")
Back to Journals » Journal of Pain Research » Volume 17
Radiofrequency vs Steroid Injections for Spinal Facet and Sacroiliac Joint Pain: A Systematic Review and Meta-Analysis
Authors Xu B, Zhao X, Zhang L, Feng S, Li J, Xu Y
Received 6 April 2024
Accepted for publication 18 August 2024
Published 4 September 2024 Volume 2024:17 Pages 2903—2916
DOI https://doi.org/10.2147/JPR.S469615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael A Ueberall
Bo Xu,1 Xudong Zhao,2 Lei Zhang,1 Shouhan Feng,3 Jinxia Li,1 Ye Xu4
1Acupuncture and Rehabilitation Department, Huzhou Traditional Chinese Medicine Hospital Affiliated to Zhejiang Chinese Medical University, Huzhou, Zhejiang, People’s Republic of China; 2Physical Therapy Center, Huzhou Third Municipal Hospital, the Affiliated Hospital of Huzhou University, Huzhou, Zhejiang, People’s Republic of China; 3Oncology Department, Huzhou Traditional Chinese Medicine Hospital Affiliated to Zhejiang Chinese Medical University, Huzhou, Zhejiang, People’s Republic of China; 4Rehabilitation Department, Huzhou Third Municipal Hospital, the Affiliated Hospital of Huzhou University, Huzhou, Zhejiang, People’s Republic of China
Correspondence: Ye Xu, Rehabilitation Department, Huzhou Third Municipal Hospital, the Affiliated Hospital of Huzhou University, No. 2088 Tiaoxi East Road, Huzhou City, Zhejiang Province, People’s Republic of China, Email [email protected]
Purpose: Pain management for spinal facet joint (SFJ) and sacroiliac joint (SIJ) pain is challenging, often requiring interventions like radiofrequency ablation (RFA) or corticosteroid injections (CI). This study aims to assess and compare the effectiveness of CI and RFA in treating SFJ and SIJ pain. We combine these treatments due to their shared pathophysiology, similar therapeutic interventions, and the necessity for an integrated approach to spinal pain management.
Patients and methods: Literature search from PubMed, Scopus, CENTRAL and Google Scholar for published studies upto 31st December 2023, and reporting data of patients who were treated using CI of RFA for SFJ and SIJ pain. Pooled standardized mean difference (SMD) with a 95% Confidence Interval (CI) was calculated.
Results: Our meta-analysis incorporated thirteen studies. Overall, patients, treated with CI had a higher pain intensity score compared to patients treated with RFA (SMD=0.92; 95% CI: 0.19 to 1.65) at 3 months, and at 6 months (SMD=1.53; 95% CI: 0.66 to 2.40) after the treatment. No significant association was reported at 12 months (SMD=1.47; 95% CI: − 0.03 to 2.97). Subgroup analysis based on joint types revealed increased pain intensity scores in patients who were treated with CI for SIJ (SMD=1.25; 95% CI: 0.39 to 2.11) and SFJ (SMD=1.33; 95% CI: 0.09 to 2.57) pain. A negative but not significant effect was detected in patients, treated with CI for cervical joint pain (SMD=− 0.40; 95% CI: − 0.90 to 0.10). Patients treated with CI exhibited higher functional disability score compared to patients treated with RFA at 3 months (SMD=1.28; 95% CI: 0.20 to 2.35) post-treatment.
Conclusion: This study suggests that RFA may offer superior pain relief with longer duration compared to steroid injections for spinal facet and sacroiliac joint pain. Decision regarding specific interventions should be individualized and consider patient preferences, clinical context, and potential risks.
