")
Back to Journals » Journal of Inflammation Research » Volume 17
Predictive Value of SYN-1 Levels for Mortality in Sepsis Patients in the Emergency Department
Authors Hu L, Wang J, Zhang Y, Wang J, Wei B
Received 7 May 2024
Accepted for publication 14 September 2024
Published 26 November 2024 Volume 2024:17 Pages 9837—9846
DOI https://doi.org/10.2147/JIR.S468763
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Adam Bachstetter
Le Hu,1– 3 Jia Wang,1– 3 Ye Zhang,1– 3 Junyu Wang,1– 3 Bing Wei1– 3
1Emergency Medical Center, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Beijing Key Laboratory of Cardiopulmonary Cerebral Resuscitation, Beijing, People’s Republic of China; 3Clinical Center for Medicine in Acute Infection, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Bing Wei; Junyu Wang, Email [email protected]; [email protected]
Objective: To evaluate and predict adverse outcomes associated with serum Syndecan-1 (SYN-1) levels in patients with early sepsis, and to explore the prognostic risk factors in sepsis and septic shock.
Methods: This retrospective single-center observational study included 168 sepsis patients admitted to the Emergency Department of Beijing Chao-Yang Hospital Shijingshan Branch, Capital Medical University, from October 2020 to October 2021. Patients were categorized into sepsis (n=114) and septic shock (n=54) groups based on Sepsis 3.0 criteria. They were further divided into survival (n=128) and death (n=40) groups. Comparative analyses included general demographics and laboratory findings (SYN-1, lactic acid [LAC], procalcitonin [PCT], C-reactive protein [CRP]) within 3 hours of admission, as well as Acute Physiology and Chronic Health Evaluation II (APACHE II) and Sequential Organ Failure Assessment (SOFA) scores. Statistical methods included receiver operating characteristic (ROC) curve analysis, correlation analysis, and logistic regression.
Results: Serum SYN-1 levels were significantly higher in the septic shock group (138.89± 9.26) compared to the sepsis group (102.89± 8.97) (P < 0.05). SYN-1 levels were also significantly higher in the death group (150.19± 7.65) compared to the survival group (103.301± 86.59) (P < 0.05). The area under the ROC curves for SYN-1, LAC, and APACHE II scores in predicting 28-day mortality were 0.668, 0.641, and 0.666, respectively. SYN-1 showed a positive correlation with SOFA scores (correlation coefficient=0.228). SYN-1, APACHE II score, and LAC were identified as independent risk factors for 28-day mortality in sepsis patients.
Conclusion: SYN-1 demonstrates high sensitivity and specificity in early prediction of poor outcomes in sepsis patients. SYN-1, APACHE II score, and LAC serve as independent risk factors for 28-day mortality in sepsis patients.
Keywords: Syndecan-1, sepsis, septic shock
Background
Sepsis is characterized by a systemic inflammatory response syndrome that can lead to severe outcomes including multiple organ failure and shock.1 Due to its rapid progression, severity, and high mortality rate, it is of utmost concern to clinicians. Early identification of sepsis severity and prognosis through effective detection methods is crucial for reducing mortality rates.2
Various severity scoring systems have been studied extensively in critically ill patients, such as the Acute Physiological and Chronic Health Evaluation II (APACHE II) score,3 Glasgow Coma Scale (GCS),4 and the Sequential Organ Failure Assessment (SOFA) score.5 However, the diverse etiologies of sepsis necessitate the exploration of novel biomarkers for assessing and stratifying patients at high risk. This research is essential for clinicians to facilitate precise treatment, prioritize surveillance efforts, and allocate resources effectively.
Increasingly, biomarkers such as Syndecan-1 (SYN-1) are being utilized as early adjuncts in clinical settings. SYN-1 is a transmembrane proteoglycan cell adhesion molecule and a key member of the heparan sulfate proteoglycan family. It plays pivotal roles in various pathophysiological processes, including cell morphology maintenance, tissue repair promotion, immune function regulation, and host defense.6 Notably, SYN-1 is crucial for stabilizing the intestinal epithelial barrier, serving as a vital protective mechanism.7
This study focuses on assessing SYN-1 levels in sepsis patients to determine its clinical significance in predicting severity and 28-day mortality.
