")
Back to Journals » Clinical Ophthalmology » Volume 19
Preoperative Retinal Detachment Variables Causing Macular Detachment
Authors Nishimura S , Okuda T, Higashide T, Sugiyama K
Received 9 October 2024
Accepted for publication 10 December 2024
Published 3 January 2025 Volume 2025:19 Pages 11—18
DOI https://doi.org/10.2147/OPTH.S499960
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shunsuke Nishimura, Tetsuhiko Okuda, Tomomi Higashide, Kazuhisa Sugiyama
Department of Ophthalmology, Kanazawa University Graduate School of Medical Science, Kanazawa, Japan
Correspondence: Tetsuhiko Okuda, Department of Ophthalmology, Kanazawa University Graduate School of Medical Science, 13-1 Takara-machi, Kanazawa, Ishikawa Prefecture, 920-8641, Japan, Tel +81-76-265-2403, Fax +81-76-222-9660, Email [email protected]
Purpose: The factors that contribute to the progression of macular involvement in RRD have not been extensively investigated. The purpose of this study is to evaluate the association between the preoperative characteristics and macular status of the eyes with rhegmatogenous retinal detachment (RRD).
Methods: This is a retrospective cohort study. All patients with RRDs who underwent initial pars plana vitrectomy or scleral buckling were included. Patients with RRD and macular hole retinal detachment, traumatic RD, proliferative diabetic retinopathy, proliferative vitreoretinopathy grade C or higher, diabetic retinopathy, or retinal vein occlusion were excluded. High myopia was defined as an axial length > of 26.5 mm.
Results: A total of 1026 eyes of 1026 patients (mean, 55.4± 15.5 years) were included. There was a significant difference in the male (68.4%) to female (31.6%) ratio (the chi-squared test: P < 0.001). A total of 351 patients (34.2%) had high myopia. The 50– 59 years age group had the highest number of eyes with high myopia. The proportion of highly myopic eyes in the 40– 49 years group was the highest. Multiple logistic regression analysis indicated that prior cataract extraction and shorter axial length (≤ 24.5 mm) were significantly associated with macula-off RRD (P = 0.018, P = 0.043, respectively). Superior and temporal retinal breaks significantly increased and superior nasal retinal breaks significantly decreased the odds ratio of macular detachment (P = 0.018, P < 0.001, and P < 0.001, respectively).
Conclusion: Previous cataract extraction, shorter axial length, and superior and temporal retinal breaks are important risk factors for macular detachment.
Keywords: axial length, high myopia, macular detachment, rhegmatogenous retinal detachment, scleral buckling, vitrectomy
Introduction
The epidemiology of rhegmatogenous retinal detachment (RRD) has been studied extensively. Previous studies have revealed that male sex,1–5 increasing age,1,2 cataract surgery,6 right eye,1 prior history of RRD in the fellow eye,2,7 and myopia2,7 are risk factors for RRD. According to Van Leeuwen et al,8 the rise in the occurrence of primary RRD in the Netherlands cannot be solely attributed to a shift in age distribution or an increase in cataract surgery rates. They highlighted the possible contribution of a myopic shift in the Dutch population to the higher RRD incidence. Concomitant high myopia (>-6.0D) has been reported in 10.51%,3 33.8%,9 and 23%10 of patients with RRD, and the proportion of individuals with high myopia in the control group was significantly higher.11 Kim et al12 reported that 31% of patients with RRD had high myopia with axial lengths of ≥26 mm. It has also been reported that high myopia (≥-6 diopters) is more prevalent among patients with bilateral (57.1%) than among those with unilateral (32.4%) RRD.9
Macular involvement in RRD is likely to result in poor visual outcomes. Eyes with macula-off RRD have postoperative metamorphopsia more frequently than those with macula-on RRD.13 Therefore, performing surgery for RRD before it extends to the macula has important prognostic implications for anatomical and visual outcomes. In addition, cataract surgery has been identified as one of the major risk factors for RRD.6 Potic et al14 reported that pseudophakia and axial lengths less than 25 mm are independent predictive factors for macular involving RRD. However, the factors that contribute to the progression of macular involvement in RRD have not been extensively investigated.
