")
Back to Journals » Clinical Ophthalmology » Volume 18
Real-World Healthcare Resource Utilization, Healthcare Costs, and Injurious Falls Among Elderly Patients with Geographic Atrophy
Authors Sarda SP, Germain G, Mahendran M, Klimek J, Cheng WY, Luo R, Duh MS
Received 18 June 2024
Accepted for publication 24 October 2024
Published 9 November 2024 Volume 2024:18 Pages 3215—3226
DOI https://doi.org/10.2147/OPTH.S475331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sujata P Sarda,1 Guillaume Germain,2 Malena Mahendran,3 Jacob Klimek,3 Wendy Y Cheng,3 Roger Luo,1 Mei Sheng Duh3
1Apellis Pharmaceuticals, Waltham, MA, USA; 2Groupe d’analyse, Ltée, Montreal, Québec, Canada; 3Analysis Group, Inc, Boston, MA, USA
Correspondence: Guillaume Germain, Vice President, Analysis Group, Inc, 1190 avenue des Canadiens-de-Montréal, Suite 1500, Montréal, QC, H3B 0G7, Canada, Tel +1-514-394-4446, Email [email protected]
Purpose: This study assessed the clinical and economic burden of geographic atrophy (GA) using real-world data from elderly patients with Medicare Advantage plans in the United States.
Patients and Methods: A retrospective cohort design of patients with GA only, GA + visual impairment (GA + VI), GA + blindness (GA + B), and patients without GA were identified using administrative healthcare claims data from Optum Clinformatics Data Mart. Inverse probability of treatment weighting controlled for confounding when comparing patients with GA only vs without GA, GA + VI vs GA only, and GA + B vs GA only. Endpoints included all-cause and ophthalmic condition-related healthcare resource utilization (HRU), injurious falls, and healthcare costs. HRU and injurious falls were assessed per-person-per-year and per 100 person-years, respectively. Cohorts were compared using rate ratios, 95% confidence intervals (CIs), and p-values from weighted Poisson regression models. Healthcare costs were evaluated per-person-per-year using mean cost differences, 95% CIs, and p-values from weighted linear regression.
Results: The study included 18,119 patients with GA only, 2,285 with GA + VI, 1,716 with GA + B, and 72,476 patients without GA. Higher rates of all-cause hospitalizations (RR [95% CI]: 1.08 [1.03, 1.12]), outpatient visits (1.08 [1.05, 1.10]), other visits (1.14 [1.08, 1.21]), and falls with head injuries (1.24 [1.05, 1.45]) were observed in patients with GA vs without GA (P< 0.05). GA was associated with higher annual all-cause total healthcare costs, spending an average of $1,171 more after adjustment (P< 0.05). Progression to GA + VI and GA + B was associated with a more pronounced burden.
Conclusion: The clinical and economic burden of GA is substantial and escalates as the disease advances. These findings suggest early intervention aimed at slowing GA progression may help to mitigate the healthcare burden associated with advancement of GA to visual impairment and blindness.
Keywords: geographic atrophy, economic burden, claims data, retrospective, visual impairment, blindness
A Letter to the Editor has been published for this article.
Introduction
Geographic atrophy (GA) is one of two advanced forms of age-related macular degeneration (AMD), an ophthalmic condition that is the leading cause of vision loss among older adults.1,2 In the United States (US), an estimated 20 million individuals have AMD, while roughly one million are affected by GA.3 By 50 years of age, the prevalence of GA increases 4-fold with every decade of life, reaching 2.91% in adults aged 80 years.4 Given the current aging population, the prevalence of GA is expected to rise in the future.2,5
GA is characterized by irreversible loss of retinal pigment epithelium, photoreceptors and choriocapillaris,6,7 which in turn contributes to visual impairment (VI) and blindness over time.8 GA and its progression to VI and blindness are associated with a considerable humanistic and clinical burden. Patients with GA tend to report poor vision-related and overall quality of life compared to aged-matched peers without GA, including declines in social functioning and mental health.8–12 Personal safety, such as the risk of falls or injury, is often a major concern reported among patients with GA.9–11 Indeed, the annual prevalence of falls among individuals aged ≥65 years with VI and blindness was approximately 60% in 2014, nearly double the prevalence of falls among those without VI and blindness.13
Evidence suggests that VI and blindness due to ophthalmic conditions, such as GA, may also pose considerable economic burden on healthcare systems. Hospitalizations, medical services for diagnosis and treatment, and care for falls, injuries, and other accidents attributed to VI and blindness result in high direct healthcare costs.9,11,14–17 Although GA is one of the most common causes of VI and blindness, few studies have assessed its economic impact on the healthcare system and payers.9,10,18,19 Accordingly, this study evaluated the healthcare resource utilization (HRU), rate of injurious falls, and healthcare costs among elderly patients with GA relative to those without GA in the US. Further, this study assessed the incremental burden associated with VI or blindness among patients with GA.
