")
Back to Journals » Clinical Ophthalmology » Volume 19
Proactive Post-Injection Monitoring in Brolucizumab Therapy: A Study on Intraocular Inflammation and Treatment Outcomes
Authors Soman M, Jadhav A, Balakrishnan A, Sheth JU , Nair U
Received 7 February 2025
Accepted for publication 12 April 2025
Published 18 April 2025 Volume 2025:19 Pages 1313—1321
DOI https://doi.org/10.2147/OPTH.S520118
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Manoj Soman,1,2 Apoorva Jadhav,1,2 Abhaya Balakrishnan,1,2 Jay U Sheth,3 Unnikrishnan Nair1,2
1Department of Vitreoretinal Services, Chaithanya Eye Hospital and Research Institute, Trivandrum, India; 2Department of Research, Chaithanya Innovation in Technology and Eye care (Research), Trivandrum, India; 3Department of Retina, Shantilal Shanghvi Eye Institute, Mumbai, India
Correspondence: Jay U Sheth, Department of Retina, Shantilal Shanghvi Eye Institute, CS No: 3/207, 4/207, RJ Gaikwad Road, Barkat Ali Dargah Road, Wadala East, Mumbai, Maharashtra, 400037, India, Tel +91-9961167200, Email [email protected]
Purpose: Intravitreal anti-VEGF agents, such as Brolucizumab, play a crucial role in treating neovascular age-related macular degeneration (nAMD) and Polypoidal choroidal vasculopathy (PCV). While Brolucizumab offers advantages like extended duration and fewer injections, concerns about intraocular inflammation (IOI) have emerged. This study evaluates the outcomes of a proactive monitoring protocol for Brolucizumab-treated eyes with resistant nAMD and PCV.
Patients and Methods: A single-center retrospective study analyzed patients treated with Brolucizumab for resistant nAMD and PCV. Data on demographics, visual outcomes and IOI incidence, with the latter being confirmed by clinicians. Additional data on management strategies and follow-up adherence were also analyzed. Proactive monitoring included telephonic follow-up on day one and mandatory clinic visits on days 15 and 30. Retreatment followed a pro-re-nata (PRN) approach based on fluid persistence or visual acuity loss.
Results: Between February 2022 and September 2024, 311 Brolucizumab injections were administered to 144 eyes of 121 patients, with a mean follow-up of 8.6 months. IOI occurred in 7 eyes (4.9%), with a mean onset of 32.1 days. According to the HAWK and HARRIER discomfort grading scale, IOI was categorized as mild in 2 eyes (28.6%), moderate in 3 eyes (42.9%), and severe in 2 eyes (28.6%). Symptoms varied, including blurred vision, floaters, redness, and ocular pain. Inflammation was managed with topical and oral steroids, with resolution in 6 weeks for vasculitis and 9 weeks for vitritis, and no cases required intravitreal agents or vitrectomy. Visual acuity improved or remained stable for most, except in one case of persistent vitritis.
Conclusion: This study highlights the incidence of IOI with Brolucizumab in a real-world setting, emphasizing the importance of proactive monitoring and early intervention. Despite the occurrence of inflammation, visual outcomes were generally favorable, supporting the safety of Brolucizumab when managed carefully.
Keywords: brolucizumab, intraocular inflammation, proactive monitoring
Introduction
Intravitreal anti-vascular endothelial growth factor (anti-VEGF) medications remain the cornerstone of treatment for patients with neovascular age-related macular degeneration (nAMD) and Polypoidal choroidal vasculopathy (PCV). Their efficacy has been well-documented in Phase III trials, employing rigorous monthly or less frequent dosing schedule.1,2 Recently, newer anti-VEGF agents with extended duration of action, such as Brolucizumab, have been explored, particularly in treatment-naive patients with nAMD.
Brolucizumab has distinct advantages due to its small molecular size (26 kDa), excellent stability, and solubility, allowing for the administration of 6 mg in a single 50 µL intravitreal injection. This enables the delivery of a higher molar dose in the same volume compared to currently used VEGF inhibitors, ensuring an extended duration of action.3,4 The phase-3 hAWK and HARRIER trials demonstrated that, following three monthly loading doses, around half of the eyes treated with brolucizumab required 12-week intervals between treatments, while the remaining eyes showed satisfactory responses with injections every eight weeks.5,6
Despite initial excitement following FDA approval in 2019, concerns arose due to reports of intraocular inflammation (IOI). An independent safety review committee’s post-hoc analysis of the phase-3 hAWK and HARRIER trials revealed an IOI incidence of 4.6%, with concomitant vascular occlusions occurring in 2.1% eyes.7,8 However real-world data from the IRIS registry reported a lower incidence of IOI of 2.4%.9 In October 2020, Brolucizumab was regulatory approved for use in India to treat nAMD. Recent multicentric studies from India have reported even lower rates on IOI, ranging from 0.79% to 1.7%.10,11
It is speculated that proactive monitoring for IOI may detect more cases, as noted by some trials.12 Building on this premise, our proactive monitoring protocol was developed to enable earlier detection of subtle or subclinical inflammatory changes. Unlike previous strategies that predominantly relied on patient-reported symptoms or routine interval examinations, our protocol incorporates systematic and standardized assessments, thereby enhancing the potential for timely intervention. Furthermore, the design of this protocol ensures that it is both feasible for incorporation into standard clinical workflows and generalizable across diverse healthcare settings with minimal additional resources.