Keywords: radiofrequency ablation, steroid injections, spinal facet pain, sacroiliac joint pain, systematic review, meta-analysis, pain management
Introduction
Pain management for spinal facet joint (SFJ) and sacroiliac joint (SIJ) pain is challenging, and interventions, aimed to alleviate discomfort and improve patients’ quality of life are crucial.1,2
Over 25% of individuals with chronic lower back pain are reported to have SFJ, or more specifically, lumbar facet joint pain that is predominantly linked to degenerative osteoarthritis.3,4 SIJ pain accounts for up to 20% of low back pain cases, and poses its own set of challenges.5 Valid clinical and diagnostic tests for SIJ pain remain elusive, leading to diverse diagnostic approaches.6
Both SFJ and SIJ pain result from similar underlying mechanisms, including joint degeneration, inflammation, and nerve irritation, suggesting that therapies targeting one condition may also be effective for the other. An integrated approach is essential for effectively managing spinal pain, given the interconnected nature of spinal structures and the common occurrence of multi-faceted pain syndromes. Although the SIJ and facet joints differ in size and function—the SIJ being larger and primarily responsible for load transfer between the spine and lower limbs, while facet joints facilitate spinal movement and stability—there may be overlapping pain mechanisms and treatment responses. Investigating these conditions concurrently allows for the evaluation of shared diagnostic tools and therapeutic approaches, potentially leading to more efficient and effective management strategies. Additionally, comparing these distinct but related pain sources can highlight similarities and differences in their pathophysiology, enhancing the precision of interventions tailored to each condition.
Recently, radiofrequency ablation (RFA) and corticosteroid injections (CI) have emerged as prominent therapeutic modalities in pain management of such patients.7–9 The primary interventions for both conditions, RFA and CI, work by reducing inflammation and disrupting pain signals, supporting a combined therapeutic strategy. Injection with corticosteroids have shown promise in managing SFJ-related lower back pain.10 Additionally, the application of RFA in patients with SFJ pain has demonstrated effectiveness in reducing pain scores and enhancing overall quality of life.11,12 Current treatment options for patients with SIJ pain include pharmacotherapy, chiropractic manipulation, CI injections, and surgical fixation.13 Recently, RFA has gained popularity for SIJ pain management, with studies reporting promising results.14,15
However, due to variability in methodologies, including differences in techniques and selection criteria, the comparative effectiveness of RFA and CI in pain management of patients with SFJ and SIJ problem is still unclear. Given the significant impact of chronic spinal pain on quality of life, physical function, and healthcare resources, identifying the optimal treatment modality is essential. Insurance coverage for these procedures often varies, with some insurers being more inclined to cover steroid injections over RFA or vice versa. This variability can affect patients’ access to the most effective treatments. By providing a systematic comparison of the efficacy of these interventions, our study offers valuable insights that can inform insurance policy decisions. This meta-analysis aims to comparing the efficiency of CI and RFA in managing pain associated with SFJ and SIJ. Our results may provide valuable insights into the optimal approach for pain management of these conditions, guiding clinicians in making informed decisions for the benefit of their patients, reducing reliance on opioids, and enhancing overall management strategies for spinal pain.
Methods
Protocol Registration
We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)16 guidelines. The study is registered with PROSPERO with the identifier no. CRD42024496067.
Search Strategy
An electronic search was conducted on PubMed, Scopus, CENTRAL (Cochrane Central Register of Controlled Trials), and Google Scholar databases for English language papers published up to 31st December 2023. The search key terms included variations of “radiofrequency ablation”, such as “RF ablation” and “Radiofrequency”, and terms related to steroid injections, such as “Steroid injections” and “Corticosteroid injections”. The focus extended to spinal facet joint pain, represented by terms like “Spinal facet joint pain” and “Facet joint syndrome”, as well as sacroiliac joint pain, identified by terms like “Sacroiliac joint pain” and “Sacroiliitis”. Additionally, we included terms associated with osteoarthritis, such as “osteoarthritis”, “degenerative joint disease”, and “OA”, and terms related to axial pain, like “axial pain”, “axial back pain”, and “axial spine pain”. Our focus also extended to terms representing spinal facet joint pain, including “spinal facet joint pain” and “facet joint syndrome”, and sacroiliac joint pain, identified by terms like “sacroiliac joint pain” and “sacroiliitis”. Bibliography of retrieved studies and relevant reviews were further screened for the potential inclusion of additional studies.
