")
Back to Journals » Journal of Inflammation Research » Volume 18
Prognostic Value of the Preoperative Lymphocyte‐to‐Monocyte Ratio for Postoperative Adverse Events in Patients with Acute Type a Aortic Dissection
Authors Jia L, Wang Y, Wang J, Lin Y, Wang C, Chen C
Received 28 August 2024
Accepted for publication 21 December 2024
Published 10 January 2025 Volume 2025:18 Pages 519—529
DOI https://doi.org/10.2147/JIR.S490339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Limin Jia,1 Yanfeng Wang,2 Junqiang Wang,1 Yulian Lin,1 Chunguo Wang,1 Caihua Chen1
1Department of Cardiothoracic Surgery, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Taizhou, Zhejiang, People’s Republic of China; 2Department of Geriatrics, Taizhou Central Hospital (Taizhou University Hospital) of Zhejiang, Taizhou, Zhejiang, People’s Republic of China
Correspondence: Caihua Chen, Department of Cardiothoracic Surgery, Taizhou Hospital of Zhejiang Province affiliated to Wenzhou Medical University, No. 150, Ximen Street, Linhai City, Taizhou, Zhejiang, 317000, People’s Republic of China, Tel +86-13867656416, Email [email protected]
Objective: To investigate the prognostic value of the preoperative lymphocyte‐to‐monocyte ratio (LMR) for postoperative adverse events in patients with acute type A aortic dissection (ATAAD).
Methods: A retrospective study of the clinical data collected in our hospital between March 2015 and January 2024 was performed on 290 patients diagnosed with ATAAD who underwent surgical treatment and met the inclusion criteria for patient selection. The included patients were divided into a low LMR group (< 1.70, 50 cases) and a high LMR group (≥ 1.70, 51 cases). Clinical data, including white blood cell counts (WBCs), D-dimer (D-D) levels, lymphocyte count (LYM) and platelet count (PLT), were compared between the two groups. Logistic regression analysis assessed the association between the preoperative LMR and postoperative adverse events.
Results: The high LMR group had lower WBCs and NEU than the low LMR group (P < 0.05). The high LMR group also had higher LYM than the low LMR group (P < 0.05). Within 30 days postoperative, the all‐cause mortality rate was higher in the low LMR group than in the high LMR group (P = 0.047). Within 1 year postoperative, the incidence of aortic adverse events (AAEs) (P = 0.010), Re-intervention events (P = 0.011) and Cardiovascular and cerebrovascular adverse events (P < 0.001) has no difference between the high LMR group and the low LMR group. Logistic regression analysis indicated that the preoperative LMR was a significant prognostic marker for AAEs within 30 days and 1 year postoperative.
Conclusion: The preoperative LMR is a prognostic indicator of all‐cause mortality within 30 days and 1 year postoperative in patients with ATAAD.
Keywords: lymphocyte‐monocyte ratio, acute type A aortic dissection, adverse aortic event
Introduction
Aortic dissection (AD) is a critical aortic condition with a low incidence and a high mortality rate.1 The annual incidence ranges from 2.5 to 15 per 100,000 cases.2 This condition primarily occurs due to a tear in the aortic intima, allowing blood to enter and dissect the layers of the aortic wall, creating a false lumen that runs parallel to the true aortic lumen.3 This false lumen can extend along the direction of the tear, affecting many important distal branches and leading to severe complications or even death.4 The Stanford system, introduced in 1970, is the most commonly used classification system for AD.5,6 Patients with Stanford type A AD (TAAD) are at a higher risk of experiencing complications such as dissection rupture, cardiac tamponade and heart failure than those with Stanford type B AD (TBAD). Consequently, the 30‐day mortality rate for patients with TAAD is 2–3 times higher than that for other types of AD.7 Acute Stanford type A AD (ATAAD) refers to TAAD cases within 14 days of onset, accounting for 58%–62% of all AD cases.7,8 The overall mortality rate for ATAAD is approximately 73%, with 18%–49% of patients dying before reaching the hospital.2,9
The mainstay of treatment for patients with ATAAD includes medical therapy and surgical intervention. In contrast, different from high mortality rate of medical therapy, surgical treatment has been found to reduce the 30-day or in-hospital mortality rate to 5%–24%.10 Therefore, guidelines describe surgery as the treatment of choice for patients with ATAAD.11 However, the procedure for ATAAD is complex, with high rates of complications and mortality. For cardiac surgeons, preventing life-threatening postoperative complications in patients with ATAAD is one of the greatest challenges. Therefore, it is crucial to identify as many factors as possible that affect postoperative outcomes in these patients.