Materials and Methods
Study Design
This retrospective single-center observational study focused on critically ill patients admitted to the emergency department of Beijing Chao-Yang Hospital Shijingshan Branch between October 2020 and October 2021. A total of 215 patients were enrolled, with 168 patients included in the study. Due to the family’s decision for palliative care, 47 patients were subsequently excluded from the study, with data collected on age, sex, vital signs, and comorbidities. Based on Sepsis 3.0 criteria, patients were categorized into the sepsis group (n=114) and septic shock group (n=54). The study received ethical approval from the Ethics Committee of Beijing Chaoyang Hospital (Approval number: 2021-ke-636), and informed consent was obtained from all participants. The study design process is depicted in the flowchart. (Figure 1)
 |
Figure 1 The flowchart of the study. |
Inclusion and Exclusion Criteria
Inclusion criteria: 1. Patients meeting the diagnostic criteria of the International Conference on Sepsis and Septic Shock (SEPSIS 3.0).5 2. Adult patients (≥18 years old). 3. Availability of blood routine, PCT, CRP, LAC, and other test results within 24 hours of admission.
Exclusion criteria: 1. Patients with advanced tumors. 2. Patients receiving chemotherapy, glucocorticoids, and/or immunosuppressant therapy. 3. Patients who discontinued treatment or were automatically discharged due to financial constraints or other factors.
Methods
All 168 patients underwent comprehensive laboratory testing within 3 hours of admission, including SYN-1, blood urea nitrogen (BUN), procalcitonin (PCT), homocysteine, platelet count (PLT), aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (TBIL), and C-reactive protein (CRP) levels. SYN-1 was measured using Human Syndecan-1 ELISA Kit (CD138) (Abcam Inc. Ab46506) via the colorimetric method. Additionally, GCS evaluations,8,9 APACHE II scores,3 and SOFA scores5 were completed within 24 hours of admission. Patient survival status was monitored up to 28 days. Laboratory test results were compared between the sepsis and septic shock groups, and risk factors influencing 28-day mortality were analyzed based on these findings.
Statistical Analyses
Data were analyzed using SPSS 26.0 software. Categorical variables were presented as frequencies and percentages, and compared using the Chi-square test. Normally distributed continuous variables were expressed as mean ± standard deviation and compared using the independent samples t -test. Non-normally distributed variables were presented as median (interquartile range). Pearson correlation analysis, area under the receiver operating characteristic curve (AUC-ROC), and logistic regression models were employed for statistical analyses. A significance level of α=0.05 was used, with P<0.05 considered statistically significant.
Results
Demographic and Clinical Characteristics of Included Patients
A total of 168 patients were enrolled in this study, comprising 114 patients with sepsis and 54 patients with septic shock. Among these, 40 patients died during hospitalization, resulting in 128 cases in the survival group and 40 cases in the death group. In a cohort of 168 enrolled patients, 32 cases were admitted to the Intensive Care Unit (ICU), with an admission rate of 19%. There were 54 cases of septic shock, accounting for 32% of the total. Thirty-seven patients required vasoactive medication, representing 22% of the cohort. Twenty-nine patients needed non-invasive ventilation, which is 17% of the total. Fifteen patients underwent invasive mechanical ventilation therapy, constituting 8% of the enrolled patients. Among the 168 enrolled patients, 35 cases had comorbid cardiovascular diseases, which is 20% of the total. Ninety-six patients had comorbid respiratory system diseases, such as pneumonia and chronic obstructive pulmonary disease (COPD), accounting for 57% of the total. Thirty-nine patients had comorbid type 2 diabetes, which is 23% of the total. Thirty-one patients had comorbid cerebrovascular diseases (cerebral hemorrhage and cerebral infarction), making up 18% of the total. The study analyzed patient age, laboratory test results, disease severity scores including APACHE II, GCS, and SOFA scores, as detailed in Table 1.