Inclusion Criteria (PICOS)
Population (P): Patients with spinal facet joint (SFJ) or sacroiliac joint (SIJ)
Intervention (I): Radiofrequency ablation
Comparison (C): Corticosteroid injections
Outcome (O): Pain intensity
Study Design (S): Randomized controlled trials (RCTs).
Exclusion Criteria
- Non-English or non-human studies
- Studies lacking adequate data or with short follow-up periods
- Mixed interventions, inappropriate comparators, or high risk of bias
- Irrelevant conditions or duplicate data, published beyond a predefined date.
Data Extraction
During the initial phase of our systematic review, databases were searched, and titles and abstracts of identified studies were independently assessed by the two authors. Subsequently, full texts of papers meeting eligibility criteria were obtained for further analysis. The comprehensive data extraction process included key details such as author information, publication year, age distribution within the studied population, sample size, intervention specifics, pain intensity scores, functional disability scores, and any reported adverse events.
Outcomes
The primary outcome, pain intensity, was evaluated by visual analogue scale (VAS) or numerical rating scale (NRS). Pain intensity measurements were categorized into three distinct follow-up periods (3, 6, and 12 months after the procedure). Functional disability was measured using the Oswestry Disability Index (ODI) at 3 months after the treatment.
Quality Assessment
We used Grading of Recommendations, Assessment, Development, and Evaluations (GRADE), and specifically, GRADEpro tool, to assess evidence certainty for the outcomes. This tool considers factors such as study design, risk of bias, inconsistency, indirectness, imprecision, and publication bias.
Publication Bias
Publication bias was assessed by funnel plot analysis17 and Egger’s regression test.18
Statistical Analysis
All statistical analyses were done by STATA, version 12.0 (Stata Statistical Software, Release 12; StataCorp LP, College Station, TX) and Review Manager (RevMan v5.3 2014; Cochrane, London, England).
Results were presented as standardized mean difference (SMD) with 95% confidence interval (CI) for pain intensity and functional disability. Heterogeneity was assessed by the I2 statistic. In cases of significant (I2 > 50%) heterogeneity, random effects model was used. For I2 < 50%, fixed-effect model was used. Sensitivity analyses were done to validate the pooled observed effect. P <0.05 was statistically significant.
Results
The PRISMA flow diagram of our study (Figure 1) illustrates the systematic process of identifying and selecting relevant studies. Our initial systematic search across various databases yielded a total of 117 studies. After removing duplicate entries, we were left with 46 unique articles. These full texts were then meticulously screened for eligibility based on our inclusion and exclusion criteria. During this screening process, 31 studies were deemed irrelevant as they did not meet our criteria, and 2 studies were excluded because they did not report outcomes of interest. Finally, 13 studies19–31 were incorporated in the analysis.
 |
Figure 1 PRISMA 2020 Flow diagram for the selection of studies and specific reasons for exclusion from the present meta-analysis. Note: *Databases: PubMed, Scopus, CENTRAL and Google Scholar; **31 studies were deemed irrelevant as they did not meet our criteria; irrelevant populations (n=14), different interventions (n=5), lacking a comparator group (n=7), and non-randomized design (n=5). |
Characteristics of Studies
As shown in Table 1, eight out of 13 studies focused on patients with lumbar pain, two on cervical pain, and three on sacroiliac joint pain. The publication years of the studies ranged from 2012 to 2023, with sample sizes varying between 11 and 50 participants, and follow-up durations spanning from 6 to 12 months. Six studies were conducted in Asian populations, while seven were carried out in Caucasian populations.
 |
Table 1 Characteristics of Included Studies Investigating for Radiofrequency vs Steroid Injections for Spinal Facet and Sacroiliac Joint Pain |
All studies incorporated combined regimen of corticosteroid and local anesthetics for the corticosteroid groups. Methylprednisolone was used in six trials, typically in dosages ranging from 20 mg to 40 mg and often combined with varying amounts of bupivacaine. Betamethasone, used in three trials, had dosages ranging from 3 mg to 12 mg, while dexamethasone, used in two trials, was consistently dosed at 10 mg. Additionally, triamcinolone was used at 10 mg. These steroids were frequently combined with local anesthetics such as bupivacaine or lidocaine to enhance their effectiveness. Eight trials utilized pulsed radiofrequency (PRF), and five trials applied continuous RF (CRF). Adverse events were not reported in seven trials. A study by Lim et al 25 reported an increase in lower back pain (LBP) for two patients during the follow-up period, while another study by Do et al 19 reported hyperglycemia in one patient.
