")
Back to Journals » Clinical Ophthalmology » Volume 19
Progress in the Management of Retinal Detachment Associated With Morning Glory Syndrome
Authors Wu S , Wang W, Liu L, Wang W, Jiang K , Peng C , Sun H, Zhang J
Received 9 November 2024
Accepted for publication 22 January 2025
Published 11 February 2025 Volume 2025:19 Pages 459—468
DOI https://doi.org/10.2147/OPTH.S505086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Suping Wu,1 Wenting Wang,2 Lei Liu,3 Wei Wang,2 Keke Jiang,2 Chuanzhi Peng,4 Huixin Sun,1 Jie Zhang2
1Department of Ophthalmology, Binzhou Medical College, Binzhou, Shandong, People’s Republic of China; 2Department of Ophthalmology, Weifang Eye Hospital, Weifang, Shandong, People’s Republic of China; 3Department of Ophthalmology, Guangdong Provincial People’s Hospital, Guangzhou, Guangdong, People’s Republic of China; 4Department of Ophthalmology, Shandong Second Medical University, Weifang, Shangdong, People’s Republic of China
Correspondence: Jie Zhang, Department of Ophthalmology, Weifang Eye Hospital, Weifang, Shandong, People’s Republic of China, Email [email protected]
Abstract: Morning glory syndrome (MGS) is a rare congenital optic disc malformation characterized by a distinctive funnel-shaped optic disc resembling a blooming morning glory flower, typically diagnosed in childhood or adolescence and primarily presenting unilaterally, although bilateral cases have been reported. The anomaly features an enlarged optic disc, radiating blood vessels, and surrounding excavation, leading to visual impairment that can range from mild to profound. The etiology of MGS is not fully understood but has been associated with genetic factors, particularly mutations in the PAX6 and PAX2 genes, which play critical roles in eye development. MGS is often linked with other ocular and systemic anomalies, including retinal detachment, a significant complication that may be exudative, tractional, or rhegmatogenous. Surgical interventions are generally employed to manage complications, especially retinal detachments, with procedures such as vitrectomy, paraoptic disc laser photocoagulation, and the use of silicone oil or gas tamponade, though success rates can vary widely. Long-term outcomes for patients with MGS largely depend on the severity of associated complications and the timing of interventions; while some individuals may attain reasonable visual function post-treatment, others may continue to experience challenges due to the underlying malformation and its consequences. Thus, MGS remains a complex condition requiring a multidisciplinary approach for effective management and enhanced patient outcomes, emphasizing the need for continued research into its genetic underpinnings and optimal treatment strategies to improve understanding and care for those affected.
Keywords: morning glory syndrome, retinal detachment, vitrectomy, paraoptic disc laser photocoagulation
Introduction
Morning glory syndrome (MGS), is a rare congenital malformation of the ocular fundus characterized by an abnormal optic disc development that resembles a blooming morning glory flower.1 The incidence of MGS is approximately 3.6 per 100,000 individuals, with a higher prevalence observed in females compared to males, being about twice as common in females.2,3 MGS typically presents with juvenile onset, predominantly affecting one eye, although it can occur bilaterally.4 The characteristic fundus appearance includes an enlarged, pink, funnel-shaped optic disc that is displaced posteriorly, often accompanied by a cluster of white or gray retinal pigmentary disturbances around the peripapillary region.3 Additionally, the disc exhibits a concentric ring of retinal-choroidal atrophy, which is frequently pigmented, while the peripheral area shows retinal choroidal atrophy.5 The vascular pattern may be atypical, with an increased number of blood vessels radiating outward from the disc, diverging from the usual central branching pattern, and there is often less vascularization overall, with the vascular trunks obscured by white glial tissue, making arteriovenous differentiation challenging.6 Occasionally, a white sheath may be present. Depending on the extent of the peripapillary choroidal involvement, when the macula is encompassed within the excavation, the term “macular capture” is used.7 The native position of the macula can be inferred from the dense pigmentation surrounding the abnormal optic disc.1,8 Patients with MGS typically experience low vision, often ranging from counting fingers to 20/100.1 Current understanding suggests that morning glory syndrome is associated with mutations in the PAX6 or PAX2 genes,9 with inheritance patterns that can be autosomal dominant or recessive, though the specific genetic mechanisms remain unclear. The primary complication of morning glory syndrome is retinal detachment,10 which can occur in up to 30% of cases.7 This type of detachment usually occurs around the deeply excavated optic disc and is often confined to the posterior pole of the retina.11 Furthermore, MGS is commonly associated with other ophthalmic conditions such as refractive errors, strabismus, nystagmus, microcornea, pupillary membrane closure, cataracts, persistent fetal vasculature, retinal folds, retinal pigment degeneration, choroidal coloboma, scleral staphyloma, optic nerve atrophy, choroidal neovascularization, eyelid hemangiomas, and preretinal glioma.2,3,7,12–16 Additionally, systemic complications can include Aicardi syndrome,17 renal coloboma syndrome,18 basal encephalocele,19 and moyamoya disease.7
MGS combined with retinal detachment can be managed through various surgical approaches. This article reviews specific case studies involving surgical methods such as vitrectomy combined with paraoptic disc laser photocoagulation, vitrectomy alone, simple paraoptic disc laser photocoagulation, and paraoptic disc laser photocoagulation aimed at preventing retinal detachment. The advantages and disadvantages of each surgical method are discussed, with a focus on whether they are performed in conjunction with retinal tears (Table 1). For cases involving multiple surgical interventions, classification is based on the final surgical procedure or the innovative aspects of the surgical approach.
