")
Back to Journals » Clinical Ophthalmology » Volume 19
Prognostic Factors for Successful Surgical Outcomes in Trochlear Nerve Palsy: A Retrospective Study and Literature Review
Authors Srimanan W
Received 27 February 2025
Accepted for publication 29 April 2025
Published 5 May 2025 Volume 2025:19 Pages 1489—1503
DOI https://doi.org/10.2147/OPTH.S525257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Worapot Srimanan
Division of Ophthalmology, Phramongkutklao Hospital, Bangkok, Thailand
Correspondence: Worapot Srimanan, Ophthalmology Division, Phramongkutklao Hospital, 315 Ratchawithi Road, Thung Phayathai Subdistrict, Ratchathewi, Bangkok, Thailand, Tel +662-763-9300, Fax +662-354-9309, Email [email protected]
Purpose: Trochlear nerve palsy is a common cause of double vision, particularly vertical diplopia. Surgery might be necessary if the condition does not improve independently. The success of the surgery can vary based on the method employed, and clear factors to predict its effectiveness are not evident. This study evaluates surgical techniques, success rates, and prognostic factors for trochlear nerve palsy at a tertiary hospital.
Patients and Methods: A retrospective chart review was conducted on patients undergoing strabismus surgery for trochlear nerve palsy at Phramongkutklao Hospital between April 2012 and July 2024. Collected data included demographics, visual acuity, stereopsis, etiology, preoperative angles, surgical methods, and postoperative outcomes. A literature review regarding surgical success and prognostic factors was also conducted.
Results: Seventy-two cases were included, with 79.2% involving decompensated congenital trochlear nerve palsy. The overall surgical success rate was 76.39%, and inferior oblique myectomy was the most common and effective procedure (44.4% of cases). Based on multivariate logistic regression analysis, a preoperative hypertropia of ≤ 15 prism diopters was the significant factor for predicting successful outcomes in this study (OR 5.13, 95% CI 1.19– 22.18).
Conclusion: Inferior oblique muscle surgery effectively addresses small-angle deviations in trochlear nerve palsy. A < 15 prism diopters vertical deviation strongly predicted positive surgical outcomes in this study. Further studies are needed to compare surgical techniques and explore additional prognostic factors to optimize long-term outcomes and improve patient care.
Plain Language Summary: Trochlear nerve palsy can lead to double vision, and surgery is required if there is no spontaneous improvement. The success of surgical procedures varies based on technique, and there are limited known predictors for which patients may achieve optimal results. When the condition does not resolve independently, surgery is necessary to rectify eye misalignment. This study explored various surgical methods, their success rates, and the factors affecting favorable outcomes from trochlear nerve palsy surgery.
A review of medical records for 72 patients who underwent surgery for trochlear nerve palsy at Phramongkutklao Hospital between 2012 and 2024 showed that congenital causes were the most prevalent, accounting for 79.2% of cases. The findings indicated that 76.39% of the surgeries were successful, with inferior oblique myectomy being the most effective and frequently performed procedure. The primary predictor for a successful surgery was having a preoperative eye misalignment, specifically hypertropia, of ≤ 15 prism diopters.
Notably, inferior oblique surgery successfully addresses small-angle deviations, with preoperative hypertropia remarkably predicting the surgical success. Further studies are necessary to compare surgical methods and explore other factors that may enhance long-term outcomes.
