")
Back to Journals » Clinical Ophthalmology » Volume 19
Preliminary Evaluation of Clinical and Non-Clinical Outcome Metrics in Patient Satisfaction After Implantation of a Non-Constant Aberration-Correcting Monofocal IOL
Authors Schallhorn SC , Teenan D , Venter JA , Schallhorn JM , Hannan SJ
Received 9 November 2024
Accepted for publication 4 February 2025
Published 10 March 2025 Volume 2025:19 Pages 795—806
DOI https://doi.org/10.2147/OPTH.S505584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Steven C Schallhorn,1– 3 David Teenan,2 Jan A Venter,2 Julie M Schallhorn,1,4 Stephen J Hannan2
1Department of Ophthalmology, University of California, San Francisco, CA, USA; 2Optical Express, Glasgow, UK; 3Carl Zeiss Meditec, Inc, Dublin, CA, USA; 4F.I. Proctor Foundation, University of California, San Francisco, CA, USA
Correspondence: Steven C Schallhorn, Department of Ophthalmology, University of California, 490 Illinois St, San Francisco, CA, 94158, USA, Tel +1-858-455-6800, Email [email protected]
Purpose: To evaluate patient-reported outcomes after implantation of a non-constant aberration-correcting monofocal IOL and explore factors affecting postoperative satisfaction with vision.
Methods: This retrospective study comprised patients who underwent cataract surgery with bilateral implantation of CT LUCIA 621P IOL (Carl Zeiss Meditec AG, Jena, Germany). Factors affecting postoperative satisfaction with vision were evaluated, including patient demographics, clinical and non-clinical variables (visual acuities, adverse events, ocular comorbidities, general health, depression scores, personality types), and other patient-reported outcomes (visual phenomena, dry eye). Questionnaires were used to assess patient-reported visual outcomes, depression, and personality types. The outcomes of the last available clinical visit were evaluated.
Results: A total of 97 patients were included, of whom 63.9% reported to be very satisfied and 30.9% were satisfied with postoperative vision. Only three patients were dissatisfied, and the reasons were mostly related to their postoperative clinical findings. In a multivariate logistic regression analysis, the patient’s age and postoperative uncorrected visual acuity were significant predictors of postoperative satisfaction. Some non-clinical and clinical variables were signaling potential trends in satisfaction, but a larger cohort of patients would be required to explore them.
Conclusion: Satisfaction of cataract patients implanted with a monofocal IOL remains high. When evaluating postoperative satisfaction, non-clinical factors and interactions with other patient-reported outcomes (visual phenomena or dry eye) should not be underestimated.
Keywords: monofocal IOL, non-constant aberration-correcting design, patient satisfaction
Introduction
The causes of dissatisfaction in patients with multifocal IOLs are frequently debated in the literature, mainly due to a higher prevalence of visual side effects.1–4 The factors affecting the satisfaction of patients implanted with monofocal IOLs are less commonly explored. In patients undergoing cataract surgery, some parameters influencing patient satisfaction might be more noticeable as they are related to visual function and ocular characteristics, such as visual acuity, ocular comorbidities, postoperative adverse events, presence of visual phenomena, or dry eyes.5–15 However, other less obvious, non-ocular factors could potentially play a role in postoperative satisfaction, and these are not commonly considered when evaluating postoperative satisfaction. Examples include patient personality traits, depression, demographics, or general medical history.7,9,11,14–17
In one of our previous studies, we assessed the refractive and visual outcomes of patients implanted with a new aspheric non-constant aberration-correcting monofocal IOL, CT LUCIA 621P (Carl Zeiss Meditec AG, Jena, Germany).18 The study reported predictable refractive outcomes and high levels of postoperative visual acuity. However, there is a need to evaluate how the claims of better quality of vision of the non-constant aberration-correcting optic concept relate to patient-reported quality of vision and visual phenomena rates.
In the current study, we evaluated patient-reported outcomes in patients bilaterally implanted with the CT LUCIA 621P IOL and explored preoperative and postoperative variables that could be related to patient satisfaction.
Patients and Methods
The study was deemed exempt from review by the Institutional Review Board at the University of California, San Francisco because it used only retrospective, deidentified patient data. Postoperative patient-reported outcomes of cataract patients implanted with monofocal CT LUCIA 621P IOL between June 2022 and October 2023 were assessed. All patients provided written consent to undergo cataract surgical procedures and to use their deidentified records for research purposes. The study adhered to the tenets of the Declaration of Helsinki.
Data were retrospectively extracted from the electronic medical record of Optical Express, United Kingdom, with the following requirements: cataract surgery with the implantation of CT Lucia 621P IOL in both eyes, preoperative corneal astigmatism ≤ 1.50 D, completed a minimum of 1-month postoperative visit, and completed postoperative patient experience questionnaire. The extracted variables included preoperative visual acuity and refractive error, demographics, preoperative questionnaire (including medical history, self-reported depression scores, and personality types), preoperative ocular comorbidities, adverse events, postoperative refraction and visual acuity, and postoperative patient-reported outcomes.
