")
Back to Journals » Clinical Interventions in Aging » Volume 20
Preoperative Prognostic Nutritional Index Is a Predictive Factor for Postoperative Delirium in Elderly Patients with Femoral Neck Fracture
Received 31 January 2025
Accepted for publication 29 May 2025
Published 2 July 2025 Volume 2025:20 Pages 941—950
DOI https://doi.org/10.2147/CIA.S518366
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Yuansheng Xu,1 Yongjun Luo2
1Department of Orthopedics, The Affiliated Jinling Hospital of Nanjing University, Nanjing, Jiangsu, People’s Republic of China; 2Department of Orthopedics, The Fourth Affiliated Hospital of Soochow University, Suzhou, Jiangsu, 215123, People’s Republic of China
Correspondence: Yongjun Luo, Email [email protected]
Objective: This study aimed to investigate the potential risk factors of postoperative delirium (POD) in elderly patients (≥ 65 years old) undergoing femoral neck fracture (FNF) surgery, and explore whether preoperative prognostic nutritional index (PNI) could predict the occurrence of POD.
Methods: A total of 260 cases with FNF were included in this study at The Affiliated Jinling Hospital of Nanjing University from May 2018 and May 2024. The baseline characteristics were recorded. The receiver operating characteristic (ROC) curve analysis was developed to evaluate the diagnostic ability of preoperative PNI for POD. LASSO regression and multivariate logistic regression analyses were used to identify the risk factors for POD.
Results: Eighty-one of the 260 cases with FNF suffered POD with an incidence of 31.2%. Patients with POD showed lower Mini-Mental State Examination (MMSE) score (P=0.011), lymphocyte count (P=0.002), albumin level (P=0.011), and PNI level (P< 0.001) than those in non-POD group. ROC curve analysis indicated that PNI was a good predictor for POD with an area under the curve (AUC) value of 0.708 (95% CI: 0.648– 0.762, P< 0.001); the sensitivity and specificity were 79.01 and 60.89, respectively. LASSO regression analysis identified eleven key variables including gender, age, body mass index, diabetes mellitus, surgery duration, anesthesia duration, fracture position, neutrophil, lymphocyte, PNI, and MMSE score. Multivariate logistic regression analysis showed that MMSE score < 27, BMI > 23.9 kg/m2, and PNI < 45.45 were independent risk factors of POD.
Conclusion: In conclusion, preoperative PNI is a significant predictor for POD in elderly patients after FNF surgery.
Keywords: postoperative delirium, femoral neck fracture, prognostic nutritional index, predictor
Introduction
As the aging global population increases, femoral neck fracture (FNF) is an arising problem in elderly patients due to impaired walking ability and bone fragility.1 Globally, nearly 1.3–2.2 million FNFs occur every year.2 FNF is associated with high disability and mortality, which could lead to the reduction life quality and other healthy complications.3,4 The treatment methods for FNF include hemiarthroplasty, total hip arthroplasty, and internal fixation.5 Complications occur usually after FNF surgery,6 and postoperative delirium (POD) emerges as a significant issue for patients with FNF.7
Delirium is a common syndrome characterized by disturbance of consciousness. Patients with FNF are vulnerable to delirium. POD is one of the most common complications of FNF in elderly patients, which could prolong the length of hospital stay time and increase the burden of hospitalization expense.8 A meta-analysis showed that the pooled incidence of POD after hip fracture was 16.93% among adult patients.9 Accumulating evidence suggested that malnutrition was associated with the risk of delirium.10–12 A meta-analysis indicated that preoperative malnutrition was related with POD in surgical patients.13 Mazzola et al observed an association between the risk of POD and malnutrition following hip fracture surgery in elderly adults.14
Prognostic nutritional index (PNI), a nutritional indicator, is calculated according to serum albumin concentration and total lymphocyte count. PNI could assess the nutritional status of surgical patients. PNI is regarded to be a significant predictor for postoperative complications,15,16 including POD.17,18 In this study, we intended to 1) identify potential risk factors of POD; 2) explore whether preoperative PNI could predict POD in elderly patients with FNF.
