")
Back to Journals » Journal of Inflammation Research » Volume 17
Red Blood Cell Distribution Width Predicts Mortality in Hospitalized Patients with Severe Fever with Thrombocytopenia Syndrome
Authors Zhang S, Zhang Q , Wang J, Pan Y, Zhang Z, Geng Y, Jia B, Tian B , Xiong Y, Yan X, Li J, Wang H, Huang R, Wu C
Received 12 March 2024
Accepted for publication 11 July 2024
Published 22 July 2024 Volume 2024:17 Pages 4895—4904
DOI https://doi.org/10.2147/JIR.S468388
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Shaoqiu Zhang,1,* Qun Zhang,2,* Jian Wang,1,3,* Yifan Pan,4 Zhiyi Zhang,5 Yu Geng,1 Bei Jia,1 Bing Tian,2 Yali Xiong,1 Xiaomin Yan,1 Jie Li,1,3– 5 Huali Wang,6 Rui Huang,1,3– 5 Chao Wu1,3– 5
1Department of Infectious Diseases, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China; 2Department of Infectious Diseases, Affiliated Zhongda Hospital of Southeast University, Nanjing, Jiangsu, People’s Republic of China; 3Institute of Viruses and Infectious Diseases, Nanjing University, Nanjing, Jiangsu, People’s Republic of China; 4Department of Infectious Diseases, Nanjing Drum Tower Hospital Clinical College of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 5Department of Infectious Diseases, Nanjing Drum Tower Hospital Clinical College of Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China; 6Department of General Practice, Nanjing Second Hospital, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Wu; Rui Huang, Department of Infectious Diseases, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, No. 321 Zhongshan Road, Nanjing, Jiangsu, 210008, People’s Republic of China, Tel +86-25-83105890, Fax +86-25-83307115, Email [email protected]; [email protected]
Background: Severe fever with thrombocytopenia syndrome (SFTS) is an emerging epidemic infectious disease with high mortality rate. This study aimed to investigate the association of red blood cell distribution width (RDW) and mortality risk in hospitalized SFTS patients.
Methods: Clinical data of SFTS patients was retrospectively collected from three hospitals between October 2010 and August 2022. Cox proportional hazards model was used to identity the risk factors for fatal outcome. The predictive value of RDW for fatal outcome was evaluated by the receiver operating characteristic (ROC) analysis and Kaplan–Meier methods.
Results: Of 292 patients, the median age was 61.5 years. Non-survivors showed higher RDW value than survivors (13.6% vs.13.0%, P < 0.001). The mortality rate was 44.8% in patients with elevated RDW compared to 18.4% of patients with normal RDW, with a relative risk (RR) of 2.439. Elevated RDW was an independent risk factor of mortality (hazards ratio: 1.167, P = 0.019). Patients with elevated RDW had a higher cumulative mortality than patients with normal RDW. The area under the ROC curve (AUC) of RDW for the prediction of mortality was 0.690 (P < 0.001).
Conclusion: Elevated RDW was associated with higher mortality risk for patients hospitalized for SFTS. RDW may be helpful for risk stratification in SFTS patients.
Keywords: severe fever with thrombocytopenia syndrome, red blood cell distribution width, prognosis, survival
Introduction
Severe fever with thrombocytopenia syndrome (SFTS) is an emerging epidemic infectious disease caused by a novel bunyavirus (SFTS virus, SFTSV). It first emerged in China in 2010 with an estimated high mortality rate up to 30%1,2 and had later been reported in Korea,3 Japan,4 Thailand5 and the United States.6 Patients with SFTS mainly presented with fever, thrombocytopenia, leukocytopenia and other systemic symptoms including gastrointestinal, haemorrhagic, and neurological presentations.7–9 Among critically ill SFTS patients, the clinical symptoms typically deteriorate quickly within a week after symptom onset, and most patients died of multiorgan dysfunction.10 The widespread distribution and high mortality rate have made this novel disease a serious public health concern. Therefore, it is of vital importance for clinicians to distinguish patients in severe conditions as early as possible to avoid a fatal outcome. Previous studies have assessed many clinical and laboratory variables to be associated with mortality risk including older age, elevated level of blood urea nitrogen (BUN), viral load and the presence of neurological symptoms9,11–15 and have attempted to establish risk models for mortality prediction.16–20 However, there were still lack of consistent conclusions, and the significant risk factors for fatal outcome of SFTS patients remained to be determined.