Keywords: fourth nerve, paresis, prognosis, long-term, surgery, strabismus, neuro-ophthalmology
Introduction
The trochlear cranial nerve exclusively supplies the superior oblique muscle. Isolated or unilateral weakness in this muscle typically results in hypertropia, whereas bilateral weakness often causes torsional diplopia.1,2 Population-based studies on trochlear nerve palsy report an incidence rate of approximately 3.74–5.73 per 100,000 cases annually.1,2 Common etiologies include congenital, presumed vascular, compressive, idiopathic causes, and postinfectious etiology, with varying distributions observed across studies.1–3 Notably, congenital forms are the most frequently identified, accounting for 49%–76.7% of cases.2–4 However, some case series suggest a predominance of acquired causes in specific cohorts.3
The recovery rate of trochlear nerve palsy varies substantially, with estimates ranging from 24.6% to 82.6%.5–7 Partial recovery lowered the quality of life, resulting in diplopia, compensatory head posture, and visual issues. The treatment options for patients with partial or nonrecovery include conservative approaches, such as patching, prisms, eyeglasses, and surgical interventions. Surgical procedures typically address vertical misalignment and often involve inferior oblique weakening, superior oblique tucking, or vertical rectus muscle weakening, which can be performed individually or in combination based on the measured deviation. Conversely, individualized surgical planning is essential for managing torsional diplopia.8 The reported success rates of surgery for trochlear nerve palsy range from 61.9% to 100%, with outcomes varying based on the surgical technique employed and the criteria used to define success.4,9–19 Inferior oblique myectomy, inferior oblique anterior transposition, and superior oblique tucking achieve success rates of 61.9%–94.7%,12,14,15 89%–100%,12,15 and 85.19%,18 respectively. However, inferior oblique recession, a less commonly performed technique, has received limited attention in the literature, with a reported success rate of 84.2% in one study.11 The lack of comprehensive data on inferior oblique recession limits direct comparisons with other techniques. Additionally, a study conducted in Thailand reported an overall surgical success rate of 82.75%. However, specific procedures were not delineated.20 This highlights the need for further research on surgical outcomes in diverse populations, particularly within Southeast Asia, to bridge the existing knowledge gaps.
Despite extensive reporting on surgical outcomes, a comprehensive understanding of the prognostic factors influencing success remains elusive. Previous studies identified amblyopia,16 older age,13,21 and larger vertical deviations13,22 as predictors of the need for reoperation. Thus, identifying additional factors is essential for guiding clinical decision-making and improving patient care. This report examined the types of surgical procedures performed, their long-term success rates, and the factors influencing favorable outcomes in trochlear nerve palsy treatment in a tertiary hospital setting.
Materials and Methods
Study Participants
This retrospective study collected data from individuals with strabismus. Electronic data was retrospect from April 1, 2012, to July 31, 2024. I used the International Classification of Diseases, Ninth Revision (ICD-9) codes 15.1–15.9 to find strabismus procedures, matching with ICD-10 code H491 for trochlear nerve palsy. I collected general data, including age, sex, onset duration, diagnosis, stereopsis, ocular version, preoperative angle, and surgery outcomes during the following period.
Inclusion criteria were individuals who had trochlear nerve palsy and received strabismus surgeries for the first time in only one cyclovertical muscle with complete data collected. Participants must be postoperatively followed and receive the examination at least four times annually. The exclusion criteria were individuals who had trochlear nerve palsies with previous surgery and incomplete data.
A total of 92 cases received surgical treatment, 20 of which were excluded due to missing data. Hence, this study included the remaining 72 cases. Figure 1 shows the flowchart of participant recruitment.
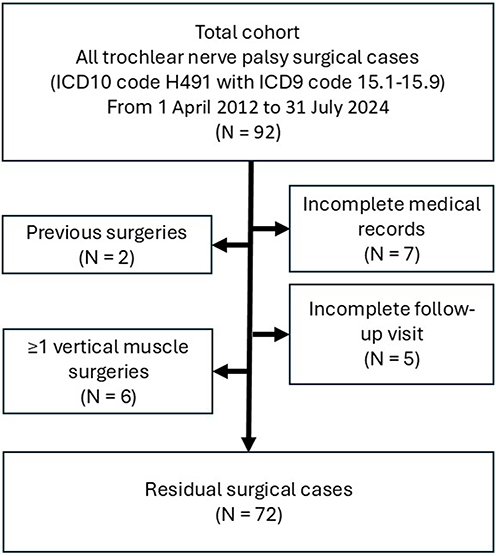 |
Figure 1 Flowchart of participant recruitment. Abbreviations: ICD, International Classification of Diseases; N, number of participants. |
Disease Definition
Trochlear nerve palsy is a trochlear nerve weakness that causes vertical diplopia with or without excyclotorsional symptoms. Congenital cases have typical features, including facial asymmetry, large vertical fusional amplitude, and absence of torsional diplopia.
