")
Back to Journals » Clinical Ophthalmology » Volume 19
Proposing a New Classification for Managing Prostaglandin-Induced Enophthalmos in Glaucoma Patients
Authors Ferraro V, Gaeta A, Barone G, Confalonieri F, Tredici C, Vinciguerra P, Di Maria A
Received 29 March 2025
Accepted for publication 17 June 2025
Published 16 July 2025 Volume 2025:19 Pages 2295—2303
DOI https://doi.org/10.2147/OPTH.S531288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Vanessa Ferraro,1 Alessandro Gaeta,2 Gianmaria Barone,3 Filippo Confalonieri,4 Costanza Tredici,4 Paolo Vinciguerra,3,4 Alessandra Di Maria4
1Department of Ophthalmology, Humanitas San Pio X, Milan, Italy; 2Department of Internal Medicine and Medical Specialties (DIMI), Università Di Genova, Genova, Italy; 3Department of Biomedical Sciences, Humanitas University, Pieve Emanuele, Milan, Italy; 4Department of Ophthalmology, IRCCS Humanitas Research Hospital, Rozzano, Milan, Italy
Correspondence: Alessandra Di Maria, Humanitas Research Hospital, Via Alessandro Manzoni, 56, Rozzano, Milan, 20089, Italy, Email [email protected]
Purpose: Glaucoma is commonly treated with prostaglandin analogs (PGAs), which effectively reduce intraocular pressure. However, PGAs can cause ocular side effects, including prostaglandin-associated periorbitopathy syndrome (PAPS), characterized by fat loss, enophthalmos and increased orbital structure prominence. The underlying mechanism is believed to involve adipocyte apoptosis, altered lipid metabolism, and changes in soft tissue dynamics. Currently, there is no standardized grading for enophthalmos, complicating its management. This study aimed to classify prostaglandin-induced enophthalmos and explore surgical or minimally invasive treatments, focusing on Italian Caucasian patients.
Materials and Methods: The study, conducted at IRCCS Humanitas Research Hospital between 2005 and 2023, assessed PAPS in primary open-angle glaucoma patients. It included a two-phase approach: (1) classification of enophthalmos using clinical and radiological measures to create a composite PAPS score; and (2) evaluation of treatment options, including Calcium Hydroxylapatite (CAHY) injections and autologous fat grafting.
Results: A retrospective analysis of 120 glaucoma patients with prostaglandin-induced enophthalmos identified severity levels using the PAPS classification. The proposed therapeutic algorithm stratifies treatment: mild cases benefit from conservative management or fillers, moderate cases from calcium hydroxyapatite (CAHY) injections, and severe cases from combined CAHY and autologous fat grafting.
Conclusion: A lack of a standardized grading system hinders consensus on management of PAPS. We propose a novel composite scoring system integrating six clinical parameters to stratify patients and tailor a minimally invasive therapeutic approach using calcium hydroxyapatite fillers and autologous fat grafting to restore orbital volume, improve eyelid aesthetics, and reduce complications. This classification system may serve as a clinical tool in patients with persistent or advanced PAPS who seek cosmetic correction or relief from functional symptoms.