At baseline, all patients underwent a full ophthalmic examination, including visual acuity testing, slit lamp examination, and dilated fundus examination. Diagnostic scans included autorefraction and tonometry (Tonoref II, Nidek Co. Ltd., Gamagory, Japan), corneal tomography (Pentacam, Oculus Optikgeräte GmbH, Wetzlar, Germany), endothelial cell count (SP 2000P specular microscope, Topcon Corp, Tokyo, Japan), biometry (IOLMaster 700, Carl Zeiss Meditec AG, Jena, Germany) and retinal optical coherence tomography (Cirrus 4000/5000 OCT, Carl Zeiss Meditec AG, Jena, Germany). The patients were advised to return for day one, one week, one month, and three months postoperative visits, and thereafter as required. Variables recorded on postoperative visits were visual acuities (corrected distance visual acuity, CDVA, and uncorrected distance visual acuity, UDVA), refraction, keratometry, intraocular pressure measurement, slit-lamp examination, and the presence of any adverse event.
Patients were asked to complete questionnaires on the preoperative visit and all postoperative visits. The questions included in the analysis were preoperative patient-reported personality type and depression symptoms,19,20 postoperative general satisfaction questions, the severity of visual phenomena (glare, halo, starburst, ghosting/double vision), and the severity and frequency of dry eye symptoms. All questions used in the study are summarized in Table 1. The data from the last available postoperative exam that contained full refractive, visual acuity, and patient-reported outcomes were used in the analysis.
 |
Table 1 Preoperative and Postoperative Questionnaire |
The surgeries were performed using the standard phacoemulsification technique by four surgeons in three surgical centers. The fully preloaded CT LUCIA 621P IOL was successfully implanted into the capsular bag in all cases using the BLUESERTTM (Carl Zeiss Meditec AG, Jena, Germany) injector through a 2.75 mm clear corneal incision.
Postoperative regimen included 250mg acetazolamide tablet per oral taken 4–6 hours after surgery, topical antibiotic drops (levofloxacin 5mg/mL) for 2 weeks (every two hours for the first 24 hours and then four times a day for the remaining 13 days), and topical steroid drops (dexamethasone 0.1%) for four weeks (every two hours for the first 24 hours, four times a day for 13 days and three times a day for further 14 days).
Intraocular Lens
The CT LUCIA 621P is a single-piece C-loop monofocal aspheric hydrophobic acrylic IOL with a 6.0 mm optic diameter and an overall length of 13.00 mm. It is step-vaulted with 0° angulation and features a 360° square edge design for posterior capsule opacification prevention. The IOL is equipped with a patented ZO (Zeiss Optic; Carl Zeiss Meditec AG, Jena, Germany) profile. It is a non-constant aberration-correcting profile with a central zone with negative spherical aberration, which changes from negative to positive spherical aberration towards the periphery of the optic. Such a design is supposed to improve the tolerance of the lens to possible decentration. The profile was derived from Liou & Brennan’s eye model,21 attempting to imitate the normal human eye’s aberration and imaging properties. The detailed features of the ZO design have been previously described.18
Statistical Analysis
Basic postoperative refractive and visual outcomes of the study cohort were summarized using the standard graphs for reporting outcomes of intraocular lens-based surgery in the cataract population, and the incidence rate of postoperative satisfaction, visual phenomena, and dry eye was calculated. The characteristics of patients who reported to be “Very Satisfied” with postoperative outcomes were compared to all other patients. The compared variables included demographics, visual acuities, postoperative symptoms of visual phenomena and dry eye, pre-existing co-pathology, postoperative adverse events, general health conditions, patient preoperative depression scores, and personality types. Continuous variables were compared using an independent t-test or Mann–Whitney U-test (depending on the normality assumption), and the percentages were compared using a Chi-square test. Additionally, a logistic regression model was constructed to assess whether any of these variables had an independent effect on the odds of being “Very Satisfied” with postoperative vision. The data from the last available postoperative exam that contained full refractive, visual acuity, and patient-reported outcomes were used in analysis.