The aim of this study was to evaluate the outcomes of a proactive monitoring protocol for eyes receiving Brolucizumab for resistant nAMD and PCV.
Materials and Methods
We conducted a single-centre retrospective study of patients receiving intravitreal Brolucizumab for treatment-resistant nAMD or PCV between February 2022 and September 2024. The study was approved for conduct by the Institutional Review Board of Chaithanya Eye Hospital and Research Institute, and was carried out in accordance with the tenets outlined in the Declaration of Helsinki. Written informed consent was obtained from all the patients for participation in the study and for the publication of their data. Patient demographics including age, gender, diagnosis, baseline visual acuity, the total number of Brolucizumab injections received, the order of injection at which IOI occurred, the time of inflammation onset, management protocols, outcomes and final visual acuity were analysed.
Resistant disease was defined as inadequate or no change in fluid on OCT after at least three injections in PCV and nAMD, or at least 2 injections in pachychoroid neovasculopathy (PNV) eyes. Exclusion criteria included eyes with choroidal neovascularization (CNV) due to other aetiologies, significant media opacities that hindered fundus observation at baseline, coexisting diabetic retinopathy, and patients with a history of systemic vasculitis, autoimmune disease or anterior or posterior segment inflammation.
All the patients underwent preoperative evaluation using a standardized assessment sheet and were actively monitored postoperatively. Injections were administered under sterile conditions in the operating theatre. Postoperatively, all patients received topical ciprofloxacin 0.5% for one week. As part of our “proactive post-procedure monitoring” we conducted a telephonic check-in on the first postoperative day and ensured mandatory clinic visits on day 15 (±1 week) and day 30 (+ 1 week). Additionally, patients were instructed to any ocular or systemic adverse events immediately. Also, as part of the proactive monitoring protocol, patients were contacted via telephone calls to assess for symptoms suggestive of intraocular inflammation (IOI). All patients were sensitized to the risk of IOI during pre-treatment counselling, which ensured high responsiveness to follow-up calls. Calls were attempted multiple times (1–5 attempts) until contact was established, and there were no instances of missed or unanswered calls during the study period.
At baseline and all subsequent follow-up, patients underwent comprehensive clinical examinations, including best-corrected visual acuity (BCVA) assessment using the Snellen’s visual acuity chart, intraocular pressure (IOP) measurement with the Goldmann applanation tonometer, anterior segment evaluation using slit-lamp biomicroscopy and fundus examination with both slit-lamp biomicroscopy (+90D lens) and indirect ophthalmoscopy (+20D lens). Spectral domain optical coherence tomography (SD-OCT) was performed on days 15 and 30 of follow-up or as deemed necessary by the physician. A detailed history was taken at each visit regarding any ocular or systemic adverse events. (IOI) was assessed using the HAWK and HARRIER grading system,7 and all cases were confirmed clinically during examinations.
Retreatment was offered to all patients on a pro-re-nata (PRN) basis, no earlier than eight weeks, for persistent or worsening fluid, subretinal hemorrhage, or a loss of more than one Snellen line of visual acuity. A PRN strategy was employed from the first injection, with no loading doses used. All demographic and clinical data were extracted from the electronic medical database and compiled in an excel sheet for analysis.
Statistical Analysis
Data were entered into a secure database and analyzed using SPSS 23.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were utilized to summarize patient demographics and clinical parameters. Visual acuity measurements obtained from the Snellen chart were converted to logMAR for analysis. Continuous variables such as age, baseline and final BCVA, number of Brolucizumab injections, and time to onset of IOI were expressed as means ± standard deviation (SD). Categorical variables, including gender, diagnosis, presence of IOI, and management outcomes, were presented as frequencies and percentages.
