")
Back to Journals » Risk Management and Healthcare Policy » Volume 18
Rational Analysis of the Utilization of Pentoxifylline in a Tertiary Hospital: Central Hospital Affiliated to Shandong First Medical University
Authors Zheng Y, Yin Y, Liu H, Gao W, Wang Q
Received 21 February 2025
Accepted for publication 23 June 2025
Published 9 July 2025 Volume 2025:18 Pages 2335—2350
DOI https://doi.org/10.2147/RMHP.S517679
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Yuanyuan Zheng,1,2,* Yanhui Yin,1,* Hong Liu,3 Wenwen Gao,1 Qian Wang1
1Department of Pharmacy, Central Hospital Affiliated to Shandong First Medical University, Jinan, 250013, People’s Republic of China; 2The First Affiliated Hospital of Shandong First Medical University, Jinan, 250014, People’s Republic of China; 3Department of Pharmacy, Laiwu District People’s Hospital, Jinan, 271100, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qian Wang, Department of Pharmacy, Central Hospital Affiliated to Shandong First Medical University, No. 105 Jiefang Road, Lixia District, Jinan City, Shandong Province, 252213, People’s Republic of China, Email [email protected]
Objective: This study aimed to evaluate the rational use, safety, and economic implications of pentoxifylline in a hospital setting and provide recommendations for its appropriate clinical application.
Methods: A retrospective analysis was conducted on 322 patients discharged from September to December 2020, who received pentoxifylline. Data were collected from the hospital information system, and the rationality of prescriptions was assessed based on drug instructions and guidelines. Adverse drug reactions (ADRs) were analyzed using CTCAE criteria. Economic evaluations included defined daily dose cost (DDDc) and incremental cost-effectiveness ratio (ICER) analyses.
Results: The rational prescription rate for pentoxifylline was 38.51%, with the main irrationalities observed in indications (31.82%), dosage and usage (21.21%), contraindications (47.98%), and drug combinations (40.40%). Adverse reactions were reported in 12 cases (3.73%), primarily involving the nervous (75.00%) and digestive systems (41.67%). Most ADRs were mild (58.33%) or moderate (41.67%), with no severe cases observed. The DDDc of pentoxifylline was 143.4 yuan. Cost-effectiveness analysis demonstrated strong economic viability, with ICER values of 55.7 yuan per percentage point improvement in ulcer healing rate and 9.0 yuan per additional meter of pain-free walking distance, significantly below the willingness-to-pay threshold.
Conclusion: Pentoxifylline demonstrates cost-effectiveness and manageable safety risks but has a low rational prescription rate, highlighting the need for improved clinical practices. Enhanced collaboration between pharmacists and medical staff, alongside stricter adherence to guidelines, is essential to optimizing its utilization.
Keywords: pentoxifylline, special evaluation, adverse drug reactions, defined daily dose consumption, rational use
Introduction
Pentoxifylline (PTX), a methylxanthine derivative and phosphodiesterase inhibitor, improves microcirculation by enhancing erythrocyte deformability, reducing blood viscosity, and promoting fibrinolysis, thereby optimizing tissue perfusion.1,2 Initially approved for intermittent claudication in the United States, PTX is now widely used in China for peripheral vascular diseases, cerebral/ocular/ear circulatory disorders, and diabetic microangiopathy.3,4 Beyond its vasodilatory effects, emerging preclinical studies highlight its anti-inflammatory, antifibrotic, and immunomodulatory properties. Recent research demonstrates PTX’s efficacy in attenuating hepatic fibrosis via inhibition of TGF-β1 signaling,5 ameliorating type 2 diabetes and chronic kidney disease,6 and reducing neuroinflammation in Alzheimer’s disease models.7 These findings underscore its potential for repurposing in diverse conditions.
Despite its therapeutic promise, PTX’s safety profile warrants scrutiny. Common adverse reactions include dizziness, gastrointestinal disturbances, and hypotension, while severe events like thrombocytopenia and anaphylaxis are rare but critical.8 Concurrently, economic evaluations remain sparse despite growing emphasis on cost-effective therapies under China’s evolving healthcare policies.
This study retrospectively analyzed 322 inpatients receiving PTX at a tertiary hospital in Jinan, China, to (1) assess prescription rationality based on indications, dosage, contraindications, and drug interactions; (2) evaluate safety through adverse reaction monitoring; and (3) conduct cost-effectiveness analyses comparing PTX to standard therapies. Our objective is to propose evidence-based recommendations for the rational use of PTX, optimizing its clinical deployment while minimizing risks and costs.
Data and Methods
Data
The data came from the Hospital Information System (Xinyi) of a hospital in Jinan City. The study analyzed data from September to December 2020 to capture a representative sample of PTX utilization prior to significant shifts in clinical practices post-COVID-19. This period was selected to ensure data completeness and minimize confounding factors related to pandemic-driven treatment modifications. This study was conducted at a municipal tertiary Grade A general hospital (Central Hospital Affiliated to Shandong First Medical University). At the time of data extraction (2020), the hospital had 1,780 open beds. Following the opening of a new campus in 2022, the current bed capacity increased to 2,585. The medical records of all discharged patients treated with PTX from September 1, 2020 to December 31, 2020, were collected through the system, excluding patients who did not use PTX. A retrospective study was carried out and Microsoft Excel v.2016 was used to collect data such as patient information, drug use information, and adverse reactions. The PTX special comment table was designed according to the instructions for PTX, Beijing Guidelines for Special Comments on Prescriptions for Medical Institutions, Norms for the Management of Hospital Prescription Comments (Trial), and Prescription Management Measures (see in Tables S1–S5).
PTX injection used in the hospital is purchased from Guangzhou Wanzheng Pharmaceutical Co., LTD., with a concentration of 0.02g/mL.
Evaluation Criteria
The content of the review includes indications, usage and dosage, contraindications, drug combination, rational comments on drug use, and drug related adverse reactions. The evaluation criteria are formulated by the specification and the 18th edition of New Pharmacology.9 Prescription rationality was assessed by a multidisciplinary team of clinical pharmacists specializing in relevant therapeutic areas (eg, endocrinology, neurology). Initial evaluations utilized a standardized template aligned with drug labeling and guideline criteria. Discrepancies were resolved through iterative consensus discussions, with final validation by senior pharmacists (associate chief rank or higher) to ensure methodological rigor.
Indication
Based on the drug instructions and guidelines, the indications for PTX that can be assessed as reasonable are listed in Table 1. If PTX was applied without the indications listed in Table 1, it is evaluated as no prescription drug.