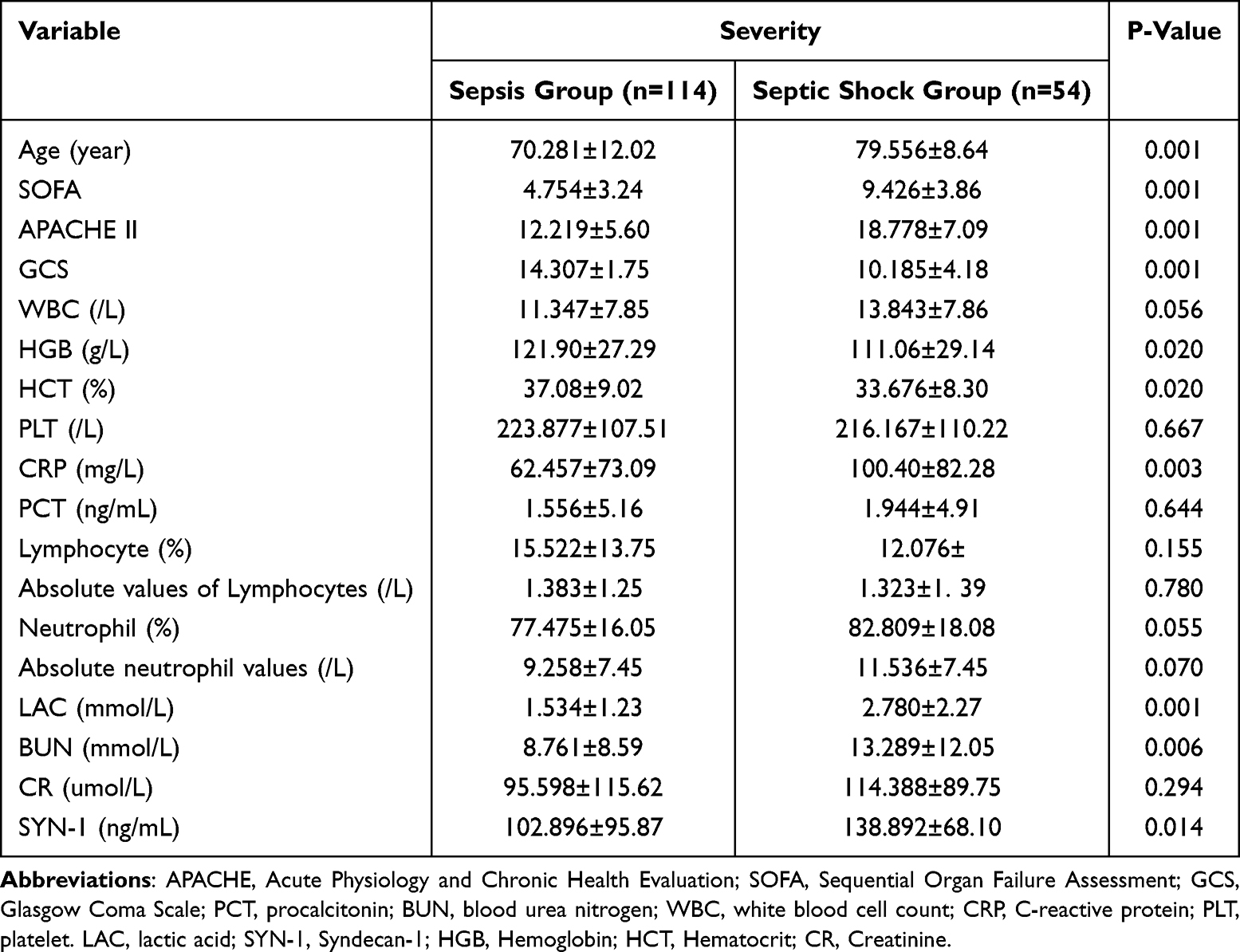 |
Table 1 Comparison of General Data, Laboratory Test Indicators and Related Scores of Patients with Sepsis and Septic Shock |
Comparison of SYN-1 Index: Elevated Levels in Septic Shock Group Over Sepsis Group
The SYN-1 levels were significantly higher in the septic shock group compared to the sepsis group. Specifically, SYN-1 levels were 138.892±68.10 ng/mL in the septic shock group and 102.896±95.87 ng/mL in the sepsis group (P=0.014). Other indicators such as CRP (P=0.003), LAC (P=0.001), BUN (P=0.006), APACHE II (P=0.001), and SOFA (P=0.001) scores were significantly lower in the sepsis group compared to the septic shock group, indicating statistical significance (P<0.05). The GCS score was higher in the sepsis group compared to the septic shock group, also showing statistical significance (P<0.05), as shown in Table 1.
Higher SYN-1 Index Observed in the Death Group Compared to the Survival Group
The results indicated that the SYN-1 levels in the death group (150.194±89.54 ng/mL) was markedly higher than that in the survival group (103.301±86.59 ng/mL) (P=0.003), demonstrating a statistically significant difference (P<0.05). Analysis of other indicators revealed that CRP (P=0.003), LAC (P=0.001), BUN (P=0.001), APACHE II (P=0.001), and SOFA (P=0.001) scores were lower in the sepsis group compared to the septic shock group, with statistically significant differences (P<0.05). Additionally, the GCS score was higher in the sepsis group compared to the septic shock group, showing statistical significance (P<0.05), as depicted in Table 2.
 |
Table 2 Comparison of General Information, Laboratory Test Indicators and Relevant Scores Between Surviving and Death Groups |
Further Analysis of Its Potential to Predict 28-Day Prognosis and Mortality
Following identification of these relevant factors, their potential to predict prognosis and mortality at 28 days was further examined. Logistic regression analysis was conducted on the identified correlating factors. The results indicated that SYN-1(OR =1.004, P=0.041, 95% CI: 0.576–0.761), LAC (OR=1.390, P=0.003, 95% CI: 0.536–0.745), and APACHE II score (OR=1.085, P=0.005, 95% CI: 0.565–0.767) were independent risk factors for mortality at 28 days, as shown in Table 3.