Materials and Methods
This study was conducted at The Affiliated Jinling Hospital of Nanjing University from May 2018 and May 2024. A total of 260 patients with FNF were included in this study. Inclusion criteria of cases were as follows: (1) age ≥65 years, (2) consent to participate this study; and (3) received the surgical treatment of FNF. Patients with the following conditions were excluded: (1) with a history of psychiatric disorders including depression, dementia, delirium, and so on; (2) using antipsychotic medications before surgery; (3) refused to participate in the study; (4) with cancers or infectious diseases which may affect the levels of albumin and lymphocyte; and (5) with incomplete data. This study was approved by the ethics committee of The Affiliated Jinling Hospital of Nanjing University. Informed consent form was obtained from all participants. This study was in line with the Declaration of Helsinki.
We collected all the patients’ baseline characters, including age, gender, body mass index (BMI), smoking, drinking, diabetes mellitus, and hypertension. Clinical parameters including surgery duration, anesthesia duration, American Society of Anesthesiologists (ASA) grade, Mini-Mental State Examination (MMSE) score, and fracture position were recorded. Neutrophil, lymphocyte, and albumin were also collected before surgery.
Definition of PNI
The PNI was calculated by the following formula: PNI = albumin (g/L) + 5 × lymphocyte count (109/L).19
Diagnosis of POD
POD was diagnosed according to the criteria of Confusion Assessment Method (CAM).20 The CAM score included four items, which were described as follows: (1) dramatic fluctuations in mental status; (2) inattention, (3) confusion or incoherence of thinking, and (4) alternations of consciousness. POD was evaluated twice daily (morning and afternoon) from the first day to the seventh day postoperatively. There were no procedures for preventing and managing delirium in this study.
Statistical Analysis
Statistical analyses were performed using MedCalc software, R software (version 4.1.3), and SPSS 21.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were presented as numbers with percentage; continuous variables were shown as median with interquartile range or mean ± standard deviation as appropriate. The Chi-square test or Fisher exact test was used to analyze categorical variables; Mann–Whitney U-test or Student’s t-test was used to calculate continuous variables as appropriate. The areas under the receiver operating characteristic curve (AUC) of PNI were calculated; sensitivity, specificity, and Youden index were also evaluated. LASSO regression and multivariate logistic regression analyses were used for identifying the risk factors for POD. A two- sided P < 0.05 was considered significant.
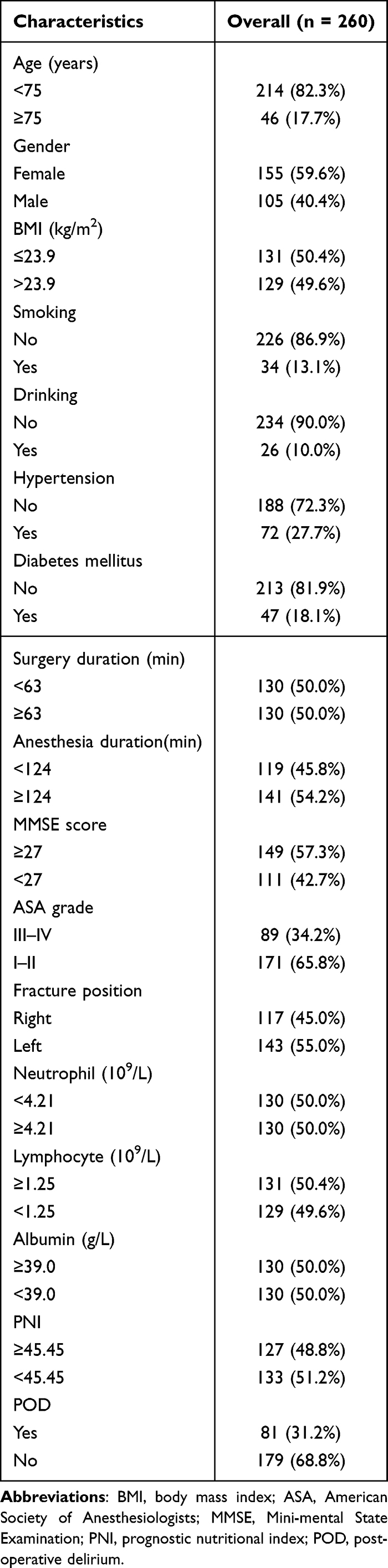 |
Table 1 Baseline Characteristics of 260 Patients with Femoral Neck Fracture |
 |
Table 2 Comparison of Characteristics Between POD and Non-POD Groups |
Results
Baseline Characteristics
Totally, 260 elderly patients aged ≥65 years old were included in this study (Figure 1). Among 260 cases, 81 (31.2%) POD cases occurred (Table 1). There were 105 (40.4%) males and 155 (59.6%) females. Patients with FNF were divided into POD and non-POD group. The detailed characteristics of cases with POD or not are presented in Table 2. Patients with POD showed lower MMSE score (P=0.011), lymphocyte count (P=0.002), albumin level (P=0.011), and PNI level (P<0.001) than those in non-POD group. Regarding age, gender, BMI, smoking, drinking, diabetes mellitus, hypertension, surgery duration, anesthesia duration, ASA grade, fracture position, and neutrophil, no significant differences were observed (all P>0.05). The average day after the operation that delirium developed was 2.81 days.