Results
Between February 2022 to September 2024, a total of 311 Brolucizumab injections were administered in 144 eyes of 121 patients. The treatment was primarily indicated for PCV, PNV, and nAMD resistant to other anti-VEGF therapies. The average follow-up duration was 8.6 months (range: 4–18 months). A PRN regimen was followed from the initiation of treatment, with at least 8 weeks between consecutive injections, regardless of the underlying condition. The study population had a mean age of 69.56 years (range 36–89 years), with 74 males and 70 females. A total of 111 eyes were diagnosed with nAMD, 32 with PCV, and one with PNV. All eyes had previously received other anti-VEGF agents and were categorized as resistant based on predefined criteria. Twenty-three patients received bilateral Brolucizumab injections, while 98 patients received injections in one eye. Prior to Brolucizumab treatment, patients received a mean of 3.57 (range 2–7) injections with agents such as Ranibizumab and Aflibercept. The mean number of Brolucizumab injections per eye was 2.17 (range 1–9) over a follow up period ranging from 4 to 18 months. At the conclusion of the study, 80 eyes (55.6%) were classified as inactive, with no documented fluid or hemorrhage. Fifty-three eyes (36.8%) remained active.
Intraocular Inflammation (IOI) Incidence and Management
Proactive post-injection monitoring revealed IOI in 7 out of the 144 treated eyes, an incidence of 4.9%. Of these 7 patients (7 eyes), 4 were females, and 3 were males, with a mean age of 73.7 years (Range 67–85). The patient cohort included 4 pseudophakic and 3 phakic patients. Of these, 2 eyes had PCV, and 5 eyes had nAMD. IOI occurred after the first injection in 4 eyes (57.1%), after the second injection in 2 eyes (28.6%), and after the third injection in 1 eye (14.3%). None of the patients developed bilateral inflammation, even though 23 patients received bilateral injections. Symptoms of IOI appeared between 14 and 72 days post-injection, with a mean onset of 32.1 days. The presenting symptoms of IOI varied: 2 eyes (28.6%) reported blurred vision, 2 eyes (28.6%) experienced floaters, 3 eyes (42.9%) presented with redness, and in 2 eyes (28.6%) had ocular pain. Based on the HAWK and HARRIER discomfort grading scale, the IOI was classified as mild in 2 eyes (28.6%), moderate in 3 eyes (42.9%), and severe in 2 eyes (28.6%).
The inflammatory responses included isolated anterior uveitis with keratic precipitates, cells, and flare in the anterior chamber (AC), with or without hypopyon in 2 eyes (28.6%). In 3 eyes (42.9%), vitritis was present alongside an AC reaction, and 2 eyes (28.6%) vasculitis was observed along with vitritis. Fundus fluorescein angiography (FFA) confirmed the diagnosis of vasculitis in these eyes, with no evidence of vascular occlusion or increased IOP. The mean time from injection to presentation of IOI was 41 days for isolated anterior uveitis, 38 days for vitritis, and 14.5 days for vasculitis.
Eyes with isolated anterior uveitis were successfully managed with topical Prednisolone acetate for a mean duration of 4 weeks, tapering the steroid dose as inflammation subsided. Eyes with vitritis and vasculitis were treated with a combination of topical and oral steroids. Vitritis resolved in an average of 9 weeks (Range; 4 weeks to 15 weeks), while vasculitis resolved within 6 weeks. No intravitreal agents were required for treating inflammation, and none of the patients underwent vitrectomy or diagnostic vitreous tap. There was no instance of infectious endophthalmitis during the study.
Visual acuity at baseline for the IOI group was 0.97 logMAR (Range 0.3–1.7 logMAR). During the episode of IOI, 3 eyes experienced a decrease in vision, while 4 eyes maintained stable vision compared to the pre-injection levels. Ata minimal follow up of 4 months, the mean final BCVA was 0.78 logMAR (Range 0.2–1.7 logMAR) in this group. All eyes either regained their vision or remained stable, except for one eye with vitritis, which did not improve. Eyes with the severe inflammation, including vitritis and vasculitis, demonstrated favorable visual recovery, with one eye each returning to baseline vision and the other improving.
At the last follow-up, three eyes showed improvement, including one with anterior uveitis, one with vitritis, and one with vasculitis. One eye with vitritis did not reach baseline vision, attributed to worsening macular pathology (Table 1; Case 6). This patient achieved baseline vision at the end of the treatment for IOI but experienced a one-line drop during the 4-month follow-up period, likely due to the absence of further injections.
 |
Table 1 Characteristics of Patients with Documented IOI After Intravitreal Brolucizumab |
Among the 7 affected eyes, 2 eyes received a second dose of Brolucizumab without any subsequent inflammation or vasculitis. Two patients (2 eyes) opted to switch to another anti VEGF (Aflibercept) after developing IOI with Brolucizumab, while the remaining 3 eyes showed no further activity and did not require additional anti-VEGF treatment. One of these eyes later received Brolucizumab in the contralateral eye without any IOI.
Figure 1 illustrates one representative case from the study population.