Main Findings
Pain Intensity at 3 Months
Nine studies reported data for pain intensity score at 3 months (Figure 2a). CI correlated with higher pain intensity score compared to RFA (SMD=0.92; 95% CI: 0.19 to 1.65), with substantial heterogeneity (I2 = 93%). Subgroup analysis based on type of joints showed that CI correlated with higher pain intensity score compared to RFA in patients with sacroiliac region (SMD=1.25; 95% CI: 0.39 to 2.11) and lumbar region (SMD=1.33; 95% CI: 0.09 to 2.57) pain. Negative, although not statistically significant effect of CI was reported in patients with cervical region pain (SMD=−0.40; 95% CI: −0.90 to 0.10).
 |
Figure 2 (a-d) Forest Plot for comparing the pain intensity in Radiofrequency vs steroid injections for spinal facet and sacroiliac joint pain across various time points (a) Pain intensity at 3 months, (b) Pain intensity at 6 months, (c) Pain intensity at 12 months and (d) Functional disability at 3 months. |
Pain Intensity at 6 Months
Eleven studies reported data of pain intensity score at 6 months (Figure 2b). CI led to higher pain intensity score than RFA (SMD=1.53; 95% CI: 0.66 to 2.40), with substantial heterogeneity (I2 = 95.4%). Subgroup analysis based on the type of joints showed higher pain intensity score in CI group compared to the RFA group in patients with the sacroiliac region (SMD=1.62; 95% CI: 0.79 to 2.45) and lumbar region (SMD=1.94; 95% CI: 0.92 to 2.97) pain. CI treatment was associated with negative effect in patients with the cervical region pain (SMD=−0.24; 95% CI: −0.74 to 0.26), but the difference was not statistically significant.
Pain Intensity at 12 Months
Five studies reported data of pain intensity at 12 months after the treatment (Figure 2c). Pain scores on the CI and the RFA groups were comparable (SMD=1.47; 95% CI: −0.03 to 2.97), with substantial heterogeneity (I2 = 97%). Subgroup analysis based on type of joints also showed comparable pain intensity scores in patients with sacroiliac region (SMD=0.10; 95% CI: −0.52 to 0.72) and lumbar region (SMD=1.82; 95% CI: −0.03 to 3.66) pain. No data were available for pain scores of patients with cervical region pain.
Functional Disability at 3 Months
Five studies reported data of functional disability scores at 3 months after the treatment. As shown in Figure 2d, patients in the CI group had a higher functional disability score compared to RFA group (SMD=1.28; 95% CI: 0.20 to 2.35), with substantial heterogeneity (I2 = 93.6%). Subgroup analysis based on type of joints also showed the CI correlated with significantly higher functional disability than RF ablation in patients with the sacroiliac region (SMD=0.75; 95% CI: 0.01 to 1.50) and lumbar region (SMD=1.41; 95% CI: 0.08 to 2.73) pain. No data were available for patients with the cervical region pain.
Sensitivity Analysis
Sensitivity analysis demonstrated that the pooled SMD estimates were not significantly influenced by the removal of any individual study (Figure 3). These findings indicate the robustness of our meta-analysis results, reassuring that they are not driven by any single study, enhancing confidence in the validity of our findings.
 |
Figure 3 Sensitivity plot for comparing the pain intensity in radiofrequency vs steroid injections for spinal facet and sacroiliac joint pain. |
Publication Bias
Funnel plot analysis revealed no apparent signs of asymmetry, with studies evenly distributed around the estimated effect. This suggests the absence of significant publication bias that could impact the results. Funnel plots for pain intensity at 3 months (p = 0.55), 6 months (p = 0.35), and 12 months (p = 0.30) and functional disability at 3 months (p = 0.69) are shown in Figure 4a–d.