 |
Table 3 ROC Curve of Preoperative PNI for Predicting the Postoperative Delirium |
 |
Figure 1 The flow chart of this study. |
Diagnostic Ability of Preoperative PNI for POD
The diagnostic ability of preoperative PNI was evaluated (Table 3). ROC curve analysis indicated that PNI was a good predictor for POD with an area under the curve (AUC) value of 0.708 (95% CI: 0.648–0.762, P<0.001, Figure 2). The cut-off value of PNI was 45.45; the sensitivity and specificity were 79.01 and 60.89, respectively. The Youden index was 0.3991. Totally, the diagnostic ability for POD were moderate.
 |
Figure 2 The diagnostic abilities of preoperative values of preoperative PNI in predicting POD among patients following THA. |
Risk Factors of POD
To explore independent risk factors for POD, LASSO regression analysis was firstly used. Through this rigorous selection process, eleven key variables were identified: gender, age, BMI, diabetes mellitus, surgery duration, anesthesia duration, fracture position, neutrophil, lymphocyte, PNI, and MMSE score (Figure 3A and B). Next, we used these above mentioned variables to conduct the multivariate logistic regression. Multivariate logistic regression analysis showed that MMSE score < 27, BMI > 23.9 kg/m2, and PNI < 45.45 were independent risk factors of POD; gender, age, diabetes mellitus, surgery duration, anesthesia duration, fracture position, neutrophil, and lymphocyte were not risk factors for POD (Table 4). In conclusion, preoperative PNI was a significant predictor for POD in elderly patients after FNF surgery.
 |
Table 4 Multiple Logistic Regression Analysis of Risk Factors for Postoperative Delirium |
 |
Figure 3 Predictor selection using the LASSO logistic regression analysis. (A) Cross-validation for the predictor selection of optimal lambda value in the LASSO model. (B) Lasso coefficient profiles of the selected predictors. |
Discussion
Up to date, the pathophysiological mechanism of POD is still unclear. It was shown that delirium might be caused by cerebral neuronal damage, as a consequence of hypoxia, hypotension, oxidative stress, embolisms and so on.21–24 Malnutrition was reported to be correlated with a high risk of POD in surgery.12 Nutrient replenish may help patients with delirium to accelerate rehabilitation.25,26
PNI, a new nutritional marker, was determined by serum albumin level and lymphocyte count. PNI was significantly associated with the risk of postoperative complications.27–29 Tei et al showed that preoperative PNI was an independent risk factor for POD for elderly patients with colorectal cancer.30 However, a meta-analysis revealed that preoperative PNI was not a risk factor for POD in patients with colorectal carcinoma.31 In addition, Ida et al did not observe an association between PNI level and the risk of POD following abdominal surgery.32 For noncardiac surgery, a study showed that preoperative PNI did not correlate with the risk of POD in elderly patients.17 Song et al indicated that PNI was a significant predictor for POD in patients undergoing non-neurosurgery and non-cardiac surgery.18
 |
Table 5 The Characteristics of the Studies About the Association Between PNI and the Risk of POD in Orthopedic Surgery |
Regarding orthopedic surgery, several studies investigated the association between PNI and the risk of POD. Table 5 summarizes the details of these studies.19,33–37 Oe et al from Japan indicated that preoperative PNI was associated with the risk of POD among patients with adult spinal deformity,33 which was consistent with the findings of another Japanese study in elderly patients (≥75 years) undergoing spinal surgery.35 Another study uncovered that preoperative PNI was a useful factor for predicting POD after primary total joint arthroplasty.36 Mi et al also observed that preoperative PNI was associated with the risk of POD in elderly patients with hip fractures,37 which was