")
Back to Journals » Clinical Ophthalmology » Volume 18
Real-World-Data of Treatment-Naïve and Previously Treated Patients Receiving Up to 3 Injections of Faricimab in Neovascular Age-Related Macular Degeneration
Authors Kunzmann BC, Schweig AS, Bartz-Schmidt KU, Sobolewska B
Received 7 August 2024
Accepted for publication 3 December 2024
Published 28 December 2024 Volume 2024:18 Pages 4029—4039
DOI https://doi.org/10.2147/OPTH.S482948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Berenike Cornelia Kunzmann, Alexandra Stefanie Schweig, Karl Ulrich Bartz-Schmidt, Bianka Sobolewska
University Eye Hospital, Centre for Ophthalmology, University of Tuebingen, Tuebingen, Germany
Correspondence: Berenike Cornelia Kunzmann, University Eye Hospital Tübingen, Department of Ophthalmology, Elfriede-Aulhorn-Str. 7, Tübingen, 72076, Germany, Tel +49 7071 29 64356, Fax +49 7071 29 5216, Email [email protected]
Purpose: To evaluate visual and anatomical outcome of consecutive patients who received intravitreal injections (IVI) of faricimab for the treatment of neovascular age-related macular degeneration (nAMD).
Patients and methods: A retrospective study of patients treated for nAMD with one to three IVIs of faricimab from October 2022 to January 2024. Demographic data, treatment history, best corrected visual acuity (BCVA), anatomic parameters, and adverse events (AEs) were collected.
Results: After one IVI of faricimab, previously treated (n=160) eyes with a mean of 33.51 IVIs and treatment-naïve (n=10) eyes showed a mean BCVA gain of +0.59± 0.52 letters (p=0.364) and +5.00± 6.50 letters (p=0.461), respectively, and a mean central subfield thickness (CST) reduction of − 27.65± 5.33 μm (p< 0.001) and − 94.10± 39.74 μm (p=0.042), respectively. In treatment-refractory eyes after switching from aflibercept (n=108), mean BCVA increased by +0.42± 0.66 (p=0.745) and the mean CST improved by − 21.98± 6.04 (p< 0.001). After three IVIs of faricimab previously treated (n=106) and treatment-naïve (n=5) eyes showed a mean BCVA increase of +1.57± 0.88 letters (p=0.051) versus +12.50± 8.14 letters (p=0.185), and a mean CST reduction of − 25.51± 5.82 μm (p< 0.001) versus − 82.60± 36.20 μm from baseline, respectively. In treatment-refractory eyes after switching from aflibercept (n=79), mean BCVA improved by +2.15± 1.08 letters (p=0.029) and mean CST decreased by − 27.46± 7.04 μm (p< 0.001). Mean pigment epithelial detachment (PED) was also significantly reduced even between the first and the third faricimab injection in previously treated eyes (p=0.03). The proportion of eyes with intraretinal fluid and subretinal fluid improved significantly in all eyes and treatment-refractory eyes after switching from aflibercept. Ocular AEs were reported in three out of 170 eyes, and one patient had two stroke events during faricimab therapy.
Conclusion: Three IVIs of faricimab have the potential to improve visual acuity and anatomical parameters even in treatment-refractory nAMD eyes with a mean dosing interval of more than 6 weeks.
Keywords: anti-vascular endothelial growth factor, intravitreal injection, treatment resistant nAMD, intravitreal dosing interval, Vabysmo
Introduction
In addition to the currently most commonly used anti-VEGF drugs (approved: aflibercept, ranibizumab and brolucizumab; off-label: bevacizumab) for neovascular age related macular degeneration (nAMD), the Food and Drug Administration has approved faricimab for the treatment of nAMD and diabetic macular edema.1–4 Faricimab is an IgG monoclonal antibody and – as a novelty – for the first time a bispecific antibody that inhibits two signaling pathways by independently and simultaneously binding and neutralising both, angiopoietin-2 receptors and VEGF alpha.4 Angiopoietin-2, which is primarily produced by vascular endothelial cells, is elevated by hypoxic stress and is a cofactor for new vessel development.4 The burden for patients, their caregivers and the healthcare system to facilitate continuous monitoring and frequent injections is a major challenge. Longer duration and better patient outcomes are therefore essential goals for drug manufacturer and physicians.5 TENAYA and LUCERNE were the nAMD Phase 3 treatment-naïve clinical trials of intravitreal faricimab. At 48 weeks, visual acuity improvement and morphological outcome were comparable and non-inferior to aflibercept 2mg. Given a fixed 8-week aflibercept interval, faricimab could be administered at up to 16-week intervals with an acceptable safety profile.4
Real-world studies are essential to complement the results of clinical trials and provide additional data on the efficacy and safety of faricimab in the treatment of nAMD. The first real-world retrospective studies have been published.6–24 Two Japanese studies reported results of 40 to 60 eyes with treatment-naïve nAMD,8,9 and three American studies described results for larger numbers of eyes with previously treated nAMD.10–12 Sim et al showed one-year-effects of faricimab for 117 eyes being switched due to high treatment burden.15 In addition, a prospective study presented the results of 26 previously treated nAMD patients who were switched to intravitreal faricimab due to an unsatisfactory fluid-free interval of up to 8 weeks.13 However, more real-world results are essential to improve and deepen our understanding of faricimab responses.