The objective of this study was to investigate the relationship between the preoperative characteristics of patients and the condition of the macula in eyes affected by RRD at Kanazawa University Hospital, particularly the distribution of highly myopic eyes and the factors influencing macular detachment.
Methods
Data Collection
This retrospective cohort study included patients who underwent initial pars plana vitrectomy or scleral buckling for RRD at Kanazawa University Hospital between January 2012 and December 2021. RRD was defined as retinal detachment with a retinal break detected before or during surgery. Patients with RRD and macular hole retinal detachment (MHRD), traumatic RD, proliferative diabetic retinopathy, proliferative vitreoretinopathy grade C or higher, diabetic retinopathy, or retinal vein occlusion were excluded. Preoperative information, including age, sex, axial length, presence of macular detachment, history of cataract surgery, and location of retinal breaks, was obtained from the electronic medical records or surgical reports. The locations of the retinal breaks were categorized into eight sectors. The number and types of breaks were not investigated. For bilateral RRD cases, only the first eye was utilized for statistical analysis. An analysis was conducted on a total of 1026 eyes belonging to 1026 patients. The study protocol was approved by the ethics committee of Kanazawa University Hospital and adhered to the principles of the Declaration of Helsinki. Written informed consent was obtained from all the patients.
Clinical Examination
After the patients were diagnosed with RRD, the axial length was measured using A-mode ultrasonography (UD-1000; Tomey Corporation, Japan) or OA-2000 (Tomey Corporation, Japan) as part of routine preoperative examinations. If the length was measured using A-mode ultrasonography for eyes with macular detachment, it was measured to the retinal pigment epithelium because the neurosensory retina was detached. Both eyes were assessed, and the mean values were used for analysis. High myopia was defined as an axial length of > 26.5 mm. According to Flitcroft DI et al,15 high myopia is defined as a spherical equivalent refractive error ≤ 6.00 D, however, only the axial length was used in this study because the presence of macular detachment may affect the refractive error.
Statistical Analyses
The mean scores and standard deviations were calculated for age and axial length. The differences in axial length across the age groups and sexes were compared using a generalized linear mixed model analysis with Bonferroni post hoc analysis. An Independent t-test and Mann–Whitney-U test were performed to compare the axial lengths and ages of the eyes with and without macula-off RRD. The chi-squared test was used to compare the proportions of male patients with high myopia who had macula-off and macula-on RRD and the proportion of cases of high myopia for various age groups and both sexes using Bonferroni post-hoc analysis. A multivariate logistic regression analysis was conducted to identify factors associated with macular-off RRD. Explanatory variables included age, sex, preoperative lens status, and axial length. For axial length, three variables were created: a continuous variable and categorical variables splitting AXL at 26.5 mm or 24.5 mm. These were entered into separate multivariate models, and the best model was selected according to the Akaike’s information criterion (AIC). Another multivariate logistic model was created to identify the retinal break location associated with macula-off RRD. Statistical significance was set at P < 0.05. All statistical analyses were conducted using SPSS for Windows (version 29.0; SPSS Inc., Chicago, IL, USA).
Results
There were 1026 eyes from 1026 patients with RRD who received initial pars plana vitrectomy or scleral buckling between January 2012 and December 2021 at Kanazawa University Hospital. Table 1 shows the demographic information. The age range of the patients was from 10 to 87 years, with an average age of 54.4 ± 15.5 years. Fifty-four patients (5.3%) had bilateral RRD, and 351 eyes (34.2%) had high myopia. RRD was more prevalent in males (702 eyes, 68.4%) than in females (324 eyes, 31.6%; P < 0.001).
 |
Table 1 Demographic Data of the Patients Who Underwent Rhegmatogenous Retinal Detachment Surgery |
Age and Axial Length Distribution
The axial length varied between 20.48 and 32.99 mm, with an average length of 25.71 ± 1.85 mm (Figure 1). It was found that on average, the axial length was significantly longer in males compared to females (P < 0.001, 25.91 vs 25.28). The age distribution had a single peak for the 50–59 and 60–69 years age groups, and it was not statistically significant between males and females (P = 0.26). The mean axial length was the highest for the 30–39 years age group for both male and female patients and significantly greater in the male than in the female patients older than 50 years (P < 0.001, P = 0.002, and P = 0.011, respectively).