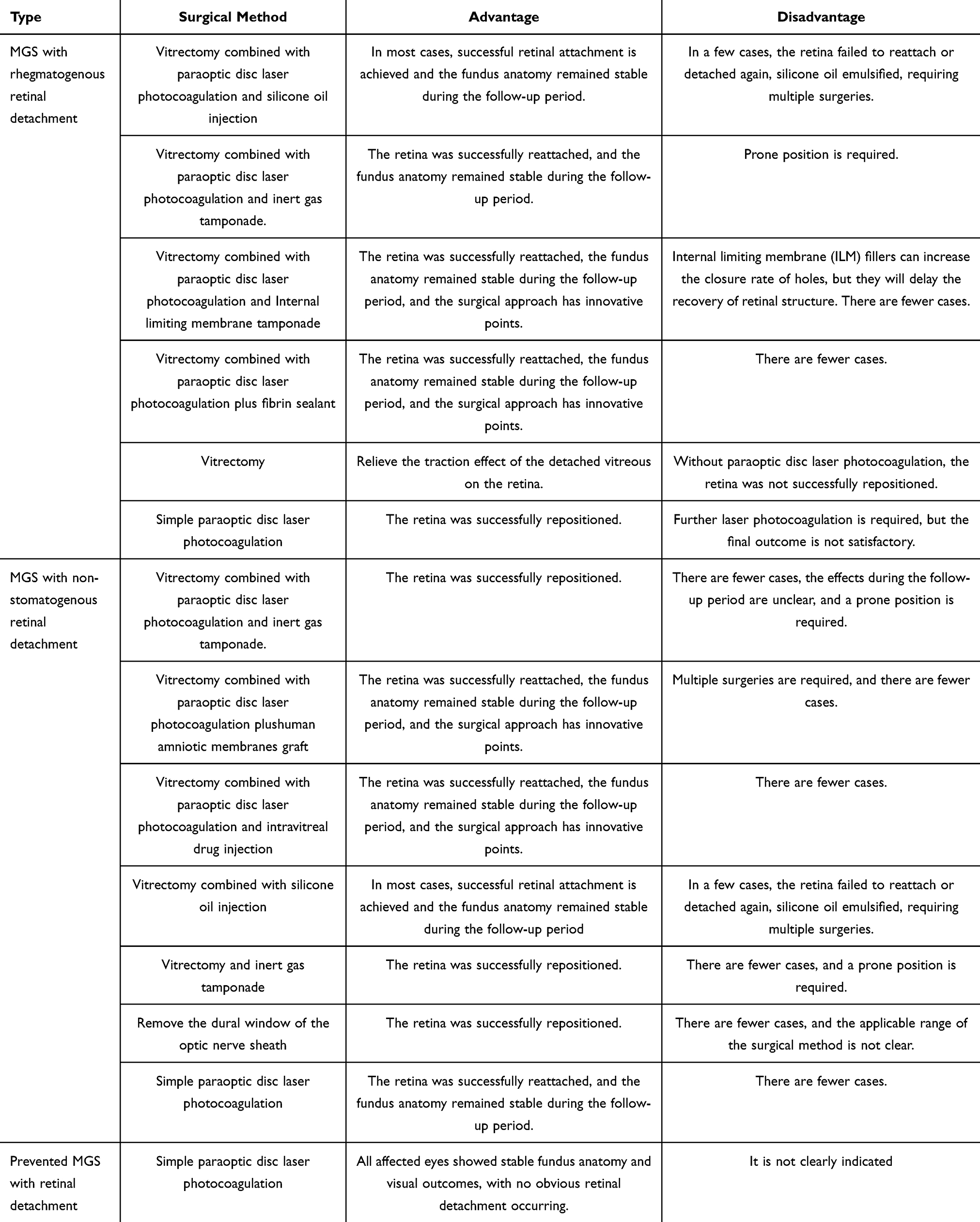 |
Table 1 Advantages and Disadvantages of Different Surgical Methods for Treating MGS with Retinal Detachment |
Morning Glory Syndrome Combined with a Retinal Detachment Mechanism
Morning Glory Syndrome Complicated with Exudative Retinal Detachment
MGS is most commonly associated with exudative retinal detachment.20 Chang et al demonstrated that contrast agents injected into the mimidamide pool could enter the subretinal space from the subarachnoid space via the optic nerve sheath.21 This finding suggests the existence of an abnormal pathway between the subarachnoid and subretinal spaces, which allows cerebrospinal fluid to accumulate in the subretinal space. Additionally, liquefied vitreous may enter the subretinal space through the optic disc depression.10,20,22,23 Furthermore, abnormal blood vessels at the optic disc or fluid exudation from the surrounding choroid can lead to subretinal fluid accumulation.24 Traction exerted by the vitreous on the retinal area may also cause fluid to leak from the vitreous cavity into the subretinal space.10 These mechanisms highlight the complex interactions between vitreous dynamics, cerebrospinal fluid, and retinal structures in MGS, underscoring the need for further investigation into their implications for visual outcomes and treatment strategies.