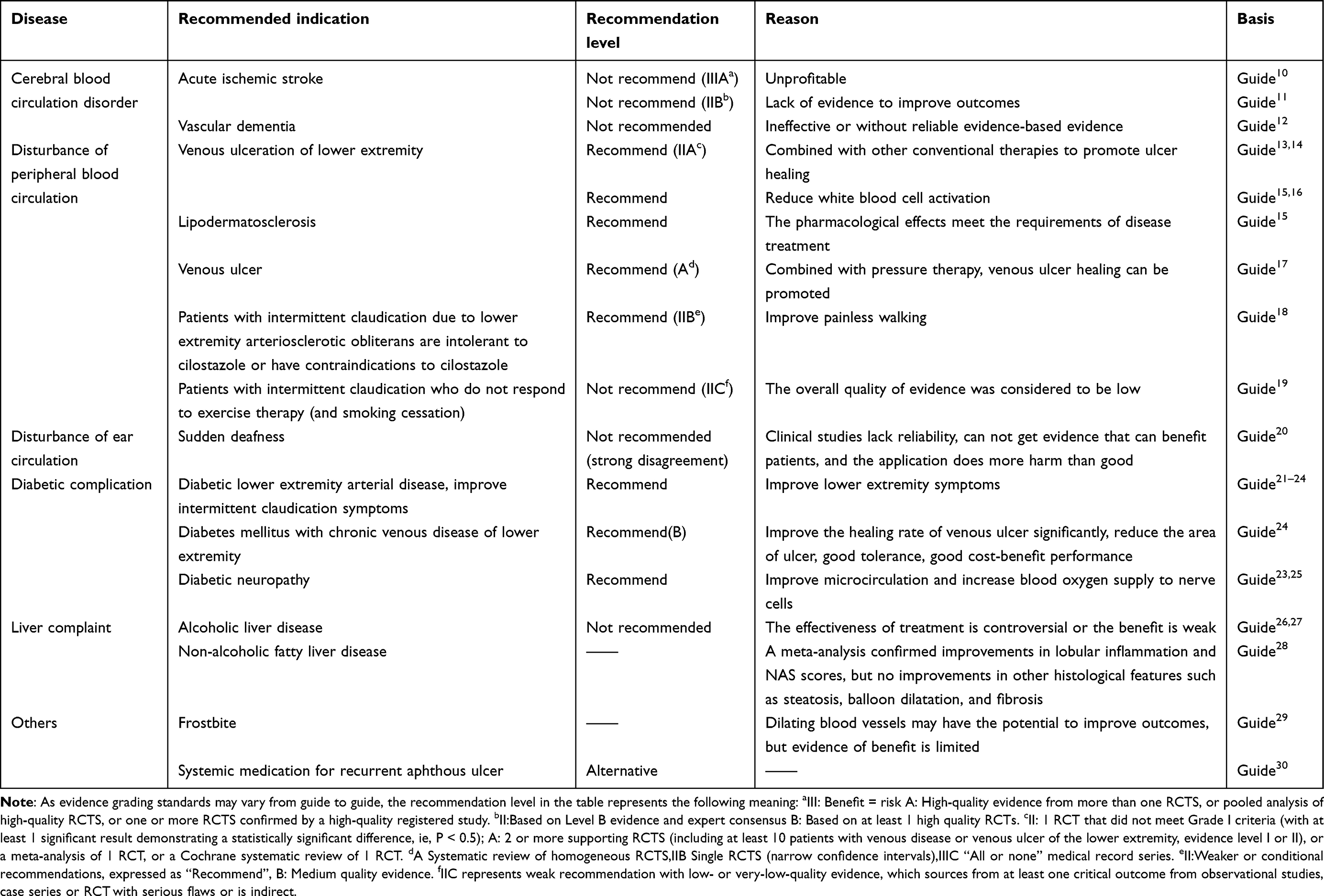 |
Table 1 Guidelines-Recommended Indications for Pentoxifylline |
Usage and Dosage
The usage and dosage of PTX is based on the drug instructions:
PTX can be compatible with 0.9% sodium chloride injection or 5% glucose injection. The drug was administered by intravenous drip for 2–3 hours. The maximum drop rate does not exceed 100mg/h. The initial dose is 100mg, which can be increased by 50mg each time according to patient tolerance, but the dosage should not exceed 200mg each time. Patients can take the drug 1–2 times a day, and the maximum dose should not exceed 400mg/24h. A course of treatment of at least 8 weeks is recommended.
Contraindication
The contraindications of PTX were evaluated according to Table 2. If a patient has a contraindicated evaluation item, PTX is still used, then it should be evaluated as contraindicated. For patients with prudent use, dose adjustment, or evaluation items requiring monitoring, statistical analysis should also be carried out based on their medical history information.
 |
Table 2 The Evaluative Principle of Contraindications of Pentoxifylline |
Drug Combination
According to Table 3, the rationality of drug combination in patients with PTX was evaluated. PTX and ketochromic acid should not be used together. When PTX is combined with other drugs listed in Table 3, corresponding measures, such as dose adjustment and monitoring, should be taken. Otherwise, the combination of drugs will be evaluated as inappropriate.
 |
Table 3 The Evaluative Principle of Drug-Drug Interactions of Pentoxifylline |
Safety Analysis
Adverse reaction information was collected through the hospital information system, including but not limited to clinical records, nursing records, laboratory test results, and patient-reported symptoms; for symptoms reported by patients, the research team assessed the causality between the symptoms and PTX use based on the drug package insert and relevant literature. In this study, adverse drug reactions (ADRs) were defined as any undesirable symptoms or signs occurring during the use of PTX that were related to the drug, including but not limited to nervous system reactions (eg, dizziness, head distension), gastrointestinal reactions (eg, nausea, vomiting), and abnormalities in other organ systems. The classification of adverse reactions was performed according to the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0,31 which categorizes adverse reactions into the following five grades: (1) Grade 1 (Mild): Asymptomatic or mild symptoms that do not require medical intervention and do not affect daily activities; (2) Grade 2 (Moderate): Requiring non-urgent medical intervention, without life-threatening consequences, but may limit daily activities; (3) Grade 3 (Severe): Significantly limiting daily activities and requiring urgent medical intervention; (4) Grade 4 (Life-threatening): Poses an immediate threat to life, requiring emergency medical intervention or resuscitation; (5) Grade 5 (Fatal): Results in the death of the patient.
Economical Analysis
Defined Daily Dose (DDD) Analysis
By using the Defined daily dose (DDD) analysis method, the total consumption sum of PTX injection was calculated, and the frequency of medication (DDDs) and daily cost (DDDc) were calculated. DDD is the average daily maintenance dose for adults used for primary therapeutic purposes and is a unit of measurement rather than the actual dose administered.32 The DDD value of PTX administered by the WHO designated parenteral route was 0.3g.
DDDs= Total consumption of pentothemine/DDD value of pentoxifylline;
DDDc= Total sales amount of pentothemine/DDDs value of pentoxifylline.
