")
Back to Journals » Journal of Inflammation Research » Volume 17
Prevalence and Risk Factors of Thromboembolic Events in Dermatomyositis in China: A 10-Year Retrospective Analysis
Authors Li L , Ding T, Shi Q, Zhu H, Ma Q, Zhou M, Yuan Y, Wen Z, Xu H, Tan H, Chen D
Received 14 August 2024
Accepted for publication 19 November 2024
Published 23 November 2024 Volume 2024:17 Pages 9539—9547
DOI https://doi.org/10.2147/JIR.S482055
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Liubing Li,1,* Tangdan Ding,1,2,* Qiong Shi,1,* Hongji Zhu,1,2 Qinghua Ma,1,2 Mianjing Zhou,3 Ying Yuan,4 Zhihua Wen,5 Hongxu Xu,1,2 Hongxia Tan,1 Dubo Chen1
1Department of Laboratory Medicine, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, 510080, People’s Republic of China; 2Department of Laboratory Medicine, Nansha Division of The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, 511466, People’s Republic of China; 3Department of Rheumatology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, 510080, People’s Republic of China; 4Department of Cardiology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, 510080, People’s Republic of China; 5Department of Radiology, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, 510080, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dubo Chen; Hongxia Tan, Email [email protected]; [email protected]
Objective: Dermatomyositis (DM) is an autoimmune disease characterized by chronic muscle inflammation and weakness. Patients with DM are at an increased risk of thromboembolic events (TEs). This study aimed to investigate the prevalence of TEs in DM and to identify the independent predictors.
Methods: A total of 543 patients hospitalized for DM within the past 10 years were analyzed retrospectively and compared with patients with DM with and without TEs for demographic, clinical, and laboratory characteristics. The independent predictors were analyzed using multivariate logistic regression analysis. The diagnostic performance was calculated by a receiver operating curve (ROC).
Results: Twenty-two (4.1%) patients with DM had TEs, including 12 (54.5%) with venous thromboembolism and 10 (45.5%) with arterial thromboembolism. Multivariate logistic regression analysis demonstrated that glucocorticoid therapy (odds ratio (OR)=0.003, 95% confidence interval (CI) 0.00– 0.03, P< 0.001) was a protective factor for the patients with DM developing TEs, whereas increased D-Dimer (OR=1.885, 95% CI 1.21– 2.95, P=0.006) was a risk factor. The combined ROC analysis of glucocorticoid therapy and D-Dimer indicated high diagnostic values in distinguishing patients with both DM and TEs from patients without TEs, with 86.4% sensitivity, 98.9% specificity, and 0.983 area under the ROC curve (95% CI 0.962– 1.000, P< 0.001).
Conclusion: Patients with DM who have never received glucocorticoid therapy and have increased D-Dimer (> 1.3 mg/L fibrinogen equivalent units) should be screened for TEs.
Keywords: Dermatomyositis, thromboembolic events, prevalence, risk factors
Introduction
Idiopathic inflammatory myopathies (IIMs) are a heterogeneous group of autoimmune disorders characterized by chronic muscle inflammation and weakness. IIMs have an incidence of 0.2 to 2 per 100,000 person-years and a prevalence of 2 of 25 per 100,000 people.1–4 Dermatomyositis (DM) is a common clinical IIM subtype, primarily presenting with skin manifestations, which can affect the lungs, joints, esophagus, and heart.5 The prevalence of DM is approximately 1 to 6 per 100,000 people, with a predominance in women. The average age at diagnosis in adults ranges from 40 to 60 years.6,7 Early diagnosis and more effective drug treatment improve DM; nonetheless, the patients have greater mortality than the general population.8 Before the introduction of corticosteroids in DM treatment, its prognosis was poor, with mortality ranging from 50% to 61%.7
Thromboembolic events (TEs) are caused by at least one of these potential factors such as endothelial damage, stagnant blood flow, and blood hypercoagulability.9–11 DM is typically characterized by systemic inflammation, which can result in a hypercoagulable state associated with endothelial dysfunction, leading to TEs.12 TEs presentation in patients with DM is often sudden but may be asymptomatic.13 Patients with DM demonstrate a 2.85 to 4.36-fold increased risk of TEs,4,14–16 which includes thrombosis in veins and arteries. Venous thrombosis primarily includes venous thromboembolism (VTE), a multifactorial disease manifesting as either deep vein thrombosis (DVT) or pulmonary embolism (PE). Arterial thromboembolism (ATE) primarily includes acute coronary syndrome and cerebral infarction. TEs are serious complications of DM because they have been associated with a case-fatality rate of up to 30% within 30 days.17
The prevalence of DM with TEs in Southeast China remains unclear. Additionally, the TEs-associated independent predictors in patients with DM have not been thoroughly identified. In this study, we retrospectively reviewed 543 hospitalized patients with DM for the prevalence of TEs within the past 10 years at our hospital. The demographic characteristics, clinical features, laboratory data, and treatments were recorded to identify the independent factors for TEs.