Morning Glory Syndrome Complicated with Stretch Retinal Detachment
The continuous pulling force generated by the gradual depression and expansion of the optic disc,6,22 along with vitreous traction25 and periretinal nonperfusion,26 can lead to tractional retinal detachment. According to Abel et al, significant movement of the optic disc contraction was observed when fibrous glial tissue was removed, which was interpreted as a muscle contraction mechanism. This contraction of the optic disc may result in the formation of retinal folds and subsequently lead to tractional retinal detachment.25 These mechanisms collectively contribute to the development of tractional retinal detachment in patients with morning glory syndrome.
Morning Glory Syndrome Complicated with Rhegmatogenous Retinal Detachment
Jo et al suggests that congenital defects in the affected eye, excessive growth and widening of the optic disc depression, and the traction of the vitreous and optic disc may contribute to the formation of retinal breaks.27 Additionally, S. Chang er al. posits that this traction can lead to secondary retinal ruptures.28 In the context of MGS, retinal breaks located in the abnormal tissue of the optic disc serve as channels for fluid to flow between the vitreous and subretinal spaces.10,29 Therefore, these retinal breaks are critical in facilitating the accumulation of fluid that can exacerbate the condition.
Treatment of Morning Glory Syndrome Combined with Rhegmatogenous Retinal Detachment
Vitrectomy Combined with Paraoptic Disc Laser Photocoagulation
Vitrectomy Combined with Paraoptic Disc Laser Photocoagulation and Silicone Oil Injection
Zhang et al performed standard three-port vitrectomy surgery (3 cases of 20G, 5 cases of 23G) on 8 patients with synergetic traction macular hole retinal detachment associated with proliferative changes and papillitis syndrome. Among these, 2 cases had combined funneled retinal detachment. During the surgery, the glial tissue around the optic disc was removed, and several tiny holes around the optic disc were found. Paraoptic disc laser photocoagulation was performed to seal the holes, followed by silicone oil tamponade. After 8 months to 4 years of follow-up, the final best corrected visual acuity (BCVA) ranged from 6/600 to 6/30, with no recurrence of retinal detachment and no silicone oil entering the subretinal space.30 Additionally, Jo et al reported a successful case of a large retinal hole extending from the temporal region to the optic disc, leading to subretinal fluid accumulation and superficial retinal detachment, sparing the macula. After two years of follow-up, a subretinal incision was made, followed by 20% SF6 gas injection and optic disc laser photocoagulation. The retina reattached after the gas dissipated, but it re-detached one-month post-surgery, necessitating a silicone oil-fluid exchange and additional laser treatment. By the five-year follow-up, the hole had closed, and the retina remained attached without subretinal fluid.27 Sato et al also described a case involving a child with intellectual disabilities who underwent vitrectomy. Post-operative vitreous detachment allowed for subretinal fluid discharge, and laser photoretinal fixation was performed with 10% C3F8 gas. Unfortunately, complete retinal detachment occurred three weeks later, leading to hyperplastic vitreoretinopathy. Subsequent surgeries included lensectomy, intraocular lens implantation, and laser photocoagulation, but retinal attachment ultimately failed after four operations, likely due to the child’s mental retardation and excessive head movement during crying.31 Ma et al reported four successful treatments of macular hole proliferative retinal detachment associated with morning glory syndrome using vitrectomy, peripapillary photocoagulation, and silicone oil tamponade, with follow-up periods ranging from 8 months to 4 years, during which the retinas were flattened without complications.32
Vitrectomy Combined with Paraoptic Disc Laser Photocoagulation and Inert Gas Tamponade
Chang et al observed six affected eyes with MGS and found that subretinal fluid could dissolve within approximately 12 months, with two cases resolving retinal detachment spontaneously. In three eyes with MGS and peripapillary retinal breaks, vitrectomy involved creating posterior vitreous detachment, trimming fibroglial tissue around the optic disc, filling with perfluoroethane gas, and performing laser photocoagulation, resulting in anatomical stability during follow-ups of 7 months, 9 months, and 10 years.28 Ho et al successfully treated a case of MGS with rhegmatogenous retinal detachment by separating glial tissue and closing a temporal hiatus with 15% perfluoropropane and laser photocoagulation, maintaining retinal attachment over a 2-year follow-up.33 Yang et al achieved reduction of MGS-related rheogenic retinal detachment via vitrectomy, laser fixation, and 20% perfluoropropane tamponade, with retina restoration after 4 months.24 Xie et al performed vitrectomy and cataract extraction, drained subretinal fluid, and applied 360-degree laser photocoagulation along the optic disc, successfully restoring the retina at the 1-year follow-up.34
Vitrectomy Combined with Paraoptic Disc Laser Photocoagulation and Internal Limiting Membrane Tamponade