Therefore, the aim of this real-world study was to evaluate the clinical functional and morphological outcomes of faricimab treatment in consecutive nAMD patients, which, together with the present real-world results, may provide further insights into the challenges of nAMD treatment, especially in the previously treated nAMD.
Materials and Methods
Study Design
This is a retrospective, observational, single-centre study of patients with neovascular AMD who were treated with 6 mg (0.05 mL of 120 mg/mL faricimab) intravitreal injections of faricimab between October 2022 and January 2024, at the Centre of Ophthalmology, Eberhard-Karls University Tuebingen. By including all patients who received at least one injection of faricimab for the treatment of nAMD after European-approval, without using exclusion criteria, the real-word data were evaluated. This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Ethics Committee of the University of Tuebingen (441/2023BO2). Informed consent was waived for this retrospective study because all identifying patient data was omitted.
At the baseline visit before the first faricimab injection, demographic data were collected including age, gender, number and name of previous anti-VEGF agents, if applicable. An ophthalmological examination including best corrected visual acuity (BCVA), slit lamp biomicroscopy, and macular optical coherence tomography (Spectralis OCT; Heidelberg Engineering, Heidelberg, Germany) was performed before each faricimab injection. OCT-Angiography was not regularly taken, so we excluded it from our data collection.
All treatment-naïve patients underwent fluorescein angiography at baseline. Snellen visual acuity was converted to the Early Treatment Diabetic Retinopathy Study (ETDRS) letter scores using the following formula “ETDRS = 85 + 50 × log10 (Snellen Fraction)”.25 OCT was used to assess the following variables: central subfield thickness (CST), the presence of subretinal and/or intraretinal fluid (SRF/IRF) and pigment epithelium detachment (PED). A custom 20° x 15° volume acquisition protocol, which covered a 5.8 mm x 4.4 mm surface of the macula with 37 B-scans, corresponding to 121 µm interscan distance, was used. CST was determined as the mean retinal thickness between inner limiting membrane and Bruch’s membrane of the circular area within 1mm diameter around the fovea.26 The elevation of the PED was measured from retinal pigment epithelium to Bruch’s membrane at the highest point of the PED. Assessment of the scans was done by a single investigator (BK).
The primary outcomes were functional and anatomic efficacy of the real-world data.
Statistical Analysis
Mean and standard error (SEM) were used for continuous variables and percentages for categorical and dichotomous variables, unless otherwise stated. Two continuous variables were compared using the Wilcoxon signed-rank test if they were not normally distributed, or by using the paired samples t-test if they were normally distributed. The McNemar test was used to analyze two dichotomous variables. When more than two time points of dependent samples were analyzed, the Friedman-Test (for continuous variables that were not normally distributed) or one-way analysis of variance (for normally distributed variables) was used.
In addition, the following subgroup analyses were performed to determine the outcome in 1) all patients with at least one faricimab for the treatment of nAMD without using exclusion criteria in both previously treated and treatment-naïve patients, and 2) in patients with treatment-refractory nAMD who crossed over from aflibercept and received at least 6 consecutive anti-VEGF injections prior to faricimab initiation. Statistical analyses were performed using commercial software (GNU PSPP version 0.10.2-g654fff) and a p-value < 0.05 was considered statistically significant.
Results
Demographics and Patient Characteristics
One hundred and seventy eyes (136 patients) were treated with one intravitreal injection of faricimab. The mean age was 79.13±7.57 (standard deviation) (55–93) years. 55.9% (n=76) were female and 64.7% (n=110) were pseudophakic. Ten (5.1%) eyes were treatment-naïve and 160 (94.9%) eyes had received a mean of 33.51 injections of other anti-VEGF agents prior to the first injection of faricimab. Baseline patient demographics are shown in Table 1.