also replicated in another Chinese study.19 Xing et al found that preoperative PNI level was related to the risk of POD in elderly patients after hip fracture surgery.34 It is of note that they showed that PNI ≥ 47.45 was a risk factor for POD in Table 5,34 indicating that low PNI was not a risk factor for POD. We think the data need to be taken with caution.34 A recent meta-analysis showed that preoperative PNI was not related to with risk of POD in patients undergoing orthopedic surgery.38 The meta-analysis only included three papers about orthopedic surgery;33,35,36 a study was not included in their meta-analysis,34 which underpowered the credibility of this meta-analysis.38
In this study, we found that preoperative PNI was a predictive factor for POD in elderly FNF patients, which is consistent with the findings of other studies.19,34,36,37 To the knowledge, this is the first study to observe an association between preoperative PNI and the risk of POD among elderly FNF patients. In addition, this study showed that MMSE score (<27) and BMI (>23.9 kg/m2) were also risk factors for POD. For MMSE score, Mi et al indicated that MMSE was a risk factor for POD in elderly patients with hip fractures,37 while Xing et al did not find it.34 Age was a recognized risk factor for delirium.24 In this study, our data suggested that age was not a risk factor for POD, which was inconsistent with other studies.19,34,36 Mi et al also showed that age was not associated with the risk of POD.37 We assumed that varied sample sizes, different definitions of POD, and clinical heterogeneity could be potential reasons to explain the different results of age.
POD not only caused significant cognitive impairment but also resulted in prolonged hospital stay time, elevated economic burden, and increased mortality rates for patients.39–42 A Japanese study showed that managing comorbidities could improve long-term postoperative clinical outcomes of proximal femur fracture.43 For perioperative managements for FNF patients, surgeons paid little attention to POD. Up to now, the efficacy of pharmacological interventions to prevent delirium remains uncertain. Current practice guidelines indicated that routine use of medication intervention to treat delirium was not recommended.44 However, studies provided evidence that dexmedetomidine could be regarded as a potential treatment for POD.45–47 Obviously, further studies are urgently needed on drugs for treating delirium.
According to our study, preoperative PNI should be recommended as a routine assessment to identify potential POD patients among elderly FNF individuals. PNI should be assessed dynamically to prevent the occurrence of POD. Effective interventions such as albumin supplement may reduce the incidence of POD for elderly FNF patients. In the future, prospective studies with large sample sizes need to verify our hypothesis.
This study had some limitations. One, it was a retrospective study and selection bias may not be evitable. Two, the sample size was not large enough in this study. Three, intraoperative and postoperative factors were not investigated. Four, we evaluated the POD among elderly patients aged ≥65 years. Patients aged <65 years should be included in further studies. Five, delirium was inherently fluctuating, and we did not evaluate the delirium of patients at night. Six, due to this study was retrospective, the data we collected were not comprehensive enough, which may have an impact on the final conclusions. Last but not the least, the potential mechanisms why preoperative PNI level could predict the occurrence of POD were unclear.
Conclusions
Taken together, this study shows that low preoperative PNI level is an independent predictive factor for POD in elderly patients after FNF surgery. PNI could help surgeons to do perioperative management to prevent the occurrence of POD in elderly patients with FNF.