Red blood cell distribution width (RDW) is a routine blood parameter in a conventional haemogram and it is used to identify anisocytosis combined with mean corpuscular volume (MCV).21,22 RDW reflects the volume differences between red blood cells (RBCs) as well as between individual RBC during its circulation of approximately 115 days.23 Previous studies have demonstrated the association of elevated RDW and high mortality rate in patients with influenza,24 sepsis,25 acute kidney injury,26 severe acute pancreatitis,27 and pulmonary disease,28 such as coronavirus disease 2019.29–31 It is speculated that pro-inflammatory state results in deficient and delayed erythropoiesis with variation of RBCs in structure and function, along with increased production and turnover of platelets and leukocytes.32 Although the specific mechanism for RDW increase during the process of these diseases remains unclear, numerous studies suggested that RDW is a practical indicator for the stratification of mortality risk among numerous acute diseases.31,33,34 However, the association of RDW with adverse prognosis in SFTS has not been well established. Therefore, this study aimed to investigate the association of RDW and mortality among patients with SFTS.
Methods
Design and Subjects
For this multi-center, retrospective cohort study, we collected clinical data of consecutive SFTS patients admitted to three hospitals (Nanjing Drum Tower Hospital, The Second Hospital of Nanjing, and Zhongda Hospital Southeast University) between October 2010 and August 2022.
Inclusion and Exclusion Criteria
Patients with laboratory-confirmed SFTSV infection were included in the study. The diagnosis of SFTSV infection was confirmed by at least one of the criteria as follows:9,35 (1) positive results of serum viral RNA, (2) seroconversion or a 4-fold or higher increase of antibody titers between two serum samples collected at an interval of more than two weeks, (3) isolation of SFTSV from cell culture. Those who were positive for other tick-borne pathogens or were not confirmed by laboratory examinations were excluded.9
Data Collection
The data analyzed were extracted from medical records using a structured data frame, including demographic information, underlying conditions, clinical manifestation and course, treatment regimens, and laboratory tests results. The primary outcome in our study was all-cause mortality. The follow-up time of survivor was calculated from the day of admission to discharge, and the duration of non-survivors was calculated from the day of admission to that of death.
Data Analysis
Continuous variables were described as median (interquartile range, IQR) for the skewed distribution of the data, and categorical variables were expressed as frequencies or proportions to compare the characteristics between survivors and non-survivors. We use Cox proportional hazards model to calculate the mortality hazards ratios (HRs) and 95% confidence interval (95% CI). Demographic characteristics and laboratory parameters were included in univariate analysis. Parameters with a P value < 0.05 were further included in the multivariate model. The Kaplan-Meier methods and Log rank tests were adopted to compare survival differences among patient groups stratified by RDW. An elevated RDW was defined as over 14.0%. A receiver operating characteristic (ROC) curve was constructed to evaluate the capacity of RDW for mortality prediction. Relative risks (RRs) of mortality for patients with an elevated RDW were calculated among different age groups.
We analyzed statistical differences between groups using a Pearson chi-square and Fisher’s exact test for proportions or frequencies and a two-sided Mann–Whitney U-test for medians. RRs were analyzed using modified Poisson regression. All statistical analysis were conducted with SPSS version 25.0 and all graphs were plot by RStudio version 4.2.1. P < 0.05 was considered as statistically significant.
Results
Baseline Characteristics of Patients
The study screened 307 hospitalized in-patients from three hospitals and finally included 292 patients diagnosed with SFTSV infection in the analysis (261 from Nanjing Drum Tower Hospital, 17 from The Second Hospital of Nanjing, and 14 from Zhongda Hospital Southeast University) (Figure S1). Out of which, 69 (23.6%) patients were deceased. The clinical features of study population are summarized in Table 1. Male patients represented 51.4% and the median age of the cohort was 61.5 (51.3–70.0) years. The median time from symptom onset to hospital admission was 7.0 (5.0,9.0) days, and the median length of hospital stay was 10.0 (7.0,14.0) days. The most common symptoms were fever (99.3%), anorexia (87.7%), feeble (80.1%) and diarrhea (45.9%). Non-survivors were older than survivors (67.0 years vs 59.0 years, P < 0.001). Symptoms were similar between survivors and non-survivors except for dyspnoea, headache and myalgias (P < 0.05). Non-survivors had higher median levels of blood urea nitrogen (BUN) (6.3 mmol/L vs 4.1 mmol/L, P < 0.001), lactate dehydrogenase (LDH) (1198.0 U/L vs 685.5 U/L, P < 0.001), creatinine (Cr) (80.0 μmol/L vs 59.0 μmol/L, P < 0.001), prothrombin time (PT) (12.3 s vs 11.2 s, P < 0.001) and activated partial thromboplastin time (APPT) (56.7 s vs 36.7 s, P < 0.001) than survivors. Nearly all patients had thrombocytopenia, leukopenia, or both. Comorbidities were comparable between survivors and non-survivors. The median level of RDW was 13.2% (IQR, [12.7%-13.9%]) at admission. Non-survivors had significantly higher RDW values (13.6%, IQR [13.1%-14.2%]) compared to survivors (13.0%, IQR [12.6%-13.7%], P < 0.001).