Methods
Study Design and Patients
Patients who were hospitalized for DM in The First Affiliated Hospital of Sun Yat-sen University from January 2014 to December 2023 were selected for this study. To identify DM cases, we compiled a list of all patients aged ≥18 years with at least one International Classification of Diseases 10 code for DM (M33.0–1, M33.9). Using their manual medical records, they were evaluated for adult-onset DM according to the European League Against Rheumatism/American College of Rheumatology 2017 classification criteria.18 This criterion is used to identify a well-defined, relatively homogenous population of individuals with DM. Any individual with definite DM as indicated by a score ≥7.5 without muscle biopsy or ≥8.7 with muscle biopsy, along with at least one of the three skin criteria, met the criteria for DM.18 Patients with active DM or those with other autoimmune diseases at presentation were excluded. TEs were determined by ultrasonography, computed tomography, magnetic resonance imaging, or angiogram. This study was approved by the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University in China, and the requirement for written informed consent was waived because of the retrospective analysis of the anonymized data (No. IIT-2021-778). We confirmed that the data maintained with confidentiality and compliance with the Declaration of Helsinki.
Data Acquisition and Laboratory Tests
Demographic and clinical information was collected from the hospitalization records, including types of TEs, age at sample collection, sex, complications, medications, and laboratory indices. Creatine kinase (CK) was measured with an AU5800-automatic biochemical analyzer using Beckman reagents (Beckman Coulter, CA, USA). Hemoglobin (HGB) and the following laboratory indices were collected: inflammatory markers, such as white blood cells, neutrophils, lymphocytes, C-reactive protein, erythrocyte sedimentation rate, procalcitonin (PCT), ferritin, serum amyloid A, fibrinogen, complement 3, and complement 4; coagulation parameters, such as platelets, D-Dimer, anticardiolipin immunoglobulin G, and β2 glycoprotein 1 immunoglobulin G; and cardiac injury indicators, such as creatine kinase-myocardial band, troponin T, and N-terminal prohormone of brain natriuretic peptide (NT-proBNP). Serum autoantibodies against 16 autoantigens (Jo-1, OJ, EJ, PL-7, PL-12, MDA5, TIF1γ, SAE1, Mi-2α, Mi-2β, NXP2, SRP, Ku, PM-Scl75, PM-Scl100, and Ro-52) were measured using a commercial line blot assay (EUROLINE Autoimmune Inflammatory Myopathies 16 Ag [IgG] Euroimmun, Lubeck, Germany).19
Statistical Analysis
Statistical analysis was performed using SPSS Statistics version 26 (IBM Corporation, NY, USA) and GraphPad Prism version 9 (GraphPad Software, CA, USA). Continuous variables with normal or non-normal distributions are expressed as mean ± standard deviation (SD) or median (interquartile range [IQR]). Categorical variables are presented as percentages. Student’s t-test was conducted to compare the normally distributed parameters, whereas the Mann–Whitney test was conducted to compare the non-normally distributed parameters. Categorical variables were compared using the Chi-squared test or Fisher’s exact test. Potential predictors for TEs in patients with DM were identified using a univariate logistic regression model. Significant univariate predictors (P<0.05) were entered into multivariable logistic regression (stepwise forward algorithm) to identify the independent factors. A receiver operating characteristic (ROC) curve was plotted to evaluate the sensitivity and specificity. The optimal cut-off value was determined by the maximal Youden index (sensitivity+specificity-1). A P-value <0.05 was considered statistically significant.
Results
Patient Selection
We enrolled a retrospective cohort of 543 patients with DM and identified 22 patients with TEs. The prevalence of TEs was 4.1% in patients with DM. The most common types of TEs were VTE (54.5%), including DVT (36.4%) and PE (18.2%) (Table 1). DVT was predominant in the lower limbs (31.8%) than in the upper limbs (4.5%). ATE comprised 45.5% of TEs, primarily represented by cerebral stroke (36.4%), followed by acute coronary syndrome (9.1%). Four patients without TEs were randomly selected for each case. They were matched by their age, admission location (medical ward), and admission date. Thus, 110 patients with DM, including 22 patients with TEs and 88 patients without TEs were enrolled (Figure 1).