The value of DDDc can reflect the economy of PTX to a certain extent, the smaller the value, the better the economy of the drug.33,34
Cost-Effectiveness Analysis (CEA)
A cost-effectiveness analysis (CEA) was conducted to further evaluate the economic value of PTX. This approach compares the additional costs incurred with PTX to the additional clinical benefits achieved, using the incremental cost-effectiveness ratio (ICER). The ICER is calculated as: ICER = ΔC/ΔE. ΔC is the difference in costs between PTX treatment and the comparator (eg, standard therapy or no treatment), and ΔE is the difference in clinical effectiveness, such as ulcer healing rate or improvement in pain-free walking distance. To evaluate the incremental cost-effectiveness of PTX, a control group (n = 300) was included for comparison. The control group received standard therapies for the same indications: cilostazol (100 mg twice daily) for peripheral vascular diseases and comprehensive wound care (debridement, infection control, and moisture balance) for diabetic complications. Cost data for both groups were collected from hospital records, including drug costs, hospitalization expenses, and auxiliary service fees. Clinical effectiveness was measured by ulcer healing rate (%) for diabetic complications and pain-free walking distance (meters) for peripheral vascular diseases, as these indicators are commonly used in studies evaluating the efficacy of PTX for these conditions.35 The ICER was calculated by comparing the additional costs and clinical benefits of PTX with those of the control group. Sensitivity analysis was conducted to evaluate the robustness of the results under different assumptions, including a ±10% variation in drug prices and a ±20% variation in clinical effectiveness. The willingness-to-pay (WTP) threshold of three times the per capita GDP used in this study is a globally recognized standard recommended by the WHO.36 For China, the per capita GDP in 2023 was approximately 80,000 yuan, making the WTP threshold 240,000 yuan per quality-adjusted life year (QALY) or equivalent.37 This standard has been widely applied in health economics studies to evaluate the cost-effectiveness of interventions. This threshold provides a benchmark to determine whether PTX is a cost-effective intervention compared to standard care.
Statistic Analysis
GraphPad v.10 software was used for statistical analysis, and statistical charts were generated for descriptive statistics. Economic analyses were conducted using Microsoft Excel and TreeAge Pro software for data modeling and analysis. Continuous variables, such as hospitalization costs, were expressed as mean ± standard deviation (SD). Categorical variables, such as ulcer healing rate, were summarized as frequencies and percentages. Due to the observational nature of this study without a parallel control group, formal inferential statistical comparisons (eg, t-tests or chi-square tests) were not performed. Economic analyses utilized descriptive comparisons and sensitivity modeling. ICER results were presented using curves and charts, while sensitivity analysis results were visualized with Tornado diagrams to illustrate the impact of different parameters on ICER variation.
Result
Baselines
A total of 322 patients were included in the study (Table 4). The mean age was 65.2 ± 12.3 years (range: 42–89 years), with 190 men (59.0%) and 132 women (41.0%). Among the included cases, 95% were middle-aged and elderly patients over 40 years old, and 66.2% were elderly patients over 60 years old (Figure 1). The most common diagnoses were cerebral circulatory disorders (44.7%, 144/322), diabetic complications (22.7%, 73/322), and peripheral vascular diseases (19.3%, 62/322). A total of 198 cases (61.5%) were classified as having irrational prescriptions, resulting in a rational prescription rate of 38.5%.
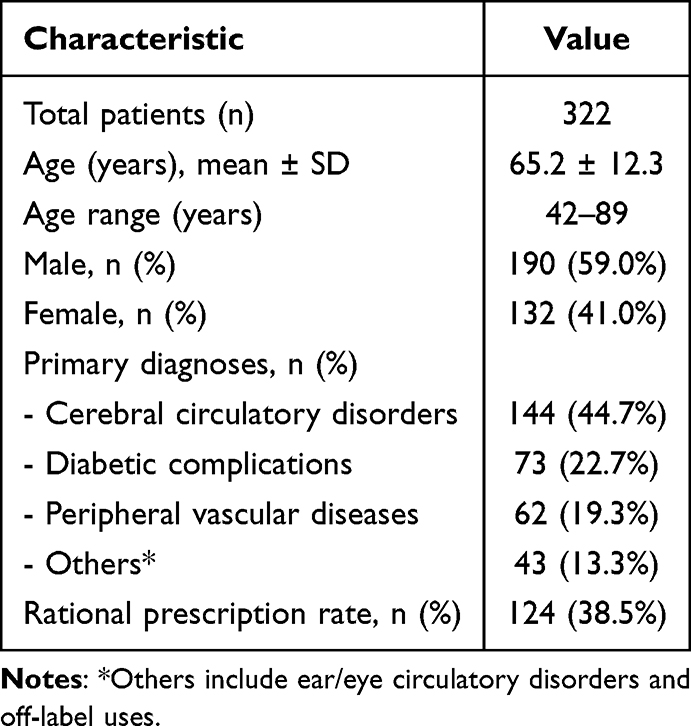 |
Table 4 Baseline Characteristics of Patients Receiving Pentoxifylline |
 |
Figure 1 Age distribution of patients who used pentoxifylline. |
Distribution of Medication Departments
The distribution of departments using PTX is shown in Figure 2. Among them, health care department (29.50%), neurology department (26.40%), endocrinology department (18.01%), vascular surgery department (17.70%) were the main departments using PTX. Although there were fewer cases of PTX used in the departments of surgery, gastroenterology, nephrology, and rheumatology, the rate of irrational prescription (100%) was relatively high (Table 5).
 |
Table 5 Unreasonable Prescription in Different Clinical Departments |
 |
Figure 2 The use of PTX in different clinical departments. |
Table 5 describes the situation of irrational drug use in different departments. The main reason for irrational drug use in the health care profession and neurology department is inappropriate contraindicated population and combined drug use. Endocrinology is mainly used for contraindicated population, inappropriate combination of drugs and drugs without indications. Vascular surgery is mainly used for non-indications and contraindicated people. In other departments with low dosage of PTX, the proportion of irrational prescription was relatively high due to the unindicated use and inappropriate usage.
Reasons for Unreasonable Prescription
The main problems of irrational prescription included: no indication of drug use (31.82%), inappropriate usage and dosage (21.21%), conjunctive population use (47.98%), and inappropriate combination of drug use (40.40%) (Table 5).
Indication Evaluation
A total of 259 cases (80.43% of the total cases) were clinically diagnosed in accordance with the application of pentoketothemine, including cerebral blood circulation disorders, diabetes complications and peripheral blood circulation disorders. Among them, the number of cerebral blood circulation disorders was the largest (144 cases), accounting for 44.72% of the total cases.
Evaluation of Usage and Dosage
A total of 280 cases (86.96% of the total cases) were reasonably evaluated in terms of usage and dosage. The unreasonable usage and dosage were all due to the dose not conforming to the recommended dose in the manual (“initial dose of 100mg”), and the dosage in one case exceeded the maximum dosage each time (“the dosage should not exceed 200mg each time”). The solvent of PTX was 250mL normal saline, intravenous infusion, and administered once a day. Only 33 cases (10.25%) had the infusion time noted by doctors when issuing medical orders, 30 cases had the remarks of more than 1.5 hours, and only 1 case had the remarks of 2–3 hours. The vast majority of cases with documented infusion time were from the endocrinology department (93.94%).