The pathogenesis of ATAAD is highly complex, involving hereditary diseases (such as Marfan syndrome and bicuspid aortic valve malformation, which are recognised as definite risk factors for ATAAD), uncontrolled hypertension (HP), aortic atherosclerosis, trauma or iatrogenic injury.12 Currently, risk factors such as advanced age, obesity, preoperative nerve injury, massive blood transfusion, operation time, poor tissue and organ perfusion and hemodynamic impairment caused by cardiac tamponade or inadequate coronary artery perfusion are considered independent predictors of mortality in patients with ATAAD. However, these risk factors still do not fully meet the needs of clinical practice.13 Existing evidence shows that coagulation system disorders and severe inflammatory responses during AD are closely associated with poor postoperative outcomes. White blood cells, platelets and D-dimer (D-D) have been identified as independent risk factors for postoperative prognosis in related studies.14 Novel composite inflammatory markers, such as the neutrophil-to-lymphocyte ratio (NLR), the platelet-to-lymphocyte ratio (PLR), the lymphocyte-to-monocyte ratio (LMR) and the platelet-to-neutrophil ratio, have gained attention in research because relevant data can be obtained from basic tests and simple calculations, demonstrating high prognostic value in coronary artery disease and other cardiovascular conditions.15–17 The LMR has been increasingly recognised as a significant inflammatory marker in various cardiovascular diseases, including ATAAD.18 In the context of ATAAD, the LMR has been investigated for its potential role as a prognostic indicator. Research suggests that the LMR may reflect the balance between pro-inflammatory and anti-inflammatory processes, which is crucial in the pathogenesis of ATAAD and its complications. Several studies have explored the association between the LMR and postoperative outcomes in patients with ATAAD. One study found that an elevated baseline LMR was independently associated with a lower risk of postoperative acute kidney injury (AKI) in patients with ATAAD.19 This suggests that the LMR could serve as a protective factor against AKI following emergency cardiac surgery for ATAAD. The available evidence supports the notion that the LMR is not only a marker of systemic inflammation but also a potential prognostic factor in ATAAD. Higher LMR values may indicate a better prognosis by being associated with a lower risk of postoperative complications such as AKI. However, further research is needed to fully understand the mechanisms by which the LMR influences outcomes in ATAAD and to validate its use as a clinical biomarker.
Studies have shown that the NLR and the PLR are associated with the early prognosis of ATAAD.20 However, the impact of the LMR on the early prognosis of ATAAD remains controversial. With continuous advancements in surgical techniques and diagnostic methods, more indicators are now available to aid in making detailed prognostic predictions for patients. Against this backdrop, this study investigates whether the preoperative LMR is associated with an increased incidence of early postoperative adverse events and whether an elevated preoperative LMR is an independent predictor of early adverse events in patients with ATAAD.
Study Participants and Methods
Study Participants
This study retrospectively collected clinical data from 290 hospitalised patients diagnosed with ATAAD in the department of cardiovascular surgery between March 2015 and January 2024. Based on the following inclusion and exclusion criteria, 189 patients were excluded, and 101 patients who underwent surgical treatment were ultimately included in this study.
The inclusion criteria were as follows: (1) patients diagnosed with TAAD based on symptoms, full-course aortic computed tomography angiography (CTA) and surgical confirmation; (2) patients with an onset time of less than 14 days; (3) patients aged 18 years or older with no family history of hereditary diseases; and (4) patients who underwent surgery via median sternotomy with cardiopulmonary bypass support.
The exclusion criteria were as follows: (1) patients with missing critical data; (2) patients who abandoned surgery or whose dissection ruptured before surgery and did not receive surgical treatment; (3) patients with concurrent rheumatic immune diseases, haematological diseases, malignant tumours or severe trauma that could affect laboratory results; (4) patients with concomitant heart failure or severe liver and kidney failure; (5) pregnant patients; (6) patients undergoing a second cardiac surgery; (7) patients on long-term use of glucocorticoids, immunosuppressants or other medications affecting laboratory test results; and/or (8) patients who used anticoagulant drugs, such as aspirin or clopidogrel, before hospitalisation and could not undergo surgery in the near term.
Methods
Diagnostic Criteria
The diagnosis and staging of AD were performed according to the Chinese experts’ consensus on the standardised diagnosis and treatment for acute aortic syndrome.21 The staging was as follows: (1) acute phase dissection: dissection diagnosed within 14 days of symptom onset; (2) subacute phase dissection: dissection diagnosed between 15 and 90 days of symptom onset; and (3) chronic phase dissection: dissection diagnosed more than 90 days after symptom onset.