Previously, Shen et al reported a case of internal limiting membrane (ILM) flap filling for MGS complicated with rhegmatogenous retinal detachment. The best corrected visual acuity (BCVA) of the eye was 0.12, and the retinal hole was located at the lateral temporal margin of the optic disc. After eye check, The patient underwent a 25G vitrectomy, nasal retinal incision to drain subretinal fluid, and laser coagulation of the incision, and injection of silicone oil. The retina was successfully attached but the retinal hole was not closed, and the retina contracted in the direction of the blood vessel. After half a year of follow-up, the retina was still remained flat, and the best corrected visual acuity was 0.15. A 23G vitrectomy was performed again one and a half years after surgery. Silicone oil was removed intraoperatively, glial tissue around the optic disc was cut off, and part of ILM was removed along the temporal margin of the optic disc. The histoma was closed with ILM flap and residual glial tissue, the ILM flap was fixed with 0.1mL autoserum, and C3F8 gas was injected. The BCVA of the eye in the early postoperative period was 0.12, the intraocular pressure was normal, the retina was attached, the temporal histoma of the optic disc was closed, and no obvious contractile movement was observed. This case may indicate that the inner boundary membrane inverted flap filling can increase the closure rate of the hole, but delay the recovery of the retinal structure.35
Vitrectomy Combined with Paraoptic Disc Laser Photocoagulation Plus Fibrin Sealant
Fibrin sealants are formed by mixed fibrinogen and thrombin. Saab et al performed a 100% C3F8 gas filling procedure on an 8-year-old boy with MGS combined with bullous retinal detachment. The boy was placed in the prone position after surgery. On the first day post-operation, the retina was completely detached, and gas was accumulated under the retina. After that, the second 25G vitrectomy was performed. During the operation, small retinal holes in the optic disc were found. After air and liquid exchange, subretinal fluid was drained through the holes, 360 paraoptic disc laser photocoagulation, enough fibrin sealant was injected to cover the entire enlarged optic disc of the depression, retinal holes were closed and filled with 20%C3F8. The patient was supine for 1 day and prone position for 6 days. The retinas remained attached at 6 months of follow-up,36 This case demonstrates the successful use of fibrin sealants combined with vitrectomy to effectively manage retinal detachment associated with morning glory syndrome. The patient maintained retinal attachment at the 6-month follow-up, highlighting the potential of innovative surgical techniques in improving outcomes for complex retinal conditions.
Vitrectomy
Masuo Sakamoto reported two cases of MGS associated with complete retinal detachment, characterized by optic disc contraction movements synchronized with respiratory or cardiac beats and unaffected by intraoperative intraocular pressure or photostimulation. In the first case, an 8-year-old boy with MGS in the left eye, which had a small eyeball, underwent vitreous cutting. During the procedure, optic disc contraction was observed, and after creating a vitreous detachment, perfluorooctane (PFO) was injected into the isolated retina. However, the PFO migrated through the contraction hole into the inferior retinal cavity, Then expelled through the sclera, there was no optic disc laser photocoagulation performed. The patient was subsequently filled with 10% perfluoropropane gas, but two months later, retinal detachment recurred without further treatment. The second case involved a 3-year-old girl with MGS who presented with nasal retinal detachment while the macula remained attached. Despite conservative treatment for 21 months, ultrasound suggested total retinal detachment, leading to vitrectomy and lentomy. Intraoperatively, severe hyperplastic vitreoretinopathy with funnel closure was found, and despite stripping the proliferative membrane, retinal detachment persisted at the 15-month follow-up. In summary, these cases illustrate the complexities of managing retinal detachment in patients with MGS, highlighting the challenges posed by optic disc contraction and the potential for recurrent detachment despite surgical intervention.37
Simple Paraoptic Disc Laser Photocoagulation
Zhang et al reported an intriguing case that highlights the challenges of managing retinal complications associated with congenital anomalies. The patient presented with a choroidal defect accompanied by retinal detachment, where an oval hole was observed at the lateral edge of the optic disc, along with cystoid macular edema. To address this condition, paraoptic disc laser photocoagulation was initially performed to seal the hole, leading to the disappearance of the patient’s occlusion. However, despite this intervention, the macula remained edematous. A second round of laser photocoagulation was conducted to further target the macular edema, but the results were unsatisfactory, leaving the edema unresolved. This case underscores the complexities and challenges associated with treating retinal conditions linked to structural defects, such as choroidal abnormalities. It highlights the need for continued investigation and potentially more innovative therapeutic strategies to effectively manage persistent complications like cystoid macular edema in such patients.38
Treatment of Morning Glory Syndrome with Non-Stomatogenous Retinal Detachment
Vitrectomy Combined with Paraoptic Disc Laser Photocoagulation
Vitrectomy Combined with Paraoptic Disc Laser Photocoagulation and Inert Gas Tamponade