Keywords: prostaglandin-associated periorbitopathy syndrome, prostaglandin-induced enophthalmos, calcium hydroxyapatite, autologous fat grafting, glaucoma therapy complications, classification system, enophtalmos, orbital changes in glaucoma
Introduction
Glaucoma, a leading cause of irreversible blindness, is commonly managed with prostaglandin analogs (PGAs), which are effective in reducing intraocular pressure (IOP). Despite their benefits, PGAs such as latanoprost, bimatoprost, and travoprost are associated with several ocular side effects, including periocular fat atrophy, which can lead to enophthalmos.1
Prolonged use can lead to atrophic changes in the periorbital tissues, collectively referred to as prostaglandin-associated periorbitopathy syndrome (PAPS).2 Clinical features include enophthalmos, ptosis, deepening of the upper eyelid sulcus, loss of periocular fat, and increased prominence of orbital structures.3 These changes, while typically reversible upon discontinuation, may cause aesthetic concerns and impact patient adherence to treatment. Early recognition of these effects is essential for clinicians to adjust therapy and manage patient expectations.4 The pathophysiology of prostaglandin-induced enophthalmos is multifactorial. The exact mechanism is not fully understood, but it is hypothesized that prostaglandins stimulate adipocyte apoptosis or alter local lipid metabolism.5 PGAs are believed to influence periocular fat metabolism, leading to localized fat atrophy.6 Additionally, PGAs may induce changes in orbital soft tissue dynamics and vascularization, exacerbating volume loss and structural changes in the orbit. Subclass differences have been observed, with bimatoprost showing a higher propensity for inducing these changes compared to latanoprost.7 Suppression of adipogenesis, inhibition of preadipocyte proliferation and adipocyte differentiation were suggested as possible pathophysiologic mechanisms in vitro studies.8
The absence of a consensus on grading enophthalmos complicates its evaluation and management. This study was structured in two phases. The first phase aimed to establish a classification of prostaglandin-induced enophthalmos. The second phase focused on proposing a surgical or minimally invasive management approach for enophthalmos correction, particularly in Italian Caucasian patients.
While mild forms of PAPS may go unnoticed or resolve with discontinuation of therapy, a subset of patients experience persistent or symptomatic changes requiring further evaluation. The aim of this study is to offer a structured approach for those patients with clinically significant, non-reversible manifestations.
Materials and Methods
Patients were treated and enrolled by the Oculoplastic Unit at the Department of Ophthalmology, IRCCS Humanitas Research Hospital, Rozzano, Milan, Italy, from January 2005 to December 2023. The study adhered to the Health Insurance Portability and Accountability Act and followed the principles outlined in the Declaration of Helsinki (2013). The study received approval from the Institutional Review Board.
Patients included in the study were diagnosed with primary open angle glaucoma (POAG) and exhibited documented enophthalmos following at least three years of PGAs use despite cessation of prostaglandin therapy for at least six months. Specific exclusion criteria were applied to ensure a homogeneous study population and minimize confounding factors. Patients were excluded if they had a history of orbital trauma, previous orbital or eyelid surgery, or congenital or acquired orbital disorders unrelated to prostaglandin use. Those with concomitant use of other medications known to affect orbital fat distribution, such as corticosteroids or systemic prostaglandin analogs, were also not considered for the study. Furthermore, individuals with significant ocular surface disease, severe dry eye, or other conditions that could interfere with the assessment of enophthalmos and eyelid position were excluded. Finally, patients with insufficient clinical records or incomplete follow-up data were not included in the study.
The study consisted of two phases: (1) classification of PAPS and (2) evaluation of surgical and minimally invasive management strategies.
Phase 1: Classification of Prostaglandin-Associated Periorbitopathy Syndrome
A comprehensive clinical assessment was conducted to establish a classification system based on clinical, functional, and radiological parameters. Detailed history is taken to investigate the use of prostaglandin-based eye drops, with a focus on the duration of treatment.
Examination
- Measurement of globe position using Hertel exophthalmometry categorized into the following ranges: <11 mm for mild enophthalmos, 11–13 mm for moderate enophthalmos, 13–15 mm for severe enophthalmos, and >15 mm for very severe enophthalmos. These ranges were used to assess the degree of orbital recession and classify the severity of enophthalmos in the study cohort.
- Measurement of Upper Eyelid Fold Position was classified into the following ranges: <20 mm for a normal position, 16–20 mm for a slight elevation, 10–16 mm for moderate elevation, and <10 mm for a markedly elevated eyelid fold.
- Assessment of marginal reflex distances (MRD1/MRD2) to quantify changes related to ptosis and enophthalmos severity: 0 mm for no visible upper eyelid margin, 0.5 mm for minimal visibility, 0.5–1.5 mm for moderate visibility, and >1.5 mm for pronounced visibility of the upper eyelid margin.
- Levator function was classified into the following ranges: <7 mm for poor levator function, 7–9 mm for fair function, 9–11 mm for good function, and >11 mm for excellent levator function.
