")
Back to Journals » Open Access Journal of Contraception » Volume 16
Predictors of Family Planning Choices in Rwanda: Insights from the 2019-2020 Demographic and Health Survey
Authors Kubahoniyesu T , Mugabo H
Received 26 April 2025
Accepted for publication 4 July 2025
Published 9 July 2025 Volume 2025:16 Pages 71—80
DOI https://doi.org/10.2147/OAJC.S527717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Theogene Kubahoniyesu,1 Hassan Mugabo2
1African Centre of Excellence in Data Science, University of Rwanda, Kigali, Rwanda; 2Research, Innovation and Data Science Division, Rwanda Biomedical Centre, Kigali, Rwanda
Correspondence: Theogene Kubahoniyesu, Email [email protected]
Background: Family planning is a key public health priority that supports informed reproductive choices. This study examined the socio-demographic determinants influencing contraceptive method preferences among women of reproductive age in Rwanda.
Methods: This study employed a cross-sectional design through analysis of data from the 2019– 2020 Rwanda Demographic and Health Survey (RDHS). The analysis included 5,578 women aged 15– 49 years who were using any contraceptive methods. Logistic regression was applied to identify factors associated with the choice between modern and traditional contraceptive methods. A significance level of 5% (p < 0.05) was used to determine the associations.
Results: Overall, 91.1% of contraceptive users reported using modern methods, with implants being the most commonly used (42.9%) and female condoms the least used (0.05%). Factors significantly associated with modern methods choice included living in female-headed households (AOR = 1.22), older age (AOR = 2.68 for ages 30– 34), married women (AOR = 1.92), and those in higher wealth quintile (AOR = 1.71). In contrast, living in rural areas (AOR = 0.77) and identifying as Adventist (AOR = 0.68), were associated with lower odds of modern contraceptive choice.
Conclusion: The findings underscore a strong preference for modern contraceptive methods among Rwandan women. However, sociodemographic disparities remain, particularly among rural population and specific religious groups. Tailored family planning policies are needed to address these gaps and ensure equitable access to modern contraceptive methods accross all population subgroups.
Keywords: contraceptive methods, family planning, Rwanda, DHS, predictors
Introduction
Family planning refers to the deliberate efforts taken individuals or couples to control or space the number of children they have, primarily through the use of contraceptive methods.1 Contraceptive methods are generally categorized into two groups: Traditional Family Planning Methods (TFPM) and Modern Family Planning methods (MFPM). The TFPM includes the rhythm method (periodic abstinence), withdrawal (coitus interruptus), fertility awareness-based approaches, the lactational amenorrhoeic method (LAM), and other culturally rooted or folk practices. In contrast, MFPM which consist of barrier methods such as male and female condoms, diaphragms, cervical caps, and sponges, as well as hormonal contraceptives like oral pills, injectables, vaginal rings, implants, and intrauterine devices (IUDs).2 Some contraceptive methods, such as male condoms, withdrawal, and rhythm methods, have been in use for a long time, whereas others, such as the pill and intrauterine device (IUD), were introduced in the 1960s. More recently, options like the vaginal ring, emergency contraception, subcutaneous injections, and implants have also become available.3
Worldwide, the prevalence of contraceptive use among women of reproductive age who are married or living with a partner increased from 54.8% (95% uncertainty interval: 52.3–57.1) in 1990 to 63.3% (60.4–66.0) in 2010, reflecting a rise of 8.5 percentage points (4.7–12.1).4 Previous studies have demonstrated that greater access to various modern contraceptive methods leads to an increase in modern contraceptive use, while a heavy reliance on just one or two methods may indicate a restricted availability of options.4 Since 1994, the use of rhythm and withdrawal methods has decreased, with the most significant decline observed in Europe and North America. 6% of women still use traditional family planning methods, despite their reduced popularity following the introduction of more effective methods.2
According to the study in Nigeria,5 African mothers traditionally practice intensive breastfeeding for longer than 24 months, and it can go up to 36 months. Some societies also practice postpartum marital separations, where the women would go and stay with their parents for some time, which would keep the partners without sexual intercourse for some time and thus prevent pregnancy.6 However, modern family planning methods that were more organized started coming into the subcontinent in the early 1950s, and there was a high gear for establishing FP methods in the region. It started with Rhodesia (now known as Zimbabwe) in 1955, Uganda in 1956, Kenya in 1957 and others followed.7
To understand the behavioral mechanisms underpinning contraceptive method choices, this study adopts the Health Belief Model (HBM) as its theoretical framework.8 The HBM posits that individual health-related decisions, such as the use of family planning, are influenced by perceptions of susceptibility to unintended pregnancy, perceived benefits of modern contraceptive methods, perceived barriers such as access or religious constraints, and cues to action, including partner involvement or healthcare outreach. By using the HBM as our guide, we look at how different social and demographic factors reflect these perceptions and affect the choice of contraceptive methods among women in Rwanda.