Data Gathering
I collected each participant’s demographic data, including age, sex, symptom duration, etiology, visual acuity, refractive error, preoperative head tilt, stereopsis, preoperative deviation angle, and surgical outcomes over time. Stereopsis was assessed using the Randot stereo test, with results presented in arcseconds. A strabismus specialist conducted all strabismus evaluations. A grading scale from 1+ to 4+ assessed inferior oblique overaction and superior oblique underaction. Visual acuity was measured as a Log Mar unit, and subjective refraction was measured. A contour stereo test was used for stereopsis measurement.
A comprehensive literature search was conducted using the PubMed database for English-language articles published between January 1, 2016, and June 30, 2024. Specific search keywords included “trochlear nerve palsy”, “fourth nerve palsy”, “strabismus surgery”, “muscle surgery”, “inferior oblique myectomy”, “inferior oblique recession”, “inferior oblique anterior transposition”, and “inferior oblique weakening”. I searched for relevant studies that included success rates and, principally, prognostic factors related to trochlear nerve palsy surgery. Our review comprised original research articles and case series. Case reports are excluded from the review of surgical outcomes in trochlear nerve palsy due to their limited sample size, lack of statistical significance, and absence of standardized methodology, which can reduce the reliability and generalizability of conclusions drawn from such isolated cases.
Surgeries
Participants’ surgeries focused on a single cyclovertical muscle, operated on using one of three surgical techniques: inferior oblique myectomy, inferior oblique recession, and inferior oblique anterior transposition. Inferior oblique myectomy is a surgical procedure in which a portion of the inferior oblique muscle is removed to weaken its function. The inferior oblique recession technique used graded recession guidelines.21 The inferior oblique anterior transposition technique attaches the inferior oblique’s insertion point 2 mm posterior to the point of inferior rectus insertion. Successful surgery was defined as ocular alignment within five prism diopters without diplopia symptoms. Three surgeons performed all surgeries during data collection.
Statistical Analysis
Descriptive statistics were used to distinguish demographic data for the sample group from the general data. Group data regarding the amount and percentage of quantitative data were analyzed. The mean for a normal distribution was measured along with the mean and standard deviation. The average value for irregular distribution was summed with the median. Numbers and percentages represent clustered data.
I used the Mann–Whitney U-test for continuous variables and Fisher’s exact categorical variables to compare outcomes between successful and unsuccessful surgical groups in trochlear nerve palsy surgery. I used a logistic regression analysis to assess prognostic factors influencing surgical success. Univariate logistic regression analyses were used to adjust for patient age, preoperative hypertrophic angle, head tilt, and stereopsis and mitigate potential bias. Patients’ ages were categorized as younger (<15 years) or older (≥15 years). Preoperative hypertropia was classified as small (≤15 prism diopters) or large (>15 diopters). Stereopsis was categorized as good (≤200 arcseconds) or poor (>200 arcseconds). Patients’ preoperative head tilts were grouped by degree: small (<5°) or large (≥5°). Because there were so few unsuccessful cases, multivariate analysis could not be performed on patients with poor surgical outcomes. A significant p-value of <0.05 was applied to identify statistical significance. Stata 14 (StataCorp LLC, the USA) was utilized for analysis.