Taboo Population Evaluation
There were 227 cases (70.50% of total cases) with reasonable evaluation of drug use in contraindicated population. The contraindications included recent bleeding (5.59% of the total cases) and coronary arteriosclerosis with hypertension (25.40% of the total cases). A total of 63 patients were operated recently, all of whom were monitored for bleeding risk. A total of 9 patients were evaluated as renal dysfunction, and dose reduction measures should be taken, which was evaluated in the column of usage and dosage, and there were 2 unreasonable cases (accounting for 0.62% of the total cases).
Evaluation of Drug Combination
There were 242 cases (75.16% of total cases) with reasonable evaluation of combined drug use. The combined use of PTX included in the study mainly included hypoglycemic agents, aspirin, and dihydroxyproprofylline (1 case). The unreasonable combination of drugs was due to the failure to monitor the coagulation time of aspirin. Blood glucose was routinely monitored in patients treated with hypoglycemic drugs.
Safety Analysis
In this study, among the 322 patients, a total of 12 cases (3.73%) experienced PTX-related adverse reactions, primarily involving the nervous system (9 cases, 75.00%) and the digestive system (5 cases, 41.67%) (Percentages exceed 100% as some patients experienced adverse reactions in multiple systems). According to the CTCAE grading criteria, Grade 1 (mild) adverse reactions accounted for 7 cases (58.33%), mainly presenting as mild dizziness (4 cases) and slight nausea (3 cases), which resolved spontaneously without special treatment. Grade 2 (moderate) reactions accounted for 5 cases (41.67%), including significant head distension with nausea (3 cases) and transient hypotension (2 cases). These symptoms subsided after symptomatic treatment without the need to discontinue the drug. No Grade 3 or more severe adverse reactions were observed. Analysis revealed that the incidence of adverse reactions among patients aged 60 years and older (4.17%) was higher than the overall rate (3.73%). All adverse reactions occurred in patients receiving doses ≤200 mg per administration, and the incidence was higher in cases where the infusion time was not clearly recorded. Among all adverse reaction cases, 50% achieved complete symptom resolution after drug discontinuation or dose adjustment, 33.33% improved with symptomatic treatment, and the remaining 16.67% had no recorded management measures, with symptoms possibly resolving spontaneously. This study did not observe any severe or long-term adverse reactions, nor were there any fatal events (Table 6).
 |
Table 6 Adverse Reactions/Adverse Events Associated with PTX |
Among the 12 patients with adverse reactions, 7 cases (58.33%) were associated with irrational prescriptions, including 2 cases without indications, 2 cases with inappropriate dosage, 2 cases involving contraindicated populations, and 4 cases with improper drug combinations. Notably, 3 cases exhibited multiple irrational factors. 7 cases (58.33%) were older than 60 years old, and 5 cases (41.67%) were aged between 50 and 60 years old (Table 7). There were 6 cases (50%) with cerebral blood circulation disorder and 2 cases (16.67%) with no indication. Infusion time was noted in only 1 case (8.33%). Adverse reactions/adverse events occurred in 4.17% of patients with cerebral circulatory disorders. Table 8 summarizes the factors associated with the occurrence of PTX ADR/ADE.
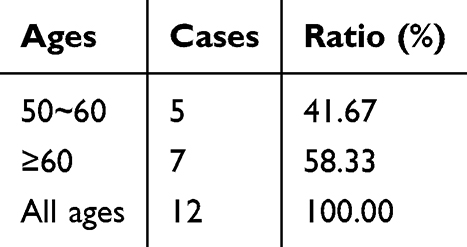 |
Table 7 Age Distribution of Patients with ADR/ADE |
 |
Table 8 Factors Affecting the Occurrence of ADR/ADE |
Defined Daily Dose (DDD) Analysis
In this study, the total consumption of PTX was 297.6 g, and the total consumption amount of PTX was 142252.8 yuan.
DDDs=992
DDDc=143.4 yuan
Cost-Effectiveness Analysis (CEA)
The cost-effectiveness analysis compared PTX treatment (n = 322) to a control group receiving standard therapy (n = 300), with costs and clinical outcomes assessed across both groups. Among irrational prescriptions, PTX injection (manufacturer: Guangzhou Wanzheng Pharmaceutical Co., Ltd., specification: 5mL: 0.1g/vial, unit price: ¥47.8) was administered in 1,790 vials, totaling ¥85,562 (60.2% of total drug costs). This highlights the significant economic impact of irrational prescriptions.
For diabetic complications, PTX achieved an ulcer healing rate of 74.6% versus 66.3% with standard wound care (ΔE = 8.3%). The additional cost (ΔC) of PTX therapy was 462.5 yuan per patient, resulting in an ICER of 55.7 yuan per percentage point improvement in ulcer healing rate. This value is well below the willingness-to-pay (WTP) threshold, defined as three times the per capita GDP (750 yuan per percentage point) (Figure 3).
 |
Figure 3 Comparison of costs and clinical effectiveness between pentoxifylline and standard therapy. (A) illustrates the average treatment costs (Yuan) for the Pentoxifylline group and the Control group, with error bars representing the standard error. (B) demonstrates the clinical effectiveness comparison between the two groups, including ulcer healing rates (%) and pain-free walking distances (meters). Incremental cost-effectiveness ratios (ICER) are annotated above the bars, indicating 55.7 Yuan per percentage point improvement in healing rate and 9.0 Yuan per additional meter of pain-free walking distance for Pentoxifylline. |
For peripheral vascular diseases, pain-free walking distance increased by 54.8 meters by PTX compared to cilostazol therapy, with an additional cost (ΔC) of 495.3 yuan per patient. The ICER for this outcome was calculated to be 9.0 yuan per additional meter of pain-free walking distance. This result is also below the WTP threshold, indicating that PTX is a cost-effective intervention for this condition.
Sensitivity analysis confirmed the robustness of these results. A ±10% variation in drug prices resulted in ICER fluctuations of ±5.6 yuan per percentage point improvement for diabetic complications and ±1.2 yuan per meter for peripheral vascular diseases. Similarly, a ±20% change in clinical effectiveness led to proportional ICER variations, with no significant deviation from the cost-effectiveness threshold (Figure 4).