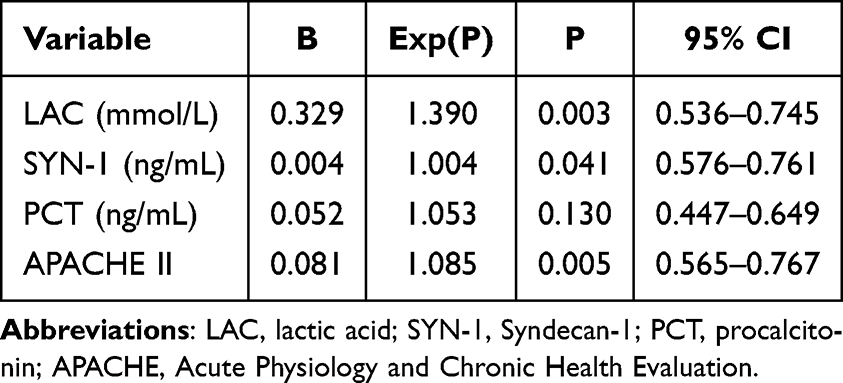 |
Table 3 Logistic Regression Analysis of Risk Factors Affecting the 28-Day Mortality of Sepsis Patients |
ROC Curve Analysis for Predicting 28-Day Mortality in Sepsis Patients Using Various Indices
The ROC curve was utilized to assess the predictive efficacy of each index for 28-day mortality in sepsis patients. SYN-1, APACHE II, LAC, and their combinations were evaluated through ROC curve analysis in the study cohort. All identified indicators and their combinations demonstrated effectiveness in predicting 28-day mortality. The area under the ROC curve for SYN-1 was 0.668, with a sensitivity of 80% and specificity of 57.8%. For LAC and APACHE II, the areas under the ROC curves were 0.641 and 0.666, respectively (Figure 2). ROC curve pairwise comparisons are depicted in Table 4. Notably, LAC exhibited a specificity of 99.2% and sensitivity of 37.5%, while APACHE II showed a sensitivity of 72.5% and specificity of 64.1%. The combined AUCs for SYN-1 + APACHE II and LAC + APACHE II in predicting 28-day mortality in sepsis patients were 0.726 and 0.748, respectively, as detailed in Table 5.
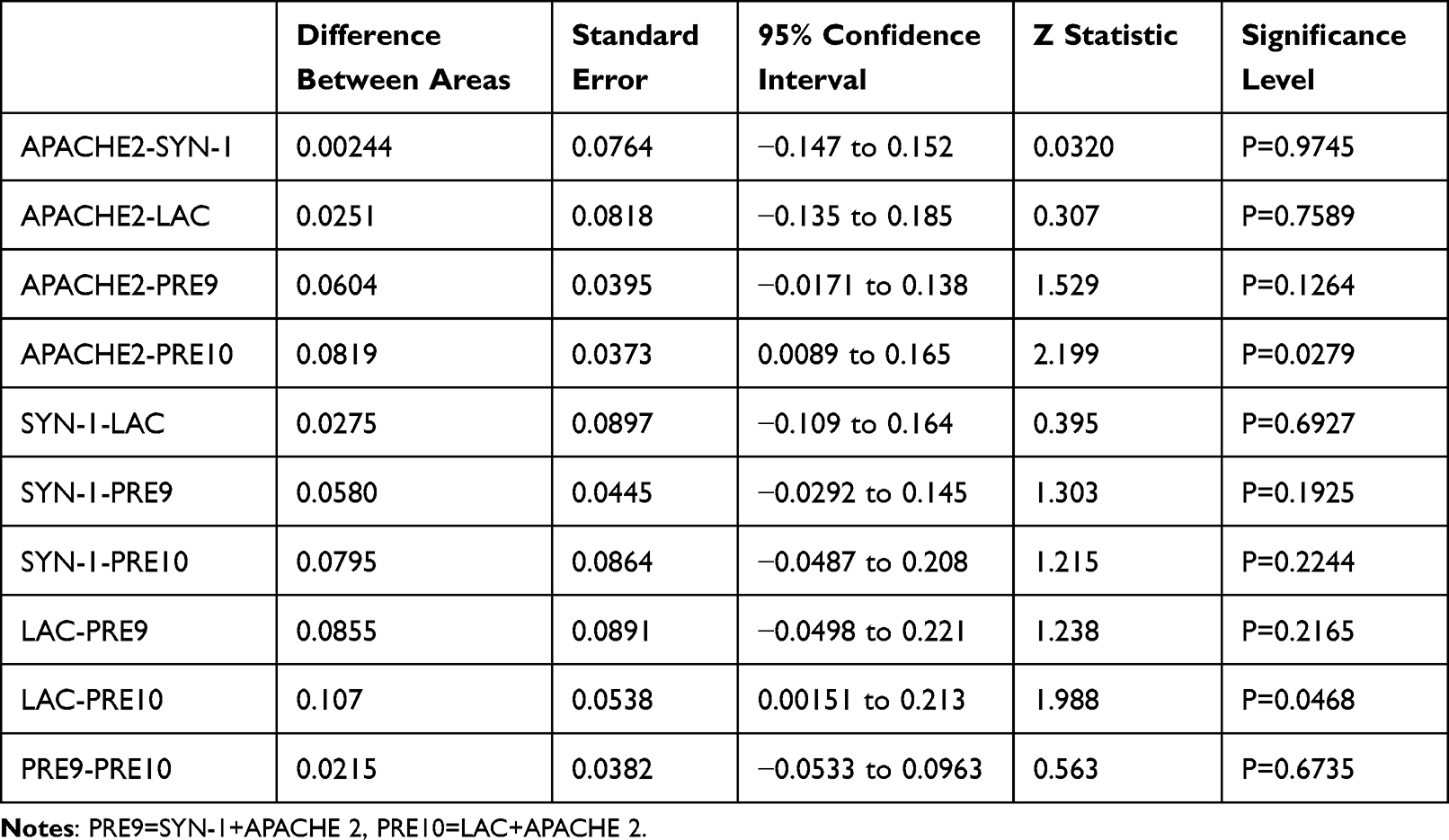 |
Table 4 Pairwise Comparison of ROC Curves |
 |
Table 5 ROC Curve Analysis and Comparison of the Predictive Ability of 28d Mortality in Sepsis Patients |
 |
Figure 2 ROC curve of 28-day mortality predicted by various inflammatory indicators. |
Correlation Analysis Between SYN-1 and Various Markers