Material and Methods
Data Source
Optum Clinformatics Data Mart (CDM) is a database with 15–19 million annual lives of UnitedHealth Group members in all US census regions and includes Medicare Advantage health plan data. The database includes historical data on patient demographics, dates of eligibility and death, claims for medical and pharmacy services, costs of services, and laboratory tests and results. A subset of the Optum CDM database spanning from January 1, 2016 to September 30, 2021 was used in this study. As data were de-identified and complied with the patient requirements of the Health Insurance Portability and Accountability Act of 1996, no institutional review board approval or exemption was required.
Study Design
A longitudinal, retrospective cohort design was used (Supplementary Figure 1). The study was comprised of four mutually exclusive cohorts based on patients’ diagnoses: (1) patients with GA only, (2) patients with GA and VI (GA + VI), (3) patients with GA and blindness (GA + B), and (4) patients with no GA, identified using the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) diagnosis codes (Supplementary Table 1). Comparisons were made between the GA only and no GA cohorts, the GA + VI and GA only cohorts, and the GA + B and GA only cohorts.
For the cohorts with GA only and no GA, the index date was defined as the date occurring 12 months after the start of eligibility. For the GA + VI and GA + B cohorts, the index date was the later of either 12 months after the start of eligibility or the first diagnosis date of VI or blindness, respectively. For all cohorts, patient demographics and clinical characteristics were assessed during the baseline period defined as the 12 months prior to the index date. Study outcomes were assessed during the follow-up period defined as the time from the index date until the earliest of end of continuous healthcare plan enrollment, end of data availability, or death.
Study Population
The three GA cohorts were required to have at least one medical claim with a diagnosis of GA within the first 12 months of patients’ eligibility between January 1, 2016 and September 30, 2021. Patients in the GA + VI and GA + B cohorts were required to have at least one medical claim with a diagnosis of VI and blindness, respectively, after the onset of GA. Patients in the no GA cohort were selected from a random sample of 9,498,776 patients in the Optum CDM Database and had no medical claims with a diagnosis of GA anytime during the study period. Moreover, patients in the no GA cohort who had at least one medical claim with a diagnosis for VI or blindness prior to the index date were excluded. On the index date, all patients were required to be 65 years or older and have Medicare Advantage insurance coverage.
Study Outcomes
Study outcomes were measured during the follow-up period and included HRU, injurious falls, and healthcare costs. All-cause and ophthalmic condition-related HRU outcomes were evaluated, including frequency of hospitalizations, length of stay for hospitalizations, emergency room (ER) visits, outpatient (OP) visits, and other visits. A medical service claim was considered ophthalmic condition-related if it was associated with an ICD-10-CM diagnosis code for an ophthalmic condition (Supplementary Table 1). All-cause and ophthalmic condition-related injurious falls included falls associated with fractures, joint dislocations, and head injuries. Injurious fall outcomes were defined as a medical claim for a fall followed by an injurious event claim for fractures, joint dislocations, or head injuries within 30 days after the fall. All-cause and ophthalmic condition-related costs included total healthcare costs, stratified by medical costs (ie, hospitalizations, ER visits, OP visits, and other visits costs), and pharmacy costs. Ophthalmic condition-related pharmacy costs included dispensings for anti-vascular endothelial growth factor (anti-VEGF) injections, prostaglandin analogs, rho kinase inhibitors, nitric oxides, miotic/cholinergic agents, and other prescription eye drops.
Statistical Analysis
Patient demographics and clinical characteristics were reported using descriptive statistics, including mean, standard deviation, and median for continuous variables and frequencies and proportions for categorical variables. Differences in baseline characteristics were assessed using standardized differences between each comparator cohort, with a standardized difference >10% indicating meaningful imbalance between cohorts.20 Cohorts were weighted using inverse probability of treatment weighting (IPTW) to balance baseline patient characteristics and control for potential confounding between each comparison. Baseline characteristics were reported for both the unweighted and weighted cohorts to determine if meaningful imbalances (ie, standardized difference >10%) were well-balanced after weighting.
The IPTW approach uses weights derived from the propensity score (PS) to create a pseudo-population where the distribution of covariates in the population are independent of diagnosis and allowing for the estimation of an unconfounded average effect across the entire population. In this study, IPTW weights were calculated separately for each comparison and then used in the respective analyses. Therefore, weighted outcomes for the GA only cohort across comparisons vary due to differences in the weights used for each comparison. The following observable patient demographics and clinical characteristics were included in the PS calculation to derive the IPTW weights: age, sex, region, race, year of index date, Quan-Charlson Comorbidity Index (CCI), frailty index, baseline HRU and costs, and comorbidities (ie, Elixhauser, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [DSM-V], and select ophthalmic-related comorbidities) with prevalence ≥5% observed in the study population. Baseline characteristics that remained imbalanced after IPTW were added to the regression models as needed to control for residual confounding, to the extent that confounding factors were observable and recorded in the data.