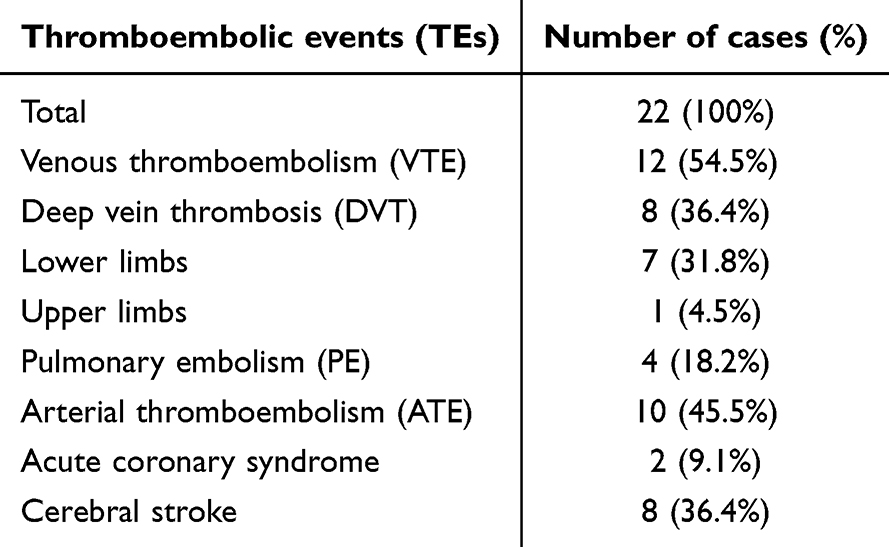 |
Table 1 Types of Thromboembolic Events in Patients with Dermatomyositis |
 |
Figure 1 Flow-chart of patient selection. Abbreviations: DM, dermatomyositis; TEs, thromboembolic events; CT, computed tomography; MRI, magnetic resonance imaging; VTE, venous thromboembolism; ATE, arterial thromboembolism. |
Comparison of Characteristics Between Patients with DM with and without TEs
Tables 2–4 summarize the demographic, clinical, and laboratory data of the 110 patients. Compared with patients without TEs, patients with TEs were older (mean age 63.1 years vs 50.1 years, P<0.001) and had a higher prevalence of hypertension (31.8% vs 10.8%, P=0.041) and a lower proportion of glucocorticoid (22.7% vs 98.9%, P<0.001) and immunosuppressant (45.5% vs 92.0%, P<0.001) therapies (Table 2). The levels of PCT (median 0.17 vs 0.07 ng/mL, P<0.001), D-Dimer (median 2.5 vs 0.90 mg/L fibrinogen equivalent units (FEU), P<0.001), and NT-proBNP (median 488.7 vs 84.2 pg/mL, P<0.001) were significantly higher in patients with TEs (Table 3). Conversely, HGB levels (median 107.0 vs 128.5 g/L, P=0.005) were significantly lower in patients with TEs (Table 3). Additionally, no significant differences in myositis-related autoantibodies were observed between the groups (Table 4).