Correlation analysis revealed that SYN-1 was positively correlated with SOFA (r=0.228), CRP (r=0.215), and PCT (r=0.214) (P < 0.01), although the correlations were moderate. Conversely, SYN-1 showed a low correlation with LAC (r=0.114), as presented in Table 6.
 |
Table 6 Pearson Correlation Analysis of SYN-1 and Various Markers |
Discussion
In this study, we investigated a novel serum model to predict 28-day mortality in sepsis. Key findings include:1 Elevated SYN-1 levels strongly correlated with sepsis severity and 28-day mortality.2 SYN-1 emerges as a reliable predictor of 28-day mortality in sepsis patients, comparable to established scoring systems like SOFA, APACHE II, and LAC.3 The high sensitivity of SYN-1 levels compensates for limitations observed in traditional scoring systems such as SOFA, APACHE II, and LAC.
Despite the widespread use of severity scoring systems in clinical practice to stratify and predict outcomes in critically ill patients (eg, APACHE II, SOFA), their ability to universally meet patient needs is limited due to the complex nature of critical illness. Emergency room patients often present with diverse comorbidities and complex medication regimens, further complicating accurate score prediction. While traditional systems may be effective for some patients, their efficacy varies. This study highlights SYN-1 as a promising serum biomarker for individual prognosis, demonstrating significant potential for clinical application in predicting outcomes like septic shock and 28-day mortality.