 |
Table 1 Baseline Demographics of All Patients with One Faricimab Injection. The Characteristics of the Study Patients (SD – Standard Deviation, ETDRS – Early Treatment Diabetic Retinopathy Study) |
Functional and Anatomic Outcome After One Injection of Faricimab
All eyes (n=170) showed a mean BCVA gain of +0.85±0.61 letters (p=0.286) and a mean CST reduction of −31.56±5.61 μm (p<0.001). One-hundred sixty eyes of these patients were treated with other anti-VEGF agents for an average of 33.51 injections prior to their first faricimab injection. After switching to faricimab, they showed a mean BCVA gain of +0.59±0.52 letters (p=0.364) and a mean CST reduction of −27.65±5.33 µm (p<0.001). In treatment-naïve patients (n=10 eyes), mean BCVA increased by +5.00±6.50 letters (p=0.461) and mean CST reduced by −94.10±39.74 μm (p=0.042). The complete overview after one injection of faricimab is shown in Table 2. Dry macula was achieved in 25.3% (n=43) of all eyes, in 25% (n=40) of previously treated eyes, and in 30% (n=3) of treatment-naïve eyes. Resolution of IRF and SRF was observed in 24.5% (n=25; p<0.001) and 34.3% (n=46; p<0.001) of all eyes, in 23.7% (n=23; p<0.001) and 33.9% (n=42; p<0.001) of previously treated eyes, and in 40% (n=2; p=0.500) and 40% (n=4; p=0.125) of treatment-naïve eyes, respectively (Figure 1). Mean height of PED decreased in all eyes by −30.63±4.72 μm (205.99±9.49 vs 175.36±8.89; p<0.001; n=139), −28.53±4.40 μm (204.09±9.39 vs 175.56±9.07; p<0.001; n=133) in previously-treated eyes and −77.33±49.55 μm (248.17±75.48 vs 170.83±49.51; p=0.179; n=6) in treatment-naïve eyes.
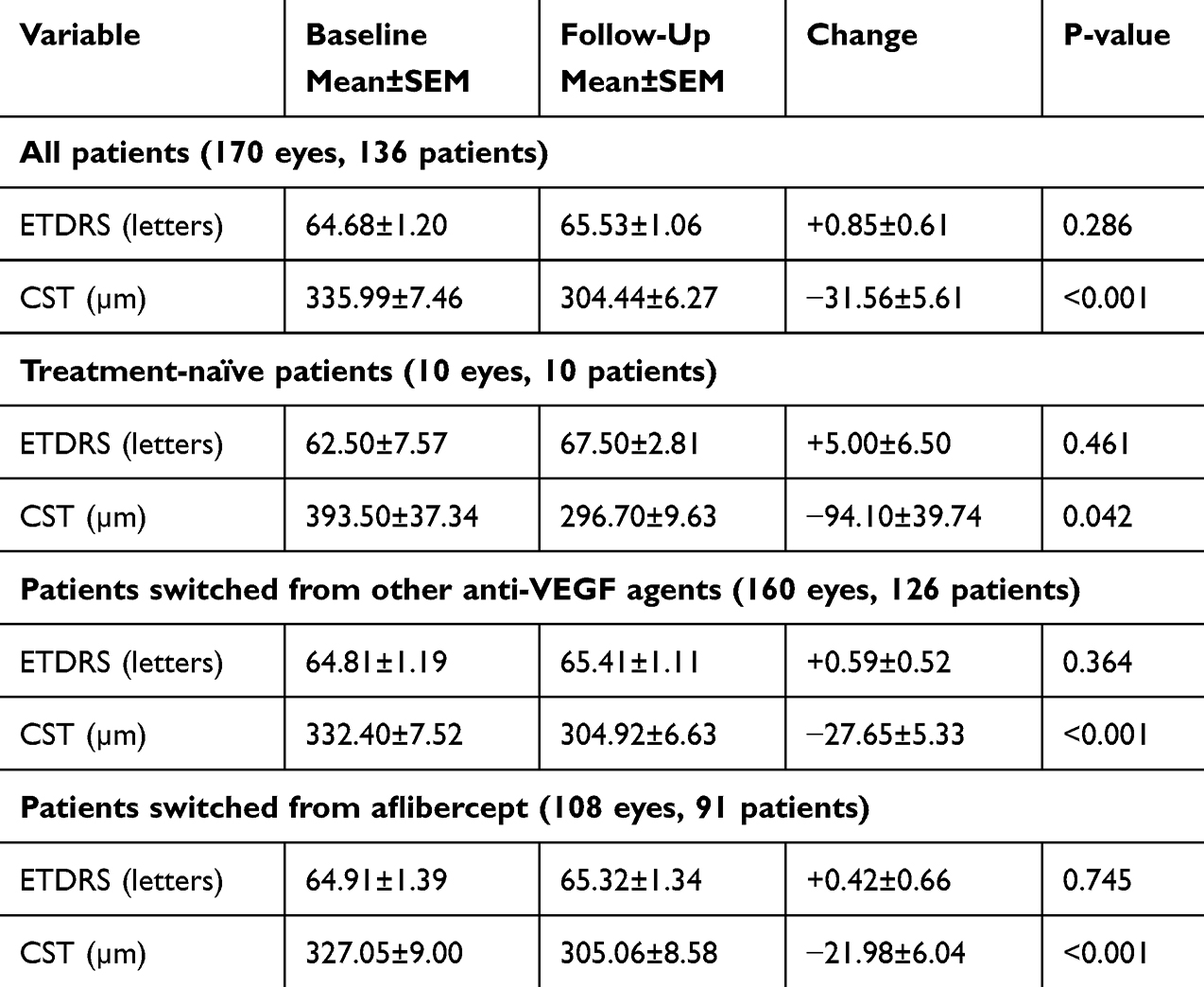 |
Table 2 Outcome After One Injection of Faricimab, n=170 Eyes (136 Patients) |
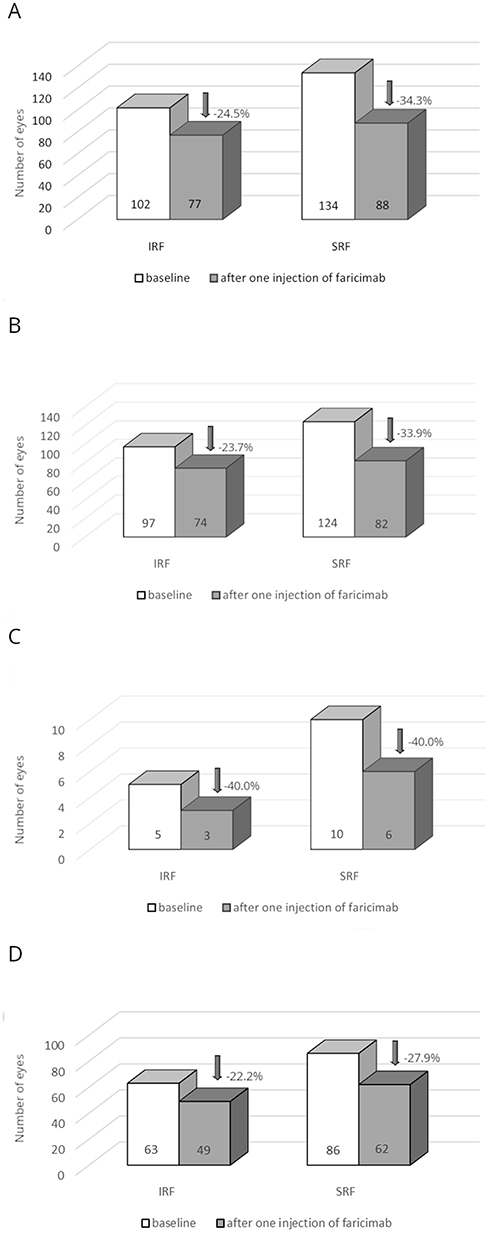 |
Figure 1 The resolution of intraretinal fluid and subretinal fluid after one injection of faricimab in: (A) all eyes. (B) previously-treated eyes. (C) treatment-naïve eyes. (D) treatment-resistant eyes after switching from aflibercept. |
Subgroup Analysis of Treatment-Refractory nAMD After One Injection of Faricimab