Surgical Procedures
Patients diagnosed with ATAAD via aortic CTA in the emergency department were transferred to the intensive care unit (ICU) for close monitoring and stabilisation before surgery. Preoperative preparations included cardiac ultrasound, routine blood tests and coagulation assessments. The surgery began with the patient under general anaesthesia, positioned supine and central venous access was obtained. A median sternotomy was performed to expose the ascending aorta, aortic arch and its branches. Cardiopulmonary bypass was initiated, and the aortic root was incised for the Bentall procedure, which involves replacing the aortic valve and ascending aorta with a valved conduit. The patient’s body temperature was lowered to facilitate the procedure. Selective cerebral perfusion was maintained during arch replacement. The frozen elephant trunk technique was employed to insert a stent graft into the descending aorta, followed by anastomosis of a four-branched graft to the stent graft and the patient’s arteries.
After ensuring thorough de-airing, circulation was restored, and the patient was gradually rewarmed. The distal end of the valved conduit was anastomosed to the graft, and mediastinal drainage tubes were placed before chest closure. The patient was sent to intensive care unit for postoperative care until the condition was stable.
Postoperative Follow‐up
Patients were routinely instructed to visit the outpatient clinic of our centre for follow-up examinations at 1, 6 and 12 months postoperatively. The follow-up data for this study were primarily collected from the electronic medical record system and outpatient follow-up records. If patients did not adhere to the scheduled follow-up visits, their condition was assessed via telephone interviews.
Endpoints include: (1)Aortic adverse events (AAEs); (2)Re-intervention events; including Endoleak, a new tear in the endograft itself and etc. (3)Multiple Organ Dysfunction Syndrome (MODS); (4)Cardiovaseular and cerebrovascular adverse events; and (5)All-cause mortality.
Data Collection
Baseline data, imaging findings and preoperative and postoperative laboratory test results were collected from the patients. Baseline data included age, height, weight, sex, heart rate and comorbidity. Laboratory test data included haematological parameters, such as white blood cell count (#WBC), neutrophil count, lymphocyte count (#LYM), monocyte count and platelet count (#PLT); the LMR; liver and kidney function parameters, such as creatinine, albumin and globulin levels; and coagulation function parameter (D-D).
Statistical Analysis
Statistical analyses were conducted using the software SPSS 26.0. The Kolmogorov–Smirnov test was employed to assess normality. Normally distributed measurement data were expressed as mean ± standard deviation and analysed using the independent samples t‐test. Non‐normally distributed measurement data were expressed as median (Q1, Q3) and compared using the Mann–Whitney U-test. Categorical data were represented by frequencies (n) or percentages (%) and analysed using the chi‐squared (χ²) test or Fisher’s exact test. Kaplan–Meier survival curves were utilised to compare the 1-year postoperative incidence rates of freedom from aortic adverse events (AAEs), all‐cause mortality and freedom from cardio‐cerebrovascular adverse events between the groups. Logistic regression analysis was used to explore the relationship between LMR and prognosis. Logistic analysis: The potential variables with P < 0.1 in univariate analysis are further included in multivariable analysis. The log‐rank test was used to compare differences between the groups. Receiver operating characteristic (ROC) curves were employed to assess the prognostic value of different parameters. A two‐tailed P‐value of less than 0.05 was considered to be statistically significant.
and analysed using the independent samples t‐test. Non‐normally distributed measurement data were expressed as median (Q1, Q3) and compared using the Mann–Whitney U-test. Categorical data were represented by frequencies (n) or percentages (%) and analysed using the chi‐squared (χ²) test or Fisher’s exact test. Kaplan–Meier survival curves were utilised to compare the 1-year postoperative incidence rates of freedom from aortic adverse events (AAEs), all‐cause mortality and freedom from cardio‐cerebrovascular adverse events between the groups. Logistic regression analysis was used to explore the relationship between LMR and prognosis. Logistic analysis: The potential variables with P < 0.1 in univariate analysis are further included in multivariable analysis. The log‐rank test was used to compare differences between the groups. Receiver operating characteristic (ROC) curves were employed to assess the prognostic value of different parameters. A two‐tailed P‐value of less than 0.05 was considered to be statistically significant.