Ethics Approval
The study was approved by the Institutional Review Board of the Royal Thai Army Medical Department (approval number S066h/67_Exp). Due to its retrospective nature, the Royal Thai Army Medical Department waived the need for informed consent. This study was conducted following the principles of the Declaration of Helsinki.
Results
Patient Demography
Table 1 presents the demographic data of the 72 patients included in this report. The average age was 21.32 years, with slightly predominantly women (n = 37). The mean onset duration of trochlear nerve palsy was 5.51 ± 4.07 years, and most cases (57/72, 79.2%) involved congenital trochlear nerve palsy. The average preoperative hypertropia was 12.64 ± 4.11 prism diopters, the mean preoperative head tilt was 3.36° ± 2.06°, and the mean preoperative stereopsis was 157.29 ± 183.3 arcseconds. The overall surgical success rate was 76.39% (55/72). Among the surgical methods, 44.44% involved inferior oblique myectomy. According to the Knapp classification, 81.9% (59/72) were type 1, 5.6% (4/72) were type 3, and 12.5% (9/72) were type 4.
 |
Table 1 Mann–Whitney U-Test of Preoperative Demographic Data in Patients With Trochlear Nerve Palsy |
Table 1 shows that the younger age group, degree of inferior oblique overaction, superior oblique underaction, preoperative stereopsis, preoperative angle, Knapp type, and inferior oblique myectomy were significantly associated with good surgical outcomes (p < 0.05).
Surgical Success Rates
Table 2 presents postoperative outcomes up to 12 months, including reoperation data. The average postoperative hypertropia at 12 months was 3.19 ± 3.25 prism diopters, and the mean postoperative stereopsis was 182.54 ± 228.13 arcseconds. By the 12-month follow-up appointment, 61.1% (44/72) of the cases demonstrated residual hypertropia, whereas 38.9% (28/72) achieved orthotropia. No instances of consecutive hypotropia were observed. Postoperative head tilt decreased to 2.08° ± 1.82°. The reoperation rate was relatively low at 8.3% (6/72), and no complications were reported in the study population.
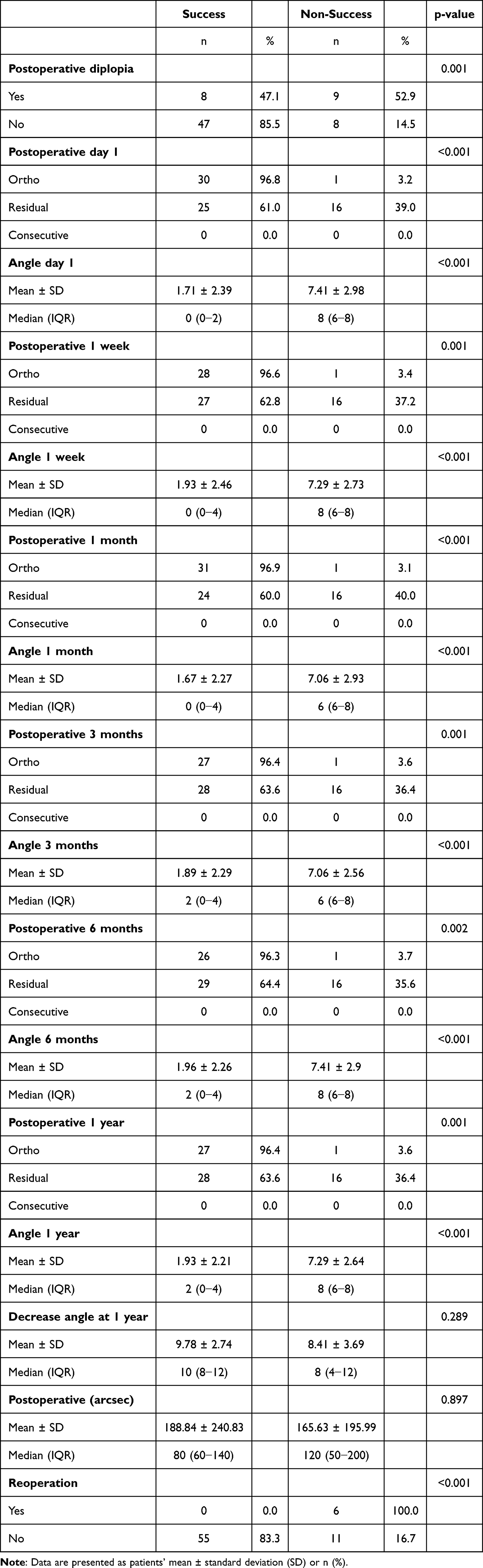 |
Table 2 Mann–Whitney U-Test of Trochlear Nerve Palsy Outcomes |
Table 3 summarizes the logistic regression analysis results, identifying factors significantly associated with successful surgical outcomes. Multivariate logistic regression revealed that a preoperative hypertropia angle of ≤15 prism diopters was significantly associated with favorable outcomes with adjusted odds ratios of 5.13 (95% confidence interval (CI), 1.19–22.18).