 |
Figure 4 Tornado chart of sensitivity analysis for pentoxifylline cost-effectiveness. This Tornado Chart illustrates the sensitivity analysis of incremental cost-effectiveness ratios (ICERs) for pentoxifylline compared to standard therapy in diabetic complications and peripheral vascular diseases. The ICER for ulcer healing rate is 55.7 yuan per percentage point improvement, and for pain-free walking distance, it is 9.0 yuan per additional meter, both significantly below the willingness-to-pay (WTP) threshold of 750 yuan. Sensitivity analysis shows that a ±10% change in drug price leads to ICER variations of ±5.6 yuan per percentage point for healing rate and ±1.2 yuan per meter for walking distance, while a ±20% change in clinical effectiveness results in proportional ICER fluctuations. Orange bars represent healing rate ICERs, green bars represent walking distance ICERs, and dashed lines indicate base ICER values. The analysis confirms pentoxifylline’s cost-effectiveness across tested scenarios, ensuring robustness in both economic and clinical contexts. |
Discussion
PTX is mainly used in middle-aged and elderly patients, especially those over 60 years old. In this study, more than half of the patients with adverse reactions were older than 60 years old. This suggests that the elderly use PTX risk is greater, we must be vigilant. While departmental utilization patterns broadly align with labeled indications, the high proportion of contraindication violations in primary prescribing departments (eg, neurology and vascular surgery) highlights systemic gaps in risk assessment prior to prescription. The distribution of irrational drug use in different departments is different, which may be related to different drug use habits in different departments. In the main departments of drug use, there was a high proportion of contraindicated people, suggesting that the contraindications of PTX need to be improved. In other departments with less PTX, it is necessary to improve the understanding of the indication and usage of PTX. In addition, the irrational rate of prescription was also different in the main departments, which may be related to the difference in the degree of attention paid to the rational use of PTX in different departments.
Besides, an important feature of elderly patients is often combined with a variety of underlying diseases, taking a variety of drugs. Therefore, special attention should be paid to whether the patient has contraindications for the use of PTX and whether the combination of drug and PTX interact. Common concomitant medications for PTX patients are hypoglycemic agents, anticoagulants (most commonly aspirin), and theophyllines. The reason for the unreasonable combination of medication in the cases included in this study was that the clotting time was not monitored while aspirin was combined. This may be because in clinical practice, in addition to drug considerations, monitoring may also take into account other factors such as the patient’s disease status, patient’s economic conditions or patient’s demands.
PTX exhibits multifaceted pharmacological activities beyond its classical vasodilatory effects. Notably, it demonstrates antioxidant properties by scavenging free radicals and suppressing lipid peroxidation, as demonstrated in models of diabetic nephropathy.38 Additionally, PTX exerts potent antifibrotic effects through inhibition of the TGF-β1/Smad signaling pathway, which has been validated in hepatic and renal fibrosis studies.39 New animal experimental evidence further suggests that regulating T cell infiltration and nuclear factor kappa B (NF - κ B) signaling has anti-tumor potential, although clinical applications in oncology are still in the research stage.40
Despite this broad therapeutic potential, our study identified systemic challenges in clinical utilization. Contraindication violations, such as administration in patients with coronary arteriosclerosis complicated by hypertension, and inappropriate dosing practices, particularly the omission of dose titration starting from 100 mg were prevalent in high-prescribing departments including neurology and vascular surgery. These issues may stem from insufficient awareness of PTX’s pharmacokinetic profile. For instance, its rapid renal excretion necessitates strict adherence to infusion protocols (2–3 hours per dose) to prevent nephrotoxicity caused by transient drug accumulation.41,42 Furthermore, PTX’s vasoactive properties necessitate cautious administration in elderly patients, who are prone to hemodynamic instability due to age-related cardiovascular changes.43 A critical concern identified was the concurrent use of PTX with anticoagulants such as aspirin without routine coagulation monitoring, which may elevate bleeding risks. This practice highlights the need for systematic screening of drug interactions, particularly in polymedicated elderly populations with multiple comorbidities.
The predominance of mild-to-moderate neurogastrointestinal adverse reactions (eg, dizziness, nausea) aligns with PTX’s known pharmacodynamic effects on phosphodiesterase inhibition and vasodilation.8 Proactive monitoring of infusion speed and concomitant medications may further reduce this burden. Elderly patients (≥60 years old) exhibited a higher incidence of adverse reactions compared to the overall rate, highlighting the need for caution when using PTX in this population. Additionally, all adverse reactions occurred in patients receiving doses ≤200 mg per administration, and cases with unclear infusion times had a higher incidence of reactions, suggesting that infusion speed may contribute to safety concerns.
The mechanism of adverse reactions caused by PTX includes immune mechanism44–51 and direct injury.52–56 Drug rash and anaphylactic shock are usually thought to be caused by immune mechanisms. Gonzalez et al48 suggested that the mechanism of PTX causing urticaria might be related to IgE. In patients with mixed connective tissue disease or systemic lupus erythematosus, PTX has a potential risk of causing aseptic meningitis, and the mechanism of action may be related to the inhibitory effect of PTX on pro-inflammatory cytokines such as TNF-α, while the underlying disease state also plays an important role in the occurrence of adverse reactions.47 Because pentoxifylline-induced thrombocytopenia appeared less than 5 days after treatment, Tan et al56 suggested that this response might be related to the presence of antibodies. In addition, PTX may have cross-allergic reactions with caffeine or other methylxanthines, and should be avoided in patients with a history of allergy to these drugs. Saez et al53 suggested that since the patient did not show any signs of allergic reaction, one case of acute liver injury caused by PTX should be a direct injury. For gastrointestinal bleeding caused by PTX, Oren et al suggested that PTX may act as a catalyst, and the possible mechanism is to interfere with the clotting mechanism by inhibiting the activity of phospholipase C and reducing the action of arachidonic acid.52 PTX adverse reactions/adverse events reported in the literature involved multiple organs or systems, and a large number of severe adverse reactions/adverse events were reported. The results of the literature review suggest that more attention should be paid to the risks of PTX when it is used, especially in elderly patients. For patients with specific disease states, such as mixed connective tissue disease or systemic arthritis, the use of this drug should be avoided as much as possible. Patients who are allergic to caffeine or other methylxanthines should also avoid using this drug. In addition, try to avoid some drugs that may interact with each other, such as theophylline or clopidogrel, if necessary, must strengthen monitoring. Due to the risk of thrombocytopenia associated with PTX, Acharya et al54 suggest that blood monitoring is also necessary when PTX is applied.
While PTX demonstrated cost-effectiveness within our institutional context, broader validation across diverse healthcare settings is needed to generalize these findings, particularly given potential deviations from WHO-recommended DDD benchmarks.36 The reimbursement ratio for PTX is 80% for residents’ medical care and 95% for employees’ medical care. Reducing the irrational use of PTX is of great significance for controlling drug costs. This study also provided a comprehensive CEA of PTX for diabetic complications and peripheral vascular diseases, comparing its costs and clinical outcomes to those of a standard therapy control group (cilostazol [100 mg twice daily] for peripheral vascular diseases and comprehensive wound care [debridement, infection control, and moisture balance] for diabetic complications). The results showed that PTX achieved significant clinical benefits at a reasonable incremental cost, with ICER values well below the WTP threshold defined as three times the per capita GDP (750 yuan [approximately $108.7] per unit of improvement). For diabetic complications, the ICER for ulcer healing rate was 55.7 yuan (approximately $8.07) per percentage point improvement, and for peripheral vascular diseases, the ICER for pain-free walking distance was 9.0 yuan (approximately $1.30) per additional meter, indicating strong cost-effectiveness in both indications.