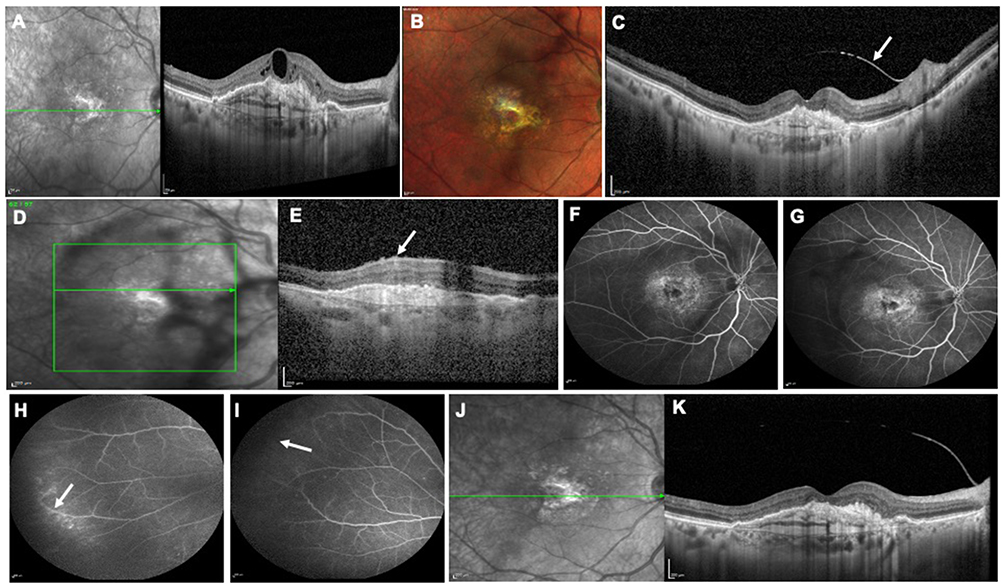 |
Figure 1 A 70-year-old male patient (Case 4) diagnosed to have neovascular age-related macular degeneration (nAMD) resistant to Ranibizumab (4 injections) at baseline presented with persistent intraretinal fluid (IRF) (A) on the spectral-domain optical coherence tomography (SD-OCT) and had a visual acuity of 6/60. He received 2 injections of Brolucizumab at 8 week intervals. At 2 weeks post-second injection mandatory examination, he was diagnosed to have anterior uveitis along with vitritis. The SD-OCT demonstrated resolution of the IRF, but revealed a reflective thickened posterior hyaloid (C, arrow) with preretinal inflammatory deposits (E, arrow). Note the vitreous membranes seen on multicolour imaging and the infrared (IR) image (B, D, arrow). The fundus fluorescein angiography (FFA) illustrated staining of the choroidal neovascular membrane (CNVM) (F and G) and peripheral vascular leakages (H) and areas of nonperfusion (I). The patient was managed with topical and oral steroids over the next 10 weeks and the vitritis resolved. The SD-OCT at 20 weeks follow up revealed scarred CNVM complex (K). Note the relatively clear IR image with resolution of the vitreous opacities (J). The patient did receive 1 Aflibercept injection 3 weeks prior for minimal IRF which seems to have resolved during this visit. The final visual acuity remained stable at 6/60 in this eye. |
Discussion
The introduction of Brolucizumab has enabled clinicians to manage nAMD and PCV eyes more effectively, offering benefits such as a longer duration of action and superior drying, which can reduce patient discomfort. However, concerns about its safety persist due to reported instances of IOI, retinal vasculitis and vascular occlusion.