 |
Table 3 Multivariate Analysis of Preoperative Factors That Promoted Successful Trochlear Nerve Palsy Surgery Outcomes |
Discussion
Previous studies have reported high surgical success rates for trochlear nerve palsy surgery;4,9–19 however, the prognostic factors influencing the optimal outcomes remain unclear. Our analysis identified a smaller preoperative hypertrophic angle as a significant predictor of excellent surgical outcomes by 12 months postoperatively. Moreover, patients in our cohort most commonly presented with Knapp type 3, and inferior oblique myectomy was the most frequently performed and most successful surgery.
Smaller preoperative hypertropia angles were significantly associated with favorable surgical outcomes in patients with trochlear nerve palsy who underwent single-muscle inferior oblique surgery. Our results are congruent with the findings of previous studies indicating that inferior oblique weakening procedures effectively correct hypertropia of <20 prism diopters.11,22–25 However, by focusing exclusively on patients who underwent single-muscle surgery, our study reveals targeted evidence that preoperative deviations of ≤15 prism diopters particularly predict successful outcomes. This finding validates the role of preoperative deviation magnitude in guiding surgical decision-making, as patients with larger deviations may require additional cyclovertical muscle procedures to achieve optimal alignment.
Univariate analysis revealed that good preoperative stereopsis (≤140 arcseconds) and younger age (<15 years) were significantly associated with favorable surgical outcomes. However, these associations lost significance in multivariate analysis, indicating that other variables, such as preoperative hypertropia, may mediate their effects. Furthermore, previous studies have determined both factors as crucial prognostic indicators for successful strabismus surgery, particularly in trochlear nerve palsy. Our results do not establish them as independent predictors, but they highlight potential trends that warrant further investigation in larger cohorts to determine their specific role in surgical outcomes.
Younger age has been a significant factor affecting trochlear nerve palsy surgical outcomes, probably due to greater vertical fusional capacity, fewer comorbidities, and improved postoperative healing, all contributing to improved alignment stability. Our results are congruent with Aoba et al13 and Lau et al21 reporting poorer outcomes and higher reoperation rates in older patients. However, conflicting evidence exists. Khanna et al23 reported superior motor outcomes in older patients, whereas Lee et al10 revealed that younger patients were less likely to experience motor function and head tilt improvements. These various results highlight the complexity of age-related factors in surgical success, emphasizing the need for further research to delineate its precise effect.
Similarly, good preoperative stereopsis (≤140 arcseconds) was associated with favorable postoperative ocular alignment 1 year after surgery. Strong preoperative binocular vision may enhance fusional amplitude in cases of residual hypertropia, particularly in congenital trochlear nerve palsy, facilitating long-term ocular stability. However, our study did not assess distant stereopsis, which may also affect surgical outcomes. Future research should explore the relationship between distant stereopsis and postoperative alignment to refine patient selection criteria and optimize long-term success.