Sensitivity analysis further confirmed the robustness of these findings. A ±10% variation in drug prices led to ICER fluctuations of ±5.6 yuan (approximately ±$0.81) per percentage point improvement for ulcer healing rate and ±1.2 yuan (approximately ±$0.17) per meter for pain-free walking distance. Similarly, a ±20% change in clinical effectiveness resulted in proportional ICER changes, with all values remaining well below the WTP threshold. These results emphasize the economic viability of PTX under varying cost and clinical outcome scenarios. Overall, PTX demonstrated strong cost-effectiveness for both diabetic complications and peripheral vascular diseases. The ICER values were consistently below the WHO-recommended WTP threshold, highlighting PTX as an economically viable option that provides meaningful clinical benefits at a reasonable incremental cost. Suggestions for rational use of PTX are shown in Table 9.
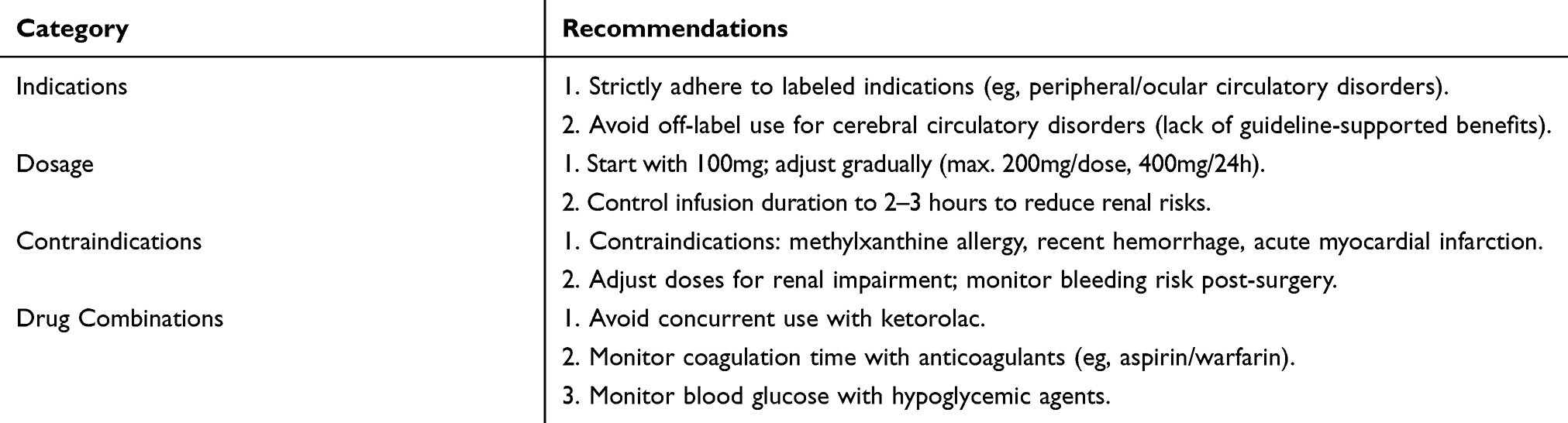 |
Table 9 Recommendations for Optimizing Pentoxifylline Prescriptions |
Globally, the utilization patterns and economic implications of PTX exhibit variability across different clinical contexts. A cost-saving analysis in chronic occlusive arterial disease (COAD) demonstrated that PTX therapy reduced annual hospitalization costs by $1,173 per patient, with overall savings of $965 when accounting for outpatient care and medications, aligning with our findings on PTX’s cost-effectiveness in peripheral vascular diseases.57 However, conflicting evidence emerges in peripheral artery disease (PAD)-related intermittent claudication: while our study reported an ICER of 9.0 yuan per additional meter of pain-free walking distance, a UK-based Markov model analysis ranked PTX as less cost-effective compared to naftidrofuryl oxalate, which showed superior efficacy in improving maximal walking distance.58 This discrepancy may stem from differences in healthcare pricing structures or outcome measurement protocols.
Notably, PTX’s role in ulcer management presents consistent benefits. Our results indicated a 74.6% ulcer healing rate with PTX, corroborated by a randomized controlled trial where PTX as an adjunct to compression therapy significantly enhanced healing rates in venous leg ulcers.59 Conversely, in alcoholic hepatitis, the STOPAH trial revealed PTX’s inferior cost-effectiveness versus prednisolone despite lower initial costs, contrasting with our economically favorable ICERs.60,61 These cross-population comparisons underscore PTX’s context-dependent value, while economically viable for diabetic ulcers and peripheral vascular conditions in our cohort, its utility diminishes in indications like alcoholic hepatitis or when benchmarked against alternative PAD therapies.
This study had some limitations. Although a control group was included for comparison, the data were derived from a single tertiary hospital in Jinan City, which may limit the generalizability of the findings. Additionally, while the study evaluated key clinical outcomes such as ulcer healing rate and pain-free walking distance, other potentially relevant outcomes (eg, quality of life or long-term cardiovascular events) were not assessed. Moreover, the reimbursement rates for PTX highlight its affordability, but the potential for overuse warrants further exploration to ensure rational drug utilization.
Future research should aim to include multicenter data, a broader range of comparative drugs, and additional outcome measures to provide a more comprehensive evaluation of PTX’s economic impact. Despite these limitations, the findings of this study support PTX as a cost-effective option for treating diabetic complications and peripheral vascular diseases, offering meaningful clinical benefits at a manageable incremental cost.
Conclusion
This study highlights critical gaps in PTX utilization at our tertiary hospital, including off-label use, inappropriate dosing, contraindication violations, and unsafe drug combinations. Despite a low adverse reaction rate, vigilance is warranted, particularly in elderly patients. Economic analyses confirmed PTX’s cost-effectiveness for diabetic ulcers and peripheral vascular diseases, yet irrational prescriptions incurred unnecessary costs. To optimize outcomes, we recommend strict adherence to guidelines, pharmacist-clinician collaboration, and real-time monitoring systems for high-risk populations.
Abbreviations
DDDc, Defined daily dose consumption; PTX, Pentoxifylline; HIS, Hospital Information System; DDD, Defined daily dose.
Data Sharing Statement
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
Human Ethics
The Ethics Committee of the Central Hospital Affiliated with Shandong First Medical University approved this retrospective study, waiving the need for formal ethics approval and individual patient consent. All methods were carried out in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was funded by Shandong Provincial Pharmaceutical Association (No.Kjyw2024-13).
Disclosure
YuanYuan Zheng and Yanhui Yin are co-first authors for this study. The authors declared that they have no conflicts of interest regarding this work.
References
1. Kitchens BP, Snyder RJ, Cuffy CA. A literature review of pharmacological agents to improve venous leg ulcer healing. Wounds. 2020;32(7):195–207.