Despite the availability of both modern and traditional family planning methods, recent data indicate that the average total fertility rate in sub-Saharan Africa remains at 4.8 children per woman, compared to an average of 3.8 children per woman across all least developed countries globally. Using data from the Rwanda Demographic and Health Survey, this study sought to explore the relationships between various factors and the preference for modern contraceptive methods. These findings are crucial for designing targeted interventions that cater to the diverse preferences of different demographic groups and support informed family planning choices.
Methods and Materials
Study Design
This cross-sectional study was based on secondary data obtained from the 2019–2020 Rwanda Demographic and Health Survey.
Study Population
The study population included only 5,578 women aged 15–49 years who reported using either modern or traditional contraceptive methods at the time of the survey. Women who were not using any method were excluded from the analysis, as the study focused on method preference among users rather than overall contraceptive uptake.
Study Setting
The Rwanda Demographic and Health Survey (RDHS) was carried out in Rwanda, a country located in Eastern Africa. Rwanda has a population of 13,246,394 people and spans an area of 26,228 square kilometers.9 The RDHS is conducted every five years, describing the data on important health and demographic characteristics of the population.
Source of Data
Data were collected from a secondary source.10 It consisted of respondents aged 15–49 who had been using one of the contraceptive methods.
Secondary data from the RDHS were processed by editing, coding, and entering it into computer statistical package (STATA) version 17.
Model Specification
A logistic regression analysis was conducted to assess the effect of each predictor (independent variable) on the outcome variable (dependent variable). In this analysis, the dependent variable, the type of contraceptive method (traditional or modern) used, was recoded into a binary variable, with 0 representing “Traditional FP” and 1 representing “Modern FP.” Reference categories were defined for each explanatory variable to enable comparison of the odds of choosing Modern versus Traditional FP Methods accross different groups..
Statistical Analysis
The dataset was weighted using STATA version 17. Descriptive statistics were applied to present the prevalence of modern and traditional contraceptive methods, while bivariate and multivariate analyses were conducted to determine the factors influencing contraceptive method choices. A 5% significance level was set, and odds ratios along with confidence intervals were computed. Missing data were minimal (<5%) and were handled through listwise deletion, consistent with DHS analytical standards. Bivariate results were primarily used as a preliminary step to inform the inclusion of covariates in the multivariate logistic regression model. Only variables that showed a statistically significant relationship with the outcome (p < 0.05) or were supported by existing literature were retained in the final model. Since the study aimed to find out what factors independently influence the choice of contraceptive methods, we decided to share only the multivariate results, as they better handle other influencing factors and give stronger estimates of the relationships.
Results
Socio-Demographic Characteristics of Respondents, Rwanda
This section explores the demographic characteristics of the respondents. Gathering this information was essential to provide a comprehensive background on the women of reproductive age who participated in the 2019–2020 Rwanda Demographic and Health Survey. Sociodemographic factors were subsequently analyzed in relation to the use of family planning methods, whether traditional or modern (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Respondents, Rwanda |
The survey included 5,578 respondents, examining the gender distribution of the respondent heads, and it became evident that male-headed households predominated, constituting 79.2% of the sample. Regarding the wealth index, it is noteworthy that the wealth distribution among respondent heads was balanced across various categories. The “Poorest” wealth group stands out as the most populated, comprising almost 21.98% of the sample, closely followed by the “Richer” and “Middle” groups, each representing about one-fifth of the population. Educational attainment among the respondents followed a similar trend. A significant proportion of the sample, 3725 (66.78%), had received primary education, indicating a substantial level of basic education. Secondary education followed suit, representing approximately 990 (17.75%) of the respondents, while a smaller proportion, around 261 (4.68%), had attained tertiary education.