One-hundred eight eyes of 91 patients (female: n=49 (53.8%)) with a mean age of 78.27±8.17 (55–93) years were refractory to aflibercept (40.17±20.26 (7–92)), the mean BCVA gain was +0.42±0.66 letters (p=0.745) and mean CST showed a reduction of −21.98±6.04 μm (p<0.001) (Table 2). Dry macula was achieved in 22.2% (n=24) of treatment-refractory eyes to aflibercept. Resolution of IRF and SRF was observed in 22.2% (n=14; p=0.001) and 27.9% (n=24; p<0.001) of treatment-refractory eyes to aflibercept, respectively (Figure 1). Mean PED showed a decrease of −25.99±5.78 μm (188.65±10.85 vs 162.66±10.43; p<0001; n=90).
After Three Injections of Faricimab
A total of 111 eyes received three injections of faricimab with a mean interval of 6.57±2.85 weeks between faricimab injections; the mean prior interval of other anti-VEGF was 7.53±6.62 weeks in previously treated patients. In all patients, mean BCVA increased by +2.16±0.95 letters (p=0.018) and mean CST decreased by −28.08±5.86 μm (p<0.001) from baseline. Patients who crossed over from other anti-VEGF agents (n=106 eyes) showed a mean BCVA increase of +1.57±0.88 letters (p=0.051) and a mean CST reduction of −25.51±5.82 µm (p<0.001) from baseline. In treatment-naïve patients (n=5), mean BCVA increased by +12.50±8.14 letters (p=0.185) and mean CST decreased by −82.60±36.20 µm from baseline (p=0.085). In the post hoc analysis, there were no significant differences between all three faricimab injections in any group. The results after three injections of faricimab are shown in Table 3.
 |
Table 3 Outcome After Three Injections of Faricimab, n=111 Eyes (99 Patients) |
Dry macula was reached in 19.8% (n=22) of all eyes, in 17.9% (n=19) of previously-treated eyes, and in 60% (n=3) of treatment-naïve eyes. Resolution of IRF and SRF was observed as follows: 13.4% (n=9; p=0.022) and 28.2% (n=24; p<0.001) in all eyes, 9.4% (n=6; p=0.109) and 26.6% (n=21; p<0.001) in previously treated eyes, and 100% (n=3; p=0.250) and 0% (n=0; p=0.250) in treatment-naïve eyes, respectively (Figure 2). Mean height of PED demonstrated a decrease of −41.91±6.07 µm (211.04±11.63 vs 169.14±10.78; p<0.001; n=95) in all eyes, −38.07±5.74 µm (207.98±11.23 vs 169.91±10.81; p<0.001; n=91) in previously treated eyes and −129.25±48.06 µm (280.75±113.40 vs 151.50±81.85; p=0.074; n=4) in treatment-naïve eyes. In the post hoc analysis, there was a significant difference of the PED height between the first and the third faricimab injection in all patients (176.14±11.07 vs 169.14±10.78; p =0.03) and in previously treated patients (177.00±11.18 vs 169.91±10.81; p = 0.03).
