")
Back to Journals » Clinical Ophthalmology » Volume 19
PRESERFLO Microshunt™ versus Non-Penetrating Deep Sclerectomy for Glaucoma Management, One-Year Results
Authors Cunha B , Gil P , Lopes E, Elisa-Luís M , Reina M, Gomes T, Cardigos J
Received 21 January 2025
Accepted for publication 1 April 2025
Published 25 April 2025 Volume 2025:19 Pages 1377—1386
DOI https://doi.org/10.2147/OPTH.S514126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bruna Cunha, Pedro Gil, Edgar Lopes, Maria Elisa-Luís, Maria Reina, Teresa Gomes, Joana Cardigos
Ophthalmology Department, ULS São José, Lisboa, Portugal
Correspondence: Bruna Cunha, Email [email protected]
Purpose: To compare the short-term efficacy and safety of the PRESERFLO™ MicroShunt (PF) versus Non-Penetrating Deep Sclerectomy (NPDS) with Esnoper®.
Methods: Retrospective comparative cohort study at a tertiary hospital including 79 eyes from 79 patients submitted to surgery (32 PF implantation, Group 1 and 47 NPDS, Group 2) between January 2022 and August 2023, with one year follow-up. Outcome measures included intraocular pressure (IOP), complications, surgical duration, postoperative major and minor interventions. Surgical failure was defined as IOP> 21 mmHg or < 20% reduction from baseline, IOP< 5 mmHg, major postoperative intervention, or loss of light perception. Conversely, success was defined as the absence of these failure criteria: complete success without glaucoma medications, and qualified success with.
Results: Baseline characteristics, including age, sex, IOP, number of IOP-lowering medications, and visual field defects, were comparable between groups (p> 0.05). After one year, IOP decreased significantly in both groups (PF: 20.13± 6.20 to 15.00± 3.15 mmHg; NPDS: 19.57± 5.73 to 13.30± 3.59 mmHg, both p< 0.001). Complete success rates were 28.1% for PF and 40.4% for NPDS (p=0.189), while surgical failure was significantly higher in the PF group (65.6% vs 38.3%, p=0.015). Major reinterventions were more frequent with PF (10 vs 3, p=0.005), partly due to encapsulated blebs, while NPDS required more minor interventions (2 vs 17, p=0.002). Complication rates were similar (31.3% vs 14.9%, p=0.073), but surgical duration was shorter in the PF group (60.03± 17.95 min vs 69.91± 15.23 min, p=0.008).
Conclusion: PF and NPDS share comparable safety profiles. Although PF surgery is faster, it is associated with a higher rate of major postoperative interventions and failure. NPDS, while requiring more minor interventions, such as goniopuncture and needling, rarely demands major re-interventions. NPDS is known for its meticulous and technically challenging technique, but once mastered, it can result in fewer invasive re-interventions and improved efficacy.
Keywords: glaucoma, Preserflo Microshunt, filtering surgery, intraocular pressure
Introduction
Glaucoma remains a leading cause of irreversible blindness worldwide,1,2 with its management typically involving pharmacologic interventions, primary using intraocular pressure-lowering medications (as prostaglandin analogs or beta-blockers). However, when pharmacotherapy or laser treatment fail to sufficiently control intraocular pressure (IOP) or when patients experience adverse effects, surgical intervention may become necessary to achieve adequate IOP control.3 The traditional gold standard for glaucoma surgery, trabeculectomy, while effective, is associated with significant complications and postoperative burden, prompting the development of safer alternatives such as less invasive glaucoma surgeries and non-penetrating procedures.4,5
The PRESERFLO™ MicroShunt (PF) is a novel subconjunctival drainage device designed to provide a less invasive and standardized surgical approach to glaucoma management. By simplifying the surgical technique and aiming to reduce intraoperative risks, PF has gained attention as a potential alternative to traditional surgeries. Non-penetrating deep sclerectomy (NPDS), on the other hand, enhances aqueous outflow through Schlemm’s canal and collector channels without penetrating the anterior chamber, offering a safer and effective option for IOP reduction with fewer complications.6,7
While comparisons have been made between each procedure and trabeculectomy, to the best of our knowledge, there has been no direct comparison between PF and NPDS, despite their increasing adoption. Understanding their efficacy, safety, and reintervention rates is crucial for guiding clinical decisions and tailoring surgical options to patient needs. This study provides a comparative analysis of PF and NPDS for glaucoma management, focusing on one-year outcomes, including IOP control, reintervention rates, and safety profiles.