Considering the age distribution, this study captures a broad range of ages among the respondent heads. The age group “30–34” stands out with the largest representation, comprising 1283 (23%) of the sample, followed by “35–39” and “25–29” age groups at approximately 1239 (22.21%) and 1023 (18.34%) respectively. Moving from individual characteristics to geographical context, the distribution by region revealed that a majority of the respondents, around 4386 (78.63%), resided in rural areas. This stark contrast with the urban population, which accounts for approximately 1192 (21.37%), reflects the ongoing urban-rural divide in Rwanda. Examining marital status, a significant proportion of the respondents were married, making up over half of the sample at 3015 (54.05%). “Living with partner” follows as the next substantial category at nearly 1661 (30%), reflecting a prevalent cohabitation practice. Moreover, the presence of individuals who are “Never in union”, “Widowed”, “Divorced”, or “No longer living together/separated” underscores the diverse marital situations that can influence family planning uses.
Lastly, when it comes to religious affiliation, the dataset shows a nearly balanced split between “Catholic” and “Protestant” respondents, each accounting for around 2188 (39%) and 2446 (44%) of the sample, respectively.
The Prevalence of Modern and Traditional Family Planning Methods
This study further establishes the prevalence of modern and traditional family planning methods in Rwanda (Figure 1).
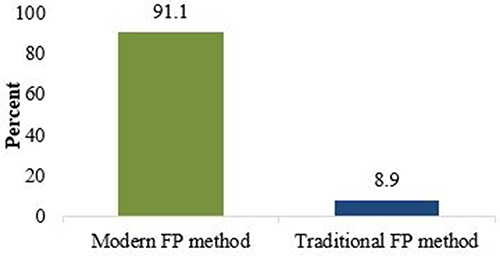 |
Figure 1 Contraceptive Prevalence rate in Rwanda (2019–2020). |
The results indicated that a higher proportion of respondents (91.1%) used modern contraceptive methods, and only 8.9% used traditional methods.
The researcher also presented a visual representation of the utilization of various family planning (FP) methods. (Figure 2) Among the modern methods, implants emerged as the most prevalent, selected by 42.94% of the respondents. Injections followed closely, with 23.54%, whereas pills were opted for by 9.75% of the participants. In addition to other methods, male condom usage was 6.11%. Notably, the least utilized modern FP method was the female condom, with only 0.05% of respondents opting for it.
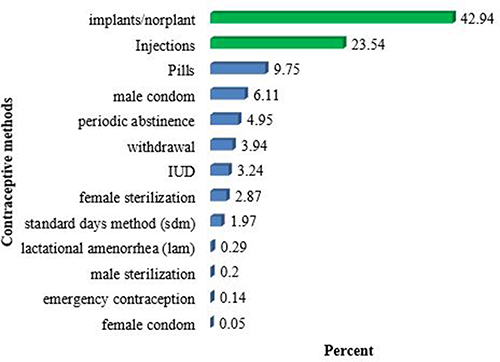 |
Figure 2 A representation of the different contraceptive methods used in Rwanda (%). |
Regarding traditional FP methods, the findings indicated that periodic abstinence was the most commonly chosen option, with a prevalence of 4.95%. Withdrawal emerged as another frequently used method, chosen by 3.94% of the participants. Conversely, the least popular traditional family planning method was lactational amenorrhea (LAM), employed by only 0.29% of respondents (Figure omitted intentionally).
The Factors That Influence the Use of Contraceptive Methods
This study further sought to determine which demographic factors influenced the type of contraceptive method used (traditional or modern). A chi-square test at the 5% level of significance was used to establish whether there was any relationship between these factors and the type of family planning method used. Significant predictors from bivariate analysis were further analyzed using logistic regression.
Logistic regression analysis provides a comprehensive understanding of how sociodemographic factors influence the use of traditional and modern contraceptive methods, as represented by binary outcomes (Table 2).
 |
Table 2 Multivariable Analysis of Factors Associated with the Use of Contraceptive Methods |
The analysis reveals that female-headed households have 22.41% higher odds of preferring modern family planning methods over traditional methods than male-headed households (AOR: 1.2241, 95% CI: [1.069–1.381], p = 0.0184).
Economic status is a significant determinant of the wealth index. As wealth has improved, the likelihood of selecting modern methods has increased. The wealthiest category exhibited a 70% increase in odds of choosing traditional methods over modern methods (AOR, 1.7063; 95% CI: [1.013–3.811], p-value: 0.022), highlighting the association between wealth and preference for modern family planning. Age played a significant role in family planning. Odds ratios above 1 indicate that with advancing age, there is a higher likelihood of preferring modern methods. For instance, individuals aged 30–34 had 167.81% higher odds of choosing modern methods compared to the youngest age group (15–19) (AOR: 2.6781, 95% CI: [2.056–3.44], p <0.001).