I found that inferior oblique myectomy was associated with favorable long-term surgical outcomes; however, inferior oblique recession produced worse outcomes in our cohort. Previous studies found that inferior oblique anterior transposition was more effective than myectomy; however, it carries a risk of inducing antielevation syndrome.2,15 Although less common, inferior oblique recession has also shown positive outcomes in some studies.11 To the best of my knowledge, this was the first study that compared these three techniques and concluded that inferior oblique myectomy is the most effective procedure potentially, because of the subjective nature of quantifying inferior oblique overaction, which can lead to inaccuracies when planning for recession, exacerbating the weakening effects of the recession and contributing to suboptimal outcomes. Conversely, inferior oblique myectomy and anterior transposition rely less on precise measurements of overaction, explaining their more consistent success as surgical correction techniques.
Knapp classification was formerly categorized as a type of superior oblique muscle palsy. Compared to types 3 and 4, type 1 was the most prevalent and associated with the best surgical outcomes. Type 1 subjects had the worst hypertropia when examining the field of action of the inferior oblique muscle, reflecting inferior oblique overaction. These patients could have benefited from the inferior oblique muscle weakening procedure. Type 3 and 4 patients demonstrated significantly superior oblique muscle underaction, necessitating the superior oblique muscle strengthening procedure. Consequently, these patients are more likely to experience poor outcomes.
A literature review was conducted using the PubMed database to evaluate recent trochlear nerve palsy surgery data. Search terms included “trochlear nerve palsy”, “fourth nerve palsy”, “surgery”, and “success”. Table 4 summarizes the surgical techniques and outcomes from studies published since 2016. Only studies examining inferior oblique weakening procedures were included.
 |
Table 4 Success Rate of Strabismus Surgery in Trochlear Nerve Palsy |
Success rates for trochlear nerve palsy surgery differ widely, ranging from 45.5% to 97.3% across different procedures.10–12,14–19,23,25 Most studies report high success rates despite success criteria, follow-up duration, and surgical approach variations. Inferior oblique myectomy and anterior transposition are the most prevalently studied procedures. Farid et al12 revealed that anterior transposition was more effective than myectomy in correcting hypertropia but was associated with a higher antielevation syndrome incidence. Similarly, Jafari et al15 reported superior outcomes for anterior transposition over myectomy in reducing strabismus angles. Our results are congruent with the findings of these studies, indicating high success rates for both procedures, with myectomy slightly outperforming anterior transposition. Reports on inferior oblique recession outcomes remain limited, and no studies have directly compared its efficacy with other techniques.11
The prognostic factors affecting surgical success remain unclear. Sanz et al16 assessed 76 patients but revealed no significant predictors. However, amblyopia was associated with an increased likelihood of reoperation (p = 0.04). Long-term outcomes differ, but surgical intervention generally improves ocular alignment and reduces diplopia in trochlear nerve palsy. Thus, future research should focus on refining surgical techniques, optimizing patient selection, and determining additional prognostic factors to improve long-term outcomes.
Limitations
Notably, our study had some limitations. First, its retrospective design carried a risk of selection bias and incomplete data. Second, the small sample size might have reduced our analysis’s statistical power, potentially affecting our findings’ robustness. Third, as this was a single-center study, the results might not be generalizable to broader populations. Fourth, the follow-up period was limited, potentially overlooking long-term or delayed outcomes. Finally, the absence of a control group restricted our ability to compare surgical outcomes with alternative treatment modalities, including nonsurgical interventions and other surgical techniques. Future multicenter prospective studies with larger sample sizes and longer follow-up periods are warranted to validate our findings.