- Entropion and Ciliary Margin Inversion were classified into the following categories: “Entropion with ciliary margin inversion” for cases where the eyelid margin was turned inward, “Grade II entropion without margin inversion” for moderate entropion without inversion of the margin, “Grade I entropion without margin inversion” for mild entropion without margin inversion, and “Absent” for cases where no entropion or ciliary margin inversion was observed.
- Fat pad atrophy was classified into the following categories: “Medial & Central” for cases where both the medial and central fat pads were atrophic, “Medial” for atrophy limited to the medial fat pad, “Central” for atrophy of the central fat pad, and “Absent” for cases with no noticeable atrophy of the fat pads.
Because the primary enophthalmos measurement (Hertel) and the Upper Eyelid Fold Position are often considered most directly related to the enophthalmos “look”, we assign them a weight of 2. The other four parameters (MRD1, Levator Function, Entropion & Ciliary Margin Inversion, Fat Pad Atrophy) are given a weight of 1. Each of the six clinical parameters is graded on a 0–3 scale (with 3 being the worst). For each patient, the composite score is calculated as follows:
Composite PAPS Score = 2×(Hertel grade) + 2×(Upper Eyelid Fold grade) + (MRD1 grade) + (Levator Function grade) + (Entropion grade) + (Fat Pad Atrophy grade)
The minimum score is 0 (if all parameters are 0) and the maximum is 24 (if all are 3).
We split the range 0–24 into four intervals:
• Group 0 (“None”): 0–6
• Group 1 (“Mild”): 7–12
• Group 2 (“Moderate”): 13–18
• Group 3 (“Severe”): 19–24
Phase 2: Management of PAPS
A structured approach for enophthalmos correction was proposed, based on previously studied treatment strategies.
- Calcium Hydroxylapatite (CAHY) Injection: Calcium hydroxylapatite (CAHY) injections were performed in the operating room under intravenous sedation and retrobulbar anesthesia (1% ropivacaine, 2 cc) to minimize pain. In the supine position, 1.3–2.6 cc of CAHY was injected transconjunctivally using a 23-gauge needle, targeting the intraconal and extraconal spaces between the medial or lateral rectus and inferior rectus muscles while avoiding deep posterior injections near the orbital apex.
- Autologous Fat Grafting (Lipofilling): Autologous fat grafting was proposed for selected patients to correct periorbital fibrotic tissue. Patients were informed about the procedure, including the unpredictable resorption rate of fat grafts, and provided informed consent. After routine preoperative analysis and antibiotic prophylaxis (cefazolin 2000 mg IV), liposuction was performed under sedation and local anesthesia, harvesting adipose tissue from the right flank. The fat was processed using the Coleman protocol and centrifuged at 3000 rpm for 3 minutes to purify the graft. Scar release with a needle preceded fat injection, ensuring even distribution through multiple entry points. Approximately 3 cc of adipose tissue was injected into fibrotic scars in the temporal area and upper and lower eyelids using a 12-gauge angiographic needle. A compressive dressing was applied to the donor site for 5 days, and antibiotic therapy was administered postoperatively.
This dual-phase approach aimed to standardize the classification of PAPS while offering a structured therapeutic framework for affected patients.
For statistical analysis, data were described as frequency and percentage.
Results
A retrospective statistical analysis was conducted on a cohort of 120 glaucoma patients with documented persistent enophthalmos following prostaglandin analog use. The gender distribution was as follows: 65 male patients (54.2%) and 55 female patients (45.8%). The median duration of prostaglandin analog use among the 120 patients was 5.2 years, with a standard deviation of 1.5 years.
For enophthalmos (Hertel), the majority of patients fell into Grade 2 (11–13 mm) with 40 patients (33.3%), followed closely by Grade 3 (<11 mm) with 45 patients (37.5%). A smaller proportion of patients were classified in Grade 1 (13–15 mm) with 30 patients (25%), while only 5 patients (4.2%) were categorized in Grade 0 (>15 mm).
Regarding the upper eyelid fold position, Grade 3 (<20 mm) was the most common category, with 50 patients (41.7%). This was followed by Grade 2 (16–20 mm), which included 35 patients (29.2%), and Grade 1 (10–16 mm) with 25 patients (20.8%). Grade 0 (<10 mm) was the least common, comprising 10 patients (8.3%).
