")
Back to Journals » Journal of Inflammation Research » Volume 18
RAR-Based Prognostic Model for Predicting Overall Survival in Hepatitis B Virus-Related Hepatocellular Carcinoma: A Multicenter Study
Authors Tan M, Liu Y, Dai W, Chen Y, Cai D, Chen B, Wang J, You R, Li D, Huang H
Received 10 March 2025
Accepted for publication 8 July 2025
Published 11 July 2025 Volume 2025:18 Pages 9159—9170
DOI https://doi.org/10.2147/JIR.S527420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Junhao Wang
Maoqing Tan,1,* Yifan Liu,2,3,* Wei Dai,1,* Yanling Chen,4 Danni Cai,1 Baomin Chen,3 Jing Wang,1 Ruolan You,1 Dongliang Li,5 Huifang Huang1
1Central Laboratory, Fujian Medical University Union Hospital, Fuzhou, Fujian, 350001, People’s Republic of China; 2First Central Clinic Institute, Tianjin Medical University, Tianjin, People’s Republic of China; 3Department of Hepatobiliary Surgery, The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, Guangdong, 510000, People’s Republic of China; 4Department of Hepatobiliary Surgery and Fujian Institute of Hepatobiliary Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian, 350001, People’s Republic of China; 5Department of Hepatobiliary Disease, Fuzong Clinical Medical College of Fujian Medical University (900TH Hospital of Joint Logistics Support Force), Fuzhou, Fujian, 350025, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huifang Huang, Central Laboratory, Fujian Medical University Union Hospital, 29 Xinquan Road, Fuzhou, Fujian, 350001, People’s Republic of China, Tel +8613365910318, Fax +86 591-87113828, Email [email protected] Dongliang Li, Department of Hepatobiliary Disease, 900TH Hospital of Joint Logistics Support Force, Xi Er Huan Bei Road, Fuzhou, Fujian, 350025, People’s Republic of China, Tel +8613665052006, Fax +86 591-22859128, Email [email protected]
Purpose: Hepatitis B virus-related hepatocellular carcinoma poses a significant global health challenge. This study aimed to develop and validate a novel prognostic nomogram integrating the red blood cell distribution width-to-albumin ratio for predicting patients’ overall survival.
Patients and Methods: A retrospective cohort of 1403 patients was divided into training, internal validation, and external validation cohorts. A multivariate Cox regression model selected variables to construct a nomogram and an online calculator, which were subsequently validated.
Results: The ratio emerged as an independent risk factor for long-term survival (hazard ratio: 5.808, 95% confidence interval: 1.721– 19.599). A prognostic nomogram incorporating nine variables based on the ratio was developed. Calibration curves demonstrated high concordance between the predicted and actual 3-year survival rates. Decision curve analysis indicated that the nomogram significantly increased the net benefit of predicting 3-year survival. Based on the area under the receiver operating characteristic curves, the nomogram outperformed traditional models in predicting survival across the three cohorts. Patients were stratified into low-, intermediate-, and high-risk groups based on risk scores calculated from the nomogram. In all cohorts, the median survival time of the high-risk group was significantly shorter than that of the intermediate- and low-risk groups. An online calculator, deployed via a web-based platform, facilitated convenient mortality risk prediction for these patients.
Conclusion: The ratio-based nomogram we developed can accurately predict the survival of patients with hepatitis B virus-related hepatocellular carcinoma, serving as an effective auxiliary tool for clinical personalized treatment and prognostic assessment.
Keywords: albumin, hepatitis B virus-related hepatocellular carcinoma, nomogram, prognosis, red blood cell distribution width
Introduction
Hepatocellular carcinoma (HCC) ranks among the most prevalent malignant tumors worldwide, with approximately 630,000 new cases reported annually.1 Notably, over half of these cases are diagnosed in China, where hepatitis B virus (HBV) infection serves as the primary etiological factor, contributing to around 80% of HCC cases.2 Individuals with chronic HBV infection face a 10- to 15-fold higher risk of developing HCC compared to those without the infection.3 Despite advancements in treatment, the prognosis for HCC remains unfavorable, characterized by a high recurrence rate and a 5-year overall survival (OS) rate of merely 18%.4,5 Consequently, accurately assessing the prognosis of HBV-associated HCC is critical for tailoring treatment plans and optimizing therapeutic outcomes.