Methods
Study Design
Retrospective comparative cohort study of consecutive patients who underwent PF or NPDS at a single tertiary centre (ULS São José), between January 2022 and September 2023, with a one-year follow-up period. The study adhered to the principles of the Declaration of Helsinki, and institutional review board (Ethics Committee of the ULS São José) approvals were obtained commensurate with the respective institutional requirements. The need for participation consent was waived due to the retrospective nature of this study. Data was anonymised to ensure confidentiality.
Patients
Inclusion criteria included adult patients with a prior diagnosis of glaucoma and IOP above target despite maximal medical therapy. Only one eye per patient was enrolled in the study. Exclusion criteria were a follow-up period of less than 12 months, baseline vision limited to no light perception, a known allergy to mitomycin-C and previous laser procedures and incisional ocular surgery (excluding uncomplicated cataract surgery) within 90 days before the surgery.
Data Collection
Demographic data, including age, gender, and ethnicity, were collected, along with clinical and surgical data. Clinical parameters included best-corrected visual acuity (BCVA), glaucoma classification, prior ocular surgeries, baseline and follow-up IOP (measured using a Goldmann Applanation Tonometer), the number of glaucoma hypotensive medications, and the baseline mean deviation (MD) of visual fields (Octopus 900, Haag-Streit, Köniz, Switzerland). Surgical details recorded included the duration of the procedure, combination with cataract surgery (phacoemulsification), postoperative complications, and the need for further intervention or glaucoma surgery. Follow-up data were obtained through a comprehensive chart review. Time points for data collection were selected according to the recommendations outlined in the Consensus Document by the World Glaucoma Association on the design and reporting of glaucoma surgical trials.8
Surgical Procedures
All surgeries were performed by three experienced glaucoma surgeons. To account for the learning curve associated with each surgical technique, the first 15 procedures performed by each surgeon were excluded from the study. Preoperative preparation for all patients included one drop of pilocarpine 2%, one drop of apraclonidine 0.5%, and 250 mL of mannitol (200 mg/mL). Local sub-tenon anaesthesia was administered, and a 7/0 silk traction suture was placed on the superior cornea. The initial surgical steps were identical for both procedures. A 3–4 mm fornix-based conjunctival flap was created, followed by dissection of Tenon’s capsule to create a posterior pocket between Tenon’s capsule and the episclera. Wet-field cautery was used to achieve haemostasis.
PRESERFLO™ MicroShunt
Following the initial steps, mitomycin-C (0.2 mg/mL) was applied to the bare sclera using three soaked sponges for 2 minutes, then irrigated thoroughly with balanced salt solution. A trypan blue mark was placed 3 mm posterior to the limbus, and a superficial scleral pocket was created using the 1-mm wide blade provided in the device kit. A 25G bent needle was then used to create a scleral tunnel from the pocket apex, parallel to the iris plane, entering the anterior chamber at the trabecular meshwork. The microshunt was gently inserted into the tunnel (bevel up) until the fin was securely positioned within the scleral pocket. Flow through the device was confirmed by observing drop formation at the scleral end of the microshunt. Closure was performed stepwise, with repositioning of the Tenon capsule followed by the conjunctiva, both secured with water-tight 7/0 polyglactin absorbable sutures to the episclera at the limbus. Intracameral cefuroxime was administered at the conclusion of the procedure.