Previously, Campos et al presented a noteworthy case of MGS characterized by serous macular detachment. After performing vitreous cutting, the surgical team filled the eye with C2F6 gas to facilitate retinal reattachment. Additionally, laser treatment was applied around the optic disc to reduce the risk of further complications. The intervention was successful, leading to a favorable outcome in the patient’s vision and retinal stability. This case highlights the importance of a multidisciplinary approach in managing complex retinal conditions associated with MGS. It emphasizes the potential for successful outcomes with timely surgical intervention and appropriate treatment strategies, providing valuable insights for clinicians dealing with similar cases in the future.39
Vitrectomy Combined with Paraoptic Disc Laser Photocoagulation Plushuman Amniotic Membranes Graft
Recently, Tomaso et al reported a case of MGS complicated by retinal detachment in the macular area, which was managed using a human amniotic membrane patch and silicone oil filling at the optic nerve defect. The patient underwent three surgeries, starting with a 25G vitrectomy where the dimpled optic disc was covered with a 3.0 mm human amniotic membrane and filled with 20% SF6 gas to maintain a prone position. However, retinal detachment recurred two weeks later, leading to a second vitrectomy with a 4.0 mm amniotic membrane and silicone oil injection. After the second surgery, the retina remained attached, but a new detachment occurred two weeks post silicone oil removal. The third operation involved another vitrectomy, a 6.0 mm amniotic membrane patch, silicone oil injection, and laser photocoagulation, resulting in successful retinal reconstruction three months later, with best corrected visual acuity remaining at 0.2 and no signs of amniotic membrane rejection. This case underscores the complexity of managing retinal detachment in morning glory syndrome and highlights the potential effectiveness of combined surgical techniques in achieving anatomical success.40
Vitrectomy Combined with Paraoptic Disc Laser Photocoagulation and Intravitreal Drug Injection
Potential for surgical intervention could manage complications associated with MGS in infants, leading to favorable anatomical outcomes. Ran et al reported a case of binocular MGS in an infant with primary embryonic blood vessels in the right eye, presenting significant challenges in early management. The patient was seen at just 3 days of age and underwent surgery at 8 months. Before the operation, the primary embryonic blood vessels in the right eye gradually regressed, resulting in massive exudation of the posterior polar retina, particularly around the optic disc, along with retinal folds in both eyes and macular displacement in the left eye. Elevated levels of VEGF-B were detected in both eyes. The surgical intervention involved binocular vitrectomy combined with paraoptic disc laser photocoagulation. During the procedure, an ethmoid defect around the optic disc in the right eye was identified and successfully closed using laser treatment. Additionally, anti-VEGF drugs were injected into the vitreous cavity of both eyes. The patient was followed up for 4 months, during which the anatomical stability of the fundus was maintained.41
Vitrectomy
Vitrectomy Combined with Silicone Oil Injection
Jiang et al reported a case of morning glory syndrome complicated by persistent primitive embryonic blood vessels, vitreous hemorrhage, temporal retinal crease, and retinal detachment. The patient underwent vitrectomy, during which glial tissue around the optic disc was removed. Complete gas-liquid exchange was performed, followed by silicone oil tamponade. After 2 years of follow-up, a small amount of subretinal fluid accumulated near the optic disc, but no significant retinal detachment was observed, and only a slight emulsification of silicone oil occurred in the anterior chamber.12 In a separate case, Tyler et al described a 19-year-old patient with morning glory syndrome and traction retinal detachment associated with a PAX6 mutation in the right eye, with the macula involved. The patient underwent successful repair through 25G vitrectomy, which included anterior retinal membrane dissection, retinotomy to release subretinal fluid, laser photocoagulation, and silicone oil injection. After 1 year of follow-up, the eye maintained anatomical stability, and the best-corrected visual acuity was count fingers. However, 18 months post-surgery, silicone oil emulsification occurred, with a small amount entering the anterior chamber, leading to worsening of a posterior subcapsular cataract. Two years after the initial surgery, the patient underwent additional procedures for vitrectomy, silicone oil removal, cataract extraction, and intraocular lens implantation, yet the best-corrected visual acuity remained CF. These cases highlight the complexities and potential complications of managing morning glory syndrome, necessitating careful long-term follow-up and intervention.20
Vitrectomy and Inert Gas Tamponade
Lyubomyr M. Lytvynchuk performed vitrectomy on a one-eyed patient with MGS complicated with non-rheogenated retinal detachment, during which the subretinal fluid was aspirated, the anterior retinal membrane and the inner boundary membrane were excised, and air was injected for tampon. After surgery, the patient was in prone position, followed up for 12 months, and the retina recovered.16
Remove the Dural Window of the Optic Nerve Sheath