Currently, the Barcelona Clinic Liver Cancer (BCLC) staging system, Tumor Node Metastasis (TNM) staging system, and Cancer of the Liver Italian Program (CLIP) scoring system are among the most widely utilized clinical prognostic assessment tools for HCC. Although these models provide insights into the prognosis of patients with HCC, they each have notable limitations. For example, the BCLC staging system is based on follow-up studies of non-surgical and non-transplant patients with HCC. However, the underlying data primarily come from small Western cohorts where HCV infection is the dominant cause, making the system potentially less applicable to Asian countries, especially China, where HBV infection is more prevalent.6,7 Furthermore, the TNM staging system is more suitable for patients undergoing surgical tumor resection, whereas its predictive power is limited when applied to non-surgical treatments.8,9 The CLIP scoring system also has its limitations, as the tumor morphology classification it uses may be overly simplistic and not universally applicable across different regions. Additionally, the CLIP system may lack sensitivity in adequately stratifying all patient groups, making it difficult to apply in certain clinical scenarios, which limits its usefulness in management decisions.10–13 Therefore, developing new HBV-HCC prognostic models as a complementary tool to these existing systems is crucial.
The red blood cell distribution width (RDW) and albumin (ALB) level serve as markers that reflect the body’s inflammatory and nutritional status, both of which are intimately linked to tumorigenesis and tumor progression. Smirne et al5 have highlighted the potential role of RDW as an early indicator of mortality risk in patients with HCC. Similarly, our prior studies demonstrated a notable elevation in RDW levels among individuals with HBV-HCC, reinforcing its promise as a prognostic biomarker for this population.14 As the most abundant plasma protein, ALB is predominantly synthesized by the liver. It contributes to key physiological processes, such as plasma volume regulation, immune modulation, oxidative stress reduction, and safeguarding endothelial cells from apoptosis.15 Evidence has shown that lower ALB levels are correlated with larger HCC tumors, whereas higher ALB levels can suppress HCC growth, invasion, and metastasis.16–19 The RDW to ALB ratio (RAR), a novel inflammatory biomarker that integrates both the RDW and ALB level, is extensively utilized in the prognostic evaluation of a spectrum of inflammatory conditions. An increased RAR, reflecting the interplay between systemic inflammation and nutritional status, has been associated not only with poor prognosis in cardiovascular diseases such as non-ischemic heart failure and post-percutaneous coronary intervention mortality,20,21 but emerging evidence also suggests its involvement in cancer progression and tumor-related inflammatory processes, underscoring its potential prognostic value in HBV-HCC.22–24
Recent methodological frameworks emphasize the importance of rigor and clinical relevance in prognostic model development.25,26 These guidelines informed the design of our model, particularly in aspects such as variable selection, validation, and generalizability.
In this study, we hypothesized that the RAR could serve as a potential prognostic marker for HBV-HCC. Our goal was to develop a novel prognostic model for HBV-HCC based on the RAR through a multicenter cohort study. This model was compared with established systems, including the BCLC, TNM, and CLIP, to evaluate its predictive accuracy. Ultimately, we aimed to provide a new foundation for the clinical development of personalized treatment strategies for HCC.
Materials and Methods
Patients
We retrospectively collected data from 4029 patients initially diagnosed with HBV-HCC across three tertiary teaching hospitals in China. The cohort consisted of 2326 patients from the 900TH Hospital of Joint Logistics Support Force (900H) diagnosed between 2012 and 2022. Additionally, 1074 and 629 patients were identified at Fujian Medical University Union Hospital (FJMUUH) and the First Affiliated Hospital of Sun Yat-sen University (FAHSYSU), respectively, from 2017 to 2019. Inclusion criteria were: (1) diagnosis of HCC confirmed by computed tomography/magnetic resonance imaging or pathology; (2) hepatitis B surface antigen detected continuously for over six months; and (3) no prior antitumor treatment. Exclusion criteria were: (1) co-infection with other hepatitis viruses; (2) concurrent malignancies; (3) gastrointestinal bleeding within the past six months; (4) concomitant hematologic disorders; and (5) incomplete clinical or follow-up data. The patient inclusion flowchart is shown in Figure S1. A total of 906 patients from 900H met the selection criteria and were randomly divided into a training cohort (n=604) and an internal validation cohort (n=302) in a 2∶1 ratio. Additionally, 497 patients from FJMUUH and FAHSYSU formed the external validation cohort.
We retrospectively collected patients’ medical histories and baseline characteristics from the case record system, including demographic information and laboratory parameters. OS was defined as the interval from radiological diagnosis to death from any cause or the date of the last follow-up (June 2023). Based on the initial treatment modality, patients were classified into a local intervention group (surgical group) and a systemic therapy group (non-surgical group). The local intervention group included hepatic resection, radiofrequency ablation (RFA), and transarterial chemoembolization (TACE), while the systemic therapy group consisted of targeted therapy, immune checkpoint inhibitors, chemotherapy, external radiotherapy, and best supportive care (BSC). It should be noted that although TACE is a minimally invasive procedure, it was classified as a local intervention in this study due to its locoregional tumor control mechanism.