In the HARRIER and HAWK Phase 3 trials,7,8 the pooled post hoc analysis revealed an IOI incidence of 4.5%. Subsequently, the real-world studies, such as the OCTOPUS and SWIFT, reported higher rates of 10.5%.12 However, the incidence of IOI-related events in clinical practice has varied widely. Many studies do not focus exclusively on IOI-related events, and reporting standards differ. For example, the IRIS/KOMODO database, which reflects predominantly Caucasian population, reported a lower incidence of 2.4%.9 In contrast, studies from Asia13–18 have reported a broader range of incidences, from 0 to 22%, with which varying study populations that included both treatment naïve and resistant cases. Additionally, treatment protocols varied, with some studies employing a posology defined loading protocol, while others used a PRN protocol without a loading phase. A recent meta-analysis including real-world studies reported an IOI incidence of ranging from 0 to 19%.19
In India, reports from real-world life settings indicate a lower incidence of IOI with Brolucizumab, ranging from 0 to 3.6%.10,11,13,14 Notably, a large multicentric, survey-based retrospective study found an incidence of 0.79%.10 However, it should be noted that these studies used diverse methods of data collection—some reported IOI per injection, while others reported per eye. Additionally, they included a mixed of treatment-naive and refractory cases. Such variability may lead to an underestimation of the true risks associated with Brolucizumab, potentially fostering complacency among treating physicians.20
In our study, which implemented a proactive monitoring protocol, the incidence of IOI was 4.9%, higher than previously reported rates in India. This proactive strategy may explain the increased detection, emphasizing the importance of diligent monitoring. It is also speculated that the presentation of IOI upon treatment with Brolucizumab may be attenuated by its potent anti-VEGF effects, which reduce vascular leakage, potentially leading to underestimation of disease severity and delayed treatment. than that reported for IOI/RV/VO of other origins. Such presentations may result in the underestimation of disease severity and, consequently, undertreatment. It is crucial to identify these cases early and manage them effectively, even though a small percentage of them may resolve spontaneously.21
The pathogenesis of IOI and retinal vascular involvement associated with the use of Brolucizumab is thought to be an immune reaction.22–25 The nature, timing, and association of these events with anti-drug antibodies (ADAs) suggest an immune response to Brolucizumab. Anti-Brolucizumab ADAs may arise due to prior immune sensitization to structurally similar proteins.23 Factors increasing the immunogenicity of Brolucizumab include its non-natural format (single-chain variable fragment), bacterial epitope similarity, and accumulation of Brolucizumab degradation products in the eye.24 Pre-existing ADA to brolucizumab have been reported in 36–52% of treatment-naïve eyes, a significant higher proportion compared to 4–5% in the pivotal studies involving Ranibizumab.7,8 This predisposition may be more pronounced in patients previously treated with other anti-VEGF agents, as seen in our series. These antibodies may induce a type 3 hypersensitivity reaction, leading to inflammation. In our series, the mean time to the presentation of IOI was 32 days, supporting the hypothesis of a delayed type 3 hypersensitivity response. Additionally, the IOI occurred after the first injection in 57% of the cases supporting the role of type 3 hypersensitivity in the pathogenesis of IOI. Interestingly, although there was a male preponderance in the cohort treated with Brolucizumab, IOI was more common in females in our study, a trend observed by other investigators. Cases of retinal vasculitis, however, presented earlier (mean of 14 days), suggesting a potential alternative inflammatory pathway.
Expert recommendations for managing Brolucizumab-associated IOI emphasize frequent monitoring and proactive identification of retinal vasculitis or vascular occlusive in patients presenting with IOI.20 We adopted a proactive follow-up strategy, which included a detailed patient history to exclude systemic vasculitis or autoimmune diseases, along with telephonic calls on postoperative day 1 and mandatory clinic visits on days 15 and 30. Our approach resulted in a higher incidence of (4.9%) compared to previous studies from the region, which reported incidence between 0% to 3.6%.10,11,13,14 The OCTOPUS and SWIFT study12 also reported higher IOI detection rates with proactive monitoring, with an incidence of 10.5%, compared to the pivotal HAWK and HARRIER trials. They also reported an earlier detection of IOI, an observation also noted in our study. This study offers valuable insights, particularly for this region, by highlighting the effectiveness of a proactive strategy in monitoring patients receiving Brolucizumab. It may also represent the largest single-center series focused on resistant cases of nAMD/PCV.
It is notable that no cases of IOI were identified through telephone follow-ups, underscoring the importance of clinical examination after brolucizumab injection to detect IOI. At the 2-week follow-up, clinical examinations revealed IOI in 4 out of 7 cases, even though 2 of these patients were asymptomatic during the visit. Similarly, the OCTOPUS and SWIFT trials12 reported that 17.0% of patients with IOI-related events were asymptomatic at time of IOI diagnosis, with no prior complaints. This highlights the potential for IOI to be missed or diagnosed later in the course of inflammation. Based on these findings, we strongly recommend performing a slit-lamp examination and dilated fundus examination at every patient visit following Brolucizumab injection.
When vitritis is detected, it is critical to perform a thorough retina al evaluation using indirect ophthalmoscopy, widefield color fundus photography (CFP), and wide-field FFA to assess for retinal vasculitis or retinal occlusive events, as emphasised by previous studies.20,26 Retinal involvement, particularly in the peripheral retina without macular involvement, may often present without visual symptoms. A recent meta-analysis reported that the incidence of retinal vasculitis and retinal occlusive ranged from 0% to 16.7%, with all affected eyes exhibiting IOI at baseline.12 While subjective symptoms are often used to identify IOI, they can be unreliable as they may not always correspond to the actual severity or location of retinal pathology. This underscores the need for objective assessments and imaging tools to ensure accurate diagnosis.
Early and aggressive management of IOI with potent corticosteroids, combined with close monitoring, may help prevent progression within this spectrum of inflammation.20,26 Retinal vasculitis and IOI associated with brolucizumab injections are characterized by variable degrees occlusion in large or small retinal arteries, often accompanied by perivenular abnormalities. This spectrum ranges from peripheral vasculitis to large retinal artery occlusions around the optic nerve or macula, which can result in severe vision loss.