Rates of HRU per person-year (PPY) were calculated as the total number of visits during follow-up divided by the total person-years of follow-up. Cohorts were compared using rate ratios, 95% confidence intervals (CIs) and p-values estimated from weighted Poisson regression models with robust variance estimators. Rates of injurious falls were reported per 100 person-years during follow-up and compared using rate ratios, 95% CIs, and p-values estimated from weighted Poisson regression models with robust variance estimators. Mean healthcare costs per-person-per-year (PPPY) were calculated by dividing the costs incurred over follow-up by the person-years of observation. Cohorts were compared using mean cost differences, 95% CIs, and p-values estimated from weighted linear regression models with robust variance estimators. Costs were inflation-adjusted to 2021 US dollars using the medical care component of the Consumer Price Index.
Results
Study Population
After applying all eligibility criteria to the GA population, the study included 18,119 patients with GA only, 2,285 with GA + VI, and 1,716 with GA + B. Among 4,357,140 patients eligible for the no GA cohort, 72,476 patients were randomly selected at four times the size of the GA only cohort as to not overpower the study when comparing patients with GA only to those with no GA (Supplementary Figure 2).
Baseline Characteristics
Unweighted patient demographics and clinical characteristics are presented in Table 1. Across the three GA cohorts, mean age ranged from 82.0–84.7 years, 67.2–71.7% were female, and over a third of patients were from the South (35.6–37.2%). Patients in the no GA cohort were 73.7 years of age on average, 59.1% female, and 41.3% were from the South.
 |
Table 1 Baseline Patient Demographics and Clinical Characteristics |
The top two Elixhauser comorbidities in the three GA cohorts were hypertension (81.2–87.5%) and cardiac arrhythmia (33.6–45.9%), followed by hypothyroidism (30.3%) among GA only patients and peripheral vascular disorders (36.4% and 39.9%, respectively) among the GA + VI and GA + B cohorts. In the no GA cohort, the top three Elixhauser comorbidities were hypertension (70.0%), diabetes (32.4%) and hypothyroidism (20.9%). Hyperlipidemia was the most common ophthalmic-related comorbidity across all cohorts (67.6–70.7%), followed by osteoarthritis (27.7–44.2%), and unstable angina (19.9–46.2%).
The mean number of injurious falls during the baseline period ranged from 0.28–0.57 across the three GA cohorts and was 0.10 in the no GA cohort. Across all cohorts, the mean number of all-cause HRU visits during the 12-month baseline period was primarily driven by OP visits (15.43–22.46) and other visits (3.35–15.23). Mean all-cause total healthcare costs during the 12-month baseline period ranged from $26,560–$42,954 across the three GA cohorts, driven primarily by hospitalization costs and OP visit costs. Patients with no GA had mean all-cause total healthcare costs of $20,684.
After weighting, nearly all patient demographics and clinical characteristics were well balanced between comparator cohorts (Supplementary Table 2A−C).
HRU During Follow-Up
Weighted all-cause and ophthalmic condition-related HRU are presented in Figure 1A and 1B, respectively. Patients with GA only had more all-cause HRU PPY than those with no GA, including 1.08 (95% CI: 1.03, 1.12) times more hospitalizations and OP visits (95% CI: 1.05, 1.10; both P<0.05) as well as 1.14 (95% CI: 1.08, 1.21) times more other visits. With the added burden of VI, patients with GA + VI used more all-cause and ophthalmic condition-related healthcare resources PPY than those with GA only. Specifically, patients with GA + VI had higher rates of hospitalizations, ER visits, and other visits than patients with GA only (all P<0.05), with the largest differences observed for ophthalmic condition-related ER visits (adjusted RR: 1.71; 95% CI: 1.03, 2.85), hospitalizations (adjusted RR: 1.70; 95% CI: 1.32, 2.18), and other visits (adjusted RR: 1.93; 95% CI: 1.47, 2.54). Patients with GA + B had higher rates of all-cause and ophthalmic condition-related hospitalizations, ER visits, and other visits PPY than patients with GA only (all P<0.05), with 2.88 (95% CI: 2.14, 3.86) times more ophthalmic condition-related hospitalizations, 1.74 (95% CI: 1.14, 2.66) times more ophthalmic condition-related ER visits, and 2.41 (95% CI: 1.90, 3.05) times more ophthalmic condition-related other visits.