Results
A total of 97 patients (194 eyes) with bilateral implantation of the CT LUCIA 621P IOL were included. The preoperative and postoperative characteristics of the study group are summarized in Table 2. Postoperatively, the mean binocular uncorrected visual acuity of the group was 0.00 ± 0.11 logMAR (20/20), with 78.4% of patients (76 out of 97) achieving 20/20 or better binocular UDVA. The percentage of eyes with postoperative manifest spherical equivalent within ±0.50 D and ± 1.00 D was 82.5% (160 out of 194 eyes) and 97.4% (189 out of 194 eyes), respectively. Corrected distance visual acuity changed from the preoperative value of 0.34 ± 0.39 logMAR (20/40−2) to 0.00 ± 0.09 logMAR (20/20) at the last available visit. Standard graphs for reporting refractive outcomes for intraocular procedures in a cataract population are summarized in Figure 1.
 |
Table 2 Preoperative and Postoperative Refractive and Visual Data of the Study Group |
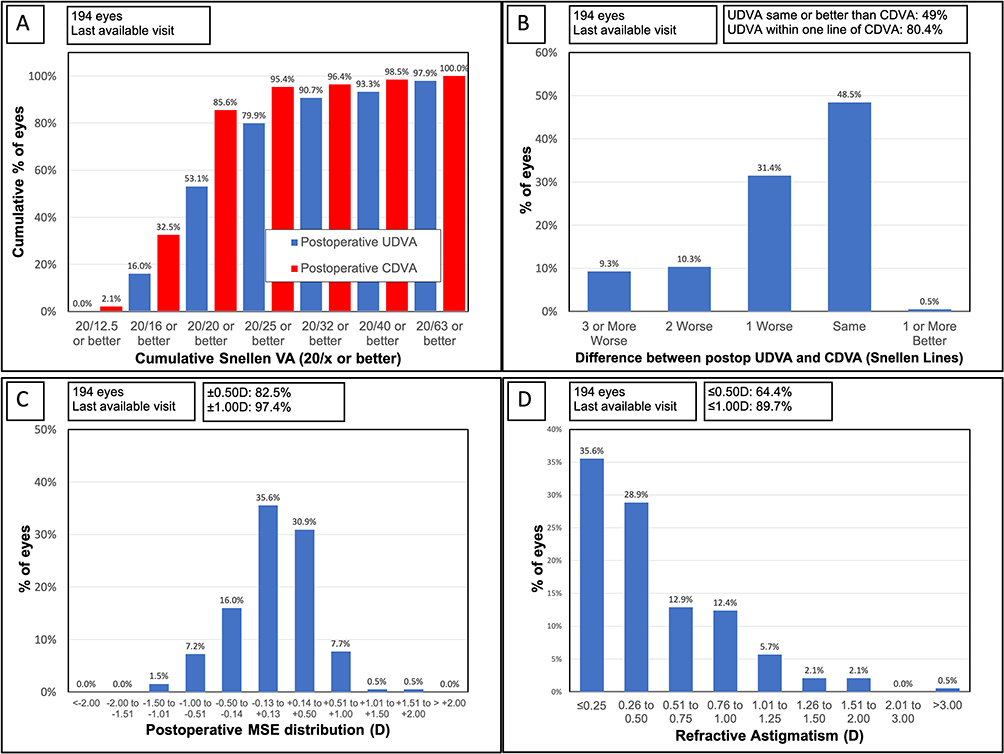 |
Figure 1 Postoperative visual and refractive outcomes. (A) Postoperative cumulative uncorrected distance visual acuity (UDVA) and postoperative corrected distance visual acuity (CDVA). (B) The difference between postoperative UDVA and postoperative CDVA. (C) The distribution of postoperative manifest spherical equivalent. (D) The distribution of postoperative refractive astigmatism. |
Postoperative Satisfaction
Figure 2A and B show the satisfaction outcomes of the study group. Of all patients, 63.9% (62 out of 97 patients) reported being “Very Satisfied” and 30.9% (30/97) reported being “Satisfied” with their postoperative vision (Figure 2A). Only three patients (3.1%) were “Dissatisfied”, no patient reported being “Very Dissatisfied”, and only 2 patients (2.1%) claimed to be neither satisfied nor dissatisfied. The reasons for dissatisfaction in the three patients were as follows: Patient 1 had preexisting age-related dry macular degeneration, limiting her postoperative quality of vision. Patient 2 had reduced visual acuity with an unidentifiable cause at the one-month visit when the questionnaire was completed (postoperative binocular UDVA was 20/63 with a minimal refractive error, compared to preoperative CDVA of 20/100). The common postoperative adverse events known to transiently reduce vision following cataract surgery (such as cystoid macular edema, posterior capsule opacification, or inflammation) and the presence of ocular co-morbidity were ruled out. His visual acuity gradually improved to 20/40 at the last available visit at three months. Patient 3 had dry eye and ocular discomfort issues. These subsided over time, and the patient had 20/12.5 binocular visual acuity at the final visit.