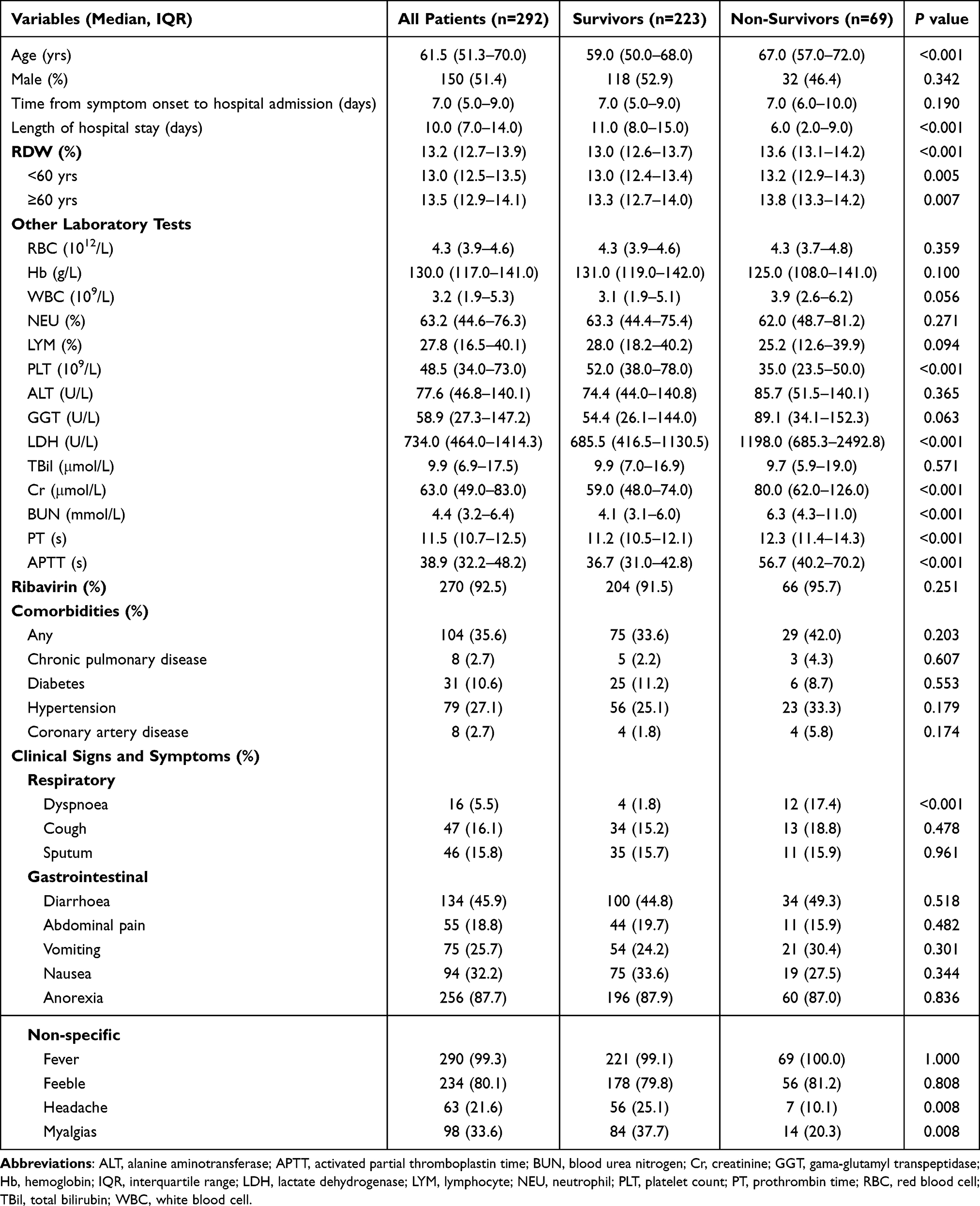 |
Table 1 Comparison of Clinical Characteristics Between Survivors and Non-Survivors |
Comparison of Mortality Risk Between Patients with Elevated RDW and Normal RDW
The mortality rate for patients with elevated RDW and normal RDW were 44.8% and 18.4% (P < 0.001), respectively. Those with an elevated RDW had a RR of 2.439 (95% CI, 1.647–3.614) for mortality compared to patients with normal RDW, and similar results were observed in both subgroups of age <60 years and ≥60 years (Table 2). The Kaplan-Meier analysis indicated that patients with elevated RDW had higher cumulative incidence of mortality than patients with normal RDW (Figure 1).