Non-Penetrating Deep Sclerectomy
A 5×5 mm square-shaped superficial scleral flap, with a thickness of 1/3 to 1/2 sclera, was dissected 1 mm into the clear cornea. Mitomycin-C (0.2 mg/mL) was applied to the bare sclera with three soaked sponges for 2 minutes and then washed out with balanced salt solution. A second, deeper 3×4 mm rectangular scleral flap, dissected to 90% of scleral depth, was created, leaving a thin layer of deep sclera over the uvea. Both flaps were created using a crescent blade. Schlemm’s canal was identified, and its external wall was delicately peeled away using Mermoud micro forceps (Huco Vision SA, St. Blaise, Switzerland), preserving Descemet’s membrane and avoiding perforation. The deeper flap was excised. To maintain the space, an implant (ESNOPER® V-200, AJL Ophthalmic, Araba, Spain) was inserted. The superficial flap was sutured, followed by the conjunctiva with 10/0 nylon sutures. Intracameral cefuroxime was administered at the end of the procedure.
For combined procedures, the surgical techniques described above for PF or NPDS were performed after completing phacoemulsification and intraocular lens implantation. Postoperative care for all patients included topical dexamethasone 0.1% administered four times daily with a gradual tapering schedule, and topical ofloxacin 0.3% applied four times daily for one week.
Outcome Measures
The primary outcome measures at one year were the cumulative rates of complete success (CS), qualified success (QS), and surgical failure (SF). SF was defined as an IOP greater than 21 mmHg or a reduction of less than 20% from baseline on two consecutive visits after three months, an IOP of 5 mmHg or less on two consecutive visits after three months, reoperation for glaucoma, or loss of light perception vision. CS was defined as cases meeting the success criteria without the use of additional medical therapy, while QS included cases achieving success with the use of anti-glaucoma medications. Minor postoperative interventions, such as needling, anterior chamber reformation, or anterior chamber washouts for hyphema, were considered postoperative manipulations and not classified as reoperations. Secondary outcomes included the reduction in the number of glaucoma medications, the incidence of surgical complications, and the rates of postoperative interventions and reoperations.
Statistical Analysis
Data normality was assessed using the Shapiro–Wilk test. Continuous variables were summarized as mean ± standard deviation (SD) or median ± interquartile range (IQR), depending on the normality of their distribution. Categorical variables were described as frequencies. Comparisons between groups were conducted using the independent-samples Student’s t-test or Mann–Whitney U-test for continuous variables, as appropriate, while categorical variables were analysed using Fisher’s exact test or the chi-square test. Changes in IOP and the number of glaucoma medications from baseline to the 12-month follow-up were evaluated using the Wilcoxon signed-rank test. The cumulative probability of success was analysed using Kaplan-Meier survival curves. A p-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS for Macintosh (version 24.0, SPSS, Inc).
Results
A total of 79 patients were included in the study (32, PF Group; 47, NPDS Group). Baseline data is summarized in Table 1. Overall, the baseline characteristics and glaucoma profile were similar between studied groups (p>0.05 for all comparisons). The proportion of combined surgeries (with phacoemulsification) was also comparable (37.5% vs 44.7%, p=0.643).
 |
Table 1 Patient Demographics and Baseline Characteristics |
IOP and number of glaucoma medications used decreased significantly in both groups one year after surgery [IOP: PF Group 18.5 (8.0) vs 14.0 (6.0), p<0.001; NPDS Group 18.0 (8.0) vs 13 (3.0), p<0.001; number of glaucoma medications: PF Group 4.0 (1.0) vs 0.0 (2.0), p<0.001; NPDS Group 4.0 (1.0) vs 0.00 (1.0), p<0.001)]. The distribution of median IOP values and mean number of glaucoma medications over time are represented in Figures 1 and 2. No differences were found regarding IOP values and number of glaucoma medications between both surgical techniques over the entire follow-up period (p>0.05 for each comparison, in each time-point).