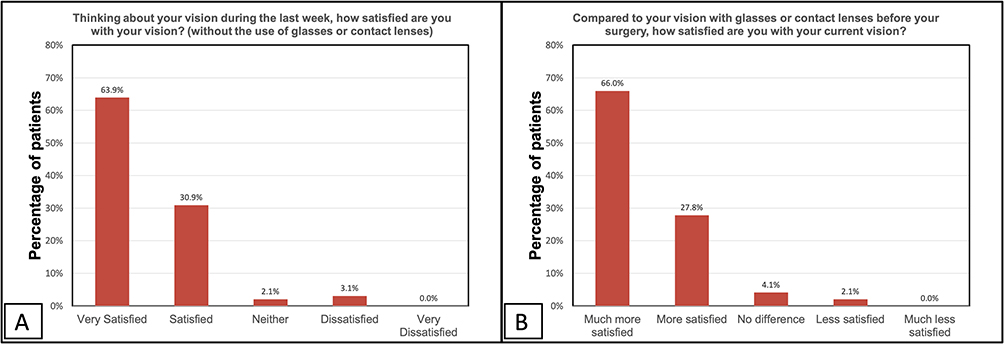 |
Figure 2 Postoperative satisfaction with vision (A), and postoperative satisfaction with vision compared to vision with correction before surgery (B), n = 97 patients. |
Of all patients, 93.8% (91 out of 97) reported to be “Much more satisfied” or “More satisfied” with their postoperative vision compared to their vision with their glasses or contact lenses before surgery (Figure 2B). Only two patients (2.1%) reported to be “Less satisfied” (“Patient 1” and “Patient 2” from the three patients dissatisfied with their postoperative vision).
Additionally, 97.9% (95 out or 97) of patients answered they would have the surgery again and 99.0% (96 out of 97) would recommend the surgery to their friends and relatives.
Visual Phenomena
The mean score for visual phenomena difficulty (rated on the scale from 1 – no difficulty to 7 – severe difficulty) was 1.57 ± 1.07 for glare, 1.20 ± 0.74 for halo, 1.35 ± 1.08 for starburst, 1.14 ± 0.50 for ghosting/double vision.
The distribution of postoperative visual phenomena is depicted in Figure 3. Most patients reported none or only mild visual phenomena postoperatively. Significant visual phenomena (scores 6 and 7 for any of the four evaluated optical side effect) were reported only by 3 patients (3.1% of the cohort). The first patient is the dissatisfied “Patient 1” with age-related dry macular degeneration from the previous discussion. The second patient had typical clinical signs of dry eye with grade 3 punctate epithelial erosions and tear-break-up time reduced to 2–3 seconds present on the day when the postoperative questionnaire was completed. The reason for significant visual phenomena in the third patient was unidentified, but gradual improvement in symptoms throughout the available postoperative course was reported.
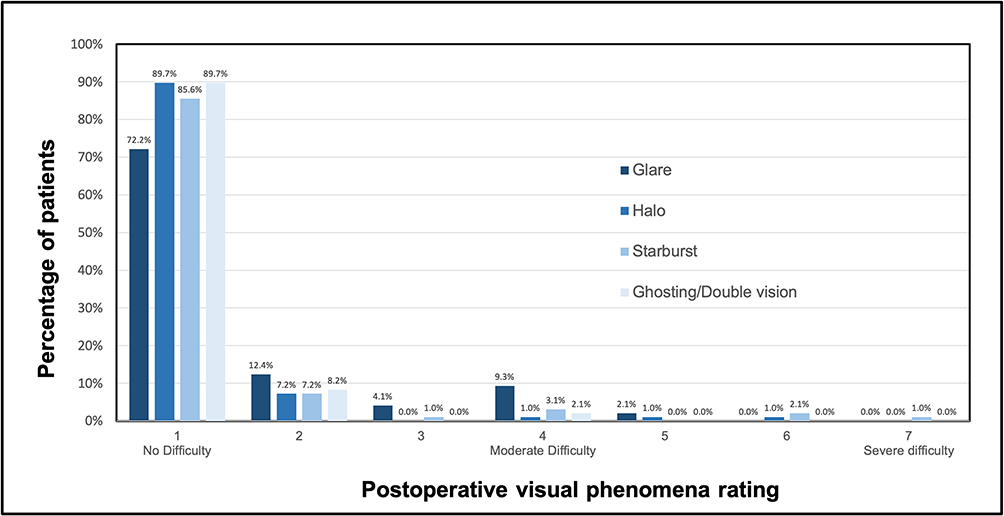 |
Figure 3 Postoperative difficulty with visual phenomena, n = 97 patients. |
Dry Eye Symptoms
The histograms in Figure 4A and B depict postoperative patient-reported dry eye severity and frequency distribution. The mean score for dry eye severity (rated on a scale from 1 – no difficulty to 7 – severe difficulty) was 1.90 ± 1.23. Of all patients, 78.4% (76 out of 97) had no or minimal difficulty (combined score 1 and 2) with dry eye symptoms, 19.6% (19/97) had moderate difficulty (combined score 3,4,5), and 2.1% (2/97) had significant difficulty (score 6 and 7).
 |
Figure 4 Postoperative dry eye severity rating (A) and dry eye frequency rating (B), n = 97 patients. |
The mean score for dry eye frequency (rated on a scale from 1 – none of the time to 5 all of the time) was 1.77 ± 1.00. Only two patients (2.1% of the cohort) in the study reported postoperative dry eye symptoms all of the time.