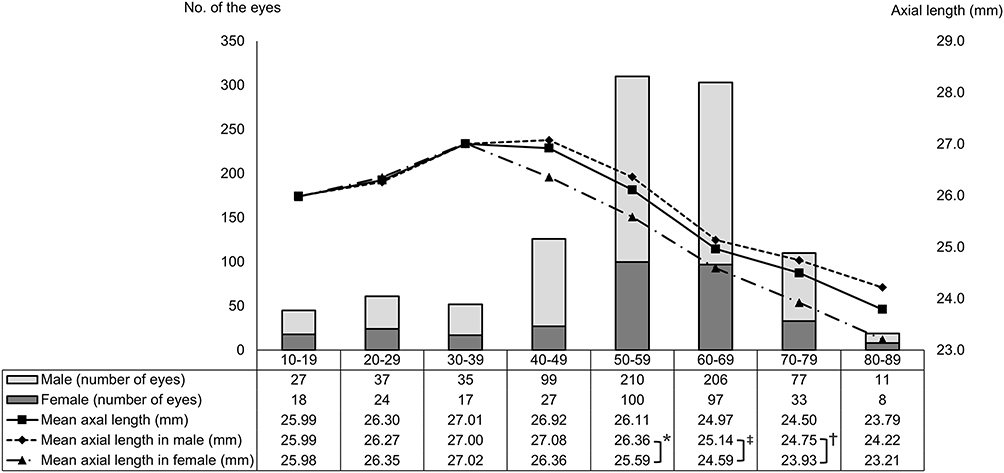 |
Figure 1 Age and axial length distributions of the age groups stratified by gender. The horizontal axis shows the age groups. Age distribution was not significantly different between males and females (P = 0.26). The mean axial length was significantly longer in the over-50 age groups of male patients than in female patients (*P < 0.001, ‡P = 0.002 and †P = 0.011, respectively). |
High Myopia (Figure 2)
We categorized the patients based on their degrees of myopia (high myopia, Axial length ≥ 26.5 mm; non-high myopia, Axial length < 26.5 mm) and compared them according to age distribution. The number of eyes with high myopia showed a single peak at 50–59 years (128 eyes). Within each age group, the proportion of highly myopic eyes was highest for the 40–49 years age group (62.7% within the age group). Additionally, in the 40–49-years and 50–59-years age groups, the data showed a significantly higher proportion of high myopia cases among male patients compared to female patients. (P = 0.017 and P = 0.005, respectively).
 |
Figure 2 Proportions of patients with high myopia in the different age groups of patients with rhegmatogenous retinal detachment. The horizontal axis shows the age groups. The proportion of highly myopic eyes was the highest in the 40–49 years age group (61.9% within the age group). In the 40–49 and 50–59 years age groups, the proportion of high myopia was significantly higher in male than in female patients (*P = 0.017 and ‡P = 0.005, respectively). |
Lens State
The study consisted of 887 phakic patients, 135 pseudophakic patients, and 4 aphakic patients. The average age of the patients with phakic eyes and eyes with prior cataract surgery were 52.9 ± 15.4 and 64.6±11.9 years, respectively. The durations between cataract surgery and the onset of RRD were identified in 119 eyes (84.0%), ranging from 23 days to > 40 years (median, 7 months).
Relationship Between Macular Status and Patient Characteristics
Table 2 presents the findings from the univariate comparisons of the preoperative macular statuses (macula-off vs macula-on). RRD was macula-off for 535 (52.1%) and macula-on for 491 (47.9%) eyes. The location of retinal breaks was recorded for 945 eyes (92.1%). Retinal breaks were observed within a single quadrant in 935 patients. The mean age was significantly lower for the macula-on than for the macula-off eye group. More eyes had undergone cataract surgery and had superior and temporal retinal breaks in the macula-off than in the macula-on group (P = 0.013, P < 0.001, and P < 0.001, respectively). Eyes with macular-on RRD were found to have a significantly higher frequency of superior nasal retinal breaks compared to eyes with macula-off RRD. There was no statistically significant correlation observed between macular status and axial length (P = 0.072).