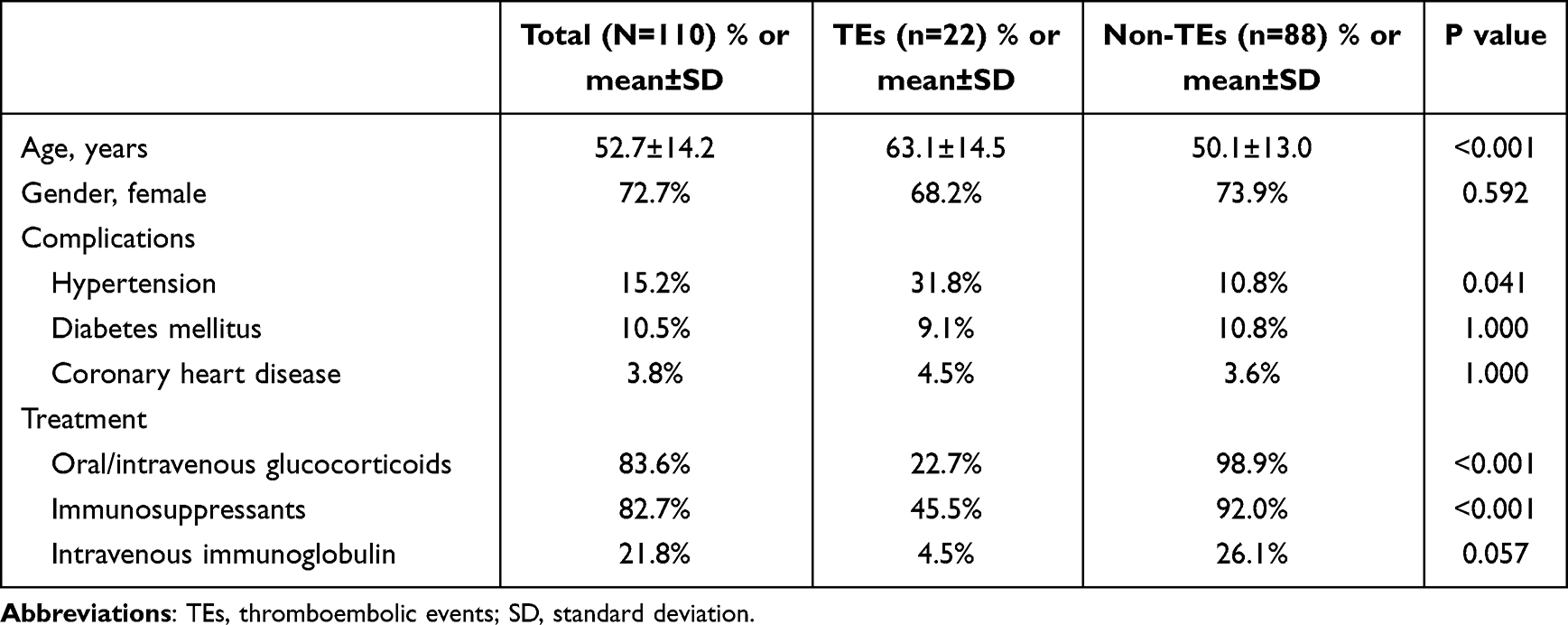 |
Table 2 Comparison of Demographic Characteristics, Complications and Treatment Between TEs and Non-TEs Groups |
 |
Table 3 Comparison of Laboratory Characteristics Between TEs and Non-TEs Groups |
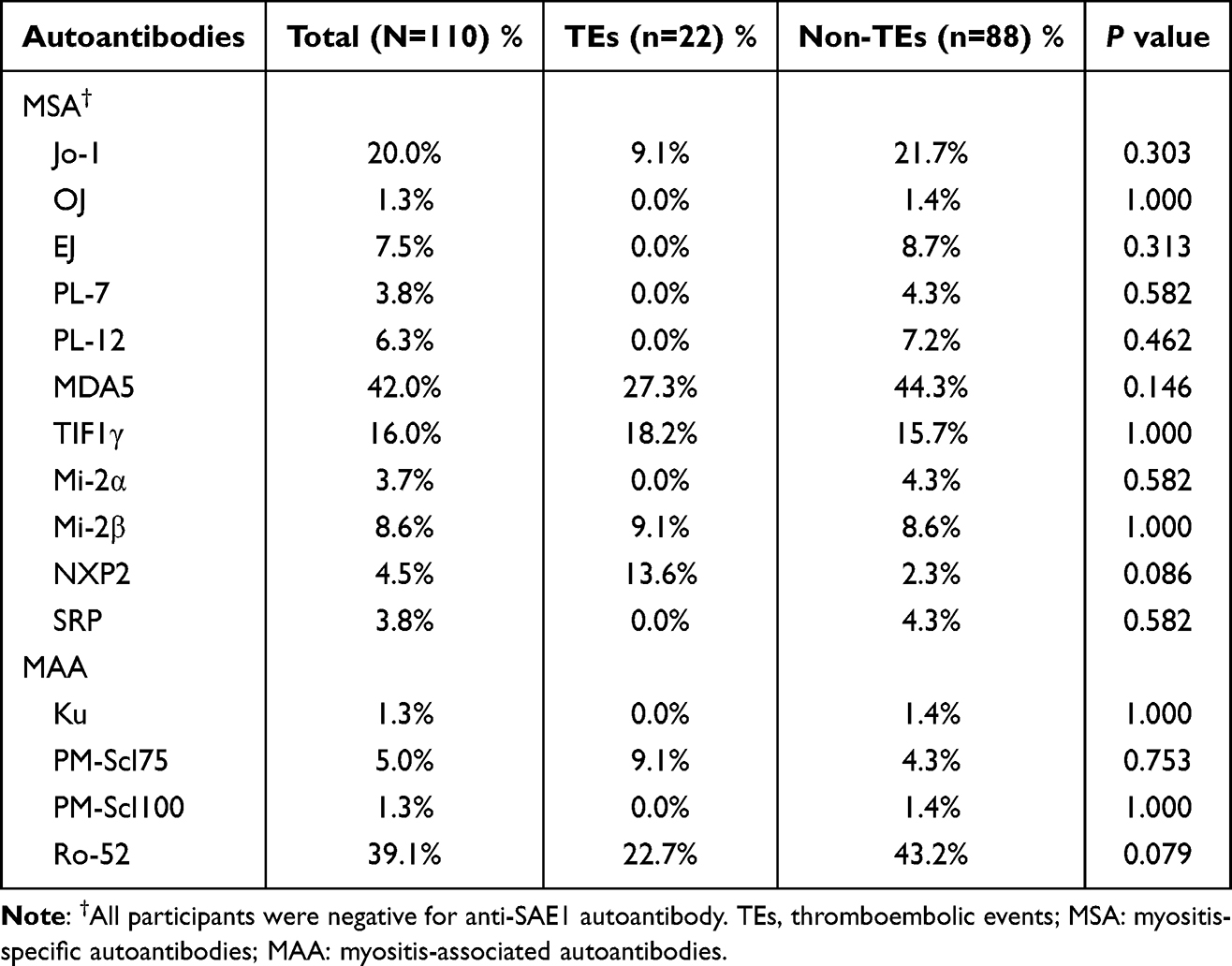 |
Table 4 Comparison of Myositis-Related Autoantibodies Between TEs and Non-TEs Groups |
Independent Predictors of TEs in Patients with DM
Univariate logistic regression suggested that age (OR=1.077, 95% CI 1.03–1.12, P<0.001), hypertension (OR=3.837, 95% CI 1.24–11.91, P=0.020), glucocorticoids (OR=0.003, 95% CI 0.00–0.03, P<0.001), immunosuppressants (OR=0.072, 95% CI 0.02–0.23, P<0.001), HGB (OR=0.971, 95% CI 0.95–0.99, P=0.005), D-Dimer (OR=2.294, 95% CI 1.44–3.65, P<0.001), and NT-ProBNP (OR=1.006, 95% CI 1.00–1.01, P<0.001) were the potential predictors of TEs (Table 5). Multivariable logistic regression suggested that glucocorticoid therapy (OR=0.003, 95% CI 0.00–0.03, P<0.001) was a protective factor for patients with DM developing TEs, whereas increased D-Dimer (OR=1.885, 95% CI 1.21–2.95, P=0.006) was a risk factor (Table 5).