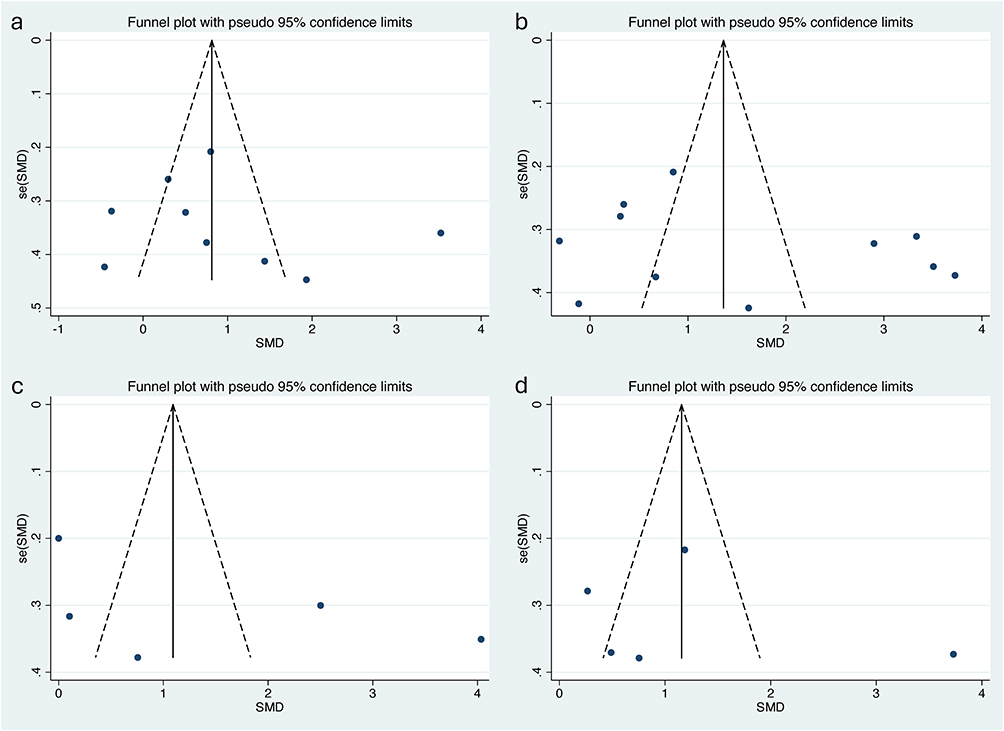 |
Figure 4 (a-d) Funnel Plot of for comparing the pain intensity in radiofrequency vs steroid injections for spinal facet and sacroiliac joint pain at various time point. |
Quality Assessment
Figure 5 illustrates the assessment of bias across various domains. The evaluation considered the method of randomization, adherence to interventions, management of missing data, precision in measurement, and reporting acceptability in a total of nine studies. Table 2 provides a summary of findings with each outcome based on GRADEpro, enhancing the understanding of the reliability of findings from the studies.
 |
Table 2 Summary of Evidences Using GRADEpro |
 |
Figure 5 Risk of Bias Summary. |
Discussion
Our findings emphasize the potential superiority of RFA in providing sustained pain relief for patients with chronic LBP. Chronic conditions such as LBP often necessitate long-term investment in conservative treatments, which are frequently limited in their efficacy. In this context, radiofrequency thermocoagulation presents itself as both an effective and relatively cost-effective alternative to traditional surgery.12 Conventional radiofrequency thermocoagulation induces localized injury with well-defined boundaries by applying radiofrequency current to heat adjacent tissue.33 Studies have shown that temperatures up to 80°C can lead to the dissolution and necrosis of unmyelinated nerve C fibers, blocking neuralgia-conducting nerves for extended periods. In contrast, pulsed radiofrequency does not induce neuro-destructive processes like conventional radiofrequency,34 a distinction particularly relevant for sensitive nerves in regions such as the head, neck, dorsal root ganglia, and trigeminal ganglia.