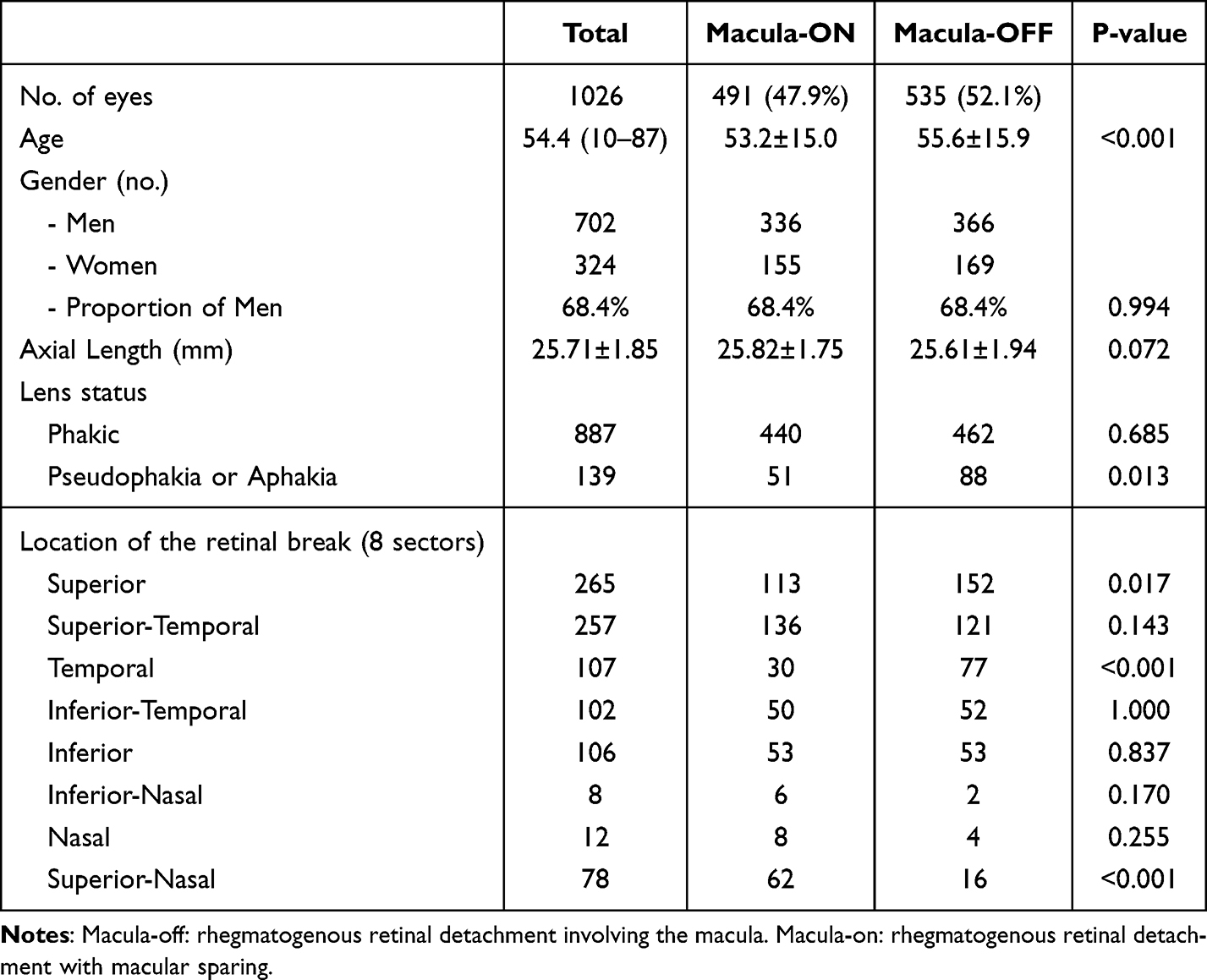 |
Table 2 Patient Characteristics Stratified by Macular Status |
Factors Associated with Macular-off RRD
Previous cataract surgery, but not age or sex, was significantly associated with macula-off retinal detachment in all multivariate models (Table 3). In the multivariate model with the smallest AIC, it was found that a shorter axial length (≤ 24.5 mm) has a significant association with macular detachment (odds ratio, 1.355; 95% confidence interval, 1.010–1.815; P value, 0.043). Regarding the location of retinal breaks, superior (1.440, 1.063–1.950, 0.018) and temporal (2.736, 1.727–4.334, < 0.001) retinal breaks were significantly associated with macula-off RRD (Table 4). In contrast, superior-nasal breaks were significantly less likely to develop macular detachment (0.280, 0.147–0.500, < 0.001).