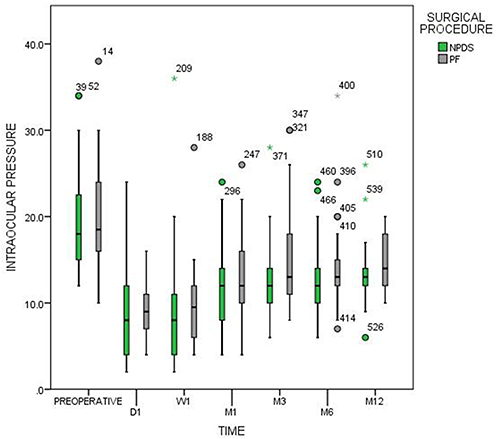 |
Figure 1 Median IOP values in mmHg (horizontal black line) and percentiles (boxes-quartiles = 25/75; whiskers = 5/95) given preoperatively and for a follow-up of 1 year. Single outliers are shown by circles. Abbreviations: D, day; W, week; M, month. |
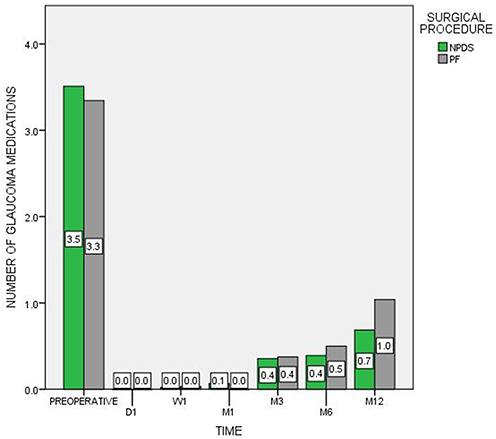 |
Figure 2 Mean number of glaucoma medications at baseline and follow-up. Abbreviations: D, day; W, week; M, month. |
Primary outcomes (CS, QS, SF) at 12-months are presented in Table 2, revealing no differences between studied groups in all evaluated parameters. Overall success (CS+QS) was higher in NPDS group (PF Group, 34.4% vs NPDS Group, 61.7%, p=0.022). No differences were found regarding success and failure rates between patients submitted to isolated glaucoma surgery compared to combined procedures (p>0.05 for all comparisons).
 |
Table 2 Treatment Outcomes |
Kaplan-Meier survival analysis was also used to compare survival probability between the 2 groups, Figure 3 (A: CS; B: CS and QS). There was no significant difference between the survival curves for the PF group and NPDS group for CS (p=0.616) but for CS and QS the survival distribution was significantly different between them (p=0.030).
 |
Figure 3 Kaplan-Meyer survival curves for the PRESERFLO™ MicroShunt and Non-Penetrating Deep Sclerectomy groups. (A) complete success; (B) qualified and complete success. |
The reasons for surgical failure are summarized in Table 3.
 |
Table 3 Reasons for Treatment Failure |
Postoperative Interventions
More PF cases underwent bleb revision with Mitomycin-C (9 vs 0; p<0.001) and more NPDP cases underwent laser goniopuncture (0 vs 14; p<0.001). Considering PF cases which underwent bleb revision, mean time of revision was 4.5 ± 1.51 months after surgery, with a mean IOP at 1-year of 14.78 ± 3.11 mmHg and a mean number of glaucoma medications of 1.56 ± 1.43.
No significant differences were found between groups, for the other performed interventions. Postoperative interventions are summarized in Table 4.
 |
Table 4 Postoperative Interventions |
Complications
Regarding intraoperative complications, we reported one case of hyphema in the PF group and one case of conjunctival buttonhole in each group. No serious intraoperative complications were verified. Postoperative complications are summarized in Table 5. No differences were found regarding the percentage of complications in each group (p=0.077).
 |
Table 5 Postoperative Complications |
Surgical Duration
NPDS procedures were significantly more time-consuming compared with PF (69.91 ± 15.23 minutes vs 60.03 ± 17.95 minutes, p=0.011).