 |
Table 2 Mortality Rates Stratified by Age and Red Blood Cell Distribution Width Elevation at Admission |
 |
Figure 1 Elevated red blood cell distribution width at hospital admission and mortality among patients with SFTS. (A) Survival curve for the overall patients; (B) Survival curve for patients aged < 60 years; (C) Survival curve for patients aged ≥ 60 years. |
Association of RDW with Mortality
We developed Cox proportional hazards model to determine whether RDW was an independent risk factor of mortality. In the univariate analysis, age, WBC, RDW, PLT, ALT, LDH, Cr, BUN, PT, and APTT were associated with mortality. Further multivariate analysis revealed that RDW (HR 1.167, 95% CI 1.026–1.328, P = 0.019) remains an independent risk factor of mortality after adjusting for confounding factors (Table 3). We further investigated the independent risk factors of fatal outcome in different age subgroups. RDW value was identified as the independent risk factor of mortality both in patients aged <60 years (HR 1.530, 95% CI 1.005–2.329, P = 0.048) and aged ≥60 years (HR 1.184, 95% CI 1.027–1.366, P = 0.020) (Table S1). The APTT values were also independent risk factors of mortality. The AUC of RDW value for mortality prediction was 0.690 (95% CI: 0.623 to 0.756, P < 0.001, Figure 2). The optimal cut-off value of RDW was 13.1%, with a sensitivity of 79.9% and a specificity of 51.1%.
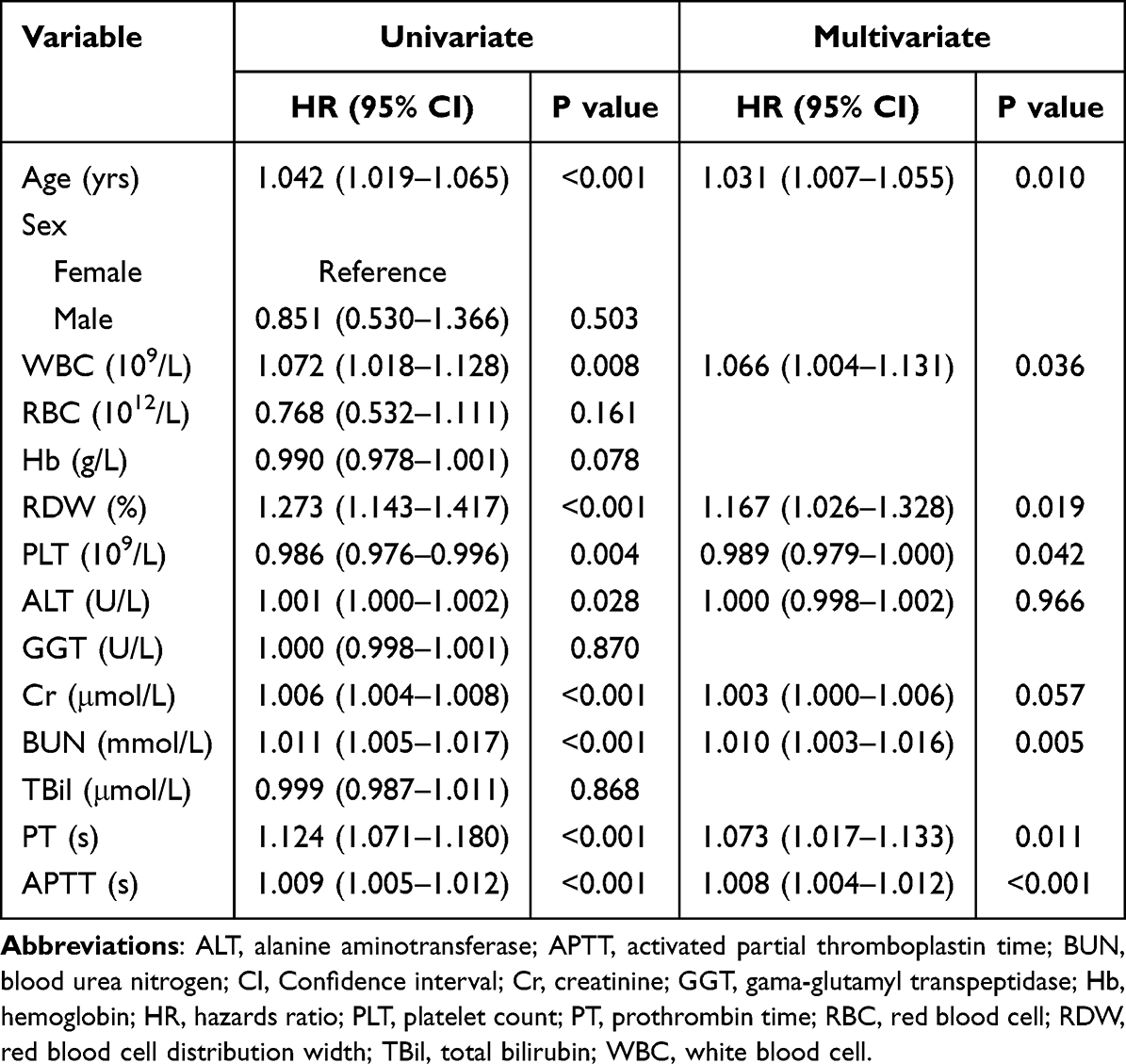 |
Table 3 Cox Proportional Hazards Modeling of Mortality Risk |
 |
Figure 2 Receiver operating characteristic curve analysis of the prediction of mortality by red blood cell distribution width. |
Dynamic Change of RDW and Mortality Risk During Hospitalization
We further investigated the relationship between changes of RDW after hospital admission and mortality risk. For patients with normal RDW at admission, non-survivors had an increasing RDW value whereas survivors had a stable value (Figure 3). Patients with initially elevated RDW who survived had a decreasing RDW. An increasing RDW value after admission was associated with elevated mortality risk. Figure 3 also shows that the mean levels of RDW in survivors was about 13.22%, compared to 13.96% in non-survivors. Non-survivors tend to have a higher level of RDW during hospitalization. The average RDW of non-survivors experienced an increase of 0.82% within the first 9 days after admission, whereas a decrease of 0.28% was found in survivors.
