")
Back to Journals » Journal of Inflammation Research » Volume 17
Red Blood Cell-Related Parameters in Rheumatoid Arthritis: Clinical Value and Immunological Significance
Authors Cheng X, Liu J , Liu S , Fang D, Chen X, Ding X , Zhang X , Chen Y , Li Y
Received 22 May 2024
Accepted for publication 27 November 2024
Published 8 December 2024 Volume 2024:17 Pages 10641—10650
DOI https://doi.org/10.2147/JIR.S479059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Xueni Cheng,1,2 Jian Liu,1,2 Shengfeng Liu,1 Dahai Fang,1 Xiaolu Chen,1 Xiang Ding,1 Xianheng Zhang,1 Yiming Chen,1 Yang Li1
1Department of Rheumatology, The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, Anhui Province, People’s Republic of China; 2Anhui Key Laboratory of Application and Development of Internal Medicine of Modern Chinese Medicine, Anhui University of Chinese Medicine, Hefei, Anhui Province, People’s Republic of China
Correspondence: Jian Liu, Department of Rheumatology, The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, Anhui Province, People’s Republic of China, Tel +86 13955109537, Email [email protected]
Abstract: Rheumatoid arthritis (RA) is characterized by chronic inflammation and autoimmunity. Moreover, the disease activity, co-morbidities, and prognosis of RA are closely associated with changes in red blood cell (RBC)-related parameters. The role of these parameters in RA has therefore been extensively studied. Accordingly, this article summarizes and analyzes the close relationship of RBC-related parameters such as RBC count, hemoglobin, and RBC distribution width with disease activity, co-morbidities, and prognosis in RA by reviewing the available literature. In addition, given the immunomodulatory functions of RBCs, their surface proteins, contents, and microparticles are involved in the immunomodulatory process during RA. Overall, this review aims to assess the important clinical value and immunological significance of RBCs and their related parameters in the monitoring and management of RA, thus providing a reference for the clinical diagnosis and treatment of RA and the direction for the research on RBC-related immunity.
Keywords: rheumatoid arthritis, red blood cell, disease activity, clinical value, inflammation, immunity
Introduction
Rheumatoid arthritis (RA) is a chronic, systemic, autoimmune inflammatory disease that primarily involves the joints and periarticular soft tissues.1 RA usually presents with symmetric polyarticular pain, swelling, and stiffness, which most often occur in the joints of both hands, and possibly joint deformity in advanced cases.2 RA is characterized by a long disease course and high disability rate, which seriously jeopardizes the health and quality of life of patients and also causes huge economic losses to the social health system.3 While RA is mostly attributed to genetic factors, the risk of developing the disease is cumulatively increased by environmental factors as well.4,5 Inflammatory and immune responses are the most fundamental pathological changes in RA, which affect red blood cells (RBCs), the most widespread and common blood cells in the body. Therefore, RBCs also play an important role in the pathogenesis of RA. The inflammatory response in RA alters the number and function of RBCs, which manifests as the development of other progressive features of the disease.6 It has been demonstrated that there is a positive correlation between RBC counts and the erosion degree of RA joints.7 In addition, RBCs have immunomodulatory functions, including regulating the activation and migration of immune cells and participating in the delivery of inflammatory mediators. Notably, RBC-derived microparticles (RMPs) can directly contribute to the pathogenesis of RA by modulating immune cell activation.8
Disease activity score in 28 joints (DAS-28), immunoglobulin (IgG), rheumatoid factor (RF), and anti-cyclic citrullinated peptide antibody have been often used to assess disease activity in RA, which are essential for monitoring disease progression and guiding therapeutic decision-making. Nevertheless, the testing of these indicators is not highly reproducible due to the influence of various factors such as subjective bias of patients and testing costs, and their dynamic monitoring is limited by high testing costs. The routine blood test, which includes RBC counts and a battery of RBC-related parameters, is a standardized, automated, and simple test at no additional cost, which enables its wide application in clinical settings. Therefore, RBCs and their related parameters are of great clinical value and immunological significance in RA. In this context, this article mainly summarizes and analyzes the existing studies on RBC-related parameters in RA, thereby providing references for the clinical diagnosis and treatment of RA and pointing out the direction for future research.
RBCs as an Important Component of the Immune System
RBCs are the most plentiful type of blood cells in the blood, with 2×1013−3 × 1013 RBCs in an adult. In general, RBCs function primarily for the transportation and release of oxygen. Additionally, RBCs can also perform an immune function in the complex immune system and immune response.9 In 1981, Siegel et al first proposed the concept of RBC immune system, who observed that erythrocytes could recognize the third and fourth components of complement (C3b or C4b) through surface receptors and adhere to antigen-antibody-complement complexes, thus performing their immune function via immunoadhesion.10 In recent years, the immune function of RBCs has aroused enormous attention in the field of immunology. For instance, mature and nucleated RBCs in mammals have been reported to have immune potential and participate in both intrinsic immunity and adaptive immunomodulation.11,12 Several studies have also revealed that RBCs are more likely than white blood cells to be charged through triboelectrification during high-speed flow in the blood circulation, attracting and phagocytosing pathogens with opposite charges and killing pathogens via intracellular oxygen.13,14 Minasyan et al14 found that RBCs in the blood of patients with bacteremia could repeatedly phagocytose and kill bacteria of different types and sizes, implicating the killing function of RBCs. RBCs contain abundant cytokines, including a wide range of pro- and anti-inflammatory factors, chemokines, and growth factors.15 RBCs possess the capabilities of signaling, as well as receiving signals from other cells, which can further induce inflammatory responses and influence immune function. Therefore, RBCs are a key component of the immune system.16 We drew a schematic diagram of RBCs in inflammatory state, as shown in Figure 1.