Sepsis is a syndrome triggered by the body’s dysregulated response to infection, presenting a significant threat to human health and life, especially in cases of septic shock, which carry a high mortality rate.10 The formal definition of sepsis began at the Consensus Meeting on Sepsis in 1991 and evolved with evidence-based medicine culminating in Sepsis 3.0, reintroduced at the 45th Annual Meeting of Critical Care Medicine in 2016. Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated response to infection, while septic shock is characterized by the need for vasopressors to maintain a mean arterial pressure ≥60mmHg despite adequate fluid resuscitation, along with a serum lactate concentration ≥2mmol/L. Sepsis 3.0 focuses on the dysregulation of the body’s response to infection and organ dysfunction, reflecting cellular-level physiological and pathological changes.11
SYNDECAN-S is a transmembrane heparan sulfate proteoglycan, a crucial class of membrane-anchored proteoglycans (HSPGs). As part of the extracellular matrix (ECM), Syndecan-S contributes to basement membrane formation and regulates cell adhesion. It plays diverse roles in physiological and pathological processes, including tissue and organ differentiation, angiogenesis, tissue regeneration, and host defense.12
SYN-1, a larger member of its family, is predominantly expressed in leukocytes and epithelial cells, playing a crucial role in maintaining normal epithelial cell morphology and structure.13,14 Heparan sulfate proteoglycans, which bind various inflammatory mediators on cell surfaces, have been demonstrated to modulate and regulate inflammatory responses in numerous animal models.15–17 SYN-1 exists in two forms upon shedding, with its soluble form, particularly the exon structure and membrane-bound separation, being stimulated in various extracellular environments (eg, bacterial toxins, growth factors, chemokines). This shedding of SYN-1 has been shown to intensify inflammatory responses, with elevated levels correlating with the severity of sepsis, making SYN-1 a potential biomarker for sepsis.18
Increased vascular permeability is a hallmark of sepsis and septic shock. Damage to vascular endothelial glycocalyx integrity leads to endothelial dysfunction and compromised barrier function, resulting in heightened vessel permeability. This leads to substantial fluid loss from circulation, tissue edema formation, reduced plasma colloid osmotic pressure, inadequate effective circulating blood volume, and ultimately exacerbates tissue hypoperfusion.19
The glycocalyx (GCX) is a critical component of endothelial cell barrier structure, including carbohydrate-rich proteoglycans and glycoproteins.20 The GCX is highly susceptible to ischemic and hypoxic damage, with its degradation often a primary factor in endothelial dysfunction and a major contributor to increased vascular permeability.21,22
In the presence of infection and inflammation, increased expression and activity of hyaluronidase can degrade the GCX, causing further damage and release of its components (proteoglycans and their glycosaminoglycan complexes).
The core protein of proteoglycans (PGs) contains a significant amount of SYN-1.23 During sepsis, the GCX scaffold undergoes extensive degradation, leading to a notable increase in SYN-1, a marker associated with the shedding of polysaccharide-coated structures, in blood concentration24. Plasma concentrations of polysaccharide degradation products correlate closely with the severity of septic shock.
Several studies have identified hypoalbuminemia as a crucial predictor of poor prognosis in sepsis patients.25–27 This phenomenon is typically attributed to abnormal capillary permeability in sepsis, causing extravascular protein redistribution.28–31 However, considering that interstitial protein levels are normally around 70% of serum albumin levels and the extravascular space is typically saturated, other loss pathways are believed to contribute.32
Studies have demonstrated increased SYN-1 shedding from intestinal epithelial cells in sepsis patients, impacting intercellular adhesion, compromising intestinal mucosal barrier function, and elevating intestinal permeability, thereby promoting excessive albumin loss through the intestine.16,30–34 SYN-1 plays a crucial role in maintaining intestinal epithelial cell stability and mucosal barrier function. The SYN-1-induced loss of intestinal protein represents another significant pathway leading to sepsis-related hypoalbuminemia, warranting careful consideration. We believe SYN-1’s prognostic value lies in its ability to rapidly indicate the extent of endothelial damage, crucial for early sepsis intervention. Our future research aims to explore SYN-1 in combination with other biomarkers to enhance prognostic accuracy. Furthermore, SYN-1 offers unique insights into sepsis pathophysiology, potentially complementing existing predictive models. Our decision to investigate SYN-1 is part of a broader initiative to develop a comprehensive biomarker panel that includes markers like LBP, L-FABP, and others, to refine sepsis outcome prediction.
While SYN-1 may currently be less accessible and costlier for bedside use, we are actively working to enhance the accessibility and cost-effectiveness of our biomarker panel. We envision integrating these biomarkers into a single point-of-care testing (POCT) device that offers clinicians a user-friendly tool for real-time decision-making.
However, this study has several limitations. It was conducted at a single center with a small sample size. The retrospective design carries the risk of incomplete data collection or bias. Insufficient proactive control over data collection may have resulted in missing information or selective reporting. The study did not track or discuss the changing trends of SYN-1 levels throughout the course of sepsis. Additionally, other uncontrolled confounding factors, such as excessive and unnecessary fluid administration potentially influencing SYN-1 levels, were not analyzed. These issues should be addressed in future research. Our follow-up studies will reassess methods for data collection and recording to ensure the accuracy and reliability of presented results. We aim to provide a detailed explanation of the data collection process and identify any factors that might have impacted data integrity.
Conclusion
In conclusion, our study identifies SYN-1 as a promising serum marker for predicting both the severity of sepsis and 28-day mortality. Elevated SYN-1 levels are significantly associated with increased risk of septic shock and higher mortality rates at 28 days. We observe a positive correlation between SYN-1 levels and SOFA and APACHE II scores. Combining SYN-1 with APACHE II or LAC scores enhances the accuracy of predicting 28-day mortality in sepsis patients.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Beijing Chaoyang Hospital (The ethical approval number was 2021-ke-636). Informed consent was obtained from all individual participants included in the study. We certify that the study was performed in accordance with the 1964 declaration of HELSINKI and later amendments. All methods were carried out in accordance with relevant guidelines and regulations.