 |
Figure 1 HRU During Follow-Up of GA Subgroups – Weighted Analysisa (A) All-Cause HRU. (B) Ophthalmic Condition-Related HRU. * P<0.05. Abbreviations: B, blindness; CI, confidence interval; DSM-V, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; ER, emergency room; GA, geographic atrophy; HRU, healthcare resource utilization; IPTW, inverse probability of treatment weighting; Quan-CCI: Quan-Charlson Comorbidity Index; RR, rate ratio; VI, visual impairment. Note: a Cohorts were weighted using the IPTW approach based on the propensity score. Variables used in the propensity score calculation included: age, sex, region, race, year of index date, Quan-CCI score, frailty indicator score, and comorbidities (ie, Elixhauser and DSM-V comorbidities, selected ophthalmic-related comorbidities) with prevalence ≥5%. Each subgroup analysis included an IPTW calculation independent of the other analyses. |
Injurious Falls During Follow-Up
Weighted all-cause and ophthalmic condition-related injurious falls are presented in Figure 2A and 2B, respectively. Although the overall rate of all-cause injurious falls per 100 person-years did not differ meaningfully between patients with GA only and those with no GA (P=0.122), patients with GA only had 1.24 (95% CI: 1.05, 1.45) times more all-cause falls with head injuries and 0.67 (95% CI: 0.51, 0.89) times fewer all-cause falls with joint dislocations per 100 person-years compared to patients with no GA (both P<0.05). The rate of ophthalmic condition-related injurious falls per 100 person-years trended higher for patients with GA + VI compared to patients with GA only (adjusted RR: 2.33; 95% CI: 1.36, 3.98; P=0.002), driven by 6.82 (95% CI: 2.19, 21.27) times more injurious falls with joint dislocations per 100 person-years (P<0.05).
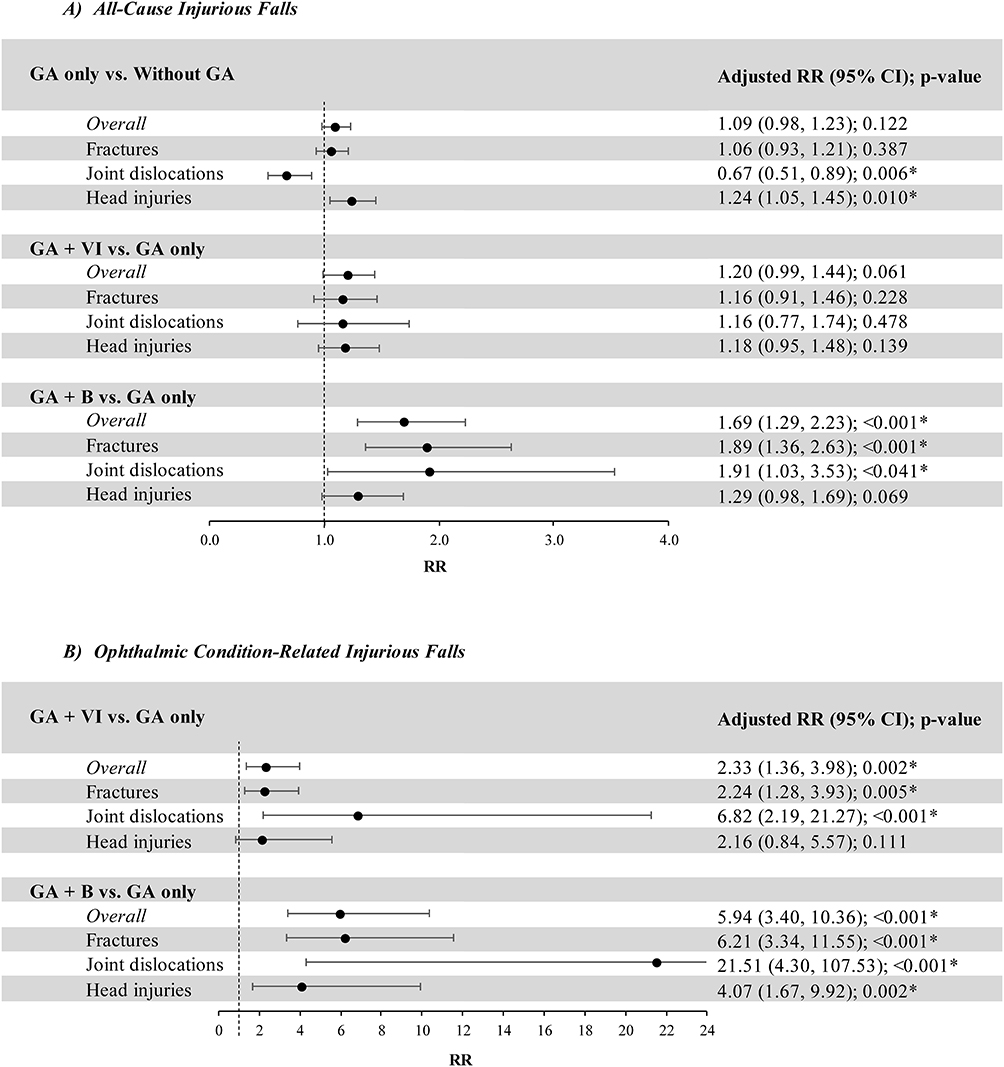 |
Figure 2 Injurious Falls During Follow-Up of GA Subgroups – Weighted Analysisa (A) All-Cause Injurious Falls. (B) Ophthalmic Condition-Related Injurious Falls. * P<0.05. Abbreviations: B, blindness; CI, confidence interval; DSM-V, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; GA, geographic atrophy; IPTW, inverse probability of treatment weighting; Quan-CCI: Quan-Charlson Comorbidity Index; RR, rate ratio; VI, visual impairment. Note: a Cohorts were weighted using the IPTW approach based on the propensity score. Variables used in the propensity score calculation included: age, sex, region, race, year of index date, Quan-CCI score, frailty indicator score, and comorbidities (ie, Elixhauser and DSM-V comorbidities, selected ophthalmic-related comorbidities) with prevalence ≥5%. Each subgroup analysis included an IPTW calculation independent of the other analyses. |
Patients with GA + B had higher rates of both all-cause and ophthalmic condition-related injurious falls, with 1.69 (95% CI: 1.29, 2.23) times more all-cause injurious falls per 100 person-years and 5.94 (95% CI: 3.40, 10.36) times more ophthalmic condition-related injurious falls per 100 person-years than patients with GA only (both P<0.05). Differences between cohorts were primarily driven by ophthalmic condition-related injurious falls involving joint dislocations (adjusted RR: 21.51; 95% CI: 4.30, 107.53) and fractures (adjusted RR: 6.21; 95% CI: 3.34, 11.55).