 |
Figure 3 Dynamic changes of red blood cell distribution width after admission among patients with SFTS. (A) The overall patients; (B) Patients with normal RDW at admission; (C) Patients with elevated RDW at admission; (D) A histogram of RDW change in survivors and non-survivors of SFTS during hospitalization. |
Discussion
In this multicenter study, we analyzed the association of RDW with clinical prognosis in hospitalized SFTS patients. The results suggested that non-surviving SFTS patients had higher RDW at admission and increasing RDW value during hospitalization. Moreover, elevated RDW was an independent predictor of mortality of SFTS patients during hospitalization.
The mortality rate of patients with SFTS was 23.6% in this study, which was similar to previous studies.3,9,20,36 We found a higher mortality risk in patients with SFTS who had older age and more commonly presented dyspnoea, headache and myalgias. Besides, there were significant differences in WBC, BUN, PLT, PT and APTT between survivors and non-survivors, which were also reported in previous studies.17,18,37–39 Among them, only PLT count was independently associated with mortality in SFTS patients, which is consistent with viral replication in substantial disease progression.11 High level of viral loads was reported to be independently associated with adverse outcome and was negatively correlated with PLT count.11,35,37 Both PLT and APTT are indicators for coagulation function, which play significant roles in hemorrhagic fever syndromes. The supportive treatment is mainly adopted for SFTS patients in clinical practice, including transfusion of blood products and intensive care for critically ill patients.7,8 Although antiviral therapy with ribavirin is clinically recommended, this study fails to find its efficiency in reducing case fatality.40,41
Some studies have reported the association of higher RDW with fatal outcomes in many diseases.24–31 Our study demonstrated that elevated RDW was associated with substantially increased mortality risk in patients with SFTS. The association remained statistically significant after adjustment for age and other serum parameters. RDW is a non-specific marker and elevated in many illnesses.24–31 The mechanisms of association between RDW and fatal outcome of SFTS remain unclear. Some studies showed an association between elevated RDW and severe inflammation as well as oxidative stress, with increased inflammatory cytokines detected.42–44 Serum SFTSV viral load was correlated with the inflammatory cytokines, and cytokine levels were further shown to correlate with laboratory parameters and clinical manifestation.11,45,46 It is speculated that a higher degree of inflammation and oxidation in non-survivors resulted in their fatal outcome. Further studies are needed to explore the association of increased RDW with oxidative stress and inflammation in SFTS patients.
Almost all patients included in this study made their first visit to hospitals after symptom onset and the time span from symptom onset to hospital admission varied. Therefore, we were not able to know whether patients with elevated RDW at admission had a higher baseline RDW before. The days from symptom onset to hospital admission between survivors and non-survivors was comparable, suggesting they might be entered into hospital at the same stage of disease. The larger increase in the elevated RDW group probably indicate a longer duration of disease before hospital admission, which is reported to be associated with an adverse outcome.10,35 Patients with chronic illness were expected to have a higher baseline RDW for the reported association of comorbidity with death. However, we failed to find the association in our study. Regardless of the reasons why RDW of patients with SFTS differed when admitted, the association of elevated RDW values with higher risk of death persisted during hospitalization. This study indicates that RDW could function as an effective marker for estimating the probability of death in SFTS patients. Compared with other markers with a significant prognostic value in SFTSV infection, RDW is easier to get because it is automatically provided in the routine blood test.