Development and Validation of a Nomogram
In the training cohort, a forward stepwise Cox regression analysis using the likelihood ratio method was employed for variable selection. The analysis included 11 continuous variables: age, white blood cell count, neutrophil count, lymphocyte count (LYMs), red blood cell count, mean corpuscular volume, hematocrit, platelet count, RAR, total bilirubin (TBIL), and tumor diameter, as well as 12 categorical variables: sex, Child–Pugh grade, alpha-fetoprotein, HBV DNA, hepatitis B e-antigen status, cirrhosis, number of tumors, portal vein tumor thrombosis (PVTT), metastasis, hypertension, diabetes, and initial treatment approach. Variables with a p-value < 0.05 were retained for model construction, and a nomogram prognostic model was subsequently developed.
Internal and external validation cohorts tested model stability, while receiver operating characteristic (ROC) curves measured its predictive power for 1-, 2-, and 3-year OS. Additionally, calibration curves were utilized to assess the predictive model’s accuracy, and decision curve analysis was conducted to determine the clinical utility of the nomogram.
Comparison of Nomogram-Based Risk Classification
The individual risk stratification was computed using the established nomogram, and patients were subsequently classified into three prognostic subgroups (low, intermediate, and high risk) through optimal threshold values determined by X-tile 3.6.1 analysis. Kaplan–Meier survival curves were constructed to compare OS among these risk groups, thereby evaluating the nomogram’s discriminative ability. Additionally, ROC curve analysis was performed to evaluate the comparative prognostic capability between our nomogram and conventional staging classifications (BCLC, TNM, and CLIP) in predicting survival outcomes for HBV-associated HCC patients.
Statistical Analysis
To examine whether the variables conformed to a normal distribution, the Kolmogorov–Smirnov test was employed. Continuous data are presented as mean ± standard deviation if normally distributed and as median with interquartile range (IQR) otherwise. Categorical variables are expressed as counts and percentages. Group comparisons involved the t-test for normal continuous data, the Mann–Whitney U-test for non-normal continuous data, and the chi-square test for categorical data. To assess whether the inclusion of our nomogram provided better discriminatory performance compared to conventional prognostic models, we applied DeLong’s test to evaluate the statistical significance of differences in AUC values. All statistical analyses were performed using R version 4.1.3 and SPSS version 26.0. A two-tailed p-value < 0.05 was considered statistically significant.
Results
Patient Characteristics
The study cohort comprised 1403 patients in total. Specifically, 906 patients were included from the 900H, with a median age of 54 (IQR: 46–63) years, comprising 86.2% (781/906) males; 70.6% (640/906) received surgical treatment. FJMUUH enrolled 379 patients, with a median age of 58 (IQR: 51–65) years, of whom 85% (322/379) were male, and 94.7% (359/379) underwent surgery. FAHSYSU contributed 118 patients, with a median age of 52 (IQR: 44–60) years, of whom 91.5% (108/118) were male, and 89.8% (106/118) received surgical treatment. Table 1 presents detailed baseline characteristics of patients from the three centers. Table S1 provides the baseline characteristics of the training and internal validation cohorts, showing no statistically significant differences between the groups (all p > 0.05).
 |
Table 1 Clinical Characteristics of the Patients in Three Healthcare Facilities |
Development of the Nomogram
Multivariate Cox regression analysis identified LYM [hazard ratio (HR): 0.715, 95% confidence interval (CI): 0.591–0.865], the RAR (HR: 5.808, 95% CI: 1.721–19.599), TBIL (HR: 1.003, 95% CI: 1.000–1.006), tumor diameter (HR: 1.062, 95% CI: 1.040–1.085), Child–Pugh grade (HR: 2.125, 95% CI: 1.201–3.759), PVTT (HR: 1.737, 95% CI: 1.342–2.248), tumor number (HR: 1.767, 95% CI: 1.414–2.207), tumor metastasis (HR: 1.360, 95% CI: 1.058–1.749), and initial treatment modality (HR: 1.842, 95% CI: 1.438–2.358) as independent prognostic factors for long-term OS in patients with HBV-HCC (Table 2). Among these, the RAR had the highest HR, indicating its significant impact on prognosis.
 |
Table 2 Multivariate Cox Regression Analysis with a Forward Likelihood Ratio Method for OS of HBV-Related HCC Patients |
Based on multivariate Cox regression findings, we constructed a predictive model (RAR-Nomogram) integrating nine identified prognostic factors to estimate 1-, 2-, and 3-year overall survival probabilities in HBV-associated HCC patients, as illustrated in Figure 1.
