doi:10.1007/s00415-021-10603-9
30. Restivo DA, Centonze D, Alesina A, Marchese-Ragona R. Myasthenia gravis associated with SARS-CoV-2 infection. Ann Intern Med. 2020;173(12):1027–1028. doi:10.7326/L20-0845
31. Singhal T. A review of coronavirus disease-2019 (COVID-19). Indian J Pediatr. 2020;87(4):281–286. doi:10.1007/s12098-020-03263-6
32. Di Stefano V, Iacono S, Militello M, et al. Comorbidity in myasthenia gravis: Multicentric, hospital-based, and controlled study of 178 Italian patients. Neurol Sci. 2024;45(7):3481–3494. doi:10.1007/s10072-024-07368-0
33. Abbas AS, Hardy N, Ghozy S, et al. Characteristics, treatment, and outcomes of myasthenia gravis in COVID-19 patients: A systematic review. Clin Neurol Neurosurg. 2022;213:107140. doi:10.1016/j.clineuro.2022.107140
34. Gilhus NE, Romi F, Hong Y, Skeie GO. Myasthenia gravis and infectious disease. J Neurol. 2018;265(6):1251–1258. doi:10.1007/s00415-018-8751-9
35. Morandi E, Jagessar SA, ‘t Hart BA, Gran B. EBV infection empowers human b cells for autoimmunity: Role of autophagy and relevance to multiple sclerosis. J Immunol. 2017;199(2):435–448. doi:10.4049/jimmunol.1700178
36. Di Spigna G, Spalletti Cernia D, Covelli B, et al. Interleukin-6 and its soluble receptor complex in intensive care unit covid-19 patients: an analysis of second wave patients. Pathogens. 2023;12(10):1264. doi:10.3390/pathogens12101264
37. Liu J, Li S, Liu J, et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine. 2020;55:102763. doi:10.1016/j.ebiom.2020.102763
38. Sassano P, Paparo F, Ramieri V, Colangeli W, Verdino G. Interleukine-6 (IL-6) may be a link between myasthenia gravis and myoepithelioma of the parotid gland. Med Hypotheses. 2007;68(2):314–317. doi:10.1016/j.mehy.2006.06.057
39. Finsterer J, Scorza FA, Scorza CA. Diagnosing myasthenic crisis in SARS-CoV-2 infected patients requires adherence to appropriate criteria. J Neurol Sci. 2020;417:117062. doi:10.1016/j.jns.2020.117062
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.