Healthcare Costs During Follow-Up
Weighted all-cause and ophthalmic condition-related healthcare costs are presented in Figure 3. Patients with GA only incurred higher annual all-cause total healthcare costs compared to patients with no GA ($26,696 vs $25,524), spending an average of $1,171 (95% CI: 204, 2,138) more per year (P=0.018). The difference in all-cause total healthcare costs was primarily driven by higher annual OP visit costs ($10,706 vs $9,996; adjusted cost difference: $740; 95% CI: 194, 1,286; P=0.008).
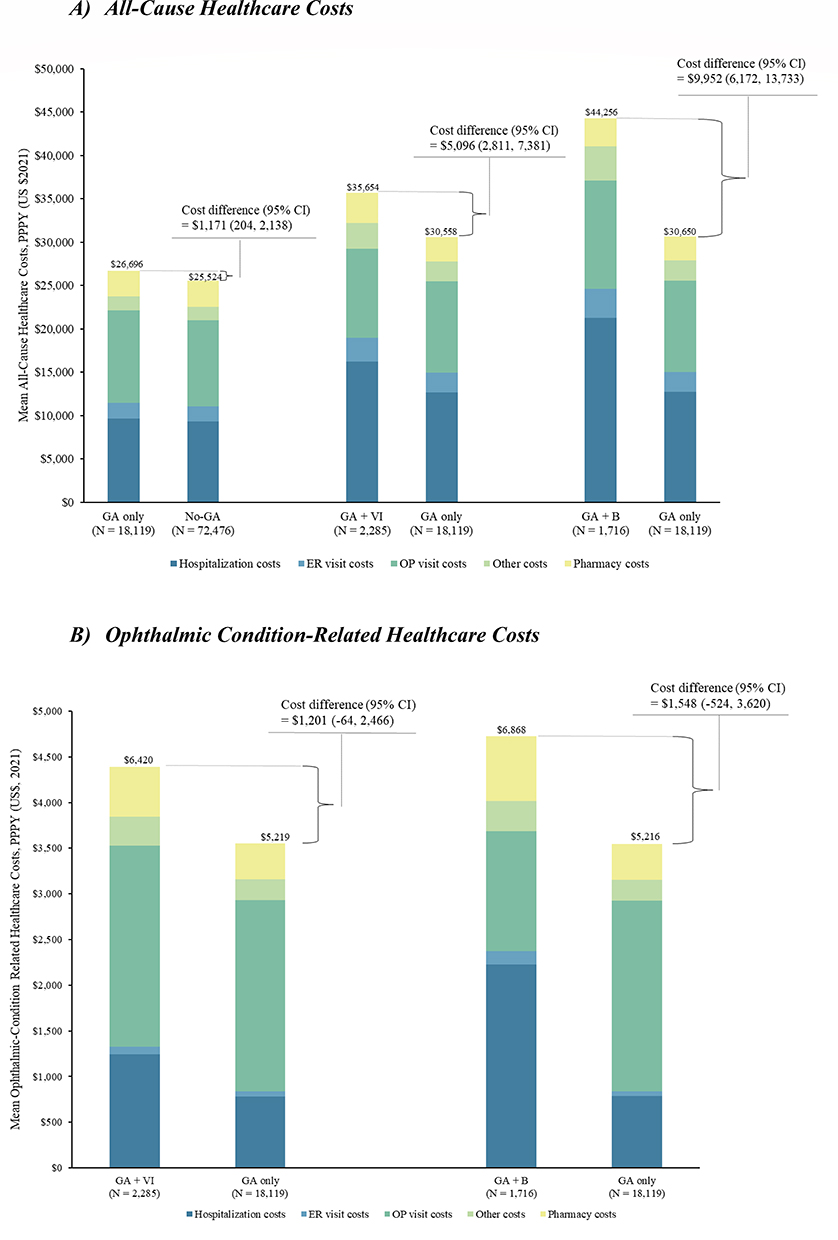 |
Figure 3 Healthcare Costs During Follow-Up of GA Subgroups – Weighted Analysisa (A) All-Cause Healthcare Costs. (B) Ophthalmic Condition-Related Healthcare Costs. Abbreviations: B, blindness; CI, confidence interval; DSM-V, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; ER, emergency room; GA, geographic atrophy; IPTW, inverse probability of treatment weighting; OP, outpatient; PPPY, per-person-per-year; Quan-CCI. Quan-Charlson Comorbidity Index; US, United States; VI, visual impairment. Note: a Cohorts were weighted using the IPTW approach based on the propensity score. Variables used in the propensity score calculation included: age, sex, region, race, year of index date, Quan-CCI score, frailty indicator score, and comorbidities (ie, Elixhauser and DSM-V comorbidities, selected ophthalmic-related comorbidities) with prevalence ≥5%. Each subgroup analysis included an IPTW calculation independent of the other analyses. |
Compared to patients with GA only, patients with GA + VI incurred higher all-cause total healthcare costs ($35,654 vs $30,558), spending an average of $5,096 (95% CI: 2,811, 7,381) more per year (P<0.001). The difference in all-cause total healthcare costs was primarily driven by annual hospitalization costs ($16,245 vs $12,686), with an adjusted cost difference of $3,559 (95% CI: 1,997, 5,121; P<0.001). Moreover, patients with GA + VI incurred higher annual ophthalmic condition-related hospitalization costs ($1,241 vs $783; adjusted cost difference: $458; 95% CI: 131, 786) and pharmacy costs ($543 vs $393; adjusted cost difference: $151; 95% CI: 14, 287; both P<0.05).
With the additional burden of blindness, patients with GA + B spent an average of $9,952 (95% CI: 6,172, 13,733) more per year in all-cause total healthcare costs compared to patients with GA only (P<0.001). The difference in all-cause total healthcare costs was primarily driven by annual hospitalization costs ($21,289 vs $12,758), which comprised 65% (adjusted cost difference: $6,463; 95% CI: 4,267, 8,659) of the adjusted cost difference. Annual all-cause ER visit costs (adjusted cost difference: $850; 95% CI: 432, 1,269) and other visit costs (adjusted cost difference: $904; 95% CI: 595, 1,213) were also higher in patients with GA + B compared to patients with GA only (P<0.001). Ophthalmic condition-related medical costs were higher in patients with GA + B compared to patients with GA only, spending an additional $897 (95% CI: 98, 1,696) per year. Annual ophthalmic condition-related hospitalization (adjusted cost difference: $1,341; 95% CI: 822, 1,861) and pharmacy costs (adjusted cost difference: $306; 95% CI: 165, 447) drove this cost difference (both P<0.001). Ophthalmic condition-related OP visit costs were lower in patients with GA + B than those with GA only, spending $610 (95% CI: –932, –289) less per year (P<0.001).