2. Uney K, Tras B, Corum O, Yildiz R, Maden M. Pharmacokinetics of pentoxifylline and its 5-hydroxyhexyl metabolite following intravenous administration in cattle. Trop Anim Health Prod. 2019;51(2):435–441. doi:10.1007/s11250-018-1710-8
3. Broderick C, Forster R, Abdel-Hadi M, Salhiyyah K. Pentoxifylline for intermittent claudication. Cochrane Database Syst Rev. 2020;10(10):CD005262. doi:10.1002/14651858.CD005262.pub4
4. Yang Q, Lang Y, Yang W, et al. Efficacy and safety of drugs for people with type 2 diabetes mellitus and chronic kidney disease on kidney and cardiovascular outcomes: a systematic review and network meta-analysis of randomized controlled trials. Diabet Res Clin Pract. 2023;198:110592. doi:10.1016/j.diabres.2023.110592
5. Hu Y, Sun C, Chen Y, Liu YD, Fan JG. Pipeline of new drug treatment for non-alcoholic fatty liver disease/metabolic dysfunction-associated steatotic liver disease. J Clin Transl Hepatol. 2024;12(9):802–814. doi:10.14218/JCTH.2024.00123
6. Donate-Correa J, Ferri CM, Mora-Fernández C, Pérez-Delgado N, González-Luis A, Navarro-González JF. Pentoxifylline ameliorates subclinical atherosclerosis progression in patients with type 2 diabetes and chronic kidney disease: a randomized pilot trial. Cardiovasc Diabetol. 2024;23(1):314. doi:10.1186/s12933-024-02393-x
7. Zheng L, Jia J, Chen Y, et al. Pentoxifylline alleviates ischemic white matter injury through up-regulating Mertk-mediated myelin clearance. J Neuroinflammation. 2022;19(1):128. doi:10.1186/s12974-022-02480-4
8. Liang X, Wang Y, Zhao C, Cao Y. Systematic review the efficacy and safety of cilostazol, pentoxifylline, beraprost in the treatment of intermittent claudication: a network meta-analysis. PLoS One. 2022;17(11):e0275392. doi:10.1371/journal.pone.0275392
9. Chen XQ, Jin YY, Tang G, et al. New Pharmacology.
10. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344–e418. doi:10.1161/STR.0000000000000211
11. Chinese Society of Neurology, Cerebrovascular Group, Chinese Society of Neurology. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018. Chin J Neurol. 2018;51(09):666–682.
12. Chinese Guidelines for Diagnosis and Treatment of Dementia and Cognitive Impairment. 2018 Chinese guidelines for diagnosis and treatment of dementia and cognitive impairment (11): treatment of non-Alzheimer’s dementia. Chin Med J. 2020;100(17):1294–1298.
13. Kelechi TJ, Brunette G, Bonham PA, et al. 2019 guideline for management of wounds in patients with Lower-Extremity Venous Disease (LEVD): an executive summary. J Wound Ostomy Continence Nurs. 2020;47(02):97–110. doi:10.1097/WON.0000000000000622
14. Sinha S, Sreedharan S. Management of venous leg ulcers in general practice - a practical guideline. Aust Fam Physician. 2014;43(09):594–598.
15. Vascular Surgery Group, Surgical Society of Chinese Medical Association. Chinese expert consensus on diagnosis and treatment of chronic lower limb venous diseases. Chin J Vasc Surg. 2014;03:143–151.
16. Vascular Surgery Group, Surgery Society of Chinese Medical Association, Vascular Surgeons Society of Chinese Medical Doctor Association, Vascular Surgery Society of China Association for the Promotion of International Healthcare Exchanges, et al. Guidelines for diagnosis and treatment of chronic venous diseases in China. Chinese Med J. 2019;99(39):3047–3061.
17. Han CM, Sun HF, Qiang LP, et al. Suggestions on diagnosis and treatment of chronic wound. Chin J Burn. 2010;26(05):390–402.
18. Conte MS, Pomposelli FB, Clair DG, et al. Society for vascular surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: management of asymptomatic disease and claudication. J Vasc Surg. 2015;61(3 Suppl):2s–41s. doi:10.1016/j.jvs.2014.12.009
19. Guyatt GH, Akl EA, Crowther M, et al. Executive summary: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):7s–47s. doi:10.1378/chest.1412S3
20. Chandrasekhar SS, Tsai Do BS, Schwartz SR, et al. Clinical practice guideline: sudden hearing loss (Update). Otolaryngol Head Neck Surg. 2019;161(1 suppl):S1–S45. doi:10.1177/0194599819859885
21. National Geriatric Medicine Center, Chinese Geriatric Medicine Branch, Chinese Geriatric Health Care Association Diabetes Professional Committee. Chinese guidelines for the diagnosis and treatment of senile diabetes (2021 edition). Chin J Diabetes. 2021;13(01):14–46.
22. Beijing Hypertension Prevention and Control Association, Beijing Diabetes Prevention and Control Association, Beijing Chronic Disease Prevention and Health Education Research Association, et al. Practice guide for integrated cardiovascular disease management at primary level 2020. Chin Med Front J. 2020;12(08):1–73.
23. Diabetes Society of Chinese Medical Association. China Type 2 diabetes prevention and treatment guidelines (2020 edition). Chin J Diabetes. 2021;13(04):315–409.
24. Chinese Medical Association Diabetes Society, Chinese Medical Association Infectious Diseases Society, Chinese Medical Association Tissue repair and regeneration Society. Guidelines for the prevention and treatment of diabetic foot in China (2019 edition). Chin J Diabetes. 2019;11(03):161–189.
25. Diabetes and microcirculation Committee of Chinese Microcirculation Society. Expert consensus on screening and prevention of primary diabetic microangionopathy. Chin J Med Front. 2018;10(02):17–25.
26. Crabb DW, Im GY, Szabo G, et al. Diagnosis and treatment of alcohol-associated liver diseases: 2019 practice guidance from the American Association for the study of liver diseases. Hepatology. 2020;71(01):306–333. doi:10.1002/hep.30866
27. Chinese Medical Association, Journal of Chinese Medical Association, Branch of Gastroenterology of Chinese Medical Association, et al. Guidelines for primary diagnosis and treatment of alcoholic liver disease (2019). J Clin Hepatobiliary Dis. 2021;37(01):36–40.
28. Eslam M, Sarin SK, Wong VW, et al. The Asian Pacific Association for the study of the liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol Int. 2020;14(06):889–919. doi:10.1007/s12072-020-10094-2
29. Mcintosh SE, Freer L, Grissom CK, et al. Wilderness medical society clinical practice guidelines for the prevention and treatment of Frostbite: 2019 update. Wilderness Environ Med. 2019;30(4s):S19–S32. doi:10.1016/j.wem.2019.05.002
30. Chinese Stomatological Association Oral Mucosal Diseases Professional Committee, Chinese Stomatological Association Integrated Traditional Chinese and Western Medicine Professional Committee, Zhou Gang. Guidelines for diagnosis and treatment of recurrent Aphthous ulcer. Chin J Stomatol. 2012;47(07):402–404. doi:10.3760/cma.j.issn.1002-0098.2012.07.005
31. U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) v5.0; 2017.
32. Zhang WS, Yang YH. Establishment of ATC/DDD system and its application in drug utilization research. J Clin Pharmacother. 2009;7(01):32–37.