Acknowledgment
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Funding
The study was supported by Suzhou Gusu Health Talent Program Talent Research Project (GSWS2022125), Suzhou Industrial Park Healthcare Talent Support Initiative (2024) 76, and National Natural Science Foundation of China (Grant No. 82102559).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jianbo J, Ying J, Xinxin L, Lianghao W, Baoqing Y, Rongguang A. Hip hemiarthroplasty for senile femoral neck fractures: minimally invasive SuperPath approach versus traditional posterior approach. Injury. 2019;50(8):1452–1459. doi:10.1016/j.injury.2019.06.006
2. Sekeitto AR, Sikhauli N, van der Jagt DR, Mokete L, Pietrzak JRT. The management of displaced femoral neck fractures: a narrative review. EFORT Open Rev. 2021;6(2):139–144. doi:10.1302/2058-5241.6.200036
3. Investigators H, Bhandari M, Einhorn TA, et al. Total Hip Arthroplasty or Hemiarthroplasty for Hip Fracture. N Engl J Med. 2019;381(23):2199–2208. doi:10.1056/NEJMoa1906190
4. Liodakis E, Antoniou J, Zukor DJ, Huk OL, Epure LM, Bergeron SG. Major Complications and Transfusion Rates After Hemiarthroplasty and Total Hip Arthroplasty for Femoral Neck Fractures. J Arthroplasty. 2016;31(9):2008–2012. doi:10.1016/j.arth.2016.02.019
5. Zelle BA, Salazar LM, Howard SL, Parikh K, Pape HC. Surgical treatment options for femoral neck fractures in the elderly. Int Orthop. 2022;46(5):1111–1122. doi:10.1007/s00264-022-05314-3
6. Liang W, Qin G, Yu L, Wang Y. Reducing complications of femoral neck fracture management: a retrospective study on the application of multidisciplinary team. BMC Musculoskelet Disord. 2023;24(1):338. doi:10.1186/s12891-023-06455-1
7. Flikweert ER, Wendt KW, Diercks RL, et al. Complications after Hip fracture surgery: are they preventable? Eur J Trauma Emerg Surg. 2018;44(4):573–580. doi:10.1007/s00068-017-0826-2
8. Kitsis P, Zisimou T, Gkiatas I, et al. Postoperative Delirium and Postoperative Cognitive Dysfunction in Patients with Elective Hip or Knee Arthroplasty: a Narrative Review of the Literature. Life. 2022;12(2). doi:10.3390/life12020314
9. Wu J, Yin Y, Jin M, Li B. The risk factors for postoperative delirium in adult patients after Hip fracture surgery: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2021;36(1):3–14. doi:10.1002/gps.5408
10. Igwe EO, Ding P, Charlton KE, Nealon J, Traynor V. Association between Malnutrition and Delirium in Older Chronic Kidney Disease Patients Admitted to Intensive Care Units: a Data Linkage Study. J Nutr Health Aging. 2023;27(7):571–577. doi:10.1007/s12603-023-1938-5
11. Liang X, Li X, Cheng H, et al. Elderly patients with dysphagia in the intensive care unit: association between malnutrition and delirium. Nurs Crit Care. 2024;29(6):1253–1262. doi:10.1111/nicc.13136
12. Moellmann HL, Alhammadi E, Boulghoudan S, et al. Risk of sarcopenia, frailty and malnutrition as predictors of postoperative delirium in surgery. BMC Geriatr. 2024;24(1):971. doi:10.1186/s12877-024-05566-1
13. Dong B, Wang J, Li P, Li J, Liu M, Zhang H. The impact of preoperative malnutrition on postoperative delirium: a systematic review and meta-analysis. Perioper Med. 2023;12(1):55. doi:10.1186/s13741-023-00345-9
14. Mazzola P, Ward L, Zazzetta S, et al. Association Between Preoperative Malnutrition and Postoperative Delirium After Hip Fracture Surgery in Older Adults. J Am Geriatr Soc. 2017;65(6):1222–1228. doi:10.1111/jgs.14764