Intraarticular (IA) injections, while potentially offering greater accuracy due to varied facet joint innervation, pose challenges due to their difficulty and increased pain compared to medial branch block (MBB). The choice between IA and MBB approaches may necessitate a trade-off between accuracy and patient comfort.35 The included studies employed diverse techniques for RFA, lacked standardized approaches, and reported varied adverse events. Different pain assessment scales and follow-up intervals were utilized, with no consensus on a superior technique or standardization. Stricter criteria for MBBs have been associated with improved outcomes in lumbar RFA, while more relaxed standards have shown reduced efficacy. The absence of a standardized approach or superior technique indicates a lack of conclusive evidence supporting one method over another, highlighting the need for further research and standardization in RFA procedures to enhance clarity for clinicians and improve patient outcomes.
The variations in steroid dosages and methodologies across the included studies present significant challenges in drawing firm conclusions about their efficacy and safety. Different types and dosages of steroids were combined with various local anesthetics in differing concentrations, making direct comparisons difficult. The methodologies employed in these studies also differed, impacting the ability to assess long-term outcomes. Additionally, the inclusion criteria and patient populations were not uniform, which could influence the generalizability of the results. The lack of standardized measures for outcomes and the reporting of adverse events further complicates the analysis, making it challenging to perform a meta-analysis or systematic review that provides definitive conclusions.
Corticosteroids can exert their anti-inflammatory effects to alleviate synovial inflammation and attenuate the excitability of nociceptive nerve fibers, thus providing pain relief. However, potential adverse effects, such as inhibition of the pituitary-adrenal axis, hyperadrenocorticism, osteoporosis, avascular necrosis, and steroid myopathy, pose safety concerns.36,37 In contrast, RFA therapy eliminates the need for corticosteroid administration, thereby avoiding these side effects.
It is essential to acknowledge limitations for a comprehensive interpretation of our findings. Small sample sizes observed in most of the included studies may compromise the generalizability and statistical robustness of the results. Larger sample sizes are necessary to improve reliability and accommodate potential variability in patient responses. Additionally, there is substantial heterogeneity among the studies due to variations in patient populations, procedural techniques, and outcome measures. The diversity in procedures and agents used across trials contributes to this heterogeneity, particularly evident within the comparison between intervention groups involving IA and MBB approaches. Moreover, the choice between pulsed and continuous RFA methods may impact outcomes, potentially influencing the depth of analysis. These limitations should be considered when interpreting the study findings, and further research is needed to address these challenges effectively.
Conclusion
This study suggests that RFA may offer superior pain relief and a longer duration of efficacy compared to steroid injections for spinal facet and sacroiliac joint pain. However, the choice between these interventions should be individualized, considering patient preferences, clinical context, and potential risks. Further research, particularly large-scale randomized controlled trials, is needed to strengthen the evidence and refine clinical recommendations.