There are several limitations in this study. Since the analysis of the predictive value of RDW were performed in hospitalized SFTS patients, the predictive value of RDW needs to be validated in SFTS patients who were not admitted to hospitals. In addition, the sample size is relatively small. Therefore, further multicenter, prospective studies were required to better evaluate the predictive value of RDW for SFTS-related mortality.
Conclusions
This cohort study confirmed an association between mortality risk and RDW at hospital admission and during hospitalization in SFTS patients. As a routine blood measure, RDW appears to be a practical indicator for the stratification of mortality risk among hospitalized SFTS patients. However, further prospective studies are needed to confirm our findings.
Abbreviations
ALT, alanine aminotransferase; APTT, activated partial thromboplastin time; AUC, area under the receiver operating characteristic curve; BUN, blood urea nitrogen; CI, confidence interval; Cr, creatinine; GGT, gama-glutamyl transpeptidase; Hb, hemoglobin; HR, hazard ratio; IQR, interquartile range; LDH, lactate dehydrogenase; LYM, lymphocyte; MCV, mean corpuscular volume; NEU, neutrophil; PLT, platelet count; PT, prothrombin time; RBC, red blood cell; RDW, red blood cell distribution width; ROC, receiver operating characteristic; RR, relative risk; SFTS, severe fever with thrombocytopenia syndrome; SFTSV, SFTS virus; TBil, total bilirubin; WBC, white blood cell.
Data Sharing Statement
The authors confirm that all relevant data are within the manuscript.
Ethics Approval and Informed Consent
This study was approved by the ethics committees of Nanjing Drum Tower Hospital (approval number: 2022-238-02), and the protocol was conducted in accordance with the Declaration of Helsinki. A waiver of informed consent was granted by the ethics committees due to a retrospective design of deidentified data and a minimal risk involved. The data presented in this study do not allow for the identification of individuals. We affirm our commitment to maintaining the confidentiality of patient data.
Funding
Dr. Rui Huang wishes to acknowledge the support from Nanjing Medical Science and Technique Development Foundation (No. QRX17121) and Natural Science Foundation of Jiangsu Province (No. BK20211004). Dr. Jie Li wishes to acknowledge the support from the National Natural Science Fund (No.81970545; 82170609), Natural Science Foundation of Shandong Province (Major Project) (No. ZR2020KH006) and Ji’nan Science and Technology Development Project (No.2020190790). Dr. Chao Wu wishes to acknowledge the support from Nanjing Important Science & Technology Specific Projects (No. 2021‐11005). Dr. Yali Xiong wishes to acknowledge the support from the Clinical Trials from the Affiliated Drum Tower Hospital, Medical School of Nanjing University (2022-LCYJ-DBZ-06).
Disclosure
All authors report no conflicts of interest in this work.
References
1. Liu Q, He B, Huang SY, Wei F, Zhu XQ. Severe fever with thrombocytopenia syndrome, an emerging tick-borne zoonosis. Lancet Infect Dis. 2014;14(8):763–772. doi:10.1016/s1473-3099(14)70718-2
2. Yu XJ, Liang MF, Zhang SY, et al. Fever with thrombocytopenia associated with a novel bunyavirus in China. N Engl J Med. 2011;364(16):1523–1532. doi:10.1056/NEJMoa1010095
3. Shin J, Kwon D, Youn SK, Park JH. Characteristics and factors associated with death among patients hospitalized for severe fever with thrombocytopenia syndrome, South Korea, 2013. Emerg Infect Dis. 2015;21(10):1704–1710. doi:10.3201/eid2110.141928
4. Kato H, Yamagishi T, Shimada T, et al. Epidemiological and Clinical Features of severe fever with thrombocytopenia syndrome in Japan, 2013-2014. PLoS One. 2016;11(10):e0165207. doi:10.1371/journal.pone.0165207
5. Rattanakomol P, Khongwichit S, Linsuwanon P, Lee KH, Vongpunsawad S, Poovorawan Y. Severe fever with thrombocytopenia syndrome virus infection, Thailand, 2019-2020. Emerg Infect Dis. 2022;28(12):2572–2574. doi:10.3201/eid2812.221183
6. McMullan LK, Folk SM, Kelly AJ, et al. A new phlebovirus associated with severe febrile illness in Missouri. N Engl J Med. 2012;367(9):834–841. doi:10.1056/NEJMoa1203378