Conclusion
This study revealed a high success rate for isolated inferior oblique muscle surgery in trochlear nerve palsy. A small preoperative hypertrophic angle (≤15 prism diopters) was significantly associated with favorable outcomes. Furthermore, younger age and good preoperative stereopsis demonstrated positive trends, although further studies are warranted to confirm their independent effects. These results reinforce the importance of preoperative assessment in surgical planning. Future research should focus on optimizing patient selection, refining surgical techniques, and assessing the long-term stability of surgical outcomes.
Abbreviations
ICD-9, International Classification of Diseases, Ninth Revision; ICD-10, International Classification of Diseases, tenth Revision; USA, United States of America; CI, Confidence interval.
Data Sharing Statement
This article includes all data generated or analyzed during this study. Further inquiries should be directed to the corresponding author.
Ethics Approval and Informed Consent
The Royal Thai Army Medical Department Institutional Review Board reviewed and approved the study protocol (approval number S066h/67_Exp). This study has been performed following the principles stated in the Declaration of Helsinki. Written informed consent for publication was waived because of the retrospective nature of the study. Participant data were kept anonymous and confidential.
Acknowledgments
I sincerely thank Dr. Thitiporn Ratanapojnart, Chief Director of the Ophthalmology Department at Phramongkutklao Hospital, for her invaluable support and guidance throughout this study. Her expertise and leadership were instrumental in the successful completion of this research.
Funding
There is no funding to report.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Jung EH, Kim SJ, Lee JY, Cho BJ. The incidence and presumed aetiologies of fourth cranial nerve palsy in Korea: a 10-year nationwide cohort study. Eye. 2021;35(11):3012–3019. doi:10.1038/s41433-020-01374-0
2. Dosunmu EO, Hatt SR, Leske DA, Hodge DO, Holmes JM. Incidence and etiology of presumed fourth cranial nerve palsy: a population-based study. Am J Ophthalmol. 2018;185:110–114. doi:10.1016/j.ajo.2017.10.019
3. Mollan SP, Edwards JH, Price A, Abbott J, Burdon MA. Aetiology and outcomes of adult superior oblique palsies: a modern series. Eye. 2009;23(3):640–644. doi:10.1038/eye.2008.24
4. Bagheri A, Fallahi MR, Abrishami M, Salour H, Aletaha M. Clinical features and outcomes of treatment for fourth nerve palsy. J Ophthalmic Vis Res. 2010;5(1):27–31.
5. Park UC, Kim SJ, Hwang JM, Yu YS. Clinical features and natural history of acquired third, fourth, and sixth cranial nerve palsy. Eye Lond Engl. 2008;22(5):691–696.
6. Phuljhele S, Dhiman R, Sharma M, et al. Acquired ocular motor palsy: current demographic and etiological profile. Asia Pac J Ophthalmol (Phila). 2020;9(1):25–28. doi:10.1097/01.APO.0000617940.70112
7. Srimanan W, Panyakorn S. Retrospective analysis of factors related to the long-term recovery of third, fourth, and sixth cranial nerve palsy with etiologies and clinical course in a tertiary hospital. Clin Ophthalmol. 2024;18:441. doi:10.2147/OPTH.S449127
8. Helveston EM, Mora JS, Lipsky SN, et al. Surgical treatment of superior oblique palsy. Trans Am Ophthalmol Soc. 1996;94:315–328.
9. Simons BD, Saunders TG, Siatkowski RM, et al. Outcome of surgical management of superior oblique palsy: a study of 123 cases. Binocul Vis Strabismus Q. 1998;13(4):273–282.