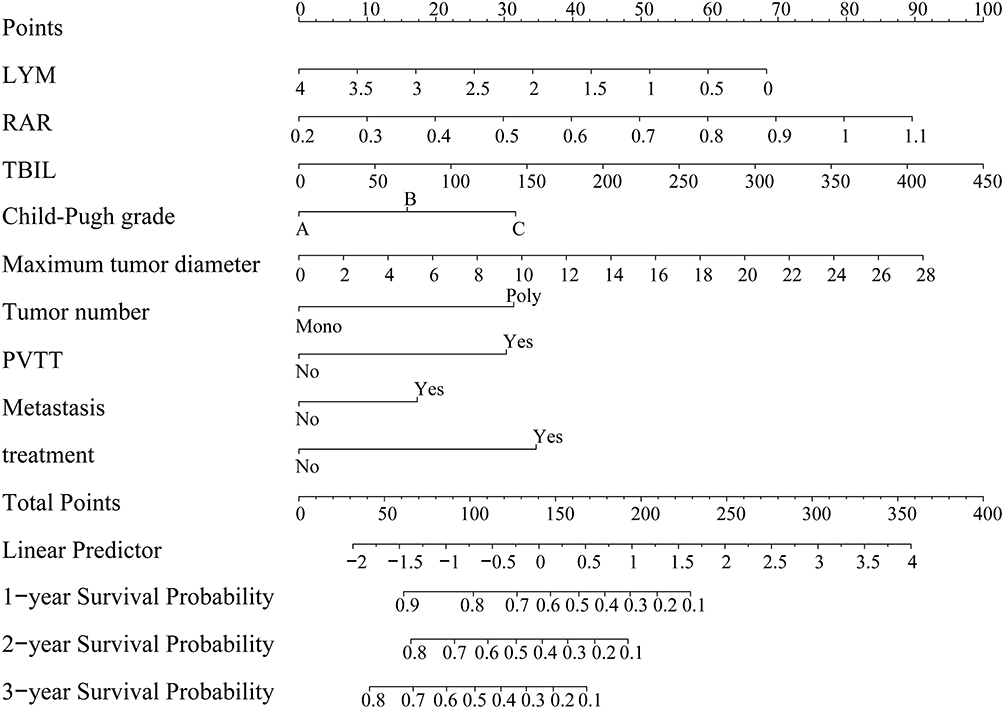 |
Figure 1 Survival nomogram for patients with HBV-HCC. Abbreviations: LYM, lymphocyte; RAR, red blood cell distribution width to albumin ratio; TBIL, total bilirubin; PVTT, portal vein tumor thrombus; HBV-HCC, hepatitis B virus-related hepatocellular carcinoma. |
Validation of the Nomogram Model
The accuracy of the RAR-Nomogram was assessed by evaluating its discriminative power and calibration performance in both internal and external validation cohorts. Discriminative ability was assessed using the area under the ROC curve (AUC). In the training cohort, the AUCs for 1-, 2-, and 3-year OS were 0.881, 0.896, and 0.890, respectively (Figure 2A). In the internal validation cohort, the AUCs for these time points were 0.883, 0.890, and 0.908, respectively (Figure 2B). For the external validation cohort, the AUCs were 0.854, 0.842, and 0.804, respectively (Figure 2C). Calibration curves indicated that, in the training cohort (Figure S2A–C), internal validation cohort (Figure S2D–F), and external validation cohort (Figure S2G–I), the predicted 1-, 2-, and 3-year OS rates closely matched the actual observed outcomes.
 |
Figure 2 ROC curves for the nomogram. (A–C) AUCs for 1-, 2-, and 3-year OS in training, internal, and external validation cohorts. Abbreviations: RAR, red blood cell distribution width to albumin ratio; AUC, area under curve; OS, overall survival; ROC, receiver operating characteristic. |
Decision Curve Analysis
The decision curve analysis results indicated that the RAR-Nomogram substantially improved the net benefit for predicting 1-year (Figure S3A–C), 2-year (Figure S3D–F), and 3-year (Figure S3G–I) OS across the training, internal validation, and external validation cohorts. They also demonstrated a wide range of threshold probabilities where the nomogram offered considerable clinical utility.
Risk Stratification Analysis
Based on the total risk scores calculated from the RAR-Nomogram, patients with HBV-HCC were stratified into different risk categories: patients with scores above 194.8 were classified as high-risk, those with scores below 128 as low-risk, and those with scores in between as intermediate-risk (Figure S4). In the training cohort, the median survival times for the high-, intermediate-, and low-risk groups were 2 months (95% CI: 1.109–2.891), 11 months (95% CI: 9.141–12.859), and 54 months (95% CI: 38.587–69.413), respectively (Figure 3A). In the internal validation cohort, the median survival times were 3 months (95% CI: 1.899–4.101), 12 months (95% CI: 9.006–14.994), and 62 months (95% CI: 51.101–72.899) for the high-, intermediate-, and low-risk groups, respectively (Figure 3B). Similar trends were observed in the external validation cohort, where the median survival times for high-, intermediate-, and low-risk groups were 2 months (95% CI: 0.326–3.674), 4 months (95% CI: 2.614–5.386), and 51 months (95% CI: 37.488–64.512), respectively (Figure 3C).