 |
Table 3 Multivariate Logistic Regression Analysis to Identify Factors Associated with Macular-off Retinal Detachment |
 |
Table 4 Multivariate Logistic Regression Analysis to Identify the Retinal Break Location Associated with Macula-off Retinal Detachment |
Discussion
This study’s logistic regression analysis demonstrates that shorter axial lengths significantly increased the odds ratio of macular detachment. Potic et al14 found that axial length < 25 mm had a suppressive effect on macular involvement. They speculated that this finding was explained by the mechanism that highly myopic eyes have a thinner choroid, which restricts retinal perfusion, resulting in inhibiting the accumulation of subretinal fluid.14 Additionally, it has been speculated that patients with high myopia are more likely to seek medical attention earlier due to prior knowledge of RRD symptoms.14 Another investigator described that there is a constant contraction force on the retina, tending towards the tangential direction due to the elasticity of the retina. This force can be deconstructed into horizontal and vertical components, with the vertical component acting to detach the retina.16 From this explanation, highly myopic eyes are speculated to have a small vertical force due to the large radius of curvature of the eyeball and decreased retinal thickness. This may provide an alternative explanation for the lower incidence of macular detachment in the highly myopic eyes with RRD.
In this study, 351 patients (34.2%) had eyes with high myopia. The Japan Retinal Detachment Registry Report ǀ17 investigated the preoperative characteristics of 3178 eyes with RRD and reported a proportion of high myopia (axial length >26.0 mm) of 39.1%, and similar results were observed in this study. Several influential Japanese cohort studies have thoroughly examined the prevalence of high myopia, with rates of 5.5% reported by Tajimi18 (2000–2001, spherical equivalent <-6.0 D), 5.5% by Hisayama19 (2005, axial length >26.0 mm), and 6.70% by Nagahama20 (2013–2016, axial length >26.5 mm). Therefore, the proportion of high myopia in eyes with RRD seems to be markedly high. The number of individuals with high myopia was notably greater than those without in Korea,12 and this trend was also evident in the current study. The large-scale cohort study conducted in the Netherlands suggests that the increasing incidence of RRD may be attributed to the increasing prevalence of myopia.8 Another analysis of a group of individuals of European descent also found a link between myopia and the risk of retinal detachment.21 In this study, the 50–59 age group had the highest number of highly myopic eyes (128 eyes), and the 40–49 years group had the highest proportion of highly myopic eyes (62.6%). These results suggest that the incidence of RRD will have a more myopic shift in older age groups in the future. Additionally, the results of the current study do not necessarily indicate a higher frequency of macular off-eye in the age group with high myopia. To the best of our knowledge, there have been no reports of risk factors for macular detachment using a large number of cases with RRD and high myopia. Based on these results, it seems that the increase in retinal detachment in high myopia in the future does not necessarily imply an increase in macular off detachment.
Having had cataract surgery before has been identified as a significant risk factor for RRD.6 PVD is more common after cataract surgery, especially in those who have undergone crystalline lens removal.22 Hilford et al23 found a higher occurrence of PVD in pseudophakic eyes than in phakic fellow eyes. In addition, there is one report about the association between RRD and the risk of macular involvement. According to Potic et al,14 the pseudophakia is an independent predictive factor for macula-off RRD. This is in accordance with the results of the current study, showing that previous cataract surgery was a marked risk factor for macular detachment. They speculated that vitreous tractional forces were risk factors for retinal detachment. These forces can result from cataract surgery, which in turn raises the risk of macular detachment.; however, more detailed research into the detailed cause is required.