 |
Figure 2 The resolution of intraretinal fluid and subretinal fluid after three injections of faricimab in: (A) all eyes. (B) previously-treated eyes. (C) treatment-naïve eyes. (D) treatment-resistant eyes after switching from aflibercept. |
Subgroup Analysis of Treatment-Refractory nAMD After Three Injections of Faricimab
Seventy-nine treatment-refractory eyes to aflibercept received three faricimab injections with a mean interval between faricimab injections of 6.25±2.54 weeks. Mean previous interval of other anti-VEGF was 7.3±5.78 weeks.
Mean BCVA increased by +2.15±1.08 letters (p=0.029) and mean CST reduced by −27.46 ±7.04 µm (p<0.001) from baseline (Table 3). Dry macula was achieved in 15.2% (n=12) of aflibercept treatment-refractory eyes. Resolution of IRF and SRF was observed in 12.5% (n=6; p=0.031) and 22.6% (n=14; p=0.004) of aflibercept treatment-refractory eyes, respectively. Mean PED decreased by −34.77±6.08 µm (202.72±12.56 vs 167.95±11.69; p<0001; n=64) in treatment-refractory eyes to aflibercept. The post hoc analysis showed no significant difference in CST, ETDRS, and PED height between all three faricimab injections.
Safety
Adverse events (AEs) were reported in four out of 170 (2.4%) eyes. There was one case of mild anterior chamber inflammation after the first injection of faricimab, which was treated with topical steroids for one week until resolution. The patient was switched back to ranibizumab. One patient had two minor strokes six weeks after the second faricimab injection without any residuals. The treatment was continued with faricimab eight weeks after the strokes without any problems. There was one case of subretinal hemorrhage two weeks after first faricimab injection. Treatment was switched back to aflibercept and the visual outcome was good. One eye had RPE-rupture after the first injection of faricimab, treatment was continued and the visual acuity remained stable after the RPE-rupture.
Discussion
Despite the demonstrated efficacy of the novel bi-specific antibody faricimab in treatment-naïve nAMD patients, the therapeutic effects of faricimab in recalcitrant nAMD patients remain unclear.4 Therefore, the main interest of this real-world study was to evaluate the response to faricimab switching in recalcitrant cases of nAMD.
In 160 consecutive eyes previously treated with anti-VEGF-agents (aflibercept, ranibizumab or bevacizumab), the results showed that after one and three injections of faricimab the BCVA was maintained (+0.59 letters) and improved (+1.57 letters), and the CST decreased significantly (−27.65 µm and −25.51 µm) compared to baseline. The height of the PED was reduced significantly after one injection (−28.53 µm) and after three injections (−38.07 µm) compared to baseline, as well as between the first and the third injection. Resolution of IRF and SRF was observed in 23.7% and 33.9% after one injection and 9.4% and 26.6% of previously treated eyes after three injections, respectively. The minority of our study patients (n=10) were treatment-naïve. The mean BCVA showed an improvement after one (+5.00 letters) and three injections (+12.50 letters) in this subgroup. The mean CST indicated a reduction after one (−94.10 µm) and three injections (−82.60 µm) and PED was reduced after one (−77.33 µm) and three injections (−129.25 µm). Resolution of IRF and dry macula was observed in 100% and 60% of treatment-naïve eyes after three injections. These results are comparable to the visual and anatomical results of the clinical trials TENAYA and LUCERNE with visual improvement of 5.8 ETDRS letters and CST reduction of −137 μm in treatment-naïve patients.4 In the first real-world study, Stanga et al reported an improvement in BCVA and central retinal thickness after one injection of faricimab in three treatment-naïve nAMD eyes and eight nAMD eyes previously treated with other anti-VEGF agents.7 The visual and anatomical results were confirmed by two Japanese studies on three injections of faricimab in treatment-naïve nAMD. Dry macula was achieved in 31 of 40 eyes (79.5%) at week 16.8 Similar results reported Mukai et al in 63 treatment-naïve eyes with nAMD. They showed a complete resolution of IRF/SRF in 82% of the eyes.9 In both studies, the statistical significance was reached after the first faricimab injection.8,9 The percentage of fluid resolution and dry macula achievement rate were similar to this study. The real-word data from the TRUCKEE-Study showed a mean improvement in BCVA of +4.9 letters and a significant reduction in CST of −84.5 μm after one injection of faricimab in 39 treatment-naïve eyes. After three injections of faricimab, thirteen treatment-naïve eyes showed an improvement in BCVA of +8.1 letters, a reduction in CST of −80.1 μm, and a resolution of IRF and SRF in 45.5% and 25%, respectively.10 The results of Khanani et al, which did not exclude any patients, were consistent with this study. All these results underline the fact that the efficacy of faricimab in treatment-naïve patients in the real-world is comparable to the results of pivotal trials.4