 |
Figure 3 Survival analysis for different risk groups. (A–C) Kaplan-Meier curves for risk groups in the training, internal validation, and external validation cohorts. |
Comparing the New Nomogram with Traditional Models
The predictive performance of the RAR-Nomogram was compared with that of three conventional HCC staging systems: BCLC, TNM, and CLIP. The RAR-Nomogram demonstrated superior discriminative ability across the training, internal validation, and external validation cohorts. In the training cohort, the AUCs for 1-, 2-, and 3-year OS for the RAR-Nomogram were 0.881, 0.896, and 0.890, respectively, surpassing those of CLIP (0.843, 0.848, and 0.838, respectively), BCLC (0.840, 0.860, and 0.862, respectively), and TNM (0.796, 0.830, and 0.838, respectively) (Figure 4A–C). Similarly, in the internal validation cohort, the AUCs for 1-, 2-, and 3-year OS for the RAR-Nomogram were 0.883, 0.890, and 0.908, respectively, outperforming CLIP (0.846, 0.840, and 0.849, respectively), BCLC (0.857, 0.857, and 0.862, respectively), and TNM (0.838, 0.821, and 0.843, respectively) (Figure 4D–F). In the external validation cohort, the AUCs for 1-, 2-, and 3-year OS for the RAR-Nomogram were 0.854, 0.842, and 0.804, respectively; again, higher than those of CLIP (0.831, 0.831, and 0.779, respectively), BCLC (0.791, 0.807, and 0.777, respectively), and TNM (0.753, 0.769, and 0.736, respectively) (Figure 4G–I). Table S2 shows time-dependent AUCs and DeLong’s test p-values comparing prognostic models with the nomogram across datasets.
 |
Figure 4 ROC analysis of the nomogram model and the traditional staging system. 1–3 year AUCs: training (A-C), internal validation (D–F), external validation (G–I). Abbreviations: OS, overall survival; ROC, receiver operating characteristic; CLIP, Cancer of the Liver Italian Program; BCLC, Barcelona Clinic Liver Cancer; TNM, tumor node metastasis. |
Constructing a Web-Based Survival Calculator
To make the model more accessible to clinicians, we developed a free, web-based calculator on the Shinyapp.io platform (Figure S5). Clinicians and researchers can access it at https://fmuuhtmq.shinyapps.io/dynnomapp/ to estimate the mortality risk for patients with HBV-HCC. By entering clinical characteristics and reviewing the graphical and tabular outputs from the dynamic nomogram, users can easily determine the predicted survival probabilities for patients over time.
Discussion
In this study, we developed and validated a novel prognostic model, the RAR-Nomogram, for predicting OS in patients with HBV-HCC. By incorporating traditional clinicopathological factors alongside the RAR—a novel biomarker reflecting systemic inflammation—this model significantly improves the predictive accuracy of OS in patients with HBV-HCC.
The RAR combines the RDW, an indicator of red blood cell volume variability, with the ALB level, which reflects liver function and nutritional status. This ratio offers a comprehensive perspective for evaluating the systemic inflammatory status and nutritional condition of patients with HCC. The RAR has been widely applied in the prognostic assessment of various inflammatory diseases, such as non-ischemic heart failure and acute myocardial infarction.20,27 However, its prognostic significance in malignancies remains underexplored. This study is the first to establish RAR as an independent prognostic factor for overall survival in patients with HBV-HCC, demonstrating predictive superiority over traditional indicators such as tumor size and number. These findings highlight the pivotal role of systemic inflammation in the progression of HCC.
The precise mechanisms by which the RAR influences HCC prognosis remain unclear. Several possible explanations are as follows: First, chronic inflammation promotes the development of a tumor microenvironment, and an elevated RAR may indicate a more severe inflammatory state, potentially associated with greater tumor aggressiveness.28,29 Second, low ALB levels reflect impaired liver function and weakened immune function, reducing the effectiveness of the antitumor immune response.30,31 Lastly, an increased RAR may signal heightened oxidative stress, which is strongly linked to HCC development and progression.32,33 These hypotheses provide valuable directions for future research into the molecular mechanisms through which the RAR contributes to HCC progression.
Prior research on inflammatory biomarkers frequently transformed continuous variables into categorical ones, largely because standardized cutoff values were unavailable.34–36 This method introduced variability, which potentially weakened statistical power and may have resulted in erroneous causal interpretations, ultimately reducing their prognostic utility.37,38 In our study, we maintained the LYM count and RAR as continuous variables when constructing the predictive model, thereby improving the reliability of the findings.