Chang et al performed surgery on a patient with morning glory syndrome complicated by complete retinal detachment, presenting with headaches and sudden vision loss. The patient had a bullotic retinal detachment in the left eye with a folded retina and a distant visual acuity of 5/200. Following a lumbar puncture and injection of a metronidazole contrast agent, diffusion was observed around the optic nerve, indicating an abnormal channel between the subarachnoid and subretinal spaces. Chang conducted a medial approach to incise the optic nerve sheath, removing the dural window, which allowed clear fluid to escape. Postoperatively, the retina was flat on the first day, but shallow detachment persisted. Seven weeks later, viscous yellow subretinal fluid was drained, resulting in complete retinal flattening and improved visual acuity to 20/200. After 15 months of follow-up, the retina remained fully attached, with no retinal holes found, attributed to continuous vitreous traction. This case demonstrates the effectiveness of surgical intervention in managing retinal detachment complications associated with morning glory syndrome.21
Simple Paraoptic Disc Laser Photocoagulation
Zhang Zhiyong treated a 4-year-old child with morning glory syndrome complicated by retinal detachment using laser photocoagulation. Over a follow-up period of 1 to 9 months post-surgery, the extent of retinal detachment progressively decreased, beginning with reconstruction from the temporal side of the optic disc and extending towards the macular region.42 The use of circular laser treatment facilitated the successful reconstruction of the retina, leading to positive outcomes. This case highlights the effectiveness of laser photocoagulation in managing retinal detachment in children with morning glory syndrome.
Simple Paraoptic Disc Laser Photocoagulation Prevented Retinal Detachment
Zou et al performed simple paratopic laser photocoagulation in 24 eyes with morning glory syndrome without significant retinal detachment to prevent retinal detachment. The method is to establish three to five rows of fused off-white laser spots around the edge of the optic disc by laser light at 520 nm wavelength, 180 to 250 mW power and 300ms duration on the retina around the optic disc at 360°. During the average follow-up of 27.7±17.5 months, the fundus anatomy and visual effects of all affected eyes were stable, and no obvious retinal detachment occurred, which indicates that paratopic laser photocoagulation has a certain effect on preventing retinal detachment.43
Prospective
Given the complex nature of MGS and its associated retinal detachment complications, future research should focus on several critical areas. Firstly, a deeper understanding of the genetic mutations, particularly involving the PAX6 and PAX2 genes, is essential for unraveling the specific mechanisms that lead to MGS. Genetic screening and counseling could provide valuable insights for affected families and aid in early diagnosis.
Secondly, prospective studies investigating the long-term visual outcomes of various surgical interventions, such as vitrectomy combined with laser photocoagulation and silicone oil tamponade, are needed. This includes evaluating the efficacy of newer techniques, such as the use of human amniotic membrane grafts and fibrin sealants in surgical repair, to determine the best practices for managing MGS and its complications.
Moreover, examining the association of MGS with systemic conditions, such as Aicardi syndrome and renal coloboma syndrome, could reveal important insights into the broader implications of this condition and inform multidisciplinary approaches to patient care. Finally, the development of standardized classification systems for retinal detachments associated with MGS will aid in comparing outcomes across studies and enhance collaborative research efforts.
Conclusion
In sum, MGS is a rare congenital malformation characterized by distinct ocular fundus features and significant complications, including various forms of retinal detachment. The complexity of MGS necessitates a multifaceted approach to treatment, involving advanced surgical techniques and thorough postoperative management to address complications effectively. For the treatment of MGS combined with rhegmatogenous retinal detachment, most scholars use vitrectomy combined with paraoptic disc laser photocoagulation. Most cases can achieve reattachment of the retina, and the fundus anatomy can remain stable during the follow-up period, but there are still some adverse outcomes, such as retinal redetachment, silicone oil emulsification, elevated intraocular pressure, etc. For the treatment of MGS combined with non-rhegmatogenous retinal detachment, scholars mostly use vitrectomy combined with paraoptic disc laser photocoagulation or vitrectomy. Both surgical methods can achieve reattachment of the retina, and the fundus anatomy is stable during the follow-up period, but also have adverse consequences such as retinal redetachment, silicone oil emulsification, etc. To prevent MGS combined with retinal detachment, simple paraoptic disc laser photocoagulation can be adopted. While the prognosis for vision remains variable, ongoing research into genetic factors and innovative treatment modalities holds promise for improving outcomes for individuals affected by MGS. Enhanced awareness and understanding among healthcare professionals will be pivotal in ensuring timely diagnosis and intervention, ultimately aiming to optimize the quality of life for patients with this condition.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no proprietary interest in any aspect of the report.