In the present study, superior and temporal retinal breaks significantly increased the odds ratio for macular detachment. A superior nasal break significantly decreased the odds ratio for macular involvement. According to Potic et al,14 the research findings revealed a significantly higher prevalence of macular detachment in eyes with temporal RD compared to those with nasal RD (54% vs 3%, P = 0.001). Interestingly, there was no significant variance in macular detachment prevalence between the eyes with superior and inferior RD (31.6% vs 45.5%, P = 0.34). Alberti et al24 reported that the progression of RRD was correlated with head movement and not with gravity or the head-positioning regimen. Jan et al25 reported that preoperative posturing suppressed the progression of RRD; however, there was no substantial association between the size of the retinal tear and RRD progression before surgery. The progression of RRD seems to be affected more by head or eye movements than by the location or size of retinal breaks or the effects of gravity.
The main limitation of the present study was its retrospective design, and there may have been some bias due to the extraction of data from a single hospital. However, the present study included more than 1000 eyes, and a large amount of data can balance such limitations. Further investigations, including large-scale prospective studies, are necessary to validate our study findings. Another limitation of this study was the measurement error in the axial length, which has been replaced from A-mode ultrasonography to a swept-source optical coherence tomography-based biometer. There have been reports indicating that the axial length measured by the Tomey OA-2000 was determined to be statistically shorter than that measured by the IOL Master.26 The substantial number of patients included in the study likely mitigated any potential impact of the difference on the results. Although the visual prognosis and the duration of macular detachment that affects it were not the purposes of this study, they are issues for future research.
Conclusion
The results of the present study demonstrate that a substantial 35.0% of eyes affected by RRD are associated with high myopia. Particularly noteworthy is the finding that the highest number of highly myopic eyes can be observed in the 50–59 age group. The highest proportion of highly myopic eyes was observed in the 40–49 years group. It is likely that the number of RRD patients with high myopia in older age groups will increase in the future, and further research is expected. Previous cataract surgery, shorter axial length, and superior and temporal retinal breaks were marked risk factors for macular detachment. This result of the present study including a large number data supported the previous researches, which is a recognized risk factor for macular detachment.
Author Contributions
All authors made a significant contribution to the work reported, including the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; have agreed on the journal to which the article has been submitted; have reviewed and agreed on all versions of the article before submission; and agreed to be accountable for the contents of the article.
Funding
There is no funding source.
Disclosure
None of the authors has any financial/conflicting interests to disclose.
References
1. Mitry D, Charteris DG, Yorston D, et al. The epidemiology and socioeconomic associations of retinal detachment in Scotland: a two-year prospective population-based study. Invest Ophthalmol Vis Sci. 2010;51:4963–4968. doi:10.1167/iovs.10-5400
2. Mitry D, Charteris DG, Fleck BW, et al. The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. Br J Ophthalmol. 2010;94:678–684. doi:10.1136/bjo.2009.157727
3. Chen SN, IeB L, Wei YJ. Epidemiology and clinical characteristics of rhegmatogenous retinal detachment in Taiwan. Br J Ophthalmol. 2016;100:1216–1220. doi:10.1136/bjophthalmol-2015-307481
4. Vande Put MAJ, Hooymans JMM, Los LI, Dutch Rhegmatogenous Retinal Detachment Study Group. The incidence of rhegmatogenous retinal detachment in the Netherlands. Ophthalmology. 2013;120:616–622. doi:10.1016/j.ophtha.2012.09.001
5. Ferrara M, Song A, Al-Zubaidy M, et al. The effect of sex and laterality on the phenotype of primary rhegmatogenous retinal detachment. Eye. 2023;37:2926–2933. doi:10.1038/s41433-023-02443-w
6. Tuft SJ, Minassian D, Sullivan P. Risk factors for retinal detachment after cataract surgery: a case-control study. Ophthalmology. 2006;113:650–656. doi:10.1016/j.ophtha.2006.01.001
7. Han X, Ong JS, An J, et al. Association of myopia and intraocular pressure with retinal detachment in European descent participants of the UK biobank cohort: a Mendelian randomization study. JAMA Ophthalmol. 2020;138:671–678. doi:10.1001/jamaophthalmol.2020.1231
8. van Leeuwen R, Haarman AEG, van de Put MAJ, et al. Association of rhegmatogenous retinal detachment incidence with myopia prevalence in the Netherlands. JAMA Ophthalmol. 2021;139:85–92. doi:10.1001/jamaophthalmol.2020.5114
9. Li X, Beijing Rhegmatogenous Retinal Detachment Study Group. Incidence and epidemiological characteristics of rhegmatogenous retinal detachment in Beijing, China. Ophthalmology. 2003;110:2413–2417.