Association Between Postoperative Satisfaction and Other Variables
Univariate Analysis
Comparative analysis was performed to assess the characteristics of patients who reported the highest level of postoperative satisfaction with vision (rated their satisfaction as “Very Satisfied”) to all other patients (‘Others’ – patients who reported to be “Satisfied”, “Neither”, or “Dissatisfied”). The compared characteristics were demographics, visual acuity, response to other patient-reported outcomes (visual phenomena and dry eye symptoms), preoperative ocular co-pathology, postoperative adverse events, self-reported personality type and depression scores, and preoperative general health conditions.
Table 3 shows the summary of the comparison based on univariate analysis. There was no statistically significant difference between “Very Satisfied” and ‘Others’ in the gender distribution. The age analysis indicated slightly older preoperative age among “Very Satisfied” patients. Even though the age difference (3.4 years) between the two groups was not statistically significant (p = 0.11), “Very Satisfied” patients had a significantly higher proportion of patients ≥60 years (Table 3).
 |
Table 3 Comparison of Patients’ Characteristics Stratified by Postoperative Satisfaction With Vision |
The outcomes are indicative of better postoperative uncorrected visual acuity in “Very Satisfied” patients, although the difference did not reach a statistically significant level in univariate analysis (Table 3). When evaluating preoperative to postoperative change in corrected visual acuity, “Very satisfied” patients had a higher gain in CDVA (over five Snellen lines gain) compared to “Others” (3.5 Snellen lines gain; p = 0.02). The change in CDVA was calculated based on the outcome of one eye per patient (the eye with a higher visual acuity gain).
Visual phenomena analysis suggested that “Very Satisfied” patients had a higher percentage of patients not experiencing any postoperative visual phenomena at all (patients who rated their visual phenomena as “1” on a 7-point scale). Even though the differences did not reach statistical significance, the trend was consistent for all four examined visual side effects (glare, halo, starburst, ghosting/double vision; Table 3).
The same findings apply to postoperative patient-reported dry eye ratings. The data are indicative of a higher percentage of patients with no dry eye symptoms at all among “Very Satisfied” patients, but again, the differences did not reach statistical significance (Table 3).
Preoperative ocular co-pathologies included in the comparison were glaucoma, preoperatively reported only in 3 patients (3.1% of the cohort), and fundus pathology (dry age-related macular degeneration or epiretinal membrane present at least in one eye of the patient), which was preoperatively recorded in 30 patients (30.9% of the cohort). Interestingly, “Very Satisfied” patients had a higher prevalence of ocular co-pathologies than “Others”, although the differences in percentages were not statistically significant (Table 3).
Postoperative adverse events (AEs) used for comparison were cystoid macular edema (CME) and posterior capsular opacification (PCO). Postoperative CME in at least one eye of a patient was recorded in 6 patients (per-patient incidence 6.2%), and PCO in at least one eye was recorded in 3 patients (incidence 3.1%). The proportion of postoperative adverse events was higher among “Others” (Table 3), but the difference did not reach statistical significance due to the low count of both AEs. It is also important to note that none of these events was present on the day when the postoperative questionnaire was completed.
Self-reported personality types and depression scores were completed on preoperative visits. Patients reported to be “Very Satisfied” with vision were more likely to report “Easy going” personality type. The proportion of patients with self-reported “Easy going” personality was over 10% higher in the group of “Very Satisfied” patients, but the difference in proportions was not statistically significant (Table 3). There was a slight trend towards lower preoperative depression score in the group of “Very Satisfied” patients, but the difference was only minor and non-significant.
Although not statistically significant, the prevalence of preoperative general medical conditions was approximately 16% higher in the “Others” group. The three diseases with the highest percentage difference between “Very Satisfied” and “Others” were asthma, history of cancer treatment, and diabetes mellitus.
Multivariate Analysis
Variables presented in Table 3 were used in a multivariate logistic regression model to find the factors affecting the odds of being “Very Satisfied” with vision. The only two variables that were statistically significant in the regression model were age and postoperative uncorrected distance visual acuity.
For every decade increase in age (considering categories: <60, 60–69, 70–79, and 80–89 years old), the odds of being “Very Satisfied” with vision increased by a factor of 2.2 (confidence interval 1.3 to 3.9, p < 0.01). Additionally, the odds of being “Very Satisfied” with vision increased by a factor of 5.3 (confidence interval 1.2 to 29.2, p = 0.03) in patients with postoperative UDVA ≥20/25 in the better eye, compared to those with UDVA worse than 20/25.