Discussion
Although the progression of GA to irreversible loss of vision and its significant impairment on quality of life are well understood,4,21 evidence on the clinical and economic impact of GA is limited. In this real-world study, we evaluated HRU, injurious falls, and healthcare costs associated with GA among elderly patients enrolled in Medicare Advantage plans in the US. Our findings suggest that, compared to patients without GA, patients with GA only used more healthcare resources, had more falls associated with head injuries, and incurred higher healthcare costs. Progression to VI and blindness was associated with a more pronounced burden, as evidenced by higher rates of HRU and ophthalmic-related injurious falls, as well as higher healthcare costs in patients with GA + VI or GA + B than in patients with GA only. Altogether, GA is associated with substantial clinical and economic burden that grows incrementally as the disease advances.
These results add to existing evidence on the healthcare burden associated with GA.9,10,19 In a retrospective analysis using administrative claims data, mean all-cause total healthcare costs were $11,672 in 2020 US dollars for patients with incident GA during the first year following diagnosis.19 Although not directly comparable, mean all-cause total healthcare costs in the present study ranged from $26,696–$44,256 PPPY among patients with incident or prevalent GA, highlighting the economic consequences associated with long-term GA management. Moreover, in a cross-sectional cohort study of patients with GA residing outside of the US, average ophthalmic condition-related healthcare costs were $2,115 PPPY.10 This value is lower than the ophthalmic condition-related healthcare costs observed in US patients in the current analysis (GA + VI: $6,420; GA + B: $6,868), though these differences may be driven by both the inclusion of patients with more advanced GA in the present study, as well as the use of country-specific unit cost estimates in the previous analysis.
Prior research has identified an increased risk of hip fractures among both Medicare patients with GA9 and patients with unilateral GA without subfoveal involvement22 compared to either patients without AMD9 or patients with early/intermediate AMD, respectively. In the present study, the increased rate of all-cause injurious falls with fractures among patients with GA only versus no GA did not attain statistical significance. Nevertheless, the trends observed are similar to prior literature and shed light on the substantial resource use and costs incurred by patients with GA.