In contrast to the study settings with treatment-naïve patients, most of our patients were previously treated with anti-VEGF-agents. They showed maintenance of BCVA (+0.59 letters) and a significant reduction in CST of −27.65 μm in previously treated eyes after one injection of faricimab. After three injections of faricimab, one hundred and six previously treated eyes showed an improvement in BCVA of +1.57 letters and a significant reduction in CST of −25.51 µm. This markedly worse visual and anatomical outcome compared to treatment-naïve patients is in line with real-world data analysis on patients with previously treated nAMD and a high average of 31.1–34.2 anti-VEGF injections before switching to faricimab.10–12 The improvement of functional outcome did not yield statistically significance similar to other real-world studies.11,14–19 That might be secondary to development of macular atrophy as discussed in the study of Sim et al14 or due to persistence of structural OCT biomarkers such as subretinal hyperreflective material (SHRM),27,28 which were evaluated until now after treatment with other anti-VEGF agents.29,30 However, treatment switch to faricimab proved a significant reduction of CST, which was consistent with other real-world studies.10–12,14,16–19 Pandit et al and Sim et al showed also improvement of anatomical outcome after ≥ 4 faricimab injections and at 12 months: the central foveal thickness decreased from 354.8 µm to 306.6 µm11 and the mean CST was reduced by 22.1 µm,14 respectively. The differences in the anatomical outcome may be explained by a high mean of anti-VEGF injections of 10.2 ± 1.8/year preceding switch.14 In addition, patients crossed over from other anti-VEGF showed a resolution of IRF and SRF in 9.4% and 26% of previously treated eyes, which is in line with the study of Khanani et al, Pandit et al and Leung et al.10–12 Furthermore, the study results regarding PED were slightly worse than in the TRUCKEE study but similar to the improvement of PED height after ≥ 4 faricimab injections in the study of Pandit et al although the mean interval between the injections was shorter in both studies than in this study (43.5 days and 37 days vs 6.57 weeks).10,11
Compared to the discussed results in previously treated patients, the results of switching from aflibercept to faricimab in eyes with refractory nAMD seem to be slightly worse than in patients treated with other anti-VEGF agents. Kataoka et al showed that central retinal thickness decreased significantly at 1 month, although statistical significance was lost at 6 months, BCVA and maximal PED elevation did not show significant changes and there were no significant reductions in SRF, IRF, or sub-RPE fluid.20 Inoda et al and Kishi et al also found no significant change in BCVA in 80 and 55 nAMD eyes previously treated with either aflibercept or brolucizumab after one injection and three injections of intravitreal faricimab, respectively.21,22 These functional results are consistent with these real-world studies, but only after one injection of faricimab. However, we did observe a significant improvement in BCVA after three injections of faricimab in treatment-refractory nAMD eyes after switching from aflibercept. In addition, a significant reduction of CST was observed, as reported by Kataoka et al, Khanani et al, and the most recent study by Raimondi et al.11,25,28 Furthermore, resolution of IRF and SRF was achieved in 12.5% and 22.6% of eyes, respectively, similar to the TRUCKEE-Study, Kishi et al and Raimondi et al.10,20,23 In summary, these data demonstrate the significant efficacy of faricimab in the reduction of the CST and maintaining visual acuity in recalcitrant nAMD-patients with up to three injections. These results suggest that patients with persistent, previously treated nAMD could benefit from a monthly loading dose of faricimab to achieve the best possible outcome of this drug. Khanani et al suggest treating these patients with three monthly injections if possible, or maintaining their previous treatment interval for three injections before attempting to extend dosing interval.10 However, Raimondi et al found no evidence that 2 vs 3 loading doses of faricimab had any effect on clinical outcomes in 68 nAMD eyes after switching from at least 6 consecutive intravitreal injections of aflibercept.23 In this study, an additional significant reduction of the PED height was observed between the first and third intravitreal faricimab injections in previously treated eyes, supporting three faricimab injections after switching from other anti-VEGF agents. Therefore, more data with longer follow-up are needed to draw conclusions regarding possible extension of the treatment interval in recalcitrant nAMD-patients.