Discussion
In this study, we evaluated satisfaction following bilateral implantation of a non-constant aberration-correcting monofocal intraocular lens. Cataract surgery is generally a very successful procedure. Even though complete spectacle independence is not typically achieved following a monofocal lens implantation, the visual gain and the clarity of vision after the extraction of a cataractous crystalline lens lead to high satisfaction rates.4 However, even among monofocal lenses, differences in optic design might affect the change in higher-order aberrations, contrast sensitivity, or how they perform under tilt or decentration.22 The monofocal IOL implanted in our case series is equipped with Zeiss Optics asphericity, characterized by a central power increment gradually transitioning toward the periphery. This optic concept has been linked to a better tolerance to misalignment, lower postoperative coma, and better intraocular stray light.23,24 However, general satisfaction with vision after cataract surgery is multifactorial and can be affected by many parameters other than the IOL design.
With regard to demographics, no association between gender and postoperative satisfaction was found in our cohort. Interestingly, we found a link between older age and higher satisfaction rates. The age-dependent satisfaction outcomes in the literature vary. Some studies postulate that younger age is typically associated with greater self-reported visual function improvement after cataract surgery,9,11 while other studies agree with our findings.15 Perhaps the interaction between the severity of cataracts and visual acuity gain could explain slightly higher satisfaction rates among older patients in our cohort.
Achieved visual acuity (VA) should be the most apparent variable associated with postoperative satisfaction with vision, although some studies indicated that objectively measured visual acuity does not always correlate with patient-reported visual functioning after cataract surgery.7 In the multivariate analysis, we found that postoperative uncorrected visual acuity increased the odds of being very satisfied with postoperative vision. The gain in corrected visual acuity signaled statistical significance in univariate analysis and could potentially become relevant if a larger sample of patients was available. The association between corrected visual acuity and patient satisfaction following cataract surgery has been previously reported in some studies. For example, Grimfors et al,9,11 using a dataset of over 10,000 cataract patients, found that improvement in self-reported visual function was greater in patients with low preoperative CDVA or high postoperative CDVA. Likewise, Mönestam et al14 found that patients with CDVA improvement of less than 0.3 logMAR had three times the odds of being dissatisfied with vision after cataract surgery. Thus, the gain in CDVA could be a valid factor in postoperative satisfaction after cataract surgery.
Monofocal IOLs generally have a much lower incidence of postoperative visual side effects compared to multifocal lenses.3,4 In our cohort, only three patients reported significant visual phenomena, and two of them had underlying conditions that could have potentially exacerbated the symptoms. Most of the patients had no visual dysphotopsia at all. We also found that “Very Satisfied” patients had a higher percentage of patients not experiencing any visual phenomena, albeit the difference was not statistically significant. Visual side effects have been commonly linked to postoperative dissatisfaction after cataract surgery.4,15 Yet, factors that affect or exacerbate visual phenomena in patients with monofocal IOLs would be worth exploring. Unfortunately, we could not perform such an analysis due to a low prevalence of visual phenomena in our cohort, but this topic deserves further attention in follow-up studies.
Dry eye and ocular discomfort symptoms have been a primary concern following corneal refractive procedures due to the direct impact of these procedures on central corneal nerves.25 However, the effect of dry eye disease on patient satisfaction following intraocular lens surgeries should not be underestimated.7,10,12 In one of our previous studies of an extended depth of focus IOL, we found a three-fold increase in dissatisfaction with increasing postoperative dry eye severity.26 In the current study, “Very Satisfied” patients had a higher proportion of patients not reporting any dry eye symptoms. Thus, we believe that dry eye disease requires thorough management in cataract surgery to mitigate the potential risks of dissatisfaction.
The presence of ocular comorbidities is one of the most commonly reported reasons for dissatisfaction or decreased self-reported visual function following cataract surgery with a monofocal IOL.5,6,8,9,11,14 Although we had one patient in whom dissatisfaction was directly related to fundus pathology, overall, we did not find a link between satisfaction and the presence of ocular comorbidities. The reason for such contradictory outcomes compared to the literature could be the severity of the disease and visual prognosis. Our patients mostly only had signs of dry macular degeneration, and their postoperative corrected visual acuity was good. Of all eyes in the cohort, 95.4% had postoperative CDVA 20/25 or better (Figure 1A), whereas other studies likely included patients with poorer visual prognosis or worse disease severity. We also have not found an association between postoperative adverse events and satisfaction, but their prevalence was low, and they were not present on the day when the postoperative questionnaire was completed, which was likely a contributing factor.