Funding
Huzhou City Science and Technology Plan Project (2022GY21).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Won HS, Yang M, Kim YD. Facet joint injections for management of low back pain: a clinically focused review. Anesth Pain Med. 2020;15(1):8–18. doi:10.17085/apm.2020.15.1.8
2. Rashbaum RF, Ohnmeiss DD, Lindley EM, Kitchel SH, Patel VV. Sacroiliac joint pain and its treatment. Clin Spine Surg. 2016;29(2):42–48. doi:10.1097/BSD.0000000000000359
3. Kalichman L, Li L, Kim DH, et al. Facet joint osteoarthritis and low back pain in the community-based population. Spine. 2008;33(23):2560–2565. doi:10.1097/BRS.0b013e318184ef95
4. Perolat R, Kastler A, Nicot B, et al. Facet joint syndrome: from diagnosis to interventional management. Insights Imag. 2018;9(5):773–789. doi:10.1007/s13244-018-0638-x
5. Cohen SP, Chen Y, Neufeld NJ. Sacroiliac joint pain: a comprehensive review of epidemiology, diagnosis and treatment. Expert Rev Neurother. 2013;13(1):99–116. doi:10.1586/ern.12.148
6. Falowski S, Sayed D, Pope J, et al. A review and algorithm in the diagnosis and treatment of sacroiliac joint pain. J Pain Res. 2020;13:3337–3348. doi:10.2147/JPR.S279390
7. Li SJ, Zhang SL, Feng D. A comparison of pulsed radiofrequency and radiofrequency denervation for lumbar facet joint pain. J Orthop Surg Res. 2023;18(1):331. doi:10.1186/s13018-023-03814-5
8. Kwak DG, Kwak SG, Lee AY, Chang MC. Outcome of intra-articular lumbar facet joint corticosteroid injection according to the severity of facet joint arthritis. Exp Ther Med. 2019;18(5):4132–4136. doi:10.3892/etm.2019.8031
9. Çetin A, Yektaş A. Evaluation of the short- and long-term effectiveness of pulsed radiofrequency and conventional radiofrequency performed for medial branch block in patients with lumbar facet joint pain. Pain Res Manag. 2018;2018:7492753. doi:10.1155/2018/7492753
10. Benoist M, Boulu P, Hayem G. Epidural steroid injections in the management of low-back pain with radiculopathy: an update of their efficacy and safety. Eur Spine J. 2012;21(2):204–213. doi:10.1007/s00586-011-2007-z
11. Das G, Surange P, Agarwal A, et al. Radiofrequency ablation in chronic pain syndromes: an evidence‑ and consensus‑based Indian Society for the Study of Pain Guidelines, 2022. Indian J Pain. 2022;36:S2–3.
12. Leggett LE, Soril LJJ, Lorenzetti DL, et al. Radiofrequency ablation for chronic low back pain: a systematic review of randomized controlled trials. Pain Res Manag. 2014;19(5):e146–153. doi:10.1155/2014/834369
13. Aranke M, McCrudy G, Rooney K, et al. Minimally invasive and conservative interventions for the treatment of sacroiliac joint pain: a review of recent literature. Orthop Rev. 2022;14(4):34098. doi:10.52965/001c.34098
14. Tseng C, Chen KT, Fong YC, et al. Biportal endoscopic radiofrequency ablation of the sacroiliac joint complex in the treatment of chronic low back pain: a technical note with 1-year follow-up. Diagnostics. 2023;13(2):229. doi:10.3390/diagnostics13020229
15. Lowe M, Okunlola O, Raza S, et al. Radiofrequency ablation as an effective long-term treatment for chronic sacroiliac joint pain: a systematic review of randomized controlled trials. Cureus. 2022;14(6):e26327. doi:10.7759/cureus.26327
16. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi:10.1186/2046-4053-4-1
17. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–1101. doi:10.2307/2533446
18. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
19. Do KH, Ahn SH, Cho YW, Chang MC. Comparison of intra-articular lumbar facet joint pulsed radiofrequency and intra-articular lumbar facet joint corticosteroid injection for management of lumbar facet joint pain: a randomized controlled trial. Medicine. 2017;96(13):e6524. doi:10.1097/MD.0000000000006524
20. Civelek E, Cansever T, Kabatas S, et al. Comparison of effectiveness of facet joint injection and radiofrequency denervation in chronic low back pain. Turk Neurosurg. 2012;22(2):200–206. doi:10.5137/1019-5149.JTN.5207-11.1
21. Duger C, Kol I, Kaygusuz K, Gursoy S, Mimaroglu C. Effects of facet joint nerve block addition to radiofrequency in the treatment of low back pain. HealthMED. 2012;6:2052–2056.
22. Dutta K, Dey S, Bhattacharyya P, Agarwal S, Dev P. Comparison of efficacy of lateral branch pulsed radiofrequency denervation and intraarticular depot methylprednisolone injection for sacroiliac joint pain. Pain Physician. 2018;21(5):489–496.