Author Contributions
Bing Wei is the lead contact. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests.
References
1. Wang L, Yang M, Zhang Y, Yuan R, Kang H. Application of mesenchymal stem cells in sepsis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019;31(4):505–508. doi:10.3760/cma.j.issn.2095-4352.2019.04.028. PMID: 31109432.
2. Poston JT, Koyner JL. Sepsis associated acute kidney injury. BMJ. 2019;364:k4891. doi:10.1136/bmj.k4891. PMID: 30626586; PMCID: PMC6890472.
3. Dey S, Karim HMR, Yunus M, et al. Relationship on Admission Hypocalcaemia aIld Illness Severi’y as Measured by APACHE一II aIld s0FA Score in Intensive care Patients. J Clin Diagn Res. 2017;1(3):UC01–UC03.
4. Wang H, Kang X, Shi Y, et al. SOFA score is superior to APACHE-II score in predicting the prognosis of critically ill patients with acute kidney injury undergoing continuous renal replacement therapy. Ren Fail. 2020;42(1):638–645. doi:10.1080/0886022X.2020.1788581
5. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287. PMID: 26903338; PMCID: PMC4968574.
6. Murata K, Takeshita H, Sakamoto K, Fuwa H. Tandem Three-Component Synthesis of syn −1,2- and syn −1,3-Diol Derivatives. Chem Asian J. 2020;15(6):807–819. doi:10.1002/asia.201901660. Epub 2020 Feb 18. PMID: 32017460.
7. Johansen ME, Johansson PI, Ostrowski SR, et al. Profound endothelial damage predicts impending organ failure and death in sepsis. Semin Thromb Hemost. 2015;41(1):16–25. doi:10.1055/s-0034-1398377
8. Kuo W-K, Hua -C-C, Yu -C-C, et al. The cancer control status and APACHE II score are prognostic factors for critically ill patients with cancer and sepsis. J Formos Med Assoc. 2020;119(1):276–281. doi:10.1016/j.jfma.2019.05.012
9. Lee H, Lim CW, Hong HP, et al. Efficacy of the APACHE II score at ICU discharge in predicting post-ICU mortality and ICU readmission in critically ill surgical patients. Anaesth Intensive Care. 2015;43(2):175–186. doi:10.1177/0310057X1504300206
10. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–211. doi:10.1016/S0140-6736(19)32989-7
11. Schmoch T, Bernhard M, Becker-Pennrich A, et al. SepNet Study Group. SEPSIS-3.0 – ist die Intensivmedizinbereit für die ICD-11? [SEPSIS-3.0-Is intensive care medicine ready for ICD-11?]. Anaesthesist. 2022;71(2):104–109. Epub 2021 Aug 5. PMID: 34351432; PMCID: PMC8807467. doi:10.1007/s00101-021-01012-8
12. Cagno V, Tseligka ED, Jones ST, et al. Heparan sulfate proteoglycans and viral attachment: true receptors or adaptation Bias? Viruses. 2019;1(1):596. doi:10.3390/v11070596
13. BECKER BF, JACOB M, LEIPERT S, et al. Degradation of the endothelial glycocalyx in clinical settings: searching for the sheddases. Br J Clin Pharmacol. 2015;80(3):389–402.
14. Ingham M, Schwartz GK. Cell-cycle therapeutics come of age. J Clin Oncol. 2017;35(25):2949–2959. doi:10.1200/JCO.2016.69.0032
15. Steppan J, Hofer S, Funke B, et al. Sepsis and major abdominal surgery lead to flaking of the endothelial glycocalix. J Surg Res. 2011;165(1):136–141. doi:10.1016/j.jss.2009.04.034
16. Sallisalmi M, Tenhunen J, Yang R, et al. Vascular adhesion protein-1 and syndecan-1 in septic shock. Acta Anaesthesiol Scand. 2011;56(3):316–322. doi:10.1111/j.1399-6576.2011.02578.x
17. Ostrowski SR I, Gaïni S, Pedersen C, et al. Sympathoadrenal activation and endothelial damage in patients with varying degrees of acute infectious disease: an observational study. J Crit Care. 2015;30(1):90–96. doi:10.1016/j.jcrc.2014.10.006
18. Smart L I, Bosio E, Macdonald SPJ, et al. Glycocalyx biomarker syndecan-1 is a stronger predictor of respiratory failure in patients with sepsis due to pneumonia, compared to endocan. J Crit Care. 2018;47:93–98.