The safety of a newly approved drug may influence the decision of retinal physicians, as there are effective and safe approved anti-VEGF agents for the treatment of nAMD. The main concern with intravitreal injection therapy is the development of endophthalmitis or a retinal vasculitis. In our study, one pigment epithelium rupture, one mild anterior chamber inflammation and one subretinal hemorrhage was observed after injection of faricimab. No endophthalmitis or retinal vasculitis was observed. A recent systematic review and meta-analysis found no statistically significant differences in ocular adverse events and serious adverse events between faricimab and other anti-VEGF agents, confirming its safety profile.24
A limitation of our study is its retrospective design with a heterogenous study population and the absence of a control group. Nevertheless, the absence of exclusion criteria is also considered as advantage of real-world-studies because it better reflects the clinical practice. Another limitation is the fact that it is a monocenter study of the University Eye Hospital of Tuebingen and therefore not representative of the average German population. However, these patients represent the most challenging nAMD-patients with persisting fluid, as all patients were recruited from a tertiary referral centre. Furthermore, the absence of data on OCTA (and therefore no differentiation between MNV-types) and structural OCT biomarkers (such as subretinal hyperreflective material) is another limitation of this study. In addition, we only evaluated the loading phase of intravitreal faricimab therapy for nAMD-patients. Therefore, the long-term outcomes of intravitreal faricimab including impact of OCT biomarkers on functional and anatomical outcome remain to be evaluated.
Conclusion
In conclusion, our real-world-data suggest that three injections of faricimab have the potential to maintain visual acuity and improve anatomical parameters, particularly for recalcitrant nAMD patients with persistent fluid and/or the need for injection interval prolongation > 6 weeks. More and longer follow-up studies are needed to clarify the stability of faricimab in the treatment of nAMD.
Abbreviations
IVI, intravitreal injections; nAMD, neovascular age-related macular degeneration; BCVA, best corrected visual acuity; AE, adverse events; CST, central subfield thickness; PED, pigment epithelial detachment; antiVEGF, anti-vascular endothelial growth factor; OCT, optical coherence tomography; ETDRS, early treatment diabetic retinopathy study; SRF, subretinal fluid; IRF, intraretinal fluid; SEM, standard error of the mean; SD, standard deviations; MNV, macular neovascular membranes; RPE, retinal pigment epithelium; SHRM, subretinal hyperreflective material.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Berenike Kunzmann is speaker for Roche. Prof Dr med Karl Ulrich Bartz-Schmidt has received consulting and speaker fees from Roche, Pixium, Alexion Pharmaceuticals Inc., Breye Therapeutics, Gyroscope Therapeutics, Apellis Pharmaceuticals Inc., Janssen-Cilag GmbH, Pixium Vision, ViGeneron GmbH, Biogen Inc., CureVac med. PD Dr med Bianka Sobolewska has received a travel grant from Galderma, Novartis, and Santen. Dr Alexandra Schweig reports Advisory Board non-personal fees from Bayer and Roche, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. MARINA Study Group, Rosenfeld PJ, Brown DM, Heier JS. et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481.
2. Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537–2548. [Erratum in: Ophthalmology. 2013;120(1):209-10]. doi:10.1016/j.ophtha.2012.09.006
3. Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127(1):72–84. doi:10.1016/j.ophtha.2019.04.017
4. Heier JS, Khanani AM, Quezada Ruiz C, et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022;399(10326):729–740. doi:10.1016/S0140-6736(22)00010-1
5. Prenner JL, Halperin LS, Rycroft C, Hogue S, Williams Liu Z, Seibert R. Disease burden in the treatment of age-related macular degeneration: findings from a time-and-motion study. Am J Ophthalmol. 2015;160(4):725–31.e1. doi:10.1016/j.ajo.2015.06.023
6. Rush RB, Rush SW. Intravitreal faricimab for aflibercept-resistant neovascular age-related macular degeneration. Clin Ophthalmol. 2022;16:4041–4046. doi:10.2147/OPTH.S395279
7. Stanga PE, Valentin-Bravo FJ, Stanga SEF, Reinstein UI, Pastor-Idoate S, Downes SM. Faricimab in neovascular AMD: first report of real-world outcomes in an independent retina clinic. Eye. 2023;37(15):3282–3289. doi:10.1038/s41433-023-02505-z
8. Matsumoto H, Hoshino J, Nakamura K, Nagashima T, Akiyama H. Short-term outcomes of intravitreal faricimab for treatment-naive neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2023;261(10):2945–2952. doi:10.1007/s00417-023-06116-y
9. Mukai R, Kataoka K, Tanaka K, et al. Three-month outcomes of faricimab loading therapy for wet age-related macular degeneration in Japan. Sci Rep. 2023;13(1):8747. doi:10.1038/s41598-023-35759-432