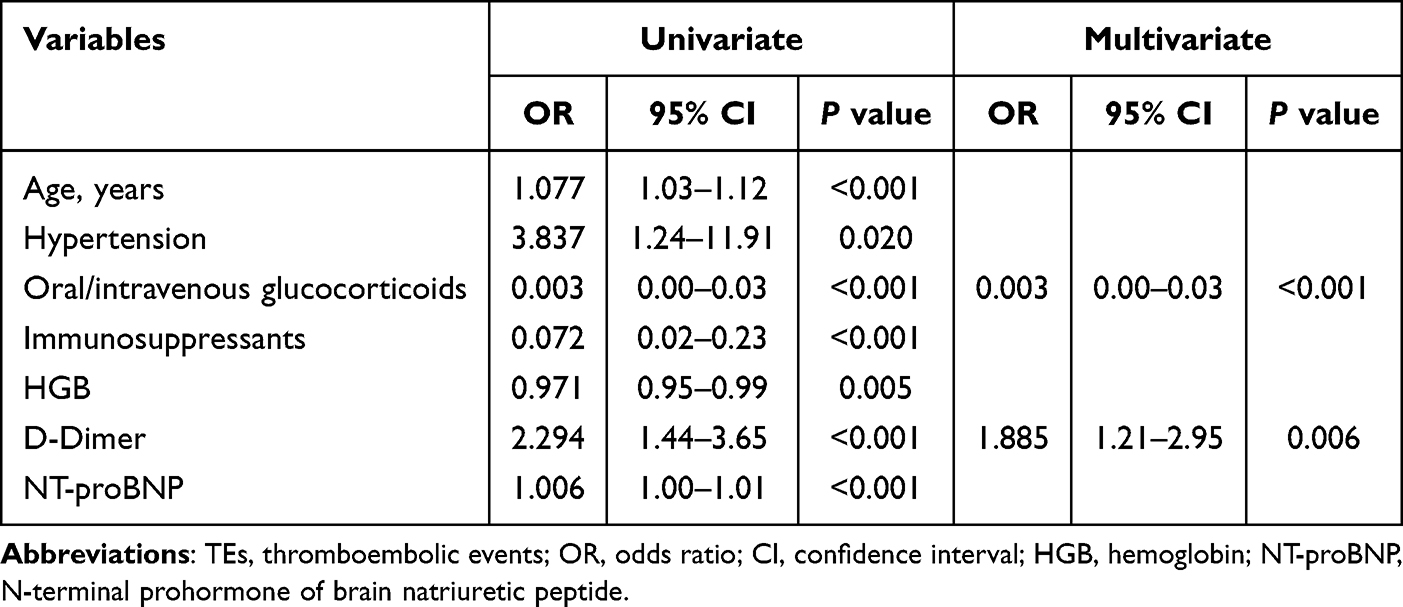 |
Table 5 Multivariate Analysis of Risk Factors of TEs in Patients with Dermatomyositis |
Diagnostic Performance of Glucocorticoid Therapy and D-Dimer for TEs in Patients with DM
The diagnostic performance of glucocorticoid therapy to differentiate the patients with and without TEs presented 77.3% sensitivity, 98.9% specificity, and 0.881 AUC (95% CI 0.774–0.987, P<0.001) (Figure 2). The ROC analysis suggested an optimal D-Dimer cut-off value of 1.3 mg/L FEU to differentiate the patients with and without TEs, with 86.4% sensitivity, 79.5% specificity, and 0.893 AUC (95% CI 0.831–0.954, P<0.001). Upon combining glucocorticoid therapy and D-Dimer to differentiate the patients with and without TEs, the AUC increased to 0.983 (95% CI 0.962–1.000, P<0.001), with 86.4% sensitivity and 98.9% specificity.