A high index of suspicion is necessary, as vitreous cells can often obscure the visualization of retinal details.27 Expert recommendations advise that all patients diagnosed with IOI should be evaluated for concomitant retinal vasculitis or vascular occlusion using multimodal imaging, including widefield imaging, FFA (with peripheral sweeps), and OCT.20 However, the lack of standardized imaging protocols can pose challenges in real-world scenarios, making it even more critical to apply comprehensive imaging strategies consistently for accurate diagnosis and effective management.
In our study, two cases of vasculitis were identified in the context of vitritis using peripheral FFA sweeps. Interestingly, the vascular changes observed in brolucizumab-induced vasculitis may result from its potent VEGF inhibition, potentially impacting the uveovascular barrier.28 FFA findings at the time of diagnosis often include delayed or irregular arterial filling and vascular non-perfusion. However, classical signs of vasculitis, such as dye leakage and vascular sheathing, may be subtle or absent. The underutilization of wide-field angiography in previous studies may have contributed to the underdiagnosis or misdiagnosis of brolucizumab-induced IOI, as evidenced by reports of suspected endophthalmitis cases in some series.29 Reports from India have shown inconsistent follow-up protocols, often excluding FFA in suspected vitritis cases.10,11,13,14 Conversely, our proactive monitoring approach likely facilitated the early detection and effective management of severe inflammation, ensuring good resolution without visual loss.
Using the HAWK and HARRIER discomfort grading system,7 IOI severity was classified as mild in 28.6% of eyes, moderate in 42.9%, and severe in 28.6%. Interestingly, the severity of inflammation did not consistently correlate with the degree of inflammation. For instance, a patient with isolated anterior uveitis graded their discomfort as severe, while one of the two vasculitis graded their discomfort as mild. This discrepancy highlights the inadequacy of symptom-based classification in reflecting disease severity or outcomes.
In our study, a PRN regimen was initiated from the first injection rather than following the conventional standard protocol. This decision was influenced by several factors pertinent to our patient population, primarily drawn from developing countries where economic constraints play a significant role in treatment adherence. Many patients come from lower socioeconomic backgrounds, and the high cost associated with continuous treatment can lead to discontinuation. Moreover, Brolucizumab’s rapid activity, particularly its swift macular drying effect, supports a more flexible treatment strategy. By offering retreatment based on changes detected in OCT biomarkers, we aim to maintain therapeutic efficacy while minimizing unnecessary injections. This approach not only addresses the economic burden for patients but also ensures that treatment is administered only when clinically indicated, thus optimizing both patient care and resource allocation.
The American Society of Retina Specialists (ASRS) guidelines recommend withholding anti-VEGF treatment until inflammation resolves.30 While brolucizumab is often avoided after IOI, we successfully reintroduced it in one case alongside topical steroids, without recurrence of IOI. There is no consensus on resuming anti-VEGF therapy following IOI resolution. For example, one SWIFT study patient12 experienced a second IOI episode after three aflibercept injections without associated visual loss. Reports of switching to other anti-VEGF agents, such as aflibercept or ranibizumab, have yielded mixed results. Other studies have reported reintroduction of other anti-VEGFs with varying results. Witkin et al reported occlusive vasculitis in 2 out of 8 patients after switching to aflibercept.30 Conversely, a large Indian retrospective study found no recurrent inflammation in four eyes that continued brolucizumab treatment.10 Data from the HAWK and HARRIER trials showed that 74% of eyes continued receiving brolucizumab post-IOI, with 67% completing follow-up without IOI recurrence.7 Nevertheless, the drug’s prescribing information advises discontinuation if IOI occurs. To our knowledge, this study represents the largest cohort of eyes evaluated with a proactive post-injection monitoring protocol for treatment-resistant nAMD/PC.
The study’s limitations include its retrospective design, single-centre setting, and inability to conduct risk factor analyses comparing eyes that developed IOI with those that did not. Also, we did not perform subgroup analyses by diagnosis or prior treatment due to the study not being powered for these comparisons. Additionally, the follow-up duration was highly variable (4–18 months), with some cases having as low as 4 months of follow-up. This variability may limit the meaningful assessment of safety outcomes. Furthermore, as this study is based on real-world data, it reflects the challenges faced in developing nations, where loss to follow-up is a common occurrence. Finally, our study cohort consisted exclusively of patients with treatment-resistant nAMD or PCV who had previously received multiple anti-VEGF agents. While this population provides valuable insights into IOI incidence in a challenging subset of patients, the findings may not fully represent outcomes in treatment-naïve cohorts or the broader population receiving Brolucizumab. Further studies are needed to explore these differences.