10. Haga A, Kawaji T, Tsutsumi T, et al. The incidence of rhegmatogenous retinal detachment in Kumamoto, Japan between 2009 and 2011. J Clin Exp Ophthalmol. 2017;08:1–6. doi:10.4172/2155-9570.1000647
11. Zou H, Zhang X, Xu X, et al. Epidemiology survey of rhegmatogenous retinal detachment in Beixinjing District, Shanghai, China. Retina. 2002;22:294–299. doi:10.1097/00006982-200206000-00007
12. Kim MS, Park SJ, Park KH, Woo SJ. Different mechanistic association of myopia with rhegmatogenous retinal detachment between young and elderly patients. BioMed Res Int. 2019;2019:5357241. doi:10.1155/2019/5357241
13. Okuda T, Higashide T, Sugiyama K. Metamorphopsia and outer retinal morphologic changes after successful vitrectomy surgery for macula-off rhegmatogenous retinal detachment. Retina. 2018;38:148–154. doi:10.1097/IAE.0000000000001510
14. Potic J, Bergin C, Giacuzzo C, et al. Primary rhegmatogenous retinal detachment: risk factors for macular involvement. Graefes Arch Clin Exp Ophthalmol. 2018;256:489–494. doi:10.1007/s00417-017-3880-x
15. Flitcroft DI, He M, Jonas JB, et al. IMI defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies. Invest Ophthalmol Vis Sci. 2019;60(3):M20–M30. doi:10.1167/iovs.18-25957
16. Kuhn F, Aylward B. Rhegmatogenous retinal detachment: a reappraisal of its pathophysiology and treatment. Ophthal Res. 2014;51:15–31. doi:10.1159/000355077
17. Sakamoto T, Kawano S, Kawasaki R, et al. Japan-retinal detachment registry report I: preoperative findings in eyes with primary retinal detachment. Jpn J Ophthalmol. 2020;64:1–12. doi:10.1007/s10384-019-00702-6
18. Sawada A, Tomidokoro A, Araie M, et al. Refractive errors in an elderly Japanese population: the Tajimi study. Ophthalmology. 2008;115:363–370. doi:10.1016/j.ophtha.2007.03.075
19. Asakuma T, Yasuda M, Ninomiya T, et al. Prevalence and risk factors for myopic retinopathy in a Japanese population: the Hisayama study. Ophthalmology. 2012;119:1760–1765. doi:10.1016/j.ophtha.2012.02.034
20. Nakao SY, Miyake M, Hosoda Y, et al. Myopia prevalence and ocular biometry features in a General Japanese population: the Nagahama study. Ophthalmology. 2021;128:522–531. doi:10.1016/j.ophtha.2020.08.023
21. Ikram MA, Brusselle GGO, Murad SD, et al. The Rotterdam study: 2018 update on objectives, design and main results. Eur J Epidemiol. 2017;32:807–850. doi:10.1007/s10654-017-0321-4
22. Lois N, Wong D. Pseudophakic retinal detachment. Surv Ophthalmol. 2003;48:467–487. doi:10.1016/s0039-6257(03)00083-3
23. Hilford D, Hilford M, Mathew A, Polkinghorne PJ. Posterior vitreous detachment following cataract surgery. Eye. 2009;23:1388–1392. doi:10.1038/eye.2008.273
24. Alberti M, Ilsby C, Christensen UC, et al. Preoperative positioning and progression of fovea-on retinal detachments. Ophthalmol Retina. 2024;8:137–147. doi:10.1016/j.oret.2023.08.016
25. de Jong JH, Vigueras-Guillén JP, Simon TC, et al. Preoperative posturing of patients with macula-on retinal detachment reduces progression toward the fovea. Ophthalmology. 2017;124:1510–1522. doi:10.1016/j.ophtha.2017.04.004
26. Hua Y, Qiu W, Xiao Q, et al. Precision (repeatability and reproducibility) of ocular parameters obtained by the Tomey OA-2000 biometer compared to the IOL master in healthy eyes. PLoS One. 2018;13:e0193023. doi:10.1371/journal.pone.0193023
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.