Residing in rural areas was associated with 23.06% lower odds of selecting modern methods than in urban areas (AOR: 0.7694, 95% CI: [0.633–0.929], p = 0.041). Marital status was also a significant factor. Being married increased the odds of opting for modern methods (1) by 92.48% (AOR: 1.9248, 95% CI: [1.422–2.480], p = 0.001), and living with a partner increased the odds by 271.47% (AOR: 3.7147, 95% CI: [2.983–4.618], p <0.001). In terms of religious affiliation, Adventists were 32.29% less likely to choose modern methods than traditional methods (AOR: 0.6771, 95% CI: [0.539–0.853], p = 0.006), while other religious categories did not consistently demonstrate significant associations.
Discussion
Although several studies have assessed the prevalence of factors related to contraceptive use, few have specifically investigated the determinants influencing the choice between modern and traditional contraceptive methods. This study found that a significant majority of respondents (91.1%) chose modern family planning methods. The dominance of modern methods signifies a significant shift in preferences and highlights the influence of evolving healthcare options and awareness campaigns. By contrast, a smaller proportion, specifically 8.9% of the respondents, still adhered to traditional family planning methods. This lower prevalence of traditional methods signals a gradual transition from longstanding practices, possibly attributable to advancements in medical knowledge and changing social norms.
These findings correlate very well with a study conducted in Zanzibar,2 which indicated that modern contraceptive methods are utilized more (short-term, 46.1%; long-term, 45.2%) than traditional methods (8.7%). The variations in the results might be due to differences in sociodemographic characteristics, particularly sex, across study areas. It also relates to a survey by the National Institute of Statistics of Rwanda (NISR)10 where it was discovered that 58% of married people currently used an MFPM, compared to 6% for the TFPM. The finding also implies that, in general, modern methods are used more often than traditional ones. The prevalence of modern contraceptive methods used was also obtained from a study conducted in sub-Saharan Africa, which indicated that more respondents used modern contraceptive methods (21.7%) than reverse methods.11
In this study, advanced age of women was found to influence the use of modern versus traditional contraceptive methods. Similarly, the study conducted in Ethiopia12 revealed that women aged 35–49 years had higher odds for modern contraceptive methods; the study also noted that being in a wealthier category is associated with a preference for modern methods.
Marital status was found to be an important predictor of choosing modern over traditional contraceptive methods, with married women and women living with partners having higher odds, which concurs with the findings from the study conducted in southern Ethiopia,13 which found that married women had 3.9 times higher odds (AOR) of using family planning than those who were not married. This may reflect the influence of partner dynamics and discussions on family planning within marriages.
The wealth group has been found to influence the use of modern contraceptive methods more than traditional contraceptive methods, where an increase in wealth positively shifts user use from traditional to modern contraceptive methods. The same findings were revealed in a study conducted in Yemen, which emphasized that women from higher-wealth groups are more likely to utilize modern contraceptive methods.14 This pattern underscores the role of socioeconomic factors in shaping decisions regarding RH.
Women living in urban areas were more inclined to select modern contraceptive methods, as demonstrated in this study, aligning with findings from research conducted across 29 countries, which highlighted that urban women tend to prefer modern over traditional family planning methods.15 This highlights the influence of urbanization on family planning.
Conclusion
This study explored the factors that influence the choice between modern and traditional contraceptive methods in Rwanda. With 91.1% of women using modern methods, it was found that female-headed households, advanced age, marriage, and higher wealth levels were associated with preference for modern contraceptive methods. In addition, urban residences have been linked to a higher modern method usage. These findings highlight the need for targeted interventions, including faith-sensitive outreach and enhanced counseling at the primary care level, particularly in rural areas. Furthermore, efforts should focus on supporting older women and female-headed households while tailoring family planning services to address the unique needs of different marital and socioeconomic groups.
Synopsis
What is already known on this topic: Previous studies were conducted on
- Previous research has indicated that modern contraceptive methods are widely adopted in many countries, including Rwanda.
- Access to family planning services, along with cultural and religious beliefs, significantly influences contraceptive preferences and usage patterns, underscoring the importance of developing targeted interventions for different demographic groups.
What This Study Adds:
- Detailed Analysis of Influencing Factors: This study provides a comprehensive analysis of sociodemographic variables, such as female-headed households, age, marital status, and wealth, which significantly influence the preference for modern versus traditional contraceptive methods in Rwanda.
- Geographic and Demographic Insights: This study highlights the impact of residing in rural versus urban areas and various socioeconomic conditions on the choice of contraceptive methods, identifying specific groups that may benefit from targeted interventions.