For MRD1, the distribution was relatively even across the categories. Grade 1 (0.5–1.5 mm) had the highest number of patients, with 40 patients (33.3%), followed by Grade 2 (0.5 mm) with 30 patients (25%). Grade 3 (0 mm) and Grade 0 (>1.5 mm) each contained 25 patients (20.8%).
In terms of levator function, Grade 1 (9–11 mm) and Grade 0 (>11 mm) both had the largest numbers of patients, each with 40 patients (33.3%). Grade 2 (7–9 mm) included 35 patients (29.2%), and Grade 3 (<7 mm) was the least common, with just 10 patients (8.3%).
For entropion and ciliary margin inversion, Grade 1 (Grade I entropion without margin inversion) had the highest proportion of patients, with 60 patients (50%), followed by Grade 2 (Grade II entropion without margin inversion) with 25 patients (20.8%). Grade 0 (Absent) included 30 patients (25%), and Grade 3 (entropion with ciliary margin inversion) had only 5 patients (4.2%).
Lastly, in the classification of fat pad atrophy, Grade 2 (Medial) had the highest number of patients, comprising 40 patients (33.3%), followed by Grade 1 (Central) with 35 patients (29.2%). Grade 0 (Absent) also included 35 patients (29.2%), while Grade 3 (Medial & Central) was the least common, with 10 patients (8.3%).
These data are summarized in Table 1.
 |
Table 1 Distribution of the 120 Patients in All the Parameters Considered. |
Applying the composite PAPS score, we obtain the following distribution of the 120 patients in 4 groups of severity (Table 2).
 |
Table 2 Distribution of the 120 Patients in 4 Groups of Enophthalmos Severity, Applying the Composite PAPS Score |
The proposed classification for managing PAPS stratifies patients into four groups based on severity (Table 3):
- Grade 3 is the most severe, with an enophthalmos measurement of less than 11 mm, an upper eyelid fold position under 20 mm, and a margin reflex distance (MRD1) of 0 mm. The levator function is also limited to less than 7 mm, and entropion is present with ciliary margin inversion. Fat pad atrophy is observed in both the medial and central regions.
- Grade 2 presents with enophthalmos between 11 and 13 mm and upper eyelid fold position ranging from 16 to 20 mm. The MRD1 is 0.5 mm, levator function is between 7 and 9 mm, and there is a Grade II entropion without margin inversion. Fat pad atrophy is restricted to the medial region.
- Grade 1 indicates less severe symptoms, with enophthalmos ranging from 13 to 15 mm, an upper eyelid fold position between 10 and 16 mm, and MRD1 between 0.5 and 1.5 mm. Levator function is 9–11 mm, and entropion is classified as Grade I without margin inversion. Fat pad atrophy is also limited to the medial region.
- Grade 0, the mildest condition, features enophthalmos greater than 15 mm, an upper eyelid fold position below 10 mm, and MRD1 greater than 1.5 mm. Levator function exceeds 11 mm, and there is an absence of entropion, margin inversion, and fat pad atrophy.
 |
Table 3 The Proposed Classification for Managing PAPS Stratifies Patients Into Four Groups Based on Severity. |
In Table 4, a stage-specific approach allows for individualized treatment based on the severity of enophthalmos and associated soft tissue changes, optimizing both functional and cosmetic outcomes:
- Stages 0 and 1: Mild alterations are managed conservatively or with minimally invasive procedures to prevent progression.