7. Seo JW, Kim D, Yun N, Kim DM. Clinical update of severe fever with thrombocytopenia syndrome. Viruses. 2021;13(7):1213. doi:10.3390/v13071213
8. Li JC, Zhao J, Li H, Fang LQ, Liu W. Epidemiology, clinical characteristics, and treatment of severe fever with thrombocytopenia syndrome. Infect Med. 2022;1(1):40–49. doi:10.1016/j.imj.2021.10.001
9. Li H, Lu QB, Xing B, et al. Epidemiological and clinical features of laboratory-diagnosed severe fever with thrombocytopenia syndrome in China, 2011-17: a prospective observational study. Lancet Infect Dis. 2018;18(10):1127–1137. doi:10.1016/s1473-3099(18)30293-7
10. Dualis H, Zefong AC, Joo LK, et al. Factors and outcomes in Severe Fever with Thrombocytopenia Syndrome (SFTS): a systematic review. Ann Med Surg. 2021;67:102501. doi:10.1016/j.amsu.2021.102501
11. Yang ZD, Hu JG, Lu QB, et al. The prospective evaluation of viral loads in patients with severe fever with thrombocytopenia syndrome. J Clin Virol. 2016;78:123–128. doi:10.1016/j.jcv.2016.03.017
12. Xu X, Sun Z, Liu J, et al. Analysis of clinical features and early warning indicators of death from severe fever with thrombocytopenia syndrome. Int J Infect Dis. 2018;73:43–48. doi:10.1016/j.ijid.2018.05.013
13. Liu W, Lu QB, Cui N, et al. Case-fatality ratio and effectiveness of ribavirin therapy among hospitalized patients in China who had severe fever with thrombocytopenia syndrome. Clin Infect Dis. 2013;57(9):1292–1299. doi:10.1093/cid/cit530
14. Gai ZT, Zhang Y, Liang MF, et al. Clinical progress and risk factors for death in severe fever with thrombocytopenia syndrome patients. J Infect Dis. 2012;206(7):1095–1102. doi:10.1093/infdis/jis472
15. Hu J, Li S, Zhang X, et al. Correlations between clinical features and death in patients with severe fever with thrombocytopenia syndrome. Medicine. 2018;97(22):e10848. doi:10.1097/md.0000000000010848
16. Wang L, Zou Z, Ding K, Hou C. Predictive risk score model for severe fever with thrombocytopenia syndrome mortality based on qSOFA and SIRS scoring system. BMC Infect Dis. 2020;20(1):595. doi:10.1186/s12879-020-05299-7
17. Wang L, Zou Z, Hou C, Liu X, Jiang F, Yu H. Score risk model for predicting severe fever with thrombocytopenia syndrome mortality. BMC Infect Dis. 2017;17(1):42. doi:10.1186/s12879-016-2111-0
18. Wang L, Wan G, Shen Y, et al. A nomogram to predict mortality in patients with severe fever with thrombocytopenia syndrome at the early stage-A multicenter study in China. PLoS Negl Trop Dis. 2019;13(11):e0007829. doi:10.1371/journal.pntd.0007829
19. Wang Y, Qin LH, Zhang K, et al. Blood urea nitrogen to albumin ratio is a novel predictor of fatal outcome for patients with severe fever with thrombocytopenia syndrome. J Med Virol. 2024;96(6):e29731. doi:10.1002/jmv.29731
20. Fang K, Song X, Bo J. A nomogram to predict mortality in patients with severe fever with thrombocytopenia syndrome. Sci Rep. 2024;14(1):10627. doi:10.1038/s41598-024-60923-9
21. Salvagno GL, Sanchis-Gomar F, Picanza A, Lippi G. Red blood cell distribution width: a simple parameter with multiple clinical applications. Crit Rev Clin Lab Sci. 2015;52(2):86–105. doi:10.3109/10408363.2014.992064
22. Li N, Zhou H, Tang Q. Red blood cell distribution width: a novel predictive indicator for cardiovascular and cerebrovascular diseases. Dis Markers. 2017;2017:7089493. doi:10.1155/2017/7089493
23. Higgins JM, Mahadevan L. Physiological and pathological population dynamics of circulating human red blood cells. Proc Natl Acad Sci U S A. 2010;107(47):20587–20592. doi:10.1073/pnas.1012747107
24. Topaz G, Kitay-Cohen Y, Peled L, et al. The association between red cell distribution width and poor outcomes in hospitalized patients with influenza. J Crit Care. 2017;41:166–169. doi:10.1016/j.jcrc.2017.05.014
25. Krishna V, Pillai G, Velickakathu Sukumaran S. Red cell distribution width as a predictor of mortality in patients with sepsis. Cureus. 2021;13(1):e12912. doi:10.7759/cureus.12912
26. Jia L, Cui S, Yang J, et al. Red blood cell distribution width predicts long-term mortality in critically ill patients with acute kidney injury: a retrospective database study. Sci Rep. 2020;10(1):4563. doi:10.1038/s41598-020-61516-y