 |
Figure 2 ROC curves for the diagnostic performance of thromboembolic events in patients with dermatomyositis. Abbreviations: ROC, receiver operator characteristic; AUC, area under the curve; CI, confidence interval; GCs, glucocorticoids. |
Discussion
DM is a systemic autoimmune disorder with activated inflammatory response and infiltrated inflammatory cells into the skeletal muscle.12 TEs, including VTE and ATE, are potentially fatal complications in patients with DM, of which VTE is predominant. European studies have demonstrated a three-fold increase in the risk of VTE in patients with IIM after hospitalization.20–22 ATE is a sudden obstruction of arterial blood flow caused by the dislodgment of a blood clot from its formation site.23 The pathogenesis of ATE differs from that of VTE and it occurs because of endovascular injury or endothelial activation caused by the action of numerous proinflammatory mediators with subsequent platelet and coagulation pathway activation.24 In our study, the prevalence of TEs was 4.1% in patients with DM, consistent with the prevalence of 4.4% to 6.6% in patients of non-Asian descent.10 Men are more likely to present with TEs than women,25 despite unclear biological explanations for sex-based differences. However, in our cohort, there was no significant difference in TEs between men and women.
Glucocorticoids are the first-line regimen and standard of care in DM treatment. The association between glucocorticoid therapy and the risk of TEs is unclear. Pan et al suggested that glucocorticoids increase the risk of TEs in a dose- and duration-dependent manner.26 An epidemiologic prospective study from the UK using the General Practice Research Database indicated a greater risk of VTE in current oral glucocorticoid users, compared with nonusers (OR=3.05, 95% CI 2.51–3.69).27 Additionally, Orsi et al reported that glucocorticoid treatment increases VTE risk.28 Glucocorticoids increase the levels of coagulants, such as plasminogen activator inhibitor-1, thus reducing fibrinolytic activity. Therefore, adverse effects, such as abnormal clotting, may increase the risk of VTE in glucocorticoid users.20–22 However, Liu et al reported that glucocorticoid application will not increase the risk of VTE.29 Multivariate analysis indicated a trend toward the prevention of relapse with glucocorticoid use (HR=0.62, 95% CI 0.40–0.97, P=0.058).30 In this study, treatment with glucocorticoids reduces the risk of TEs in patients with DM. However, the mechanism by which they reduce the risk of TEs in patients with DM, and the length and dose of glucocorticoid use are unclear, warranting further studies.
D-Dimer is a biological marker of hemostatic abnormalities as well as an indicator of fibrinolysis indicating TEs or risk of TEs.31 D-Dimer levels during the diagnosis of acute lymphocytic leukemia may help identify the patients at a high risk of VTE or ATE.32 These levels are sensitive to PE diagnosis in patients with coronavirus disease 2019.33 Thus, D-Dimer serves as a valuable marker of activated coagulation and fibrinolysis in several clinical scenarios. D-Dimer has been extensively investigated for excluding VTE diagnosis and is used routinely for this indication.34 Elevated D-Dimer levels indicate an improvement in the coagulation and fibrinolysis systems. It can be utilized as a sensitive diagnostic criterion of hypercoagulability.35 Plasma D-Dimer levels increase after TEs; conversely, non-elevated D-Dimer levels are used to exclude such events.36 In our study, D-Dimer levels were significantly higher in patients with TEs than in patients without TEs. Additionally, the difference was statistically significant, consistent with previous results.
The inflammatory state of DM, as well as the use of glucocorticoids, increases the risk of infection. Systemic or localized infections increase the risk of TEs by 2 to 20 times and are the independent risk factors for TEs.37 We analyzed infection markers in patients with DM with and without TEs; PCT was significantly increased in patients with TEs. However, the logistic regression analysis did not indicate PCT as an independent factor. The incidence of infection in patients with both DM and TEs has rarely been investigated, thus necessitating additional studies to explore the association between infection and TEs in patients with DM.
Because of the low prevalence of TEs in patients with DM, we had a relatively small sample size, which may have weakened the generalizability of our findings and affected the results. Thus, well-designed prospective studies with a large sample size would facilitate understanding the association between the prevalence of TEs in patients with DM under glucocorticoid therapy and with increased D-Dimer levels.
Conclusion
TEs are a major issue in patients with DM, which is often overlooked. The prevalence of TEs was low in patients with DM, and the absence of glucocorticoid therapy and elevated D-Dimer levels indicated an increased risk of TEs. Patients with DM and risk factors for TEs should be screened for TEs. Moreover, anticoagulation should be considered to prevent TEs. Future studies investigating the association between DM and TEs are needed to guide interventions for TEs.
Acknowledgments
We would like to express our sincere gratitude to Pingjuan Liu for her invaluable assistance in interpreting our findings, as well as for her meticulous proofreading and revisions.