References
1. Kindler P. Morning glory syndrome: unusual congenital optic disk anomaly. Am J Ophthalmol. 1970;69:376. doi:10.1016/0002-9394(70)92269-5
2. Abdoulaye N, Kole SM. [Glory morning syndrome]. Pan Afr Med J. 2017;26:176. Norwegian. doi:10.11604/pamj.2017.26.176.11445
3. Yusuf IH, Burke TR, Bates R. Cryptic uveitis in a patient with morning glory syndrome. Ocul Immunol Inflamm. 2014;22:394. doi:10.3109/09273948.2013.845230
4. Muslubas IS, Hocaoglu M, Arf S, Karacorlu M. A case of morning glory syndrome associated with persistent hyperplastic primary vitreous and Peters’ anomaly. GMS Ophthalmol Cases. 2017;7:Doc2.
5. Pei Y, Fang B, Chen Q. Morning glory syndrome. Foreign Med Ophthalmol. 1986;21.
6. De Laey JJ, Ryckaert S, Leys A. The ‘morning glory’ syndrome. Ophthalmic Paediatr Genet. 1985;5:117. doi:10.3109/13816818509007865
7. Panyala R, Mahesh M, Singh A, Samanta R. An unusual association of morning glory syndrome with chronic myeloid leukemia-Philadelphia chromosome. J Fam Med Prim Care. 2020;9:4456. doi:10.4103/jfmpc.jfmpc_892_20
8. Mi Y, Chengren L. Morning glory syndrome (Report of 5 cases). Ophthalmology. 1985;50.
9. Gines-Gallego C, Rego-Lorca D, Sanchez-Quiros J, Santos-Bueso E. Morning glory syndrome and ultrasound study. J FR Ophtalmol. 2021;44:611. doi:10.1016/j.jfo.2020.05.015
10. Bartz-Schmidt KU, Heimann K, Esser P. Vitrectomy for macular detachment associated with optic nerve pits. Int Ophthalmol. 1995;19:323. doi:10.1007/BF00130850
11. Guo HY, Xu YN, Xie L. A case report of binocular morning glory syndrome. Jilin Med Coll. 2007;28:340.
12. Jiang H, Liang Y, Long K, Luo J. Postoperative follow-up of a case of atypical morning glory syndrome associated with persistent fetal vasculature. BMC Ophthalmol. 2019;19:150. doi:10.1186/s12886-019-1154-6
13. Bozic M, Hentova-Sencanic P, Markovic V, Marjanovic I. Morning glory syndrome associated with primary open angle glaucoma--case report. Srp Ark Celok Lek. 2014;142:223.
14. Cao XG, Li XX, Bao YZ. Morning glory syndrome associated with posterior lenticonus. Open Neurol J. 2009;3:45. doi:10.2174/1874205X00903010045
15. Lit ES, D’Amico DJ. Retinal manifestations of morning glory disc syndrome. Int Ophthalmol Clin. 2001;41:131. doi:10.1097/00004397-200101000-00012
16. Lytvynchuk LM, Glittenberg CG, Ansari-Shahrezaei S, Binder S. Intraoperative optical coherence tomography assisted analysis of pars Plana vitrectomy for retinal detachment in morning glory syndrome: a case report. BMC Ophthalmol. 2017;17:134. doi:10.1186/s12886-017-0533-0
17. Al-Moujahed A, Callaway NF, Ludwig CA, et al. Morning glory optic nerve in Aicardi syndrome: report of a case with fluorescein angiography. Eur J Ophthalmol. 2021;31:NP61. doi:10.1177/1120672120942702
18. Schimmenti LA. Renal coloboma syndrome. Eur J Hum Genet. 2011;19:1207. doi:10.1038/ejhg.2011.102
19. Ru T, Song M, Haibo Y, Weitian Z. Morning glory syndrome associated with congenital nasal anomalies. Int J Pediatr Otorhi. 2020;132:109972. doi:10.1016/j.ijporl.2020.109972
20. Etheridge T, Oakey Z, Altaweel MM. Management of retinal detachment associated with morning glory disc syndrome. Case Rep Ophthal. 2021;12:457. doi:10.1159/000516205
21. Chang S, Haik BG, Ellsworth RM, Louis LS, Berrocal JA. Treatment of total retinal detachment in morning glory syndrome. Am J Ophthalmol. 1984;97:596. doi:10.1016/0002-9394(84)90379-9
22. Chan RT, Chan HH, Collin HB. Morning glory syndrome. Clin Exp Optom. 2002;85:383. doi:10.1111/j.1444-0938.2002.tb02390.x
23. Naseripour M, Ghasempour A, Falavarjani KG, Sanjari MS, Yousefi M. Perfluorocarbon liquid migration into the subarachnoid space in a patient with morning glory syndrome. J Curr Ophthalmol. 2015;27:60. doi:10.1016/j.joco.2015.09.004