Conclusion
This proactive monitoring protocol revealed a higher incidence of Brolucizumab-associated IOI in treatment-resistant nAMD or PCV than reported in other studies from this region. Early identification of inflammation and prompt treatment contributed to favorable outcomes, with complete resolution and no visual loss. Symptom-based evaluations alone are insufficient for detecting inflammation and do not reflect disease severity. Given that vasculitis may not always present with overt signs, this study highlights the importance of performing FFA in cases of vitritis, as subtle vasculitis may otherwise go undetected. We recommend adopting a proactive monitoring strategy to identify and manage type 3 hypersensitivity reactions associated with Brolucizumab, particularly in Asian eyes, which may predisposed to inflammation. This approach is relevant for both treatment-naïve and previously treated eyes; however, the retrospective nature of our study suggests that further research is needed to validate these recommendations.
Disclosure
J.S. reports support from Shantilal Shanghvi Foundation (SSF), outside the submitted work. All the other author reports no conflicts of interest in this work.
References
1. Korobelnik JF, Do DV, Schmidt-Erfurth U, et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology. 2014;121:2247–2254. doi:10.1016/j.ophtha.2014.05.006
2. Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for diabetic macular edema: results from phase III randomized trials: RISE and RIDE. Ophthalmology. 2012;119:789–801. doi:10.1016/j.ophtha.2011.12.039
3. Gaudreault J, Gunde T, Floyd HS, et al. Preclinical pharmacology and safety of ESBA1008, a single-chain antibody fragment, investigated as potential treatment for age related macular degeneration. Invest Ophthalmol Vis Sci. 2012;53:3025.
4. Tietz J, Spohn G, Schmid G, et al. Affinity and potency of RTH258 (ESBA1008), a novel inhibitor of vascular endothelial growth factor a for the treatment of retinal disorders. Invest Ophthalmol Vis Sci. 2015;56:1501.
5. Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127:72–84. doi:10.1016/j.ophtha.2019.04.017
6. Dugel PU, Singh RP, Koh A, et al. HAWK and HARRIER: ninety-six-week outcomes from the phase 3 trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2021;128:89–99. doi:10.1016/j.ophtha.2020.06.028
7. Monés J, Srivastava SK, Jaffe GJ, et al. Risk of inflammation, retinal vasculitis, and retinal occlusion-related events with brolucizumab: post hoc review of HAWK and HARRIER. Ophthalmology. 2021;128:1050–1059. doi:10.1016/j.ophtha.2020.11.011
8. Singer M, Albini TA, Seres A, et al. Clinical characteristics and outcomes of eyes with intraocular inflammation after brolucizumab: post hoc analysis of HAWK and HARRIER. Ophthalmol Retina. 2022;6:97e108. doi:10.1016/j.oret.2021.05.003
9. Khanani AM, Zarbin MA, Barakat MR, et al. Safety outcomes of brolucizumab in neovascular age-related macular degeneration: results from the IRIS registry and Komodo Healthcare Map. JAMA Ophthalmol. 2022;140:20e28. doi:10.1001/jamaophthalmol.2021.4585
10. Agarwal M, Muralidhar A, Shanmugam MP, et al. Brolucizumab-associated intraocular inflammation in Indian patients by VRSI study group. Indian J Ophthalmol. 2024;72(8):1156–1161. doi:10.4103/IJO.IJO_2973_23
11. Chakraborty D, Mondal S, Sengupta S, et al. Incidence, clinical features, risk factors, and outcomes of Intraocular inflammation following Brolucizumab in Indian eyes - a multicentric study. Indian J Ophthalmol. 2023;71(5):1979–1985. doi:10.4103/IJO.IJO_2688_22
12. Bodaghi B, Souied EH, Tadayoni R, et al. Detection and management of intraocular inflammation after brolucizumab treatment for neovascular age-related macular degeneration. Ophthalmol Retina. 2023;7:879–891. doi:10.1016/j.oret.2023.06.009
13. Chakraborty D, Maiti A, Sheth JU, et al. Brolucizumab in neovascular age-related macular degeneration - Indian real-world experience: the BRAILLE study. Clin Ophthalmol. 2021;15:3787–3795. doi:10.2147/OPTH.S328160
14. Chakraborty D, Maiti A, Sheth JU, et al. Brolucizumab in neovascular age-related macular degeneration - Indian real-world experience: the BRAILLE study - fifty-two-week outcomes. Clin Ophthalmol. 2022;16:4303–4313. doi:10.2147/OPTH.S395577