- Stage 2 (Moderate): Injectable CAHY is proposed, as in our study on postenucleation socket syndrome, patients receiving injectable CAHY achieved a significant and lasting increase in orbital volume (mean augmentation of ~3.35 at 6 months with negligible loss over 10 years), with minimal complications.9
- Stage 3 (Severe): In cases with pronounced volume loss and tissue fibrosis—often seen in patients with a history of radiotherapy—the combination of CAHY fillers with autologous fat grafting not only restores volume but also improves tissue quality. In a separate series involving patients with post irradiation fibrosis and pain, autologous fat grafting resulted in a significant release of scar retraction, improved tissue trophism, and alleviation of pain, thereby creating optimal conditions for ocular implant placement.10
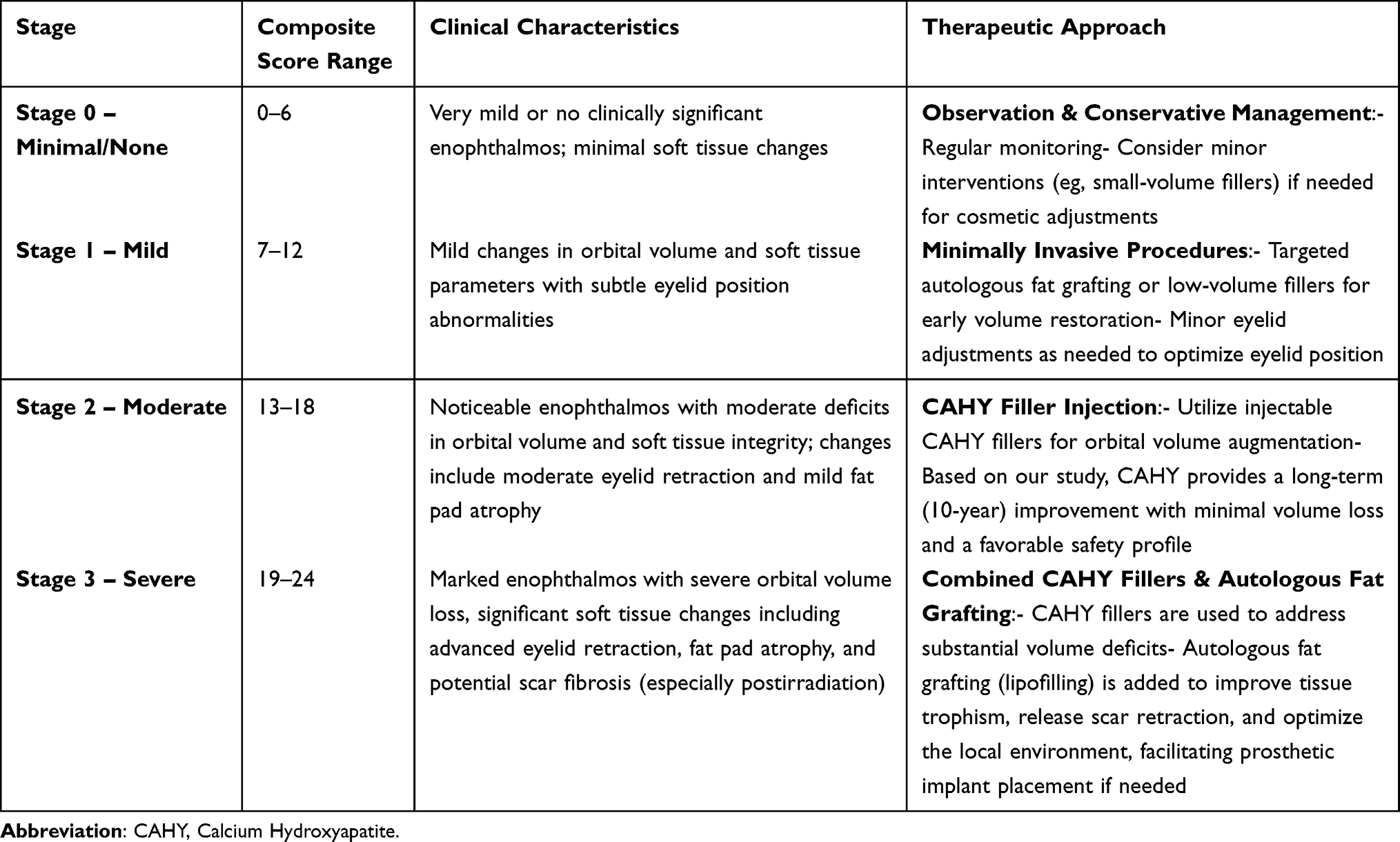 |
Table 4 Proposed Therapeutic Algorithm by Enophthalmos Stage. |
Discussion
Prostaglandins (PGs) are widely used in ophthalmology to treat glaucoma and ocular hypertension, with common analogs including latanoprost, bimatoprost, travoprost, and tafluprost. Although these drugs effectively reduce intraocular pressure (IOP) and are generally well tolerated, they can cause local and systemic side effects—one notable example being prostaglandin-associated periorbitopathy syndrome (PAPS).11 While advanced or persistent cases of PAPS may require surgical or minimally invasive correction, several studies, have shown that discontinuation of prostaglandin therapy can result in partial or even complete restoration of normal anatomy in early-stage or unilateral cases.12 This highlights the importance of timely diagnosis and careful monitoring before initiating interventional treatment. In our cohort, all patients had sustained anatomical changes persisting for at least six months following PGA discontinuation, suggesting a later stage of the syndrome with lower potential for spontaneous resolution. Nevertheless, conservative management remains an important first-line consideration, particularly in mild or early cases of PAPS.