24. Yang XL, Zhang X. Vitrectomy of rhegmatogenous retinal detachment in morning glory syndrome. Int J Ophthalmol. 2010;3:89. doi:10.3980/j.issn.2222-3959.2010.01.21
25. Ramirez-Estudillo A, Torres-Navarro K, Rojas-Juárez S, et al. Case report: fibroglial retinal tissue in contractile morning glory disc anomaly. Case Rep Ophthal. 2021;12:525. doi:10.1159/000510958
26. She K, Zhang Q, Fei P, et al. Peripheral retinal nonperfusion in pediatric patients with morning glory syndrome. Osli Retina. 2018;49:674. doi:10.3928/23258160-20180831-04
27. Jo YJ, Iwase T, Oveson BC, Tanaka N. Retinal detachment in morning glory syndrome with large hole in the excavated disc. Eur J Ophthalmol. 2011;21:841. doi:10.5301/EJO.2011.8365
28. Chang S, Gregory-Roberts E, Chen R. Retinal detachment associated with optic disc colobomas and morning glory syndrome. Eye. 2012;26:494. doi:10.1038/eye.2011.354
29. Bartz-Schmidt KU, Heimann K. Pathogenesis of retinal detachment associated with morning glory disc. Int Ophthalmol. 1995;19:35. doi:10.1007/BF00156417
30. Zhang Y, Ou H, Zhu T. Surgical treatment for the proliferative retinal detachment associated with macular hole in the morning glory syndrome. Eye Sci. 2013;28:7.
31. Sato T, Kuniyoshi K, Kodama T, Kusaka S. Recurrent proliferative vitreoretinopathy in a patient with morning glory syndrome and intellectual disability. Am J Ophthalmol Case Rep. 2022;26:101416. doi:10.1016/j.ajoc.2022.101416
32. Ma J, Jiang J, Weng Y, Xie X. In:
33. Ho CL, Wei LC. Rhegmatogenous retinal detachment in morning glory syndrome pathogenesis and treatment. Int Ophthalmol. 2001;24:21. doi:10.1023/A:1014498717741
34. Xie JY, Feng X, Zhao S. a case of morning glory syndrome with retinal detachment. J Pract Clin Med. 2009;5:79.
35. Shen J, Chen X, Gong X, Wu Z. Internal limiting membrane packing for treatment of morning glory syndrome with rhegmatogenous retinal detachment. Am J Ophthalmol Case Rep. 2022;26:101454. doi:10.1016/j.ajoc.2022.101454
36. Saab MG, Cordahi GP, Rezende FA. Fibrin sealant in the treatment of retinal detachment in morning glory syndrome. Retin Cases Brief Rep. 2011;5:326. doi:10.1097/ICB.0b013e3181ff0937
37. Sakamoto M, Kuniyoshi K, Hayashi S, Yamashita H, Kusaka S. Total retinal detachment and contractile movement of the disc in eyes with morning glory syndrome. Am J Ophthalmol Case Rep. 2020;20:100964. doi:10.1016/j.ajoc.2020.100964
38. Zhang K-W, Ya Z, Greena. A case of choroidal defect complicated with retinal detachment in morning glory syndrome. Chin J Pract Ophthalmol. 2004;838.
39. Cañete Campos C, Gili Manzanaro P, Yangüela Rodilla J, Martín Rodrigo JC. Desprendimiento de retina asociado a síndrome de morning glory [Retinal detachment associated with morning glory syndrome]. Arch Soc Esp Oftalmol. 2011;86(9):295–299. doi:10.1016/j.oftal.2011.04.009
40. Caporossi T, Ferrara S, Savastano A, et al. Management of retinal detachment associated with morning glory syndrome using the human amniotic membrane. Retin Cases Brief Rep. 2024;18:18. doi:10.1097/ICB.0000000000001303
41. Ran H, Ren J, Li S, et al. Progression of bilateral morning glory syndrome associated with unilateral persistent fetal vasculture: a case report of long term follow-up in an infant. Eur J Ophthalmol. 2023;33:NP82. doi:10.1177/11206721231156493
42. Zhang Z.
43. Zou YH, She KQ, Ren JN, et al. Prophylactic juxtapapillary laser photocoagulation in pediatric morning glory syndrome. Int J Ophthalmol. 2022;15:766. doi:10.18240/ijo.2022.05.12
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.