The prognostic model developed in this study incorporates not only the RAR but also a range of factors, including liver function (TBIL and Child–Pugh grade), tumor burden (tumor size, number, PVTT, and metastasis), and treatment modalities. This comprehensive, multifactorial approach improves the model’s accuracy and predictive power, outperforming traditional staging systems, such as TNM, BCLC, and CLIP, in three independent cohorts. These results underscore the need for a holistic evaluation of tumor characteristics, liver function, and systemic inflammatory status when assessing HCC prognosis.
Furthermore, the model can act as a crucial instrument for the meticulous stratification of patients, establishing a foundation for personalized treatment strategies. Specifically, this may entail the implementation of more aggressive therapeutic interventions and heightened vigilance for those patients categorized as high-risk. Building on this risk stratification, our model can assist clinicians in tailoring treatment intensity and follow-up schedules according to individual risk profiles. For example, patients identified as high-risk may benefit from intensified treatment regimens and more frequent monitoring, while low-risk patients could avoid overtreatment and its associated adverse effects through more conservative management. Additionally, we have developed an online calculator to facilitate rapid clinical application, supporting more informed decision-making and enhancing patient-physician communication.
However, this study is accompanied by several limitations that warrant acknowledgment. First, as a retrospective analysis, it might have been subject to selection bias. Second, the model was developed specifically for patients with HBV-HCC, and its generalizability to patients with HCC with other etiologies requires further validation. Additionally, key factors such as detailed antiviral therapy information, physical performance status, and dynamic liver function changes were not included due to missing data, which may have limited the comprehensiveness and predictive accuracy of our model. Furthermore, the categorization of treatment modalities into local intervention and systemic therapy groups, though based on clinical rationale, may oversimplify therapeutic heterogeneity; variations in treatment intensity (eg, resection vs TACE) and biological effects (eg, targeted therapy vs chemotherapy) were not fully captured, and sequential treatment strategies were not considered. Finally, the absence of dynamic RAR analysis might have underestimated its full prognostic potential. Future research should focus on large-scale, prospective studies and explore the relationship between dynamic changes in the RAR and HCC prognosis.
In conclusion, we developed and validated an RAR-based nomogram (RAR-Nomogram) to predict survival outcomes in patients with HBV-HCC. This model demonstrated strong predictive accuracy in both the development and validation cohorts, with superior discriminatory ability compared to traditional assessment models. The RAR-Nomogram shows promise as an effective tool for guiding personalized treatment and prognosis in clinical settings.
Abbreviations
HCC, Hepatocellular Carcinoma; HBV, Hepatitis B Virus; OS, Overall Survival; BCLC, Barcelona Clinic Liver Cancer; TNM, Tumor Node Metastasis; CLIP, Cancer of the Liver Italian Program; RDW, Red Blood Cell Distribution Width; ALB, Albumin; RAR, RDW to ALB Ratio; TBIL, Total Bilirubin; LYMs, Lymphocytes; PVTT, Portal Vein Tumor Thrombosis; HR, Hazard Ratio; CI, Confidence Interval; IQR, Interquartile Range; RFA, Radiofrequency ablation; TACE, Transarterial chemoembolization; BSC, Best supportive care.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author.
Ethics Approval and Informed Consent
The study adhered to the tenets of the Declaration of Helsinki and was approved by the Ethics Committees of 900TH Hospital of Joint Logistics Support Force (approval number 2022-014), Fujian Medical University Union Hospital (approval number 2023KY225), and First Affiliated Hospital of Sun Yat-sen University (approval number [2024]241). Informed consent or substitute for it was obtained from all patients for being included in the study.
Acknowledgments
The authors highly appreciate all patients who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Government-funded Project of the Construction of High-level Laboratory (Min201704) provided funding for this work.
Disclosure
The authors have no conflicts of interest for this work.