10. Khanani AM, Aziz AA, Khan H, et al. The real-world efficacy and safety of faricimab in neovascular age-related macular degeneration: the TRUCKEE study - 6 month results. Eye. 2023;37(17):3574–3581. doi:10.1038/s41433-023-02553-5
11. Pandit SA, Momenaei B, Wakabayashi T, et al. Clinical outcomes of faricimab in patients with previously treated neovascular age-related macular degeneration. Ophthalmol Retina. 2024;8(4):360–366. doi:10.1016/j.oret.2023.10.018
12. Leung EH, Oh DJ, Alderson SE, et al. Initial real-world experience with faricimab in treatment-resistant neovascular age-related macular degeneration. Clin Ophthalmol. 2023;17:1287–1293. doi:10.2147/OPTH.S409822
13. Grimaldi G, Cancian G, Rizzato A, et al. Intravitreal faricimab for neovascular age-related macular degeneration previously treated with traditional anti-VEGF compounds: a real-world prospective study. Graefes Arch Clin Exp Ophthalmol. 2024;262(4):1151–1159. doi:10.1007/s00417-023-06319-3
14. Sim SY, Chalkiadaki E, Koutsocheras G, et al. Real-world 1-year outcomes of treatment-intensive neovascular age-related macular degeneration switched to faricimab. Ophthalmol Retina. 2024. doi:10.1016/j.oret.2024.07.020
15. Penha FM, Masud M, Khanani ZA, et al. Review of real-world evidence of dual inhibition of VEGF-A and ANG-2 with faricimab in NAMD and DME. Int J Retina Vitreous. 2024;10(1):5. doi:10.1186/s40942-024-00525-9
16. Cheng A, Joshi S, Banoub RG, Saddemi J, Chalam KV. Faricimab effectively resolves intraretinal fluid and preserves vision in refractory, recalcitrant, and nonresponsive neovascular age-related macular degeneration. Cureus. 2023;15(6):e40100. doi:10.7759/cureus.40100
17. Hikichi T. Investigation of satisfaction with short-term outcomes after switching to faricimab to treat neovascular age-related macular degeneration. Jpn J Ophthalmol. 2023;67(6):652–656. [Erratum in: Jpn J Ophthalmol. 2023;67(6):657]. doi:10.1007/s10384-023-01024-4
18. Ng B, Kolli H, Ajith Kumar N, et al. Real-world data on faricimab switching in treatment-refractory neovascular age-related macular degeneration. Life. 2024;14(2):193. doi:10.3390/life14020193
19. Szigiato A, Mohan N, Talcott KE, et al. Short-term outcomes of faricimab in patients with neovascular age-related macular degeneration on prior anti-VEGF therapy. Ophthalmol Retina. 2024;8(1):10–17. doi:10.1016/j.oret.2023.08.018
20. Kataoka K, Itagaki K, Hashiya N, et al. Six-month outcomes of switching from aflibercept to faricimab in refractory cases of neovascular age‑related macular degeneration. Graefe’s Arch Clin Expl Ophthalmol. 2023;262(1):43–51. doi:10.1007/s00417-023-06222-x
21. Inoda S, Takahashi H, Takahashi R, et al. Visual and anatomical outcomes after initial intravitreal faricimab injection for neovascular age-related macular degeneration in patients with prior treatment history. Ophthalmol Ther. 2023;12(5):2703–2712. doi:10.1007/s40123-023-00779-w
22. Kishi M, Miki A, Kamimura A, et al. Short-term outcomes of faricimab treatment in aflibercept-refractory eyes with neovascular age-related macular degeneration. J Clin Med. 2023;12(15):5145. doi:10.3390/jcm12155145
23. Raimondi R, Falfeli T, Bogdanova-Bennet A, et al. Outcomes of treatment-resistant neovascular age-related macular degeneration switched from aflibercept to faricimab. Ophthalmol Retina. 2024;8(6):537–544. doi:10.1016/j.oret.2023.11.015
24. Yen WT, Wu CS, Yang CH, Chen YH, Lee CH, Hsu CR. Efficacy and safety of intravitreal faricimab for neovascular age-related macular degeneration: a systematic review and meta-analysis. Sci Rep. 2024;14(1):2485. doi:10.1038/s41598-024-52942-3
25. Gregori NZ, Feuer W, Rosenfeld PJ. Novel method for analyzing Snellen visual acuity measurements. Retina. 2010;30(7):1046–1050. doi:10.1097/IAE.0b013e3181d87e04
26. Kaiser PK, Wykoff CC, Singh RP, et al. Retinal fluid and thickness as measures of disease activity in neovascular age-related macular degeneration. Retina. 2021;41(8):1579–1586. doi:10.1097/IAE.0000000000003194
27. Fouad YA, Santina A, Bousquet E, Sadda SR, Sarraf D. Pathways of fluid leakage in age-related macular degeneration. Retina. 2023;43(6):873–881. doi:10.1097/IAE.0000000000003798
28. Metrangolo C, Donati S, Mazzola M, et al. OCT biomarkers in neovascular age-related macular degeneration: a narrative review. J Ophthalmol. 2021;2021:9994098. doi:10.1155/2021/9994098
29. Pokroy R, Mimouni M, Barayev E, et al. Prognostic value of subretinal hyperreflective material in neovascular age-related macular degeneration treated with bevacizumab. Retina. 2018;38(8):1485–1491. doi:10.1097/IAE.0000000000001748
30. Sadda S, Sarraf D, Khanani AM, et al. Comparative assessment of subretinal hyper-reflective material in patients treated with brolucizumab versus aflibercept in HAWK and HARRIER. Br J Ophthalmol. 2024;108(6):852–858. doi:10.1136/bjo-2023-323577
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.