PAPS often manifests as prostaglandin-induced enophthalmos, in which the eye appears abnormally sunken due to its deeper position within the orbit. This condition results from histological changes in orbital tissues, primarily prostaglandin-induced orbital fat reduction (orbital lipodystrophy) and is clinically similar to Post Enucleation-Socket Syndrome.13 At the molecular level, prostaglandins act by activating FP receptors—transmembrane proteins belonging to the G protein-coupled receptor (GPCR) family. When prostaglandin F2α (PGF2α) or its synthetic analogs bind to these receptors, a conformational change occurs that activates phospholipase C (PLC). This activation leads to the production of inositol trisphosphate (IP3) and diacylglycerol (DAG), which in turn elevate intracellular calcium levels and protein kinase C (PKC) activity. While these events contribute to smooth muscle contraction, altered lipid metabolism, and improved aqueous humor outflow (thereby reducing IOP), they also trigger lipolysis in orbital fat and promote periorbital fibrotic retraction—both of which disturb normal orbital-palpebral mechanics.3,14–17
Clinically, these changes can lead to a “sunken eye” appearance and facial asymmetry (pseudoproptosis). Patients might also experience a reduction in palpebral fissure width due to superior eyelid ptosis, as well as lower eyelid malpositions (such as entropion) and epiphora. The latter may result from compromised tear drainage caused by alterations in eyelid support and lacrimal pump function, changes that can also affect the position of the lacrimal puncta or cause nasolacrimal duct stenosis.18
The severity of PAPS appears to be dose-dependent, correlating with the duration of prostaglandin therapy and the specific agent used. Latanoprost, travoprost, and bimatoprost are most frequently implicated, though the prevalence and intensity of side effects may vary.19 Additionally, some studies suggest that hormonal factors may make females more susceptible, and age-related changes in skin elasticity and fat distribution may predispose older patients to these cosmetic alterations.
For example, a 2004 study observed that three patients treated unilaterally with bimatoprost developed deepening of the upper eyelid sulcus and a reduction in excess eyelid skin—findings that hinted at a link to the drug’s effect on Müller’s muscle.20 Another investigation reported that patients with primary open-angle glaucoma (POAG) exhibited reduced orbital fat volume, with orbital measurements revealing that, except in the most anterior region, individuals with POAG have bony orbits that are narrower both horizontally and vertically compared to controls, even though the overall orbital depth remains similar.8
The current literature lacks a standardized grading system for prostaglandin-associated periorbitopathy syndrome (PAPS), which has resulted in significant variability in both the diagnosis and management of the condition. Without a uniform method to assess the severity and progression of PAPS, clinicians have not been able to establish a universally accepted consensus on its treatment. This study was initiated to address this gap by developing a reliable and systematic grading framework, ultimately aiming to improve patient assessment and guide more consistent and effective therapeutic strategies.