References
1. Ding J, Wang H. Multiple interactive factors in hepatocarcinogenesis. Cancer Lett. 2014;346(1):17–23. doi:10.1016/j.canlet.2013.12.024
2. Wang M, Wang Y, Feng X, et al. Contribution of hepatitis B virus and hepatitis C virus to liver cancer in China north areas: experience of the Chinese national cancer center. Inter J Infect Dis. 2017;65:15–21. doi:10.1016/j.ijid.2017.09.003
3. Shi J, Zhu L, Liu S, Xie WF. A meta-analysis of case-control studies on the combined effect of hepatitis B and C virus infections in causing hepatocellular carcinoma in China. Br J Cancer. 2005;92(3):607–612. doi:10.1038/sj.bjc.6602333
4. Jemal A, Ward EM, Johnson CJ, et al. Annual report to the nation on the status of cancer, 1975-2014, featuring survival. J Natl Cancer Inst. 2017;109(9). doi:10.1093/jnci/djx030
5. Smirne C, Grossi G, Pinato DJ, et al. Evaluation of the red cell distribution width as a biomarker of early mortality in hepatocellular carcinoma. Dig Liver Dis. 2015;47(6):488–494. doi:10.1016/j.dld.2015.03.011
6. Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19(3):329–338. doi:10.1055/s-2007-1007122
7. Meier V, Ramadori G. Clinical staging of hepatocellular carcinoma. Dig Dis. 2009;27(2):131–141. doi:10.1159/000218345
8. Marrero JA, Kudo M, Bronowicki JP. The challenge of prognosis and staging for hepatocellular carcinoma. oncologist. 2010;15(Suppl 4):23–33. doi:10.1634/theoncologist.2010-S4-23
9. Hsu CY, Hsia CY, Huang YH, et al. Selecting an optimal staging system for hepatocellular carcinoma: comparison of 5 currently used prognostic models. Cancer. 2010;116(12):3006–3014. doi:10.1002/cncr.25044
10. The Cancer of the Liver Italian Program (CLIP) investigators. A new prognostic system for hepatocellular carcinoma: a retrospective study of 435 patients. Hepatology. 1998;28(3):751–755. doi:10.1002/hep.510280322
11. Kudo M, Chung H, Osaki Y. Prognostic staging system for hepatocellular carcinoma (CLIP score): its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score). J Gastroenterol. 2003;38(3):207–215. doi:10.1007/s005350300038
12. Llovet JM, Bruix J. Prospective validation of the Cancer of the Liver Italian Program (CLIP) score: a new prognostic system for patients with cirrhosis and hepatocellular carcinoma. Hepatology. 2000;32(3):679–680. doi:10.1053/jhep.2000.16475
13. The Cancer of the Liver Italian Program (CLIP) Investigators. Prospective validation of the CLIP score: a new prognostic system for patients with cirrhosis and hepatocellular carcinoma. Hepatology. 2000;31(4):840–845. doi:10.1053/he.2000.5628
14. Tan M, Liu B, You R, et al. Red blood cell distribution width as a potential valuable survival predictor in hepatitis B virus-related hepatocellular carcinoma. Int J Med Sci. 2023;20(7):976–984. doi:10.7150/ijms.79619
15. Jeng LB, Chan WL, Teng CF. Prognostic significance of serum albumin level and albumin-based mono- and combination biomarkers in patients with hepatocellular carcinoma. Cancers. 2023;15(4):1005. doi:10.3390/cancers15041005
16. Carr BI, Guerra V. Validation of a liver index and its significance for HCC aggressiveness. J Gastrointest Cancer. 2017;48(3):262–266. doi:10.1007/s12029-017-9971-4
17. Nojiri S, Joh T. Albumin suppresses human hepatocellular carcinoma proliferation and the cell cycle. Int J Mol Sci. 2014;15(3):5163–5174. doi:10.3390/ijms15035163
18. Carr BI, Guerra V. Serum albumin levels in relation to tumor parameters in hepatocellular carcinoma patients. Int J Biol Markers. 2017;32(4):e391–e396. doi:10.5301/ijbm.5000300
19. Fu X, Yang Y, Zhang D. Molecular mechanism of albumin in suppressing invasion and metastasis of hepatocellular carcinoma. Liver Int. 2022;42(3):696–709. doi:10.1111/liv.15115
20. Zhou P, Tian PC, Zhai M, et al. Association between red blood cell distribution width-to-albumin ratio and prognosis in non-ischaemic heart failure. ESC Heart Failure. 2024;11(2):1110–1120. doi:10.1002/ehf2.14628
21. Weng Y, Peng Y, Xu Y, et al. The ratio of red blood cell distribution width to albumin is correlated with all-cause mortality of patients after percutaneous coronary intervention - a retrospective cohort study. Front Cardiovasc Med. 2022;9:869816. doi:10.3389/fcvm.2022.869816
22. Lu C, Long J, Liu H, et al. Red blood cell distribution width-to-albumin ratio is associated with all-cause mortality in cancer patients. J Clin Lab Anal. 2022;36(5):e24423. doi:10.1002/jcla.24423