Discussion
This study provides a comparative evaluation of the PF and NPDS for glaucoma management, focusing on efficacy, safety, and reintervention rates over a one-year follow-up period. Both techniques demonstrated significant reductions in IOP and medication use, supporting their established roles in glaucoma surgery. However, key differences emerged in reintervention types and one-year outcomes.
NPDS achieved a slightly greater reduction in IOP after one year compared to PF, likely due to its mechanism of enhancing aqueous outflow through Schlemm’s canal and collector channels. While not statistically significant, NPDS demonstrated higher success rates, with a greater percentage of eyes achieving complete success and qualified success. The failure rate was significantly lower in NPDS, suggesting it may offer more reliable long-term IOP control.
The study revealed notable differences in reintervention types between the techniques. Major reinterventions, such as secondary open-bleb surgeries, were more frequent in the PF group, occurring in over half of failed cases. In contrast, NPDS required more minor reinterventions, such as argon laser goniopunctures and needlings, which are quick and less invasive and can often be performed in the clinic, avoiding additional conjunctival manipulation. Available literature revealed that PF has a similar rate of bleb revisions compared to trabeculectomy,9,10 similar or even higher11 overall rate of reinterventions and, consequently, a similar rate of patients visits.9,10,12,13 When compared with canaloplasty, the number of reinterventions was also higher in PF group.14 On the other hand, NPDS augmented with mitomycin C seems to require less postoperative interventions and significantly fewer postoperative clinic visits.6 The procedural burden associated with PF reinterventions may extend beyond the operating room, affecting postoperative visits, hospital resources, patient well-being, and surgeon workload. For patients, this burden can include the psychological and physical distress of undergoing additional surgeries, as well as the demands of a second postoperative recovery period.
Bleb encapsulation was a frequent cause of surgical failure in the PF group and accounted for a significant proportion of major reinterventions. While needling may be a less invasive alternative to bleb revision, its efficacy remains variable.15–18 Tanner A. et al15 showed that approximately 62% of PF patients undergoing needling required additional needlings or bleb revisions, as fibrosis can often be too severe for needling alone to succeed. To date, choosing between needling versus surgical revision in PF patients is an issue that needs further investigation. Higher concentration of mitomycin C (eg, 0.04 mg/mL) may potentially mitigate bleb encapsulation, by reducing fibrosis severity and need for reinterventions particularly in populations prone to aggressive scarring.19–23 In our study, a higher mitomycin concentration might have improved outcomes by decreasing the rate of bleb encapsulation and the need for major reinterventions in the PF group.
The PF’s shorter surgical time and procedural efficiency are cited as an advantage.9 While PF is an appealing option in resource-limited settings or for surgeons less experienced with complex techniques like NPDS, the increased need for major reinterventions raises questions about its long-term efficiency and long-term cost-effectiveness. Prior research comparing PF to trabeculectomy reported significant cost savings due to reduced postoperative care.9 Our findings suggest that NPDS may incur even lower overall costs by reducing the need for major reoperations comparing to PF. While a formal cost analysis was not conducted in this study, future studies incorporating detailed cost-effectiveness analyses would provide valuable insights into the economic implications of these approaches.
Both techniques demonstrated similar safety profiles, with no serious complications reported and only mild adverse events observed. These findings align with existing literature and highlight that both PF and NPDS are safer alternatives to traditional trabeculectomy.9,12,23,24
The outcomes of this study are consistent with previous research on NPDS, which has been shown to provide effective long-term IOP control with fewer major complications.6,7,20,24 The significant rate of encapsulated blebs observed in PF cases suggests that while NPDS outcomes benefit from surgeon expertise and the use of adjunctive devices such as the Esnoper® implant, further improvements in PF device design and surgical protocols may enhance its performance over time. To our knowledge, no prior study has directly compared PF with NPDS, making this research a valuable contribution to the field. While the streamlined technique and shorter surgical time of PF are advantageous, especially in resource-constrained settings, they need to be weighed against the potentially higher postoperative burden and less favourable long-term outcomes.