Results
General Data
The patients were divided into two groups based on the median LMR: the low LMR group (<1.70, n = 50) and the high LMR group (≥1.70, n = 51). The results showed that the high LMR group had lower #WBC, #NEU and CREA levels than the low LMR group, whereas the high LMR group had higher #LYM, ALB and GLO than the low LMR group (P < 0.05). There were no statistically significant differences between the two groups in sex ratio, age, body mass index (BMI) and (P > 0.05) (see Table 1).
 |
Table 1 Comparison of General Data Before Surgery Between the Two Groups |
Comparison of the Incidence of Adverse Clinical Events Within 30 Days Postoperative Between the Groups
The results showed no lost follow‐up cases within 30 days postoperative in either group. The all‐cause mortality rate was higher in the low LMR group than in the high LMR group (12.0% vs 2.0%, P = 0.047). However, the MODS rate was higher in the high LMR group than in the low LMR group (7.8% vs 0%, P = 0.043). There were no statistically significant differences between the two groups in AAEs, re-intervention events and cardiovaseular and cerebrovascular adverse events (P > 0.05) (see Table 2). Univariate and Multivariable Logistic-regression analysis were carried out on the adverse clinical events within 30 days postoperative. It was found that LMR was still related to the results after adjusting for confounding factors (95% CI: 1.152–1.864; P<0.05) (see Supplementary Table 1). Compared with other indexes, preoperative LMR can predict adverse events within 30 days (P<0.05).
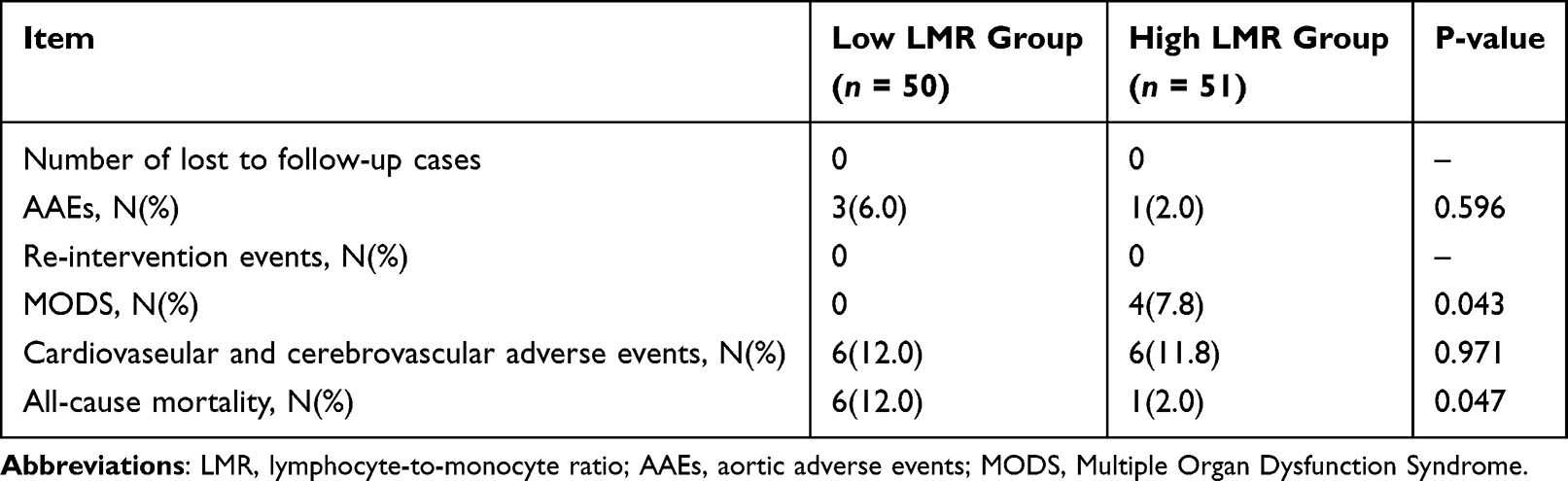 |
Table 2 Comparison of the Incidence of Adverse Clinical Events Within 30 Days Postoperative Between the Two Groups |
Comparison of the Incidence of Adverse Clinical Events Within 1 Year Postoperative Between the Groups
The results showed that during the 1‐year follow‐up, 3 patients in the high LMR group and 0 patients in the low LMR group were lost to follow‐up, with no statistically significant difference in the number of lost follow‐up patients between the groups (P = 0.248). During the follow‐up period, a total of 4 AAEs, 2 re-intervention events, 4 MODS, 11 cardiovaseular and cerebrovascular adverse events and 10 all‐cause deaths were reported. The high LMR group had lower incidences of all‐cause deaths (2.0% vs 18.0%, P = 0.018) and higher incidences of MODS (7.8% vs 0%, P = 0.018) than the low LMR group (see Table 3). Univariate and Multivariable Logistic-regression analysis were carried out on the adverse clinical events within 1 year postoperative. It was found that LMR was still related to the results after adjusting for confounding factors (95% CI: 1.010–1.135; P<0.05) (see Supplementary Table 2). Compared with other indexes, preoperative LMR can predict adverse events within 1 year (P<0.05).