23. Hashemi M, Hashemian M, Mohajerani SA, Sharifi G. Effect of pulsed radiofrequency in treatment of facet-joint origin back pain in patients with degenerative spondylolisthesis. Eur Spine J. 2014;23(9):1927–1932. doi:10.1007/s00586-014-3412-x
24. Lakemeier S, Lind M, Schultz W, et al. A comparison of intraarticular lumbar facet joint steroid injections and lumbar facet joint radiofrequency denervation in the treatment of low back pain: a randomized, controlled, double-blind trial. Anesth Analg. 2013;117(1):228–235. doi:10.1213/ANE.0b013e3182910c4d
25. Lim JW, Cho YW, Lee DG, Chang MC. Comparison of intraarticular pulsed radiofrequency and intraarticular corticosteroid injection for management of cervical facet joint pain. Pain Physician. 2017;20(6):E961–E967.
26. Martinez CH, Richardson CR, Han MK, Cigolle CT. Chronic obstructive pulmonary disease, cognitive impairment, and development of disability: the health and retirement study. Ann Am Thorac Soc. 2014;11(9):1362–1370. doi:10.1513/AnnalsATS.201405-187OC
27. McCormick ZL, Conger A, Kendall R, et al. A pragmatic randomized prospective trial of cooled radiofrequency ablation of the medial branch nerves versus facet joint injection of corticosteroid for the treatment of lumbar facet syndrome: 12 month outcomes. Pain Med. 2023;24(12):1318–1331. doi:10.1093/pm/pnad107
28. Salman O, Sayed Gad G, Mohamed A, Rafae H, Abdelfatah A. Randomized, controlled blind study comparing sacroiliac intra-articular steroid injection to radiofrequency denervation for sacroiliac joint pain. Egypt J Anaesth. 2015;32. doi:10.1016/j.egja.2015.07.005
29. Shin SM, Kwak SG, Lee DG, Chang MC. Clinical effectiveness of intra-articular pulsed radiofrequency compared to intra-articular corticosteroid injection for management of atlanto-occipital joint pain: a prospective randomized controlled pilot study. Spine. 2018;43(11):741–746. doi:10.1097/BRS.0000000000002414
30. Yasar D, Korgun O, Emine D. Radiofrequency and methylprednisolone in treatment of lower back pain caused by facet joint syndrome: comparison of the outcomes. Asian J Neurosurg. 2018;13(2):283–287. doi:10.4103/1793-5482.228569
31. Zhou Q, Zhou F, Wang L, Liu K. An investigation on the effect of improved X-rays-guided radiofrequency thermocoagulation denervation on lumbar facet joint syndrome. Clin Neurol Neurosurg. 2016;148:115–120. doi:10.1016/j.clineuro.2016.07.018
32. Cohen SP, Moon JY, Brummett CM, White RL, Larkin TM. Medial branch blocks or intra-articular injections as a prognostic tool before lumbar facet radiofrequency denervation: a multicenter, case-control study. Reg Anesth Pain Med. 2015;40(4):376–383. doi:10.1097/AAP.0000000000000229
33. Shealy CN. Percutaneous radiofrequency denervation of spinal facets. Treatment for chronic back pain and sciatica. J Neurosurg. 1975;43(4):448–451. doi:10.3171/jns.1975.43.4.0448
34. Byrd D, Mackey S. Pulsed radiofrequency for chronic pain. Curr Pain Headache Rep. 2008;12(1):37–41. doi:10.1007/s11916-008-0008-3
35. Cohen SP, Bhaskar A, Bhatia A, et al. Consensus practice guidelines on interventions for lumbar facet joint pain from a multispecialty, international working group. Reg Anesth Pain Med. 2020;45(6):424–467. doi:10.1136/rapm-2019-101243
36. Brinks A, Koes BW, Volkers ACW, Verhaar JAN, Bierma-Zeinstra SMA. Adverse effects of extra-articular corticosteroid injections: a systematic review. BMC Musculoskelet Disord. 2010;11(1):206. doi:10.1186/1471-2474-11-206
37. Kamel SI, Rosas HG, Gorbachova T. Local and systemic side effects of corticosteroid injections for musculoskeletal indications. AJR Am J Roentgenol. 2023;222(3). doi:10.2214/AJR.23.30458
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.