Evidence on the economic impact of GA progression to VI or blindness on the healthcare system and payers is limited. Existing literature evaluating the economic burden associated with increasing levels of GA severity and laterality report varied results.18,19, In this study, the increased HRU and costs observed among patients with GA and VI or blindness relative to those with GA only indicate an increasing burden associated with the advancement of GA. Moreover, although not directly compared, the numerically higher rates of HRU, rates of injurious falls, and healthcare costs observed among patients with GA + B relative to those with GA + VI highlight an incremental burden associated with the progression of GA with VI to GA with blindness.
Together, these findings signal an important need to delay the onset of VI and blindness among patients with GA, potentially through new and improved treatment options that can help alleviate the sizable burden on patients and caregivers, as well as on the healthcare system and its payers. Historically, the lack of approved medications for the treatment of GA posed a considerable challenge for patient care, given the debilitating nature of this disease.8 Given the evolving treatment landscape, the present real-world findings may help key stakeholders address the unmet needs of patients with GA and inform future cost/benefit analyses of novel treatments, given the potential burden associated with administration or complications of novel GA treatments.
The present study was subject to certain limitations. First, only injurious falls that required medical care were accounted for in the study. Other types of fall-related injuries, such as soft tissue injuries or hematomas, may be under-detected or under-recorded in billing claims. In addition, medical claims with injurious events occurring within 30 days of a fall were assumed to be related to the same event. As such, the rate of injurious falls may be overestimated. Second, ophthalmic condition-related HRU, injurious falls, and healthcare costs reported in this study included, but were not limited to, healthcare services for GA. As such, HRU, injurious falls, and healthcare costs associated with GA specifically may be lower. Third, as this study was observational in nature, confounding adjustments could only account for factors that were observable and recorded in the database. Thus, residual confounding may remain. Fourth, the study population and endpoints were identified using administrative claims data, which contain information on diagnoses and procedures for reimbursement purposes. As such, there is the potential for misclassification of patients with GA as well as uncertainty in the estimation of endpoints due to misspecification of diagnosis, procedure, or drug codes. Additionally, assessment of unilateral versus bilateral visual loss and assessment of GA severity, including proximity to the fovea and size of the area affected, was not available due to the confines of diagnostic coding. Fifth, this study evaluated multiple endpoints, which may have resulted in potential inflation of the type I error rate. As no adjustment for multiplicity was conducted for this study, results should be considered exploratory. Finally, given that the study population consisted of Medicare Advantage-insured patients in the US, the present study findings may not be generalizable to the broader population of patients with GA.
Despite these limitations, this study has several key strengths. This study helps fill gaps in the literature related to the real-world clinical and economic burden associated with the progression of GA to VI and blindness in an elderly US population, which is particularly relevant given the projected increase in incidence with the aging population. Further, the Optum CDM database used in this study is geographically diverse and representative of the national Medicare Advantage population in the US, allowing for the study results to be generalizable to this real-world population.
The results of this real-world study indicate that patients with GA experience large disease burden, including high rates of HRU and injurious falls, along with higher average healthcare costs compared to patients without GA. This burden is further increased by progression to VI or blindness. These findings suggest that initiating treatments aimed at slowing GA progression early in the disease course could reduce the healthcare burden associated with the development of GA into VI and blindness. Future studies could provide additional insight by investigating the incidence of VI, blindness, and injurious falls among patients with GA compared to patients with no GA to further delineate the clinical implications of this prevalent ophthalmic condition.
Data Sharing Statement
The data that support the findings of this study are available from Optum Clinformatics Data Mart. Restrictions apply to the availability of these data, which were used under license for this study.
Ethics Statement
Data were de-identified and comply with the patient requirements of the Health Insurance Portability and Accountability Act (HIPAA) of 1996; therefore, no review by an institutional review board was required per Title 45 of CFR, Part 46.101(b)(4) (https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/#46.101).
Acknowledgments
Medical writing assistance was provided by professional medical writer, Molly Gingrich, an employee of Analysis Group, Inc., a consulting company that has provided paid consulting services to Apellis Pharmaceuticals. These results have previously been presented at the Academy of Managed Care Pharmacy (AMCP) Nexus Meeting, October 16–19, 2023, in Orlando, FL and the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Annual Meeting, May 7–10, 2023 in Boston, MA.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Apellis Pharmaceuticals. The sponsor participated in the design of the study, interpretation of the data, and review and approval of the manuscript.
Disclosure
SS and RL are employees of Apellis Pharmaceuticals and own stock/stock options. GG, MM, JK, WC, and MSD are employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Apellis Pharmaceuticals, which funded the development and conduct of this study and manuscript. The authors report no other conflicts of interest in this work.