 |
Table 3 Comparison of the Incidence of Adverse Clinical Events Within 1 Year Postoperative Between the Two Groups |
Comparison of the Survival Curves for Adverse Clinical Events Within 1 Year Postoperative Between the Groups
Figure 1A compares the 1‐year freedom from AAEs using survival curves between the groups. In the low LMR group, 94.0% of patients did not experience AAEs within 1 year, which was significantly lower than 98.0% in the high LMR group (HR=0.13, 95% CI: 0.025–0.67; log‐rank P = 0.0257). Figure 1B shows no significant difference between the low LMR group and the high LMR group in Re-intervention events within 1 year (HR=0.29, 95% CI: 0.027–3.00;log‐rank P = 0.2675). In Figure 1C, 92.2% of patients did not experience MODS within 1 year, which was lower than the high LMR group (HR=5.10, 95% CI: 0.49–52.74; log‐rank P = 0.1714). In Figure 1D, the rates of freedom from cardiovaseular and cerebrovascular adverse events within 1 year postoperative were 84.0% (95% CI: 92.8–99.2) in the low LMR group and 94.1% (HR=0.26, 95% CI: 0.78–0.87) in the high LMR group, indicating a statistically significant difference between the groups (log‐rank P = 0.0306). In Figure 1E, the overall 1‐year survival rates for the low LMR group and the high LMR group were 82.0% and 98.0% (HR=0.096, 95% CI: 0.026–0.358), respectively, indicating a statistically significant difference between the groups (log‐rank P =0.0054).
 |
Figure 1 (A): Survival curves comparing the incidence of freedom from AAEs within 1 year between groups (P < 0.001). (B) Survival curves comparing the incidence of freedom from re-intervention events within 1 year between groups (P < 0.001). (C) Survival curves comparing the incidence of freedom from MODS within 1 year between groups (P = 0.054). (D) Survival curves comparing the incidence of freedom from cardiovaseular and cerebrovascular adverse events within 1 year between groups (P = 0.439). (E) Survival curves comparing the all‐cause mortality within 1 year between groups (P < 0.001). Abbreviations: LMR, lymphocyte‐to‐monocyte ratio. |
Prognostic Value of the Lymphocyte-to-Monocyte Ratio for AAES and All‐cause Mortality Within 30 Days and 1 Year Postoperative
Using AAEs within 30 days and 1 year postoperative as the endpoint, an ROC curve was plotted with the LMR as the test variable. The sensitivity was 0.83 (95% CI: 0.44–0.99), and the specificity was 0.56 (95% CI: 0.46–0.65). The area under the ROC curve was 0.68 (95% CI: 0.52–0.83), with a concordance index of 0.65 (95% CI: 0.60–0.71) (see Figure 2A).
 |
Figure 2 (A): ROC curve of preoperative LMR predicting AAEs within 30 days postoperative in patients with ATAAD. (B) ROC curve of preoperative LMR predicting all‐cause mortality within 30 days postoperative in patients with ATAAD. (C)ROC curve of preoperative LMR predicting all‐cause mortality within 1 year postoperative in patients with ATAAD. Abbreviations: LMR, lymphocyte‐to‐monocyte ratio; ATAAD, acute type A aortic dissection. |
Using all-cause mortality within 30 days postoperative as the endpoint, a time-dependent ROC curve was established with the LMR as the test variable. The sensitivity was 0.89 (95% CI: 0.72–0.94), and the specificity was 0.54 (95% CI: 0.44–0.67). The area under the ROC curve was 0.74 (95% CI: 0.51–0.97), with a concordance index of 0.72 (95% CI: 0.68–0.76), as shown in Figure 2B.
Using all-cause mortality within 1 year postoperative as the endpoint, a time-dependent ROC curve was established with the LMR as the test variable. The sensitivity was 0.89 (95% CI: 0.57–0.99), and the specificity was 0.55 (95% CI: 0.45–0.64). The area under the ROC curve was 0.72 (95% CI: 0.53–0.91), with a concordance index of 0.70 (95% CI: 0.64–0.76), as shown in Figure 2C.