Factors unrelated to visual function are rarely considered in studies reporting satisfaction after cataract surgery. Although we did not find a clear relationship between preoperative self-reported depression scores and satisfaction, mainly due to a low number of patients reporting severe symptoms, depression has been linked to higher dissatisfaction rates following cataract surgery7 or corneal refractive procedures.27 We have also found a slightly lower percentage of patients reporting any general medical health condition among “Very Satisfied” patients. In a study of Szakats et al,7 health anxiety (patient’s worry about health, awareness of pain, or fear of consequences of having an illness) was more closely associated with patients’ postoperative satisfaction (in conjunction with other factors) than objective measures of visual acuity, but the study had a slightly different design. Personality type might be an interesting factor, and we have observed a slight trend towards higher satisfaction rates in “easy-going” patients. In previous multifocal IOL studies, personality traits, specifically neuroticism, were associated with reduced postoperative patient-perceived quality of vision and dissatisfaction.16,17 However, the neuroadaptation of patients with multifocal lenses is markedly different, and personality traits might have a more pronounced role in the satisfaction outcomes.
Although our study provides insights into the possible factors affecting the satisfaction of patients with monofocal intraocular lenses, there are some limitations that need to be acknowledged. The study is retrospective in nature, and any selection bias would be difficult to determine. There was a low variation in reported outcomes (eg, very few patients reported being dissatisfied), but from our experience, comparing the patients who report the highest level of satisfaction (“Very Satisfied”) to all the other patients leads to clinically meaningful analysis. However, a larger sample size would allow us to explore the relationships between variables in more detail. The inclusion of objective quality of vision measures in the analysis (eg, contrast sensitivity or higher order aberrations) would be valuable, but these were not available in our retrospective cohort.
Conclusion
Despite the limitations, the study highlighted some characteristics that are not usually considered as potential factors affecting satisfaction following cataract surgery. Except for the common ocular and visual metrics (eg, postoperative visual acuity level, visual phenomena, operative and postoperative adverse events), other factors such as patient personality traits, depression, or general health status could be considered in the analysis of patient satisfaction. Thus, the concept of this study could serve as a basis for further studies. The satisfaction with non-constant aberration-corrected monofocal IOL in our cohort was very high, with minimal visual phenomena. The dissatisfaction in the few patients was likely linked with postoperative recovery and patient pre-existing conditions rather than the IOL itself. Further studies are required to examine the predictors of postoperative satisfaction.
Disclosure
Steven Schallhorn is a Chief Medical Officer for Carl Zeiss Meditec and a chairman of medical advisory board for Optical Express. Stephen Hannan, Jan Venter, and David Teenan are employees of Optical Express. Julie Schallhorn received personal fees from Carl Zeiss Meditec, Allergan, Elios, Long Bridge, ViaLase, Vanda, and Forsight V6 and has a financial interest in Journey 1, Neurotrigger, and Novus Vision. The authors report no other conflicts of interest in this work.
References
1. Hood CT, Sugar A. Subjective complaints after cataract surgery: common causes and management strategies. Curr Opin Ophthalmol. 2015;26(1):45–49. doi:10.1097/ICU.0000000000000112
2. de Vries NE, Webers CA, Touwslager WR, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859–865. doi:10.1016/j.jcrs.2010.11.032
3. Calladine D, Evans JR, Shah S, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2012;2012(9):CD003169. doi:10.1002/14651858.CD003169.pub3
4. Calladine D, Evans JR, Shah S, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Sao Paulo Med J. 2015;133(1):68. doi:10.1590/1516-3180.20151331T2
5. Pesudovs K, Weisinger HS, Coster DJ. Cataract surgery and changes in quality of life measures. Clin Exp Optom. 2003;86(1):34–41. doi:10.1111/j.1444-0938.2003.tb03055.x
6. Monestam E, Wachtmeister L. Dissatisfaction with cataract surgery in relation to visual results in a population-based study in Sweden. J Cataract Refract Surg. 1999;25(8):1127–1134. doi:10.1016/s0886-3350(99)00135-2
7. Szakats I, Sebestyen M, Toth E, Purebl G. Dry Eye Symptoms, Patient-Reported Visual Functioning, and Health Anxiety Influencing Patient Satisfaction After Cataract Surgery. Curr Eye Res. 2017;42(6):832–836. doi:10.1080/02713683.2016.1262429
8. Chatziralli IP, Kanonidou E, Papazisis L. Frequency of fundus pathology related to patients’ dissatisfaction after phacoemulsification cataract surgery. Bull Soc Belge Ophtalmol. 2011; 2011(317):21–24.