33. Zhang F, Guo Y, Li JX. Application and Case of Pharmacoeconomics. Chemical Industry Press; 2018:117.
34. Salian HH, Raghav MV, Rawat VS, Divakar A. Cost-minimization analysis of escitalopram, fluoxetine, and amitriptyline in the treatment of depression. Indian J Pharmacol. 2023;55(5):293–298. doi:10.4103/ijp.ijp_854_22
35. Criqui MH, Matsushita K, Aboyans V, et al. Lower extremity peripheral artery disease: contemporary epidemiology, management gaps, and future directions: a scientific statement from the American Heart Association [published correction appears in Circulation. 2021 Aug 31;144(9):e193. doi: 10.1161/CIR.0000000000001019]. Circulation. 2021;144(9):e171–e191. doi:10.1161/CIR.0000000000001005
36. Bertram MY, Lauer JA, Stenberg K, Edejer TTT. Methods for the economic evaluation of health care interventions for priority setting in the health system: an update from WHO CHOICE. Int J Health Policy Manag. 2021;10(11):673–677. doi:10.34172/ijhpm.2020.244
37. National Bureau of Statistics of China. Statistical Communiqué of the People’s Republic of China on the 2023 National Economic and Social Development. Available from: http://www.stats.gov.cn/.
38. Lin YC, Chang YH, Yang SY, Wu KD, Chu TS. Update of pathophysiology and management of diabetic kidney disease. J Formos Med Assoc. 2018;117(8):662–675. doi:10.1016/j.jfma.2018.02.007
39. Wen WX, Lee SY, Siang R, Koh RY. Repurposing Pentoxifylline for the treatment of fibrosis: an overview. Adv Ther. 2017;34(6):1245–1269. doi:10.1007/s12325-017-0547-2
40. Kazemi MH, Shokrollahi Barough M, Ghanavatinejad A, et al. Decrease of tumor-infiltrating regulatory T cells using pentoxifylline: an ex vivo analysis in triple-negative breast cancer mouse model. Iran J Allergy Asthma Immunol. 2022;21(2):167–177. doi:10.18502/ijaai.v21i2.9224
41. Wang YP, Li YJ, Zhang J, et al. Analysis on the labeling of drip speed limit items in the instructions of intravenous infusion drugs in a hospital. China Pharm Industry. 2020;29(04):12–15.
42. Yuan Y. Research progress of infusion speed control in intravenous drip. Contemp Nurs. 2020;27(01):4–6.
43. Fang JH, Chen YC, Ho CH, et al. The risk of major bleeding event in patients with chronic kidney disease on pentoxifylline treatment. Sci Rep. 2021;11(1):13521. doi:10.1038/s41598-021-92753-4
44. Li J. One case of adverse reaction caused by intravenous injection of pentoxifylline. J Pharmacoepidemiol. 2006;02:82.
45. Zhong SJ. Anaphylactic shock induced by intravenous pentoxifylline: a case report. Chin Modern Appl Pharm. 2004;03:229.
46. Gilbert GJ. Pentoxifylline-induced musical hallucinations. Neurology. 1993;43(8):1621–1622. doi:10.1212/WNL.43.8.1621
47. Mathian A, Amoura Z, Piette JC. Pentoxifylline-induced aseptic meningitis in a patient with mixed connective tissue disease. Neurology. 2002;59(09):1468–1469. doi:10.1212/01.WNL.0000032107.87017.DA
48. Gonzalez-Mahave I, Del Pozo MD, Blasco A, et al. Urticaria due to pentoxyfylline. Allergy. 2005;60(05):705. doi:10.1111/j.1398-9995.2005.00724.x
49. Seoane-Lestón FJ, Añibarro-Bausela MB, Mugíca-García MV, et al. Urticaria caused by pentoxifylline. J Investig Allergol Clin Immunol. 2009;19(01):74–75.
50. Patrizi A, Tabanelli M, Antonucci A, et al. Acute generalized exanthematous pustulosis induced by pentoxifylline. Int J Dermatol. 2007;46(12):1310–1312. doi:10.1111/j.1365-4632.2007.03378.x
51. Saunderson RB, Garsia R, Headley AP, et al. Pentoxifylline-induced drug rash with eosinophilia and systemic symptoms (DRESS) in a patient with caffeine intolerance. J Dermatol Case Rep. 2013;7(03):77–81. doi:10.3315/jdcr.2013.1150
52. Oren R, Yishar U, Lysy J, et al. Pentoxifylline-induced gastrointestinal bleeding. Dicp. 1991;25(03):315–316. doi:10.1177/106002809102500320
53. Sáez-Royuela F, López-Vázquez A, López-Morante A, et al. Pentoxifylline-induced acute hepatitis. J Hepatol. 1995;23(04):482–484. doi:10.1016/0168-8278(95)80212-6
54. Acharya S, Nair BC. Pentoxifylline-induced thrombocytopenia. Int J Dermatol. 1997;36(8):635–636. doi:10.1111/j.1365-4362.1997.tb01184.x
55. Vedes EC, Marques LD, Toscano Rico MC. Severe isolated thrombocytopenia after clopidogrel and pentoxifylline therapy: a case report. J Med Case Rep. 2011;5:281. doi:10.1186/1752-1947-5-281
56. Tan MW, Sklar GE. Pentoxifylline-Induced Thrombocytopenia: a Case Report. J Pharm Pract. 2015;28(6):572–576. doi:10.1177/0897190015608274
57. Neels K, Finkelstein S, Douglass C. Medical cost savings from pentoxifylline therapy in chronic occlusive arterial disease. Pharmacoeconomics. 1994;5(2):130–140. doi:10.2165/00019053-199405020-00007
58. Squires H, Simpson E, Meng Y, et al. A systematic review and economic evaluation of cilostazol, naftidrofuryl oxalate, pentoxifylline and inositol nicotinate for the treatment of intermittent claudication. Health Technol Assess. 2011;15(40):1–210. doi:10.3310/hta15400
59. Chen L, Gao Y, Liu M, et al. Efficacy and safety of pentoxifylline for chronic venous leg ulcers: study protocol for a multicenter randomized controlled trial in China (ESPECT study). Trials. 2023;24(1):491. doi:10.1186/s13063-023-07547-y
60. Thursz M, Forrest E, Roderick P, et al. The clinical effectiveness and cost-effectiveness of STeroids Or Pentoxifylline for Alcoholic Hepatitis (STOPAH). Health Technol Assess. 2015;19(102):1–104. doi:10.3310/hta191020
61. Liu P, Zheng Y, Zhong P, et al. Interpretation of the 2019 U.S. clinical practice guidelines for sudden deafness (Updated edition). J Audiol Speech Disord. 2020;28(04):480–483.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.