Discussion
Our study indicates that patients with a high LMR exhibit a significantly lower incidence of aorta-related mortality within 1 year postoperatively than those with a low LMR. This suggests that the LMR may serve as a valuable biomarker for predicting outcomes in patients with AD. The association between the LMR and reduced aorta-related mortality could be attributed to the immunomodulatory role of lymphocytes. Lymphocytes are known to produce cytokines that can modulate the inflammatory response and induce apoptosis in aortic smooth muscle cells, which is crucial in the pathogenesis of AD. A high LMR, indicating a relative abundance of lymphocytes, may reflect a more effective immune response, potentially leading to better outcomes. The key mechanism underlying the onset of AD is the medial degeneration of the aorta, characterised by the apoptosis of vascular smooth muscle cells and the degradation of the extracellular matrix. In recent years, both domestic and international researchers have demonstrated that the immune/inflammatory response plays a crucial role in the occurrence and progression of AD.22 In patients with AD, inflammatory markers such as C-reactive protein, brain natriuretic peptide and D-D are elevated and are associated with poor prognosis.22 Following the onset of AD, the body’s stress and inflammatory responses can increase levels of pro-inflammatory cytokines, further exacerbating the immune/inflammatory response.23 Additionally, the process of aortic remodelling following stent implantation can also trigger inflammation, which is potentially associated with poor prognosis and, in severe cases, can even lead to death.24 D‐dimer, reflecting the activity of the body’s coagulation/fibrinolysis system, is considered a molecular marker of this activity. When the body activates the coagulation/fibrinolysis systems and forms thrombi, D‐D levels increase. Acute AD results from the cystic medial degeneration of the aortic media, ultimately leading to a tear in the aortic intima, with blood entering the media layer of the arterial wall. The rupture of the aortic intima leads to the exposure of endothelial cells to blood clots and debris, and the damaged aorta releases tissue factors that activate the extrinsic coagulation pathway. The more extensive the involvement of the arterial vessels is, the more intense the response of the activated coagulation/fibrinolysis system becomes, and the higher the levels of D‐D are produced. Therefore, D‐D levels can reflect the occurrence and extent of acute AD,25 thereby indicating the patient’s prognosis.
Our findings are consistent with previous studies that have identified lymphocytopenia as a predictor of adverse outcomes in various cardiovascular conditions. The inverse relationship between the LMR and mortality suggests that monitoring the LMR could be a non-invasive method to assess the risk of poor outcomes in patients with AD. Neutrophils, platelets and lymphocytes play important roles in the inflammatory mechanisms of AD. Neutrophils are crucial modulators of the inflammatory response, inducing smooth muscle cell damage, platelet aggregation and the hypercoagulable state by secreting serine protease, cathepsin and reactive oxygen intermediate.26 Compared with normal aortic tissue, the aortic wall of patients with AD contains higher levels of neutrophils.27 Additionally, circulating neutrophil levels are also elevated in patients with AD. During dissection formation, platelet aggregation and activation mediate the activation of the coagulation system, which involves coagulation factor consumption and results in the hypercoagulable state. Furthermore, platelets can secrete inflammatory cytokines and growth factors into the vascular microenvironment, thereby activating neutrophils and promoting the migration of lymphocytes to peripheral lymph nodes.28 Postoperatively, platelets are involved in thrombus formation in the false lumen of the dissection and AD remodelling. Lymphocytes play a crucial role in producing cytokines and achieving cytotoxic lymphocyte‐induced cell death. Studies have shown that T lymphocytes can induce the apoptosis of aortic smooth muscle cells and the synthesis of matrix metalloproteinases.29 A reduction in circulating lymphocytes, not necessarily due to efflux into tissues, is a predictor of adverse outcomes in chronic ischemic diseases, heart failure and acute coronary syndrome.30
This study classified endpoints into AAEs, all-death mortality and others, and compared the incidence rates of these events between patient groups with high and low LMR levels. The results showed that the high LMR group had a significantly lower incidence of all-death mortality than the low LMR group. Furthermore, ROC curve analysis revealed that the LMR can be used to distinguish the risk of aorta-related mortality and all-death mortality within 1 year. However, for re-intervention events within 1 year, a larger sample size is needed for a more detailed analysis. What is different from xie31 and chen18 is that all the cases in this group are ascending aorta replacement+total aortic arch or semi-arch or sub-arch replacement, unlike the situation of dissection after stent placement in interventional surgery. It is also a kind of re-intervention event that the distal end of elephant trunk stent is not in good agreement with the diameter of descending aorta directly, which will cause internal leakage. This paper lacks foresight for such adverse events. Nevertheless, we made a detailed comparison of the predictive value of preoperative LMR for adverse outcomes, which was superior to other indicators such as NLR,PNR PNR.