The reported PF surgery success rate in this study was lower than previously reported for the same technique.9,15,16,22,23 Several factors may explain this finding. First, differences in surgeon expertise between techniques may have played a role, as the surgeons were highly experienced in NPDS but had comparatively less experience with PF, despite being beyond the theoretical learning curve. Second, variability in success criteria across studies introduces uncertainty, particularly regarding whether bleb revision should be classified as a major reintervention. If bleb revisions had not been considered major reinterventions in our study, the success rate would have been more comparable to previous reports. Moreover, the decision to perform a bleb revision instead of a needling procedure remains subject to surgeon preference, further influencing outcomes. Finally, although strong evidence is lacking in the literature, the use of a low-dose MMC regimen may have contributed to the lower success rate observed.
This study has some limitations. Its retrospective design, single-centre scope and the absence of statistical power calculation may limit the generalizability of the findings. Additionally, the one-year follow-up period may not capture long-term outcomes, particularly for PF, where encapsulation-related failures can emerge later. Another limitation is the difference in surgeon experience; while NPDS was performed by surgeons highly experienced in this technique, PF experience was relatively more limited despite being outside the learning curve. Future prospective multicentre studies with extended follow-up periods are essential to validate these findings and explore refinements in PF techniques.
In conclusion, both PF and NPDS are viable options for glaucoma surgery, each with distinct advantages. NPDS demonstrated slightly superior one-year success rates with fewer major reinterventions, making it a preferred choice for experienced surgeons seeking long-term stability. PF, on the other hand, provides procedural efficiency and accessibility, but its outcomes, particularly reinterventions and reoperations may improve with further refinements in device design and surgical technique. These findings emphasize the importance of tailoring surgical approaches to individual patient profiles, surgeon expertise, and available resources.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethics and Consent Statement
Confidentiality of Data: The authors declare having followed the protocols of their work centre on the data publication.
Author Contributions
All the authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
No funding or grant support.
Disclosure
The authors have no relevant financial or non-financial interests to disclose in this work.
References
1. Steinmetz JD, Bourne RRA, Briant PS, et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the right to sight: an analysis for the global burden of disease study. Lancet Glob Health. 2021;9(2):e144–e160. doi:10.1016/S2214-109X(20)30489-7
2. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
3. Heijl A. Reduction of intraocular pressure and glaucoma progression. Archives of Ophthalmology. 2002;120(10):1268. doi:10.1001/archopht.120.10.1268
4. Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153(5):789–803.e2. doi:10.1016/j.ajo.2011.10.026
5. Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814.e1. doi:10.1016/j.ajo.2011.10.024
6. Eldaly MA, Bunce C, ElSheikha OZ, Wormald R. Non-penetrating filtration surgery versus trabeculectomy for open-angle glaucoma. Cochrane Database Syst Rev. 2014;2014(2). doi:10.1002/14651858.CD007059.pub2
7. Rulli E, Biagioli E, Riva I, et al. Efficacy and safety of trabeculectomy vs nonpenetrating surgical procedures. JAMA Ophthalmol. 2013;131(12):1573. doi:10.1001/jamaophthalmol.2013.5059