19. Donati A, Tibboel D, Ince C. Towards integrative physiological monitoring of the critically ill: from cardiovascular to microcirculatory and cellular function monitoring at the bedside. Critical Care. 2013;17(S1):
20. Kumar D, Mundlia J, Kumar T, Ahuja M. Silica coating of carboxymethyl tamarind kernel polysaccharide beads to modify the release characteristics. Int J Biol Macromol. 2020;146:1040–1049. doi:10.1016/j.ijbiomac.2019.09.229. Epub 2019 Nov 11. PMID: 31726139.
21. Junter GA, Thébault P, Lebrun L. Polysaccharide-based antibiofilm surfaces. Acta Biomater. 2016;30:13–25. doi:10.1016/j.actbio.2015.11.010. Epub 2015 Nov 7. PMID: 26555378.
22. Deng X, Kang H. Glycolysaccharides and force conduction in endothelial cells of blood vessels. Mechan Pract. 2010;32(1):1–9.
23. Nelson A, et al. Increased levels of glycosaminoglycans during septic shock: relation to mortality and the antibacterial actions of plasma. Shock. 2008;30(6):623–701. doi:10.1097/SHK.0b013e3181777da3
24. Piotti A, Novelli D, Meessen JMTA, et al. ALBIOS Investigators. Endothelial damage in septic shock patients as evidenced by circulating syndecan-1, sphingosine-1-phosphate and soluble VE-cadherin: a substudy of ALBIOS. Crit Care. 2021;25(1):113. doi:10.1186/s13054-021-03545-1. PMID: 33741039; PMCID: PMC7980645.
25. Yamaguchi J, Kinoshita K, Ihara S, et al. The clinical significance of low serum arachidonic acid in sepsis patients with hypoalbuminemia. Intern Med. 2018;57(13):1833–1840. doi:10.2169/internalmedicine.9124-17
26. Hu J, Lv C, Hu X, Liu J. Effect of hypoproteinemia on the mortality of sepsis patients in the ICU: a retrospective cohort study. Sci Rep. 2021;11(1):24379. doi:10.1038/s41598-021-03865-w. PMID: 34934165; PMCID: PMC8692355.
27. Cai N, Liao W, Chen Z, Tao M, Chen S. A Decrease in Hb and Hypoproteinemia: possible Predictors of Complications in Neonates with Late-Onset Sepsis in a Developing Country. Int J Gen Med. 2022;15:6583–6589. doi:10.2147/IJGM.S369550. PMID: 35991939; PMCID: PMC9384870.
28. LEVITT DG, LEVITT MD. Human serum albumin homeostasis: a new look at the roles of synthesis, catabolism, renal and gastrointestinal excretion, and the clinical value of serum albumin measurements. Int J Gen Med. 2016;9:229–255. doi:10.2147/IJGM.S102819
29. Mangialardi RJ, Martin GS, Bernard GR, et al. Hypoproteinemia predicts acute respiratory distress syndrome development, weight gain, and death in patients with sepsis. Ibuprofen in Sepsis Study Group. Crit Care Med. 2000;28(9):3137–3145. doi:10.1097/00003246-200009000-00001. PMID: 11008971.
30. Godinez-Vidal AR, Correa-Montoya A, Enríquez-Santos D, Pérez-Escobedo SU, López-Romero SC, Gracida-Mancilla NI. Is albumin a predictor of severity and mortality in patients with abdominal sepsis? Cir Cir. 2019;87(5):485–489. doi:10.24875/CIRU.180003903. PMID: 31448796.
31. Furukawa M, Kinoshita K, Yamaguchi J, Hori S, Sakurai A. Sepsis patients with complication of hypoglycemia and hypoalbuminemia are an early and easy identification of high mortality risk. Intern Emerg Med. 2019;14(4):539–548. doi:10.1007/s11739-019-02034-2. Epub 2019 Feb 7. Erratum in: Intern Emerg Med. 2019 Nov;14(8):1365. PMID: 30729384; PMCID: PMC6536472.
32. Alderson P, Bunn F, Lefebvre C, et al. Human albumin solution for resuscitation and volume expansion in critically ill patients. Cochrane Database Syst Rev. 2004;18(4):CD001208.
33. Engelmannn O, Pücklerk VON, et al. Applicability of 99mTc-labeled human serum albumin scintigraphy in dogs with protein-losing enteropathy. J Vet Intern Med. 2017;31(2):365–370. doi:10.1111/jvim.14673
34. Bode L, Salvestrini C, Park PW, et al. Heparan sulfate and syndecan-1 are essential in maintaining murine and human intestinal epithelial barrier function. J Clin Invest. 2008;118(1):229–238. doi:10.1172/JCI32335
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.