It should be noted that this study has some limitations. First, it adopted a retrospective design and excluded patients with incomplete data, which could introduce selection bias. Additionally, the timing of blood sample collection from the patients was not standardised. Second, as a single-centre study, it has a relatively small sample size, warranting validation through multicentre, large-scale prospective studies. Third, while the current analysis has identified the LMR as a significant predictor of adverse outcomes, it is important to note that our study did not exhaustively examine all potential predictors that could be derived from the available data, nor did it address limitations inherent in the statistical approach. Future research could benefit from a more comprehensive analysis of these additional variables to further our understanding of the factors contributing to adverse outcomes. Finally, this study only observed the short‐term prognostic value of the LMR, and follow‐up research is needed to explore its value in long‐term prognosis.
Conclusion
In conclusion, the preoperative LMR is a significant and independent predictor of AAEs and mortality in patients with ATAAD within 30 days and 1 year postoperative. It is a highly prognostic indicator of mortality within one year after operation. Future research with larger sample sizes and multivariable analysis is necessary to confirm these results and explore their clinical implications fully.
Data Sharing Statement
All data generated or analyzed during this study are included in the article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Taizhou Hospital of Zhejiang Province affiliated to Wenzhou Medical University. Informed consent was signed by all participants in this study.
Funding
The authors have received no financial support for the research, authorship, or publication of this manuscript.
Disclosure
None of the authors have any personal, financial, commercial, or academic conflicts of interest in this work.
References
1. Jassar AS, Sundt TM. How should we manage type A aortic dissection? Gen Thorac Cardiovasc Surg. 2019;67(1):137–145. doi:10.1007/s11748-018-0957-3
2. McClure RS, Brogly SB, Lajkosz K, et al. Epidemiology and management of thoracic aortic dissections and thoracic aortic aneurysms in Ontario, Canada: a population-based study. J Thorac Cardiovasc Surg. 2018;155(6):2254–2264.e4. doi:10.1016/j.jtcvs.2017.11.105
3. Gawinecka J, Schönrath F, von Eckardstein A. Acute aortic dissection: pathogenesis, risk factors and diagnosis. Swiss Med Wkly. 2017;147:w14489. doi:10.4414/smw.2017.14489
4. Nienaber CA, Eagle KA. Aortic dissection: new frontiers in diagnosis and management: part II: therapeutic management and follow-up. Circulation. 2003;108(6):772–778. doi:10.1161/01.CIR.0000087400.48663.19
5. DeBakey ME, McCollum CH, Crawford ES, et al. Dissection and dissecting aneurysms of the aorta: twenty-year follow-up of five hundred twenty-seven patients treated surgically. Surgery. 1982;92(6):1118–1134. PMID: 7147190.
6. Gudbjartsson T, Ahlsson A, Geirsson A, et al. Acute type A aortic dissection - a review. Scand Cardiovasc J. 2020;54(1):1–13. doi:10.1080/14017431.2019.1660401
7. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897–903. doi:10.1001/jama.283.7.897
8. Landenhed M, Engström G, Gottsäter A, et al. Risk profiles for aortic dissection and ruptured or surgically treated aneurysms: a prospective cohort study. J Am Heart Assoc. 2015;4(1):e001513. doi:10.1161/JAHA.114.001513
9. Melvinsdottir IH, Lund SH, Agnarsson BA, et al. The incidence and mortality of acute thoracic aortic dissection: results from a whole nation study. Eur J Cardiothorac Surg. 2016;50(6):1111–1117. doi:10.1093/ejcts/ezw235
10. Uchida K, Karube N, Kasama K, et al. Early reperfusion strategy improves the outcomes of surgery for type A acute aortic dissection with malperfusion. J Thorac Cardiovasc Surg. 2018;156(2):483–489. doi:10.1016/j.jtcvs.2018.02.007
11. Conzelmann LO, Weigang E, Mehlhorn U, et al. Mortality in patients with acute aortic dissection type A: analysis of pre- and intraoperative risk factors from the German Registry for Acute Aortic Dissection Type A (GERAADA). Eur J Cardiothorac Surg. 2016;49(2):e44–52. doi:10.1093/ejcts/ezv356