15. Kudou K, Kajiwara S, Motomura T, et al. Risk Factors of Postoperative Complication and Hospital Mortality after Colorectal Perforation Surgery. J Anus Rectum Colon. 2024;8(2):118–125. doi:10.23922/jarc.2023-056
16. Xu M, Zhang L, Wang J, et al. Pre-operative prognostic nutrition index and post-operative pneumonia in aneurysmal subarachnoid hemorrhage patients. Front Neurol. 2023;14:1045929. doi:10.3389/fneur.2023.1045929
17. Liu H, Dai M, Guan H, et al. Preoperative Prognostic Nutritional Index Value is Related to Postoperative Delirium in Elderly Patients After Noncardiac Surgery: a Retrospective Cohort Study. Risk Manag Healthc Policy. 2021;14:1–8. doi:10.2147/RMHP.S280567
18. Song YX, Wang Q, Ma YL, et al. Preoperative prognostic nutritional index predicts postoperative delirium in aged patients after surgery: a matched cohort study. Gen Hosp Psychiatry. 2024;86:58–66. doi:10.1016/j.genhosppsych.2023.11.013
19. Hu W, Song Z, Shang H, Wang J, Hao Y. Inflammatory and nutritional markers predict the risk of post-operative delirium in elderly patients following total Hip arthroplasty. Front Nutr. 2023;10:1158851. doi:10.3389/fnut.2023.1158851
20. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948. doi:10.7326/0003-4819-113-12-941
21. Maldonado JR. Neuropathogenesis of delirium: review of current etiologic theories and common pathways. Am J Geriatr Psychiatry. 2013;21(12):1190–1222. doi:10.1016/j.jagp.2013.09.005
22. Oh ES, Fong TG, Hshieh TT, Inouye SK. Delirium in Older Persons: advances in Diagnosis and Treatment. JAMA. 2017;318(12):1161–1174. doi:10.1001/jama.2017.12067
23. Rasmussen LS, Christiansen M, Rasmussen H, Kristensen PA, Moller JT. Do blood concentrations of neurone specific enolase and S-100 beta protein reflect cognitive dysfunction after abdominal surgery?ISPOCD Group. Br J Anaesth. 2000;84(2):242–244. doi:10.1093/oxfordjournals.bja.a013410
24. Wilson JE, Mart MF, Cunningham C, et al. Delirium. Nat Rev Dis Primers. 2020;6(1):90. doi:10.1038/s41572-020-00223-4
25. Deeth S, Stevens S, Bell J, Mudge A. Nutrition care for older adults with delirium: a scoping review. J Clin Nurs. 2024;33(10):3886–3904. doi:10.1111/jocn.17069
26. Xie S, Wu Q. Geriatric nutritional risk index predicts postoperative delirium in elderly: a meta-analysis. Saudi Med J. 2024;45(9):869–875. doi:10.15537/smj.2024.45.9.20240216
27. Imai T, Asada Y, Morita S, et al. Preoperative prognostic nutritional index as a method to predict postoperative complications after major head and neck surgery with free tissue transfer reconstruction. Jpn J Clin Oncol. 2020;50(1):29–35. doi:10.1093/jjco/hyz133
28. Qi Q, Song Q, Cheng Y, Wang N. Prognostic Significance of Preoperative Prognostic Nutritional Index for Overall Survival and Postoperative Complications in Esophageal Cancer Patients. Cancer Manag Res. 2021;13:8585–8597. doi:10.2147/CMAR.S333190
29. Zhang C, Zhang T, Shen Z, Zhong J, Wang Z. Preoperative Prognostic Nutritional Index and Nomogram for Predicting the Risk of Postoperative Complications in Patients With Crohn’s Disease. Clin Transl Gastroenterol. 2023;14(3):e00563. doi:10.14309/ctg.0000000000000563
30. Tei M, Ikeda M, Haraguchi N, et al. Risk factors for postoperative delirium in elderly patients with colorectal cancer. Surg Endosc. 2010;24(9):2135–2139. doi:10.1007/s00464-010-0911-7
31. Yang Z, Wang XF, Yang LF, Fang C, Xk G, Hw G. Prevalence and risk factors for postoperative delirium in patients with colorectal carcinoma: a systematic review and meta-analysis. Int J Colorectal Dis. 2020;35(3):547–557. doi:10.1007/s00384-020-03505-1