To address the orbital volume deficit in PAPS, we propose a minimally invasive filler-based approach that offers immediate, predictable, and repeatable results with minimal discomfort and rapid recovery.21 Among available options, calcium hydroxylapatite (CAHY) is a semisolid filler—comprising 30% CAHY particles and 70% a matrix of glycerin, sodium carboxymethylcellulose, and water—that is FDA-approved for both cosmetic and functional applications, including oculoplastic surgery. Our study demonstrated that CAHY injections effectively improved enophthalmos, sulcus deformity, and ptosis without eliciting an inflammatory response while maintaining long-term orbital volume with minimal efficacy loss.9
The choice of CAHY was guided by several factors: the severity and specific location of volume loss in PAPS, the need to avoid fibrotic complications, and the advantages of rapid, outpatient treatment without the need for allergy testing. In our experience, proper injection technique—administering filler at the target site and ceasing injection before needle withdrawal—helped prevent complications such as filler migration and minimized transient injection site reactions like bruising and edema.21,22
Additionally, we recommend retrobulbar anesthesia (2 cc of 1% ropivacaine) delivered via a female Luer lock connected to a double-check valve syringe system to further reduce risks.23 For regenerative benefits, autologous fat grafting offers an alternative or adjunctive strategy, as its neovascularization and collagen deposition effects translate into improved fibrotic release, increased eyelid length, and significant pain reduction. While some graft resorption is expected, multiple small-volume sessions can optimize absorption and enhance the regenerative outcome.
One limitation of this study is the lack of stratification by specific prostaglandin analog. Due to the retrospective nature and frequent treatment switches over time, it was not feasible to isolate the effects of individual agents. Future prospective studies may help clarify the differential impact of specific PGAs on the development and severity of PAPS.
Conclusion
Prostaglandin-induced enophthalmos is a notable side effect of long-term glaucoma therapy. Early diagnosis and appropriate management can prevent aesthetic and psychological distress in selected symptomatic patients while ensuring adequate intraocular pressure control.
This novel classification and therapeutic management proposal represents a significant advancement in the tailored treatment of enophthalmos. By integrating six critical clinical parameters into a composite score, we are able to stratify patients into four distinct severity groups. This robust, evidence-based framework not only clarifies the spectrum of enophthalmos but also directly informs a stage-specific treatment algorithm. Ultimately, this innovative strategy provides clinicians with a practical and dynamic tool to optimize both functional and aesthetic outcomes, paving the way for more personalized and effective management of orbital volume deficiency.
Data Sharing Statement
Data are available upon reasonable request by the corresponding authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any sponsor or funder.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Alm A, Grierson I, Shields MB. Side effects associated with prostaglandin analog therapy. Surv Ophthalmol. 2008;53(6):S93–S105. doi:10.1016/j.survophthal.2008.08.004
2. Sakata R, Chang PY, Sung KR, et al. Prostaglandin-associated periorbitopathy syndrome (PAPS): addressing an unmet clinical need. Semin Ophthalmol. 2022;37(4):447–454. doi:10.1080/08820538.2021.2003824
3. Taketani Y, Yamagishi R, Fujishiro T, Igarashi M, Sakata R, Aihara M. Activation of the prostanoid FP receptor inhibits adipogenesis leading to deepening of the upper eyelid sulcus in prostaglandin-associated periorbitopathy. Invest Ophthalmol Vis Sci. 2014;55(3):1269–1276. doi:10.1167/iovs.13-12589