12. Yin ZQ, Han H, Yan X, Zheng QJ. Research progress on the pathogenesis of aortic dissection. Curr Probl Cardiol. 2023;48(8):101249. doi:10.1016/j.cpcardiol.2022.101249
13. Czerny M, Siepe M, Beyersdorf F, et al. Prediction of mortality rate in acute type A dissection: the German registry for acute type a aortic dissection score. Eur J Cardiothorac Surg. 2020;58(4):700–706. doi:10.1093/ejcts/ezaa156
14. Li M, Xu S, Yan Y, et al. Association of biomarkers related to preoperative inflammatory and coagulation with postoperative in-hospital deaths in patients with type A acute aortic dissection. Sci Rep. 2021;11(1):18775. doi:10.1038/s41598-021-98298-w
15. Sun M, Zhao D, Zhang Y, et al. Prognostic utility of monocyte to high-density lipoprotein ratio in patients with acute coronary syndrome: a meta-analysis. Am J Med Sci. 2020;359(5):281–286. doi:10.1016/j.amjms.2020.01.018
16. Tanriverdi Z, Gungoren F, Tascanov MB, et al. Comparing the diagnostic value of the c-reactive protein to albumin ratio with other inflammatory markers in patients with stable angina pectoris. Angiology. 2020;71(4):360–365. doi:10.1177/0003319719897490
17. Li J, Zhang Y, Li N, et al. Value of novel inflammatory indicators for predicting early HF in acute myocardial infarction patients. Chin J Geriatric Heart Brain Vessel Diseases. 2022;24(03):243–246. doi:10.3969/j.issn.1009-0126.2022.03.006
18. Chen S, Wu Z, Yun Y, et al. Lymphocyte-to-monocyte ratio associated with severe post-stenotic aortic dilation in a case-control study. BMC Cardiovasc Disord. 2022;22(1):195. doi:10.1186/s12872-022-02636-3
19. Chen W, Song X, Hong L, et al. The association between lymphocyte-monocyte ratio and postoperative acute kidney injury in patients with acute type A aortic dissection. J Cardiothorac Surg. 2022;17(1):60. doi:10.1186/s13019-022-01813-x
20. Bedel C, Selvi F. Association of platelet to lymphocyte and neutrophil to lymphocyte ratios with in-hospital mortality in patients with type a acute aortic dissection. Braz J Cardiovasc Surg. 2019;34(6):694–698. doi:10.21470/1678-9741-2018-0343
21. Committee of Great Vessels of Chinese Association of Cardiovascular Surgeons. Chinese experts’ consensus of standardized diagnosis and treatment for acute aortic syndrome. J Thorac Cardiovasc Surg. 2017;33(11):641–654. doi:10.3760/cma.j.issn.1001-4497.2017.11.001
22. Luo F, Zhou XL, Li JJ, et al. Inflammatory response is associated with aortic dissection. Ageing Res Rev. 2009;8(1):31–35. doi:10.1016/j.arr.2008.08.001
23. He R, Guo DC, Estrera AL, et al. Characterization of the inflammatory and apoptotic cells in the aortas of patients with ascending thoracic aortic aneurysms and dissections. J Thorac Cardiovasc Surg. 2006;131(3):671–678. doi:10.1016/j.jtcvs.2005.09.018
24. Arnaoutoglou E, Kouvelos G, Papa N, et al. Prospective evaluation of post-implantation inflammatory response after EVAR for AAA: influence on patients’ 30 day outcome. Eur J Vasc Endovasc Surg. 2015;49(2):175–183. doi:10.1016/j.ejvs.2014.12.006
25. Xu CL, Cao SH. Diagnostic value of D‐dimer levels in acute aortic dissection. Chin J Anal Lab Diagnosis. 2009;13(3):366–368. doi:10.3969/j.issn.1007-4287.2009.03.029
26. Totani L, Evangelista V. Platelet-leukocyte interactions in cardiovascular disease and beyond. Arterioscler Thromb Vasc Biol. 2010;30(12):2357–2361. doi:10.1161/ATVBAHA.110.207480
27. Wu D, Choi JC, Sameri A, et al. Inflammatory cell infiltrates in acute and chronic thoracic aortic dissection. Aorta. 2013;1(6):259–267. doi:10.12945/j.aorta.2013.13-044
28. Duerschmied D, Suidan GL, Demers M, et al. Platelet serotonin promotes the recruitment of neutrophils to sites of acute inflammation in mice. Blood. 2013;121(6):1008–1015. doi:10.1182/blood-2012-06-437392
29. Li Y, Yang N, Duan W, et al. Acute aortic dissection in China. Am J Cardiol. 2012;110(7):1056–1061. doi:10.1016/j.amjcard.2012.05.044
30. Giede-Jeppe A, Bobinger T, Gerner ST, et al. Lymphocytopenia is an independent predictor of unfavorable functional outcome in spontaneous intracerebral hemorrhage. Stroke. 2016;47(5):1239–1246. doi:10.1161/STROKEAHA.116.013003
31. Xie XS, Zhao YF, Xu DD, et al. Preoperative high lymphocyte-to-monocyte ratio is associated with intraoperative type I endoleak in patients with TAA with TEVAR. Vascular. 2022;30(5):977–987. doi:10.1177/17085381211039939
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.