Data Sharing Statement
The data are available on the Demographic and Health Survey website (www.dhsprogram.com) upon reasonable request.
Ethical Considerations
This study was based on secondary analysis of data from the 2019–2020 Rwanda Demographic and Health Survey (RDHS), which was approved by the Rwanda National Ethics Committee (RNEC) and the ICF Institutional Review Board. The RDHS data are publicly available and anonymized, with informed consent obtained from all participants by the DHS Program. According to the Rwandan National Guidelines for Research Involving Human Participants (2012) and institutional policy, additional ethical approval is not required for studies based solely on the secondary analysis of de-identified, publicly available data. A data use authorization was obtained from the DHS Program prior to conducting this study.
Acknowledgments
We extend our gratitude to the women who participated in the demographic and health surveys, as their valuable contributions greatly influenced the direction of our study. We acknowledge the support of the National Institute of Statistics of Rwanda (NISR) for providing data.
Author Contributions
TK conceptualized the study, designed the methodology, led the data analysis and interpretation, and drafted the manuscript. HM contributed to the literature review, interpretation of findings, and critical revision of the manuscript. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this research.
Disclosure
The authors declare that this research was conducted without any relationships or interests that could potentially create any conflicts of interest. All authors have agreed to submit this paper to this journal and are accountable for all aspects of this work.
References
1. WHO. New WHO tool helps guide contraception choices following childbirth; 2016. Available from: https://www.who.int/news/item/15-01-2016-new-who-tool-helps-guide-contraception-choices-following-childbirth.
2. Miraji KA, Babune GJ. Modern or traditional: factors influencing the adoption of family planning methods among women in urban District Zanzibar. Management. 2021;9:54–63.
3. UNAIDS. 2020 UNAIDS Data Book; 2020.
4. Biddlecom A, Kantorova V. Global trends in contraceptive method mix and implications for meeting the demand for family planning.
5. Adebayo AM, Ilesanmi OS, Falana DT, et al. Prevalence and predictors of exclusive breastfeeding among mothers in a semi-urban Nigerian community: a cross-sectional study. Ann Ibadan Postgrad Med. 2021;19:31–39.
6. Clementine U, Manasse U, Pascal N, et al. The use of immediate postpartum family planning at Kacyiru Hospital, Rwanda. Rw Public Health Bul. 2020;2:16–25.
7. Andi JR, Wamala R, Ocaya B, Kabagenyi A. Modern contraceptive use among women in Uganda: an analysis of trend and patterns (1995–2011). Etude Popul Afr. 2014;28:1009–1021. doi:10.11564/28-0-553
8. Jones CL, Jensen JD, Scherr CL, Brown NR, Christy K, Weaver J. The health belief model as an explanatory framework in communication research: exploring parallel, serial, and moderated mediation. Health Communication. 2015;30:566–576. doi:10.1080/10410236.2013.873363
9. NISR. Rwanda Population and Housing Census, 5th RPHC; 2022.
10. RDHS. 6th Rwanda Demographic and Health Survey, 2019–2020 (RDHS -VI). Kigali; 2020.
11. Kraft JM, Serbanescu F, Schmitz MM, et al. Factors associated with contraceptive use in Sub-Saharan Africa. J Women’s Health. 2022;31:447–457. doi:10.1089/jwh.2020.8984
12. Tsehay CT. Factors associated with modern contraceptive demands satisfied among currently married/in-union women of reproductive age in Ethiopia: a multilevel analysis of the 2016 Demographic and Health Survey. BMJ Open. 2022;12:1–13. doi:10.1136/bmjopen-2021-049341
13. Mesfin Yesgat Y, Gebremeskel F, Estifanous W, et al. Utilization of family planning methods and associated factors among reproductive-age women with disability in Arba Minch Town, Southern Ethiopia. Open Access J Contracept. 2020;11:25–32. doi:10.2147/OAJC.S240817
14. Boah M, Adokiya MN, Hyzam D. Prevalence and factors associated with the utilisation of modern contraceptive methods among married women of childbearing age in Yemen: a secondary analysis of national survey data. BMJ open. 2023;13:e071936. doi:10.1136/bmjopen-2023-071936
15. Ahinkorah BO, Budu E, Aboagye RG, et al. Factors associated with modern contraceptive use among women with no fertility intention in sub-Saharan Africa: evidence from cross-sectional surveys of 29 countries. Contracept Reprod Med. 2021;6:1–13. doi:10.1186/s40834-021-00165-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.