8. Kymes S, Azuara-Blanco A. Guidelines for Economic Evaluation of Glaucoma Surgical Trials; 2009.
9. Van Lancker L, Saravanan A, Abu-Bakra M, et al. Clinical outcomes and cost analysis of PRESERFLO versus trabeculectomy for glaucoma management in the United Kingdom. Ophthalmol Glaucoma. 2023;6(4):342–357. doi:10.1016/j.ogla.2022.11.006
10. Fili S, Kontopoulou K, Vastardis I, Perdikakis G, Kohlhaas M. PRESERFLOTM microshunt versus trabeculectomy in patients with moderate to advanced open-angle glaucoma: 12-month follow-up of a single-center prospective study. Cureus. 2022;14(8). doi:10.7759/cureus.28288
11. Gubser PA, Pfeiffer V, Hug S, et al. PRESERFLO microshunt implantation versus trabeculectomy for primary open-angle glaucoma: a two-year follow-up study. Eye and Vision. 2023;10(1):1–12. doi:10.1186/s40662-023-00369-8
12. Zweifel LAB, Storp JJ, Vietmeier FE, et al. PRESERFLO microshunt versus trabeculectomy: efficacy and surgical success within a heterogenous patient cohort. Life. 2024;14(9):1–12. doi:10.3390/life14091171
13. Nobl M, Grün C, Kassumeh S, Priglinger S, Mackert MJ. One-year outcomes of PRESERFLOTM microshunt implantation versus trabeculectomy for pseudoexfoliation glaucoma. J Clin Med. 2023;12(8):3000. doi:10.3390/jcm12083000
14. Habbe KJ, Kohlhaas M, Fili S. PRESERFLOTM microshunt versus ab externo canaloplasty in patients with moderate to advanced open-angle glaucoma: 12-month follow-up of a single-center retrospective study. Cureus. 2023;15(2):10–18. doi:10.7759/cureus.35185
15. Tanner A, Haddad F, Fajardo-Sanchez J, et al. One-year surgical outcomes of the PRESERFLO MicroShunt in glaucoma: a multicentre analysis. Br J Ophthalmol. 2023;107(8):1104–1111. doi:10.1136/bjophthalmol-2021-320631
16. Mercieca K, Bhayani R, Martinez-de-la-Casa JM, et al. 3-year safety and efficacy results of PRESERFLOTM microshunt in glaucoma patients: a multicentre European cohort study. AJO International. 2024;1(3):100054. doi:10.1016/j.ajoint.2024.100054
17. Chen X, Suo L, Hong Y, Zhang C. Safety and efficacy of bleb needling with antimetabolite after trabeculectomy failure in glaucoma patients: a systemic review and meta-analysis. J Ophthalmol. 2020;2020:1–13. doi:10.1155/2020/4310258
18. Midha N, Gillmann K, Chaudhary A, Mermoud A, Mansouri K. Efficacy of needling revision after XEN gel stent implantation: a prospective study. J Glaucoma. 2020;29(1):11–14. doi:10.1097/IJG.0000000000001394
19. Durr GM, Schlenker MB, Samet S, Ahmed IIK. One-year outcomes of stand-alone ab externo SIBS microshunt implantation in refractory glaucoma. Br J Ophthalmol. 2022;106(1):71–79. doi:10.1136/bjophthalmol-2020-317299
20. Riss I, Batlle J, Pinchuk L, Kato YP, Weber BA, Parel JM. Résultats à un an de l’efficacité et de l’innocuité du MicroShunt InnFocus selon l’emplacement et la concentration de MMC. J Fr Ophtalmol. 2015;38(9):855–860. doi:10.1016/j.jfo.2015.05.005
21. Schlenker MB, Durr GM, Michaelov E, Ahmed IIK. Intermediate outcomes of a novel standalone ab externo sibs microshunt with mitomycin C. Am J Ophthalmol. 2020;215:141–153. doi:10.1016/j.ajo.2020.02.020
22. Beckers HJM, Aptel F, Webers CAB, et al. Safety and effectiveness of the PRESERFLO® microshunt in primary open-angle glaucoma: results from a 2-year multicenter study. Ophthalmol Glaucoma. 2022;5(2):195–209. doi:10.1016/j.ogla.2021.07.008
23. Jamke M, Herber R, Haase MA, Jasper CS, Pillunat LE, Pillunat KR. PRESERFLO TM MicroShunt versus trabeculectomy: 1-year results on efficacy and safety. Graefes Arch Clin Exp Ophthalmol. 2023;261(10):2901–2915. doi:10.1007/s00417-023-06075-4
24. Dwivedi R, Somerville T, Cheeseman R, Rogers C, Batterbury M, Choudhary A. Deep sclerectomy and trabeculectomy augmented with Mitomycin C: 2-year post-operative outcomes. Graefes Arch Clin Exp Ophthalmol. 2021;259(7):1965–1974. doi:10.1007/s00417-021-05144-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.