27. Zhang FX, Li ZL, Zhang ZD, Ma XC. Prognostic value of red blood cell distribution width for severe acute pancreatitis. World J Gastroenterol. 2019;25(32):4739–4748. doi:10.3748/wjg.v25.i32.4739
28. Zhang W, Wang Y, Wang J, Wang S. Association between red blood cell distribution width and long-term mortality in acute respiratory failure patients. Sci Rep. 2020;10(1):21185. doi:10.1038/s41598-020-78321-2
29. Lorente L, Martin MM, Argueso M, et al. Association between red blood cell distribution width and mortality of COVID-19 patients. Anaesth Crit Care Pain Med. 2021;40(1):100777. doi:10.1016/j.accpm.2020.10.013
30. Banon T, Wortsman J, Ben Moshe S, et al. Evaluating red blood cell distribution width from community blood tests as a predictor of hospitalization and mortality in adults with SARS-CoV-2: a cohort study. Ann Med. 2021;53(1):1410–1418. doi:10.1080/07853890.2021.1968484
31. Foy BH, Carlson JCT, Reinertsen E, et al. Association of red blood cell distribution width with mortality risk in hospitalized adults with SARS-CoV-2 infection. JAMA Network Open. 2020;3(9):e2022058. doi:10.1001/jamanetworkopen.2020.22058
32. Patel HH, Patel HR, Higgins JM. Modulation of red blood cell population dynamics is a fundamental homeostatic response to disease. Am J Hematol. 2015;90(5):422–428. doi:10.1002/ajh.23982
33. Shan X, Li Z, Jiang J, Li W, Zhan J, Dong L. Prognostic value of red blood cell distribution width to albumin ratio for predicting mortality in adult patients meeting sepsis-3 criteria in intensive care units. BMC Anesthesiol. 2024;24(1):208. doi:10.1186/s12871-024-02585-8
34. Zhang Z, Hu X, Jiang Q, et al. Clinical characteristics and outcomes of acute kidney injury in patients with severe fever with thrombocytopenia syndrome. Front Microbiol. 2023;14:1236091. doi:10.3389/fmicb.2023.1236091
35. He Z, Wang B, Li Y, et al. Severe fever with thrombocytopenia syndrome: a systematic review and meta-analysis of epidemiology, clinical signs, routine laboratory diagnosis, risk factors, and outcomes. BMC Infect Dis. 2020;20(1):575. doi:10.1186/s12879-020-05303-0
36. Ding S, Niu G, Xu X, et al. Age is a critical risk factor for severe fever with thrombocytopenia syndrome. PLoS One. 2014;9(11):e111736. doi:10.1371/journal.pone.0111736
37. Guo CT, Lu QB, Ding SJ, et al. Epidemiological and clinical characteristics of severe fever with thrombocytopenia syndrome (SFTS) in China: an integrated data analysis. Epidemiol Infect. 2016;144(6):1345–1354. doi:10.1017/S0950268815002678
38. Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46(5):846–848. doi:10.1007/s00134-020-05991-x
39. Liu W, Tao ZW, Wang L, et al. Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease. Chin Med J. 2020;133(9):1032–1038. doi:10.1097/cm9.0000000000000775
40. Lu QB, Zhang SY, Cui N, et al. Common adverse events associated with ribavirin therapy for Severe Fever with Thrombocytopenia Syndrome. Antiviral Res. 2015;119:19–22. doi:10.1016/j.antiviral.2015.04.006
41. Shimojima M, Fukushi S, Tani H, Taniguchi S, Fukuma A, Saijo M. Combination effects of ribavirin and interferons on severe fever with thrombocytopenia syndrome virus infection. Virol J. 2015;12(1):181. doi:10.1186/s12985-015-0412-3
42. Pierce CN, Larson DF. Inflammatory cytokine inhibition of erythropoiesis in patients implanted with a mechanical circulatory assist device. Perfusion. 2005;20(2):83–90. doi:10.1191/0267659105pf793oa
43. Scharte M, Fink MP. Red blood cell physiology in critical illness. Crit Care Med. 2003;31(12 Suppl):S651–7. doi:10.1097/01.Ccm.0000098036.90796.Ed
44. Ghaffari S. Oxidative stress in the regulation of normal and neoplastic hematopoiesis. Antioxid. Redox Signaling. 2008;10(11):1923–1940. doi:10.1089/ars.2008.2142
45. Kwon JS, Kim MC, Kim JY, et al. Kinetics of viral load and cytokines in severe fever with thrombocytopenia syndrome. J Clin Virol. 2018;101:57–62. doi:10.1016/j.jcv.2018.01.017
46. Sun Y, Jin C, Zhan F, et al. Host cytokine storm is associated with disease severity of severe fever with thrombocytopenia syndrome. J Infect Dis. 2012;206(7):1085–1094. doi:10.1093/infdis/jis452
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.