Funding
This research was supported by the Guangdong Basic and Applied Basic Research Foundation (2020A1515110173).
Disclosure
Liubing Li, Tangdan Ding and Qiong Shi contributed equally to this work and should be considered as co-first authors. The authors report no conflicts of interest in this work.
References
1. Khoo T, Lilleker JB, Thong BY, Leclair V, Lamb JA, Chinoy H. Epidemiology of the idiopathic inflammatory myopathies. Nat Rev Rheumatol. 2023;19:695–712. doi:10.1038/s41584-023-01033-0
2. Aggarwal R, Schessl J, Charles-Schoeman C, et al. Safety and tolerability of intravenous immunoglobulin in patients with active dermatomyositis: results from the randomised, placebo-controlled ProDERM study. Arthritis Res Ther. 2024;26:27. doi:10.1186/s13075-023-03232-2
3. Xiong A, Hu Z, Zhou S, et al. Cardiovascular events in adult polymyositis and dermatomyositis: a meta-analysis of observational studies. Rheumatology. 2022;61:2728–2739. doi:10.1093/rheumatology/keab851
4. Yafasova A, Diederichsen LP, Schou M, et al. Increased long-term risk of heart failure and other adverse cardiac outcomes in dermatomyositis and polymyositis: insights from a nationwide cohort. J Intern Med. 2021;290:704–714. doi:10.1111/joim.13309
5. Long K, Danoff SK. Interstitial Lung Disease in Polymyositis and Dermatomyositis. Clin Chest Med. 2019;40:561–572. doi:10.1016/j.ccm.2019.05.004
6. De Jesus AV, De Souza JM. Clinically amyopathic dermatomyositis associated with cutaneous ulcerations: a case-based review. Ann Med Surg Lond. 2024;86:1210–1214. doi:10.1097/MS9.0000000000001669
7. Paul N, Avalos C, Estifan E, Swyden S. Interstitial lung disease in dermatomyositis complicated by right ventricular thrombus secondary to macrophage activation syndrome- A case report. AME Case Rep. 2020;4:18. doi:10.21037/acr.2020.03.06
8. Dobloug GC, Svensson J, Lundberg IE, Holmqvist M. Mortality in idiopathic inflammatory myopathy: results from a Swedish nationwide population-based cohort study. Ann Rheum Dis. 2018;77:40–47. doi:10.1136/annrheumdis-2017-211402
9. F.a. A Jr, Wheeler HB. Physician practices in the management of venous thromboembolism: a community-wide survey. J Vasc Surg. 1992;16:707–714. doi:10.1016/0741-5214(92)90225-W
10. Carruthers EC, Choi HK, Sayre EC, Avina-Zubieta JA. Risk of deep venous thrombosis and pulmonary embolism in individuals with polymyositis and dermatomyositis: a general population-based study. Ann Rheum Dis. 2016;75:110–116. doi:10.1136/annrheumdis-2014-205800
11. Fujiwara H, Yamashita T C, Kawaji T, et al. Promotion of a venous thromboembolism prevention protocol at a perioperative management center. Fujita Med J. 2023;9:179–185. doi:10.20407/fmj.2022-024
12. Menichelli D, Cormaci VM, Marucci S, et al. Risk of venous thromboembolism in autoimmune diseases: a comprehensive review. Autoimmun Rev. 2023;22:103447. doi:10.1016/j.autrev.2023.103447
13. Liu B, Ding F, Zhang D, Wei GH. Risk of venous and arterial thromboembolic events associated with VEGFR-TKIs: a meta-analysis. Cancer Chemother Pharmacol. 2017;80:487–495. doi:10.1007/s00280-017-3386-6
14. Li Y, Wang P, Li L, Wang F, Liu Y. Increased risk of venous thromboembolism associated with polymyositis and dermatomyositis: a meta-analysis. Ther Clin Risk Manag. 2018;14:157–165. doi:10.2147/TCRM.S157085
15. Lee YH, Song GG. Idiopathic inflammatory myopathy and the risk of venous thromboembolism: a meta-analysis. Rheumatol Int. 2017;37:1165–1173. doi:10.1007/s00296-017-3735-0
16. Ungprasert P, Sanguankeo A. Risk of venous thromboembolism in patients with idiopathic inflammatory myositis: a systematic review and meta-analysis. Rheumatol Int. 2014;34:1455–1458. doi:10.1007/s00296-014-3023-1
17. Naess IA, Christiansen SC, Romundstad P, Cannegieter SC, Rosendaal FR, Hammerstrom J. Incidence and mortality of venous thrombosis: a population-based study. J Thromb Haemost. 2007;5:692–699. doi:10.1111/j.1538-7836.2007.02450.x
18. Lundberg IE, Tjarnlund A, Bottai M, et al. International Myositis Classification Criteria Project consortium, S. The Juvenile Dermatomyositis Cohort Biomarker, and Repository. European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Ann Rheum Dis. 2017;76:1955–1964. doi:10.1136/annrheumdis-2017-211468