4. Hamedani M, Pournaras JAC, Goldblum D. Diagnosis and management of enophthalmos. Surv Ophthalmol. 2007;52(5):457–473. doi:10.1016/j.survophthal.2007.06.009
5. Hy C, Je L, Jw L, Hj P, Je L, Jh J. In vitro study of antiadipogenic profile of latanoprost, travoprost, bimatoprost, and tafluprost in human orbital preadiopocytes. J Ocul Pharmacol Ther off J Assoc Ocul Pharmacol Ther. 2012;28(2). doi:10.1089/jop.2011.0160
6. Custer PL, Kent TL. Observations on prostaglandin orbitopathy. Ophthal Plast Reconstr Surg. 2016;32(2):102–105. doi:10.1097/IOP.0000000000000431
7. Yamada H, Yoneda M, Gosho M, Kato T, Zako M. Bimatoprost, latanoprost, and tafluprost induce differential expression of matrix metalloproteinases and tissue inhibitor of metalloproteinases. BMC Ophthalmol. 2016;16(1):26. doi:10.1186/s12886-016-0202-8
8. Lk S, Da A, My K. Acute effects of glaucoma medications and benzalkonium chloride on pre-adipocyte proliferation and adipocyte cytotoxicity in vitro. Curr Eye Res. 2013;38(1). doi:10.3109/02713683.2012.733055
9. Di Maria A, Ferraro V, Trenti N, et al. Ten-year follow-up of orbital volume augmentation with calcium hydroxyapatite filler in postenucleation socket syndrome. Ophthal Plast Reconstr Surg. 2024;40(1):49–54. doi:10.1097/IOP.0000000000002500
10. Klinger F, Maione L, Vinci V, et al. Autologous fat graft in irradiated orbit postenucleation for retinoblastoma. Orbit Amst Neth. 2018;37(5):344–347. doi:10.1080/01676830.2017.1423358
11. Shen W, Huang B, Yang J. Ocular Surface Changes in Prostaglandin Analogue-Treated Patients. J Ophthalmol. 2019;2019:9798272. doi:10.1155/2019/9798272
12. Rabinowitz MP, Katz LJ, Moster MR, et al. Unilateral prostaglandin-associated periorbitopathy: a syndrome involving upper eyelid retraction distinguishable from the aging sunken eyelid. Ophthal Plast Reconstr Surg. 2015;31(5):373–378. doi:10.1097/IOP.0000000000000351
13. Jayaprakasam A, Ghazi-Nouri S. Periorbital fat atrophy - an unfamiliar side effect of prostaglandin analogues. Orbit Amst Neth. 2010;29(6):357–359. doi:10.3109/01676830.2010.527028
14. Olschewski H, Rose F, Schermuly R, et al. Prostacyclin and its analogues in the treatment of pulmonary hypertension. Pharmacol Ther. 2004;102(2):139–153. doi:10.1016/j.pharmthera.2004.01.003
15. García-Alonso V, Titos E, Alcaraz-Quiles J, et al. Prostaglandin E2 exerts multiple regulatory actions on human obese adipose tissue remodeling, inflammation, adaptive thermogenesis and lipolysis. PLoS One. 2016;11(4):e0153751. doi:10.1371/journal.pone.0153751
16. Narumiya S, Sugimoto Y, Ushikubi F. Prostanoid receptors: structures, properties, and functions. Physiol Rev. 1999;79(4):1193–1226. doi:10.1152/physrev.1999.79.4.1193
17. Pierce KL, Regan JW. Prostanoid receptor heterogeneity through alternative mRNA splicing. Life Sci. 1998;62(17–18):1479–1483. doi:10.1016/s0024-3205(98)00093-9
18. Di Maria A, Tredici C, Cozzupoli GM, Vinciguerra P, Confalonieri F. Effects of prostaglandin analogues on epiphora persistence after EN-DCR: a hypothesis-generating study. Eur J Ophthalmol. 2023;33(1):182–187. doi:10.1177/11206721221106138
19. Wang PX, Koh VTC, Cheng JF. Periorbital muscle atrophy associated with topical bimatoprost therapy. Clin Ophthalmol Auckl NZ. 2014;8:311–314. doi:10.2147/OPTH.S55754
20. Peplinski LS, Albiani Smith K. Deepening of lid sulcus from topical bimatoprost therapy. Optom Vis Sci off Publ Am Acad Optom. 2004;81(8):574–577. doi:10.1097/01.opx.0000141791.16683.4a
21. M R, Jcp R, Ra G. Periocular hyaluronic acid fillers: applications, implications, complications. Curr Opin Ophthalmol. 2019;30(5). doi:10.1097/ICU.0000000000000595
22. Hamed-Azzam S, B C, M A, et al. Filler migration to the orbit. Aesthet Surg J. 2021;41(6). doi:10.1093/asj/sjaa264
23. van L J, F D, P T, et al. Managing intravascular complications following treatment with calcium hydroxylapatite: an expert consensus. J Cosmet Dermatol. 2020;19(11). doi:10.1111/jocd.13353
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.