References
1. Thomas CJ, Mirza RG, Gill MK. Age-Related Macular Degeneration. Med Clin North Am. 2021;105(3):473–491. doi:10.1016/j.mcna.2021.01.003
2. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–16. doi:10.1016/S2214-109X(13)70145-1
3. Centers for Disease Control and Prevention. Prevalence of Age-Related Macular Degeneration (AMD).
4. Rudnicka AR, Jarrar Z, Wormald R, Cook DG, Fletcher A, Owen CG. Age and gender variations in age-related macular degeneration prevalence in populations of European ancestry: a meta-analysis. Ophthalmology. 2012;119(3):571–580. doi:10.1016/j.ophtha.2011.09.027
5. Varma R, Vajaranant TS, Burkemper B, et al. Visual impairment and blindness in adults in the United States: demographic and geographic variations from 2015 to 2050. JAMA Ophthalmol. 2016;134(7):802–809. doi:10.1001/jamaophthalmol.2016.1284
6. Boyer DS, Schmidt-Erfurth U, van Lookeren Campagne M, Henry EC, Brittain C. The Pathophysiology Of Geographic Atrophy Secondary To Age-Related Macular Degeneration And The Complement Pathway As A Therapeutic Target. Retina. 2017;37(5):819–835. doi:10.1097/iae.0000000000001392
7. Holz FG, Strauss EC, Schmitz-Valckenberg S, van Lookeren Campagne M. Geographic atrophy: clinical features and potential therapeutic approaches. Ophthalmology. 2014;121(5):1079–1091. doi:10.1016/j.ophtha.2013.11.023
8. Chakravarthy U, Bailey CC, Johnston RL, et al. Characterizing Disease Burden and Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration. Ophthalmology. 2018;125(6):842–849. doi:10.1016/j.ophtha.2017.11.036
9. Sarda SP, Heyes A, Bektas M, et al. Humanistic and Economic Burden of Geographic Atrophy: a Systematic Literature Review. Clinical Ophth. 2021;15:4629–4644. doi:10.2147/opth.S338253
10. Patel PJ, Ziemssen F, Ng E, et al. Burden of Illness in Geographic Atrophy: a Study of Vision-Related Quality of Life and Health Care Resource Use. Clin Ophthalmol. 2020;14:15–28. doi:10.2147/opth.S226425
11. Jones D, Nielsen J, Altman D, et al. MOSAIC: a qualitative study of the clinical, humanistic, and financial burden of geographic atrophy (GA) among patients. Invest Ophthalmol Visual Sci. 2022;63(7):4217–A0145.
12. Orr SC, Pierson R, Bogert J, et al. Disease burden associated with geographic atrophy secondary to age-related macular degeneration. Invest Ophthalmol Visual Sci. 2016;57(12):21.
13. Crews JE, Chou CF, Stevens JA, Saaddine JB. Falls Among Persons Aged ≥65 Years With and Without Severe Vision Impairment - United States, 2014. MMWR Morb Mortal Wkly Rep. 2016;65(17):433–437. doi:10.15585/mmwr.mm6517a2
14. Wittenborn JS, Zhang X, Feagan CW, et al. The economic burden of vision loss and eye disorders among the United States population younger than 40 years. Ophthalmology. 2013;120(9):1728–1735. doi:10.1016/j.ophtha.2013.01.068
15. Koberlein J, Beifus K, Schaffert C, Finger RP. The economic burden of visual impairment and blindness: a systematic review. BMJ Open. 2013;3(11):e003471. doi:10.1136/bmjopen-2013-003471
16. Rein DB, Zhang P, Wirth KE, et al. The Economic Burden of Major Adult Visual Disorders in the United States. Arch Ophth. 2006;124(12):1754–1760. doi:10.1001/archopht.124.12.1754
17. Javitt JC, Zhou Z, Willke RJ. Association between vision loss and higher medical care costs in Medicare beneficiaries costs are greater for those with progressive vision loss. Ophthalmology. 2007;114(2):238–245. doi:10.1016/j.ophtha.2006.07.054
18. Chakravarthy U, Bailey CC, Scanlon PH, et al. Direct Ophthalmic Healthcare Resource Use among Patients with Geographic Atrophy in a Large Cohort from the United Kingdom. Ophthalmol Retina. 2019;3(11):920–926. doi:10.1016/j.oret.2019.06.012
19. Kim A, Devine B, Campbell J, Shirneshan E, Zhao C, Bansal A. Healthcare Resource Utilization and Costs in Patients with Geographic Atrophy Secondary to Age-Related Macular Degeneration. Clinical Ophth. 2021;15:2643–2651. doi:10.2147/opth.S307603
20. Austin PC. Goodness-of-fit diagnostics for the propensity score model when estimating treatment effects using covariate adjustment with the propensity score. Pharmacoepidemiol Drug Saf. 2008;17(12):1202–1217. doi:10.1002/pds.1673
21. Sacconi R, Corbelli E, Querques L, Bandello F, Querques G. A Review of Current and Future Management of Geographic Atrophy. Ophthalmol Ther. 2017;6(1):69–77. doi:10.1007/s40123-017-0086-6
22. Kim A, Shirnashen E, Campbell J, Devine B, Bansal A. Pss12 Characterizing The Healthcare Resource Utilization And Costs In Patients With Geographic Atrophy Secondary To Age-Related Macular Degeneration Stratified By Disease Severity. Value Health. 2020;23:S364. doi:10.1016/j.jval.2020.04.1400
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.