23. Luo J, Zhu P, Zhou S. Association between the red blood cell distribution width-to-albumin ratio and risk of colorectal and gastric cancers: a cross-sectional study using NHANES 2005-2018. BMC Gastroenterol. 2025;25(1):316. doi:10.1186/s12876-025-03871-6
24. Tan M, You R, Cai D, et al. The red cell distribution width to albumin ratio: a novel prognostic indicator in hepatitis B virus-related hepatocellular carcinoma. Int J Med Sci. 2025;22(2):441–450. doi:10.7150/ijms.103125
25. Yang J, Ding Q, Tian J, Lai P. Technical roadmap towards trustworthy large-scale models in medicine. Innovat Med. 2024;2(1):100058. doi:10.59717/j.xinn-med.2024.100058
26. Feng G, Xu H, Wan S, et al. Twelve practical recommendations for developing and applying clinical predictive models. Innovat Med. 2024;2(4):100105. doi:10.59717/j.xinn-med.2024.100105
27. Ruan L, Xu S, Qin Y, et al. Red blood cell distribution width to albumin ratio for predicting type i cardiorenal syndrome in patients with acute myocardial infarction: a retrospective cohort study. J Inflamm Res. 2024;17:3771–3784. doi:10.2147/jir.S454904
28. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
29. Greten FR, Grivennikov SI. Inflammation and cancer: triggers, mechanisms, and consequences. Immunity. 2019;51(1):27–41. doi:10.1016/j.immuni.2019.06.025
30. Gupta D, Lis CG. Pretreatment serum albumin as a predictor of cancer survival: a systematic review of the epidemiological literature. Nutr J. 2010;9:69. doi:10.1186/1475-2891-9-69
31. Arroyo V, García-Martinez R, Salvatella X. Human serum albumin, systemic inflammation, and cirrhosis. J Hepatol. 2014;61(2):396–407. doi:10.1016/j.jhep.2014.04.012
32. Bishayee A, Politis T, Darvesh AS. Resveratrol in the chemoprevention and treatment of hepatocellular carcinoma. Cancer Treat Rev. 2010;36(1):43–53. doi:10.1016/j.ctrv.2009.10.002
33. Marra M, Sordelli IM, Lombardi A, et al. Molecular targets and oxidative stress biomarkers in hepatocellular carcinoma: an overview. J Transl Med. 2011;9:171. doi:10.1186/1479-5876-9-171
34. Wu Y, Tu C, Shao C. Inflammatory indexes in preoperative blood routine to predict early recurrence of hepatocellular carcinoma after curative hepatectomy. BMC Surgery. 2021;21(1):178. doi:10.1186/s12893-021-01180-9
35. Kim EY, Song KY. The preoperative and the postoperative neutrophil-to-lymphocyte ratios both predict prognosis in gastric cancer patients. World J Surg Oncol. 2020;18(1):293. doi:10.1186/s12957-020-02059-4
36. Sun L, Jin Y, Hu W, et al. The impacts of systemic immune-inflammation index on clinical outcomes in gallbladder carcinoma. Front Oncol. 2020;10:554521. doi:10.3389/fonc.2020.554521
37. Naggara O, Raymond J, Guilbert F, Roy D, Weill A, Altman DG. Analysis by categorizing or dichotomizing continuous variables is inadvisable: an example from the natural history of unruptured aneurysms. AJNR Am J Neuroradiol. 2011;32(3):437–440. doi:10.3174/ajnr.A2425
38. Royston P, Altman DG, Sauerbrei W. Dichotomizing continuous predictors in multiple regression: a bad idea. Stat Med. 2006;25(1):127–141. doi:10.1002/sim.2331
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Histological Severity of Cirrhosis Influences Surgical Outcomes of Hepatocellular Carcinoma After Curative Hepatectomy
Liang BY, Gu J, Xiong M, Zhang EL, Zhang ZY, Lau WY, Wang SF, Guan Y, Chen XP, Huang ZY
Journal of Hepatocellular Carcinoma 2022, 9:633-647
Published Date: 23 July 2022
Red Blood Cell Distribution Width as Novel Biomarker in Cardiovascular Diseases: A Literature Review
Arkew M, Gemechu K, Haile K, Asmerom H
Journal of Blood Medicine 2022, 13:413-424
Published Date: 2 August 2022
Association Between Red Blood Cell Distribution Width–Albumin Ratio and Hospital Mortality in Chronic Obstructive Pulmonary Disease Patients Admitted to the Intensive Care Unit: A Retrospective Study

Qiu Y, Wang Y, Shen N, Wang Q, Chai L, Liu J, Chen Y, Li M
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1797-1809
Published Date: 10 August 2022
Albumin Infusion May Improve the Prognosis of Critical COVID-19 Patients with Hypoalbuminemia in the Intensive Care Unit: A Retrospective Cohort Study
Zhang L, Yu W, Zhao Y, Chen X, Wang P, Fan X, Xu Z
Infection and Drug Resistance 2022, 15:6039-6050
Published Date: 19 October 2022
Diagnostic Value of RDW-Albumin Ratio for the Prediction of Mortality in Sepsis Associated Nonthyroidal Illness Syndrome Patients: A Retrospective Cohort Study
Zhang J, Xu P, Huang Y, Li J, Ma C, Liu G, Ye J, Guo Y, Feng Z, Jiang B, Pan S, Gao C
Journal of Inflammation Research 2024, 17:11305-11318
Published Date: 20 December 2024