10. Lee JE, Yang HK, Hwang JM. Surgical outcomes of inferior oblique myectomy in unilateral congenital superior oblique palsy with or without trochlear nerve. PLoS One. 2016;11(7):e0156872. doi:10.1371/journal.pone.0156872
11. Haugen OH, Nepstad L. A standardized recession of the inferior oblique extraocular muscle–a safe and self‐grading surgical procedure for trochlear nerve palsy: a 10‐year material. Acta Ophthalmol. 2019;97(5):491–496. doi:10.1111/aos.13988
12. Farid MF, Anany M, Abdelshafy M. Surgical outcomes of three different weakening procedures of inferior oblique muscle in the treatment of unilateral superior oblique palsy. BMC Ophthalmol. 2020;20(1):298. doi:10.1186/s12886-020-01568-w
13. Aoba K, Matsuo T, Hamasaki I, Hasebe K. Clinical factors underlying a single surgery or repetitive surgeries to treat superior oblique muscle palsy. Springerplus. 2015;4(1):166. doi:10.1186/s40064-015-0945-3
14. Akbari MR, Sadrkhanlou S, Mirmohammadsadeghi A. Surgical outcome of single inferior oblique myectomy in small and large hypertropia of unilateral superior oblique palsy. J Pediatr Ophthalmol Strabismus. 2019;56(1):23–27. doi:10.3928/01913913-20180925-03
15. Jafari K, Gibbings N, Jain S. Inferior oblique overaction in trochlear nerve palsy: anterior transposition versus myectomy. J Am Assoc Pediatr Ophthalmol Strabismus. 2021;25(1):18.e1–18.e5. doi:10.1016/j.jaapos.2020.10.008
16. Sanz PM, Escribano J, de Liaño P G, Yela R. Surgical treatment of superior oblique palsy: predictors of outcome. Indian J Ophthalmol. 2017;65(8):723–728. doi:10.4103/ijo.IJO_699_16
17. Pruett JK, Umfress AC, Donahue SP. Surgical management of superior oblique palsy with coexisting exotropia. J Am Assoc Pediatr Ophthalmol Strabismus. 2023;27(5):283.e1–283.e4. doi:10.1016/j.jaapos.2023.08.002
18. Dwivedi R, Marsh IB. Superior oblique tuck: evaluation of surgical outcomes. Strabismus. 2019;27(1):24–29. doi:10.1080/09273972.2018.1559204
19. Torrado LA, Brodsky MC. Superior oblique palsy: efficacy of Isolated inferior oblique recession in cases with ipsilateral hypertropia in abduction. J Binocul Vis Ocul Motil. 2019;69(1):8–12. doi:10.1080/2576117X.2018.1554931
20. Surachatkumtonekul T, Soontrapa P, Kampanartsanyakorn S, Dulayajinda D. Causes and treatment outcomes of third, fourth and sixth cranial nerve palsy. J Med Assoc Thail Chotmaihet Thangphaet. 2012;95(Suppl 4):S96–S101.
21. Lau FHS, Fan DSP, Sun KKW, CBO Y, Wong CY, Lam DSC. Residual torticollis in patients after strabismus surgery for congenital superior oblique palsy. Br J Ophthalmol. 2009;93(12):1616–1619. doi:10.1136/bjo.2008.156687
22. Yau GSK, Tam VTY, Lee JWY, Chan TTK, Yuen CYF. Surgical outcomes for unilateral superior oblique palsy in Chinese population: a retrospective study. Int J Ophthalmol. 2015;8(1):107–112. doi:10.3980/j.issn.2222-3959.2015.01.20
23. Khanna RK, Thoreau B, Jean-Lechner M, et al. Postoperative outcomes for unilateral congenital trochlear nerve palsy: a retrospective cohort study. J Fr Ophtalmol. 2024;47(2):104012. doi:10.1016/j.jfo.2023.05.034
24. Raoof N, Burke JP. Isolated inferior oblique myectomy for vertical deviations of at least 20 prism diopters in the primary position. J AAPOS. 2016;20(2):112–116. doi:10.1016/j.jaapos.2015.11.009
25. Sefi-Yurdakul N, Gucyetmez V. Inferior oblique overaction: the results of myectomy in cases with a primary position vertical deviation less and more than 20 prism diopters. Middle East Afr J Ophthalmol. 2020;27(2):117–122. doi:10.4103/meajo.MEAJO_150_19
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.