32. Ida M, Takeshita Y, Kawaguchi M. Preoperative serum biomarkers in the prediction of postoperative delirium following abdominal surgery. Geriatr Gerontol Int. 2020;20(12):1208–1212. doi:10.1111/ggi.14066
33. Oe S, Togawa D, Yamato Y, et al. Preoperative Age and Prognostic Nutritional Index Are Useful Factors for Evaluating Postoperative Delirium Among Patients With Adult Spinal Deformity. Spine. 2019;44(7):472–478. doi:10.1097/BRS.0000000000002872
34. Xing H, Xiang D, Li Y, Ji X, Xie G. Preoperative prognostic nutritional index predicts postoperative delirium in elderly patients after Hip fracture surgery. Psychogeriatrics. 2020;20(4):487–494. doi:10.1111/psyg.12511
35. Onuma H, Inose H, Yoshii T, et al. Preoperative risk factors for delirium in patients aged >/=75 years undergoing spinal surgery: a retrospective study. J Int Med Res. 2020;48(10):300060520961212. doi:10.1177/0300060520961212
36. Chen J, Zheng C, Zhong J, et al. Preoperative prognostic nutritional index is useful factor for predicting postoperative delirium after primary total joint arthroplasty. BMC Musculoskelet Disord. 2021;22(1):778. doi:10.1186/s12891-021-04626-6
37. Mi X, Jia Y, Song Y, et al. Preoperative prognostic nutritional index value as a predictive factor for postoperative delirium in older adult patients with Hip fractures: a secondary analysis. BMC Geriatr. 2024;24(1):21. doi:10.1186/s12877-023-04629-z
38. Hung KC, Chiu CC, Hsu CW, et al. Association of preoperative prognostic nutritional index with risk of postoperative delirium: a systematic review and meta-analysis. Front Med Lausanne. 2022;9:1017000. doi:10.3389/fmed.2022.1017000
39. Kinchin I, Mitchell E, Agar M, Trepel D. The economic cost of delirium: a systematic review and quality assessment. Alzheimers Dement. 2021;17(6):1026–1041. doi:10.1002/alz.12262
40. Mattison MLP. Delirium. Ann Intern Med. 2020;173(7):ITC49–ITC64. doi:10.7326/AITC202010060
41. Wu P, Yang Y, Yuan A, Wang Y, Zhang Y. Postoperative delirium increases follow-up mortality following Hip arthroplasty in older patients with femoral neck fracture. Australas J Ageing. 2024;43(4):715–724. doi:10.1111/ajag.13366
42. Yokoyama C, Yoshitnai K, Ogata S, Fukushima S, Matsuda H. Effect of postoperative delirium after cardiovascular surgery on 5-year mortality. JA Clin Rep. 2023;9(1):66. doi:10.1186/s40981-023-00658-0
43. Hashimoto K, Shinyashiki Y, Ohtani K, Kakinoki R, Akagi M. How proximal femur fracture patients aged 65 and older fare in survival and cause of death 5+ years after surgery: a long-term follow-up. Medicine. 2023;102(20):e33863. doi:10.1097/MD.0000000000033863
44. Devlin JW. Pharmacologic Treatment Strategies for Delirium in Hospitalized Adults: past, Present, and Future. Semin Neurol. 2024;44(6):762–776. doi:10.1055/s-0044-1791246
45. Meng C, Wang D, Zhao Y, et al. Dexmedetomidine for delirium prevention in adult patients following cardiac surgery: a meta-analysis of randomized controlled trials. J Cardiothorac Surg. 2025;20(1):110. doi:10.1186/s13019-025-03360-7
46. Sun J, Wang D, Zhao Y, et al. Intravenous dexmedetomidine for delirium prevention in elderly patients following orthopedic surgery: a meta-analysis of randomized controlled trials. BMC Pharmacol Toxicol. 2025;26(1):8. doi:10.1186/s40360-025-00841-2
47. Wu H, Wu P, Xiang L, et al. Effect of different intranasal dexmedetomidine doses on pediatric postoperative delirium and agitation: network meta-analysis. Pediatr Res. 2025. doi:10.1038/s41390-025-03851-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.