9. Grimfors M, Lundstrom M, Hoijer J, Kugelberg M. Intraoperative difficulties, complications and self-assessed visual function in cataract surgery. Acta Ophthalmol. 2018;96(6):592–599. doi:10.1111/aos.13757
10. Labetoulle M, Rousseau A, Baudouin C. Management of dry eye disease to optimize cataract surgery outcomes: two tables for a daily clinical practice. J Fr Ophtalmol. 2019;42(8):907–912. doi:10.1016/j.jfo.2019.03.032
11. Grimfors M, Mollazadegan K, Lundstrom M, Kugelberg M. Ocular comorbidity and self-assessed visual function after cataract surgery. J Cataract Refract Surg. 2014;40(7):1163–1169. doi:10.1016/j.jcrs.2013.11.033
12. Porela-Tiihonen S, Kokki H, Kaarniranta K, Kokki M. Recovery after cataract surgery. Acta Ophthalmol. 2016;94(2):1–34. doi:10.1111/aos.13055
13. Conner-Spady BL, Sanmugasunderam S, Courtright P, McGurran JJ, Noseworthy TW. Steering Committee of the Western Canada Waiting List P. Determinants of patient satisfaction with cataract surgery and length of time on the waiting list. Br J Ophthalmol. 2004;88(10):1305–1309. doi:10.1136/bjo.2003.037721
14. Monestam E, Wachmeister L. Impact of cataract surgery on the visual ability of the very old. Am J Ophthalmol. 2004;137(1):145–155. doi:10.1016/s0002-9394(03)00900-0
15. Kirwan C, Nolan JM, Stack J, Moore TC, Beatty S. Determinants of patient satisfaction and function related to vision following cataract surgery in eyes with no visually consequential ocular co-morbidity. Graefes Arch Clin Exp Ophthalmol. 2015;253(10):1735–1744. doi:10.1007/s00417-015-3038-7
16. Pinheiro RL, Raimundo M, Gil JQ, et al. The influence of personality on the quality of vision after multifocal intraocular lens implantation. Eur J Ophthalmol. 2024;34(1):154–160. doi:10.1177/11206721231176313
17. Rudalevicius P, Lekaviciene R, Auffarth GU, Liutkeviciene R, Jasinskas V. Relations between patient personality and patients’ dissatisfaction after multifocal intraocular lens implantation: clinical study based on the five factor inventory personality evaluation. Eye. 2020;34(4):717–724. doi:10.1038/s41433-019-0585-x
18. Schallhorn SC, Teenan D, Venter JA, Schallhorn JM, Hannan SJ. Early Clinical Experience with a New Hydrophobic Acrylic Single-Piece Monofocal Intraocular Lens. Clin Ophthalmol. 2023;17:3419–3427. doi:10.2147/OPTH.S433530
19. Kroenke K, Spitzer RL, Williams JB. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–1292. doi:10.1097/01.MLR.0000093487.78664.3C
20. Dell SJ. The new Dell questionnaire: a tool for the complex preoperative consultation. Cataract & Refractive Surgery Today, May 2017. Available from: https://crstoday.com/wp-content/uploads/sites/4/2017/05/crst0517_cs_Dell.pdf.
21. Liou HL, Brennan NA. Anatomically accurate, finite model eye for optical modeling. J Opt Soc Am a Opt Image Sci Vis. 1997;14(8):1684–1695. doi:10.1364/josaa.14.001684
22. Deshpande R, Satijia A, Dole K, Mangiraj V, Deshpande M. Effects on ocular aberration and contrast sensitivity after implantation of spherical and aspherical monofocal intraocular lens - A comparative study. Indian J Ophthalmol. 2022;70(8):2862–2865. doi:10.4103/ijo.IJO_19_22
23. Yan W, Auffarth GU, Khoramnia R, Labuz G. Blue-Light Filtering Monofocal Intraocular Lenses: a Study on Optical Function and Tolerance to Misalignment. J Refract Surg. 2024;40(2):e79–e88. doi:10.3928/1081597X-20240112-02
24. Liu Y, Zhao J, Hu Y, Li B, Wang J, Zhang J. Comparison of the Visual Performance after Implantation of Three Aberration-correcting Aspherical Intraocular Lens. Curr Eye Res. 2021;46(3):333–340. doi:10.1080/02713683.2020.1798467
25. Nair S, Kaur M, Sharma N, Titiyal JS. Refractive surgery and dry eye - An update. Indian J Ophthalmol. 2023;71(4):1105–1114. doi:10.4103/IJO.IJO_3406_22
26. Schallhorn SC, Hettinger KA, Teenan D, Venter JA, Hannan SJ, Schallhorn JM. Predictors of Patient Satisfaction After Refractive Lens Exchange With an Extended Depth of Focus IOL. J Refract Surg. 2020;36(3):175–184. doi:10.3928/1081597X-20200211-01
27. Morse JS, Schallhorn SC, Hettinger K, Tanzer D. Role of depressive symptoms in patient satisfaction with visual quality after laser in situ keratomileusis. J Cataract Refract Surg. 2009;35(2):341–346. doi:10.1016/j.jcrs.2008.10.046
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.