19. Li L, Wang H, Wu C, et al. Myositis-specific autoantibodies in dermatomyositis/polymyositis with interstitial lung disease. J Neurol Sci. 2019;397:123–128. doi:10.1016/j.jns.2018.12.040
20. Zoller B, Li X, Sundquist J, Sundquist K. Risk of pulmonary embolism in patients with autoimmune disorders: a nationwide follow-up study from Sweden. Lancet. 2012;379:244–249. doi:10.1016/S0140-6736(11)61306-8
21. Ramagopalan SV, Wotton CJ, Handel AE, Yeates D, Goldacre MJ. Risk of venous thromboembolism in people admitted to hospital with selected immune-mediated diseases: record-linkage study. BMC Med. 2011;9:1. doi:10.1186/1741-7015-9-1
22. Johannesdottir SA, Schmidt M, Horvath-Puho E, Sorensen HT. Autoimmune skin and connective tissue diseases and risk of venous thromboembolism: a population-based case-control study. J Thromb Haemost. 2012;10:815–821. doi:10.1111/j.1538-7836.2012.04666.x
23. Potpara TS, Lip GY. Current therapeutic strategies and future perspectives for the prevention of arterial thromboembolism: focus on atrial fibrillation. Curr Pharm Des. 2010;16:3455–3471. doi:10.2174/138161210793563400
24. Rubino R, Imburgia C, Bonura S, Trizzino M, Iaria C, Cascio A. Thromboembolic Events in Patients with Influenza: a Scoping Review. Viruses. 2022;14. doi:10.3390/v14122817
25. Kyrle PA, Minar E, Bialonczyk C, Hirschl M, Weltermann A, Eichinger S. The risk of recurrent venous thromboembolism in men and women. N Engl J Med. 2004;350:2558–2563. doi:10.1056/NEJMoa032959
26. Pan SY, Tian HM, Zhu Y, et al. Cardiac damage in autoimmune diseases: target organ involvement that cannot be ignored. Front Immunol. 2022;13:1056400. doi:10.3389/fimmu.2022.1056400
27. Huerta C, Johansson S, Wallander MA, Garcia Rodriguez LA. Risk factors and short-term mortality of venous thromboembolism diagnosed in the primary care setting in the United Kingdom. Arch Intern Med. 2007;167:935–943. doi:10.1001/archinte.167.9.935
28. Orsi FA, Lijfering WM, Geersing GJ, et al. Glucocorticoid use and risk of first and recurrent venous thromboembolism: self-controlled case-series and cohort study. Br J Haematol. 2021;193:1194–1202. doi:10.1111/bjh.17388
29. Liu F, Duan M, Fu H, Wang T. The efficacy and safety of perioperative glucocorticoid for total knee arthroplasty: a systematic review and meta-analysis. BMC Anesthesiol. 2024;24:144. doi:10.1186/s12871-024-02530-9
30. Desbois AC, Wechsler B, Resche-Rigon M, et al. Immunosuppressants reduce venous thrombosis relapse in Behcet’s disease. Arthritis Rheum. 2012;64:2753–2760. doi:10.1002/art.34450
31. Feng L, Xie Z, Zhou X, et al. Diagnostic value of D-dimer for lower extremity deep venous thrombosis caused by rib fracture: a retrospective study. J Orthop Surg Res. 2023;18:515. doi:10.1186/s13018-023-03997-x
32. Anderson DR, Stock W, Karrison TG, Leader A. D-dimer and risk for thrombosis in adults with newly diagnosed acute lymphoblastic leukemia. Blood Adv. 2022;6:5146–5151.
33. Suh YJ, Hong H, Ohana M, et al. Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: a Systematic Review and Meta-Analysis. Radiology. 2021;298:E70–E80. doi:10.1148/radiol.2020203557
34. Johnson ED, Schell JC, Rodgers GM. The D-dimer assay. Am J Hematol. 2019;94:833–839. doi:10.1002/ajh.25482
35. Wang H, Lv B, Li W, Wang S. The Impact of D-Dimer on Postoperative Deep Vein Thrombosis in Patients with Thoracolumbar Fracture Caused by High-Energy Injuries. Clin Appl Thromb Hemost. 2022;28:10760296211070009. doi:10.1177/10760296211070009
36. Favaloro EJ, Arunachalam S, Dean E. Variable Performance of D-dimer Testing by Hemostasis Laboratories: the Australasian/Asia-Pacific Experience. Semin Thromb Hemost. 2024.
37. Dalager-Pedersen M, Søgaard M, Schønheyder HC, Nielsen H, Thomsen RW. Risk for myocardial infarction and stroke after community-acquired bacteremia: a 20-year population-based cohort study. Circulation. 2014;129(13):1387–1396. doi:10.1161/CIRCULATIONAHA.113.006699
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.