15. Kim J, Lee SJ, Park TK, et al. Short-term efficacy and safety of intravitreal brolucizumab injection for treatment-naïve exudate age-related macular degeneration; A multicenter study. Korean J Ophthalmol. 2023;37:365–372. doi:10.3341/kjo.2023.0009
16. Bae KW, Kim DI, Hwang DDJ. The effect of intravitreal brolucizumab on choroidal thickness in patients with neovascular age-related macular degeneration. Sci Rep. 2022;12:19855. doi:10.1038/s41598-022-23392-6
17. Yeom H, Kwon HJ, Kim YJ, et al. Real-world study to evaluate the efficacy and safety of intravitreal brolucizumab for refractory neovascular age-related macular degeneration. Sci Rep. 2023;13:11400. doi:10.1038/s41598-023-38173-y
18. Matsumoto H, Hoshino J, Mukai R, Nakamura K, Akiyama H. One-year results of treat-and-extend regimen with intravitreal brolucizumab for treatment-naïve neovascular age-related macular degeneration with type macular neovascularization. Sci Rep. 2022;12:8195. doi:10.1038/s41598-022-10578-1
19. Baumal CR, Sørensen TL, Karcher H, et al. Efficacy and safety of brolucizumab in age-related macular degeneration: a systematic review of real-world studies. Acta Ophthalmol. 2023;101(2):123–139. doi:10.1111/aos.15242
20. Baumal CR, Bodaghi B, Singer M, et al. Expert opinion on management of intraocular inflammation, retinal vasculitis, and vascular occlusion after brolucizumab treatment. Ophthalmol Retina. 2021;5(6):519–527. doi:10.1016/j.oret.2020.09.020
21. Bodaghi B, Khanani AM, Khoramnia R, Pavesio C, Nguyen QD. Gains in the current understanding of managing neovascular AMD with brolucizumab. J Ophthalmic Inflamm Infect. 2023;13(1):51. doi:10.1186/s12348-023-00369-8
22. Witkin AJ, Hahn P, Murray TG, et al. Occlusive retinal vasculitis following intravitreal brolucizumab. J Vitreoretin Dis. 2020;4(4):269–279. doi:10.1177/2474126420930863
23. Karle AC, Wrobel MB, Koepke S, et al. Anti-brolucizumab immune response as one prerequisite for rare retinal vasculitis/ retinal vascular occlusion adverse events. Sci Transl Med. 2023;15:eabq5241.
24. Kearns JD, Wassmann P, Olgac U, et al. A root cause analysis to identify the mechanistic drivers of immunogenicity against the anti-VEGF biotherapeutic brolucizumab. Sci Transl Med. 2023;15:eabq5068.
25. Matucci A, Nencini F, Vivarelli E, et al. Immunogenicity unwanted immune responses to biological drugs can we predict them? Expert Rev Clin Pharmacol. 2021;14:47e53. doi:10.1080/17512433.2020.1772053
26. Sadda SR, Holz FG, Staurenghi G, Invernizzi A, Arnold J, Tadayoni R. The importance of imaging to identify early signs of intraocular inflammation expert opinion for brolucizumab. Ophthalmologica. 2022;245(6):588–591. doi:10.1159/000526703
27. Baumal CR, Spaide RF, Vajzovic L, et al. Retinal vasculitis and intraocular inflammation after intravitreal injection of brolucizumab. Ophthalmology. 2020;127(10):1345–1359. doi:10.1016/j.ophtha.2020.04.017
28. Garweg JG, Hänsli C. Pitfalls in the interpretation of intraocular inflammation in response to intravitreal brolucizumab injection. Ocul Immunol Inflamm. 2023;31(2):249–251. doi:10.1080/09273948.2021.1976220
29. Garweg JG, Keiper J, Pfister IB, Schild C. Functional outcomes of brolucizumab-induced intraocular inflammation involving the posterior segment-a meta-analysis and systematic review. J Clin Med. 2023;12(14):4671. doi:10.3390/jcm12144671
30. Iyer PG, Peden MC, Suñer IJ, Patel N, Dubovy SR, Albini TA. Brolucizumab-related retinal vasculitis with exacerbation following ranibizumab retreatment: a clinicopathologic case study. Am J Ophthalmol Case Rep. 2020;20:100989. doi:10.1016/j.ajoc.2020.100989
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Early Canadian Real-World Experience with Brolucizumab in Anti-Vascular Endothelial Growth Factor-Experienced Patients with Neovascular Age-Related Macular Degeneration: A Retrospective Chart Review
Giunta M, Gauvin Meunier LP, Nixon D, Steeves J, Noble J
Clinical Ophthalmology 2022, 16:2885-2894
Published Date: 30 August 2022
Efficacy, Safety, and Durability of Brolucizumab: An 8-Month Post-Marketing Surveillance Analysis
Saba NJ, Walter SD
Clinical Ophthalmology 2023, 17:2791-2802
Published Date: 20 September 2023