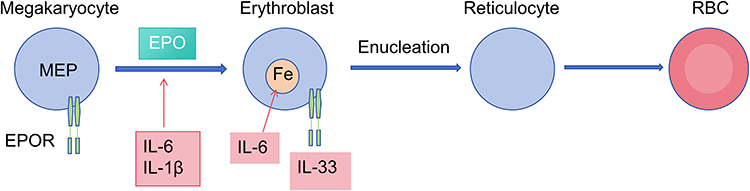 |
Figure 1 The process of erythropoiesis in the inflammatory state. |
Clinical Value of RBC-Related Parameters in RA
RBC Counts
In the normal human body, a strictly controlled balance exists between the production and clearance of RBC counts. However, this balance is usually disrupted during inflammation in infectious, autoimmune, and inflammatory diseases, resulting in acute or chronic anemia. Since the inflammatory environment of RA can inhibit erythropoiesis, anemia is one of the common extra-articular manifestations of RA.17 A study by Wolfe et al involving 2120 RA patients displayed that the prevalence of anemia in RA patients was 31.5%, which was three times higher than that in the general population.18 In RA, anemia secondary to inflammation occurs as a result of two main factors. First, pro-inflammatory cytokines, such as interleukin (IL)-1β, IL-6, and tumor necrosis factor (TNF)-α, can not only decrease EPO production by repressing erythropoietin (EPO) gene transcription19 but also reduce erythropoiesis by dampening the effect of EPO on erythroid progenitor cells in the bone marrow.20 Second, circulating monocytes in RA patients can re-differentiate into macrophages with high hemophagocytic capacity, enhancing hemophagocytosis and thus increasing RBC clearance.17 As reported, the development of anemia in patients with early RA is strongly associated with increased levels of inflammatory factors in the body. Specifically, pro-inflammatory cytokines contribute to the development of anemia in RA patients by regulating iron metabolism and suppressing erythropoiesis in bone marrow.21,22 Prior studies demonstrated that IL-6 in RA patients not only depressed erythropoiesis in bone marrow23 but also fostered the production of hepcidin mRNA, resulting in an increase in hepcidin.22 Hepcidin is considered a key factor in rheumatoid anemia due to its function in lowering serum iron levels and regulating iron transmembrane transport.24 Steenbergen et al concluded that anemia could be utilized to assess disease activity in RA patients because their studies unveiled that RA patients with anemia possessed faster radiographic progression and that anemia was independently associated with radiographic progression in RA.25,26 Furthermore, a large-sample cross-sectional study elucidated that structural damage and functional damage in the joints were more severe in RA patients with anemia than in RA patients without anemia.27 Altogether, anemia can be reflective of disease activity in RA.
Hemoglobin (Hb)
Reduced Hb concentrations are another manifestation of anemia. In a study by Möller et al, lower Hb concentrations were significantly correlated with higher DAS28 in RA patients, confirming the established relationship between inflammation and anemia.25 Additionally, this study also showed that anemia was a common manifestation of early progression of RA and that lower Hb levels were more strongly associated with the progression of joint damage compared to DAS28-C-reactive protein (CRP). Xue et al observed that Hb concentrations were lower in RA patients than in healthy controls, as well as in patients with active RA than in patients with inactive RA,7 indicating that RA patients with lower Hb concentrations have higher inflammation levels and increased disease activity compared to those with high Hb concentrations. Similar results were also obtained in the research by Padjen et al.28 These two studies illustrate a negative correlation between Hb concentrations and disease activity in RA. Another study29 exhibited that changes in Hb levels were negatively correlated with indicators of RA disease activity such as DAS28-CRP, CRP, and erythrocyte sedimentation rate (ESR) and suggested that anemia might be a predictor of poorer prognosis in RA patients. Meanwhile, Pereira et al discovered that low Hb levels might also correlate strongly with other markers of disease activity such as RF, CRP, pain and joint damage, and disease duration.30 The results of the above studies imply that disease severity and activity are higher in RA patients with low Hb levels compared to those without anemia. Moreover, a cohort study in the USA including 10,397 RA patients unraveled that the low Hb group had a higher percentage of patients with a history of comorbid cardiovascular disease (CVD), diabetes, and gastrointestinal disease, with higher disease severity and activity (P < 0.05).31 Evidently, the ability of anemia to reflect disease activity has been further validated in large-sample studies.
ESR
ESR is also a commonly used laboratory test that is used to detect the acute-phase response to inflammation for the diagnosis and monitoring of inflammatory conditions.32 ESR can be elevated in any condition that leads to an acute-phase response to inflammation, such as infections, surgery, autoimmune disease, and advanced cancer.33 Despite its low specificity and the impact of multiple disease factors, ESR holds significant clinical value in the assessment of specific clinical conditions. Notably, the diagnostic criteria for RA include ESR as one of the clinical indicators for diagnosing the disease and monitoring disease progression.34,35 Elevations in ESR of RA patients are caused by both the existence of an inflammatory state and a decrease in RBC counts due to anemia. In addition, active RA is accompanied by elevated concentrations of CRP, IgG, and fibrinogen,36 which were adsorbed into the RBC membrane when excessive, affecting the structure and function of RBCs.37 More importantly, many reports have demonstrated that fibrinogen and CRP, as well as several validated marker proteins such as IgG, IgM, IgA, and plasma albumin, play a role in inducing and maintaining increased RBC aggregation in the blood of RA patients,38,39 which may also account for the characteristic phenomenon of high ESR in RA.
Clinically, ESR is commonly used in combination with DAS28 to assess disease activity in RA patients. Many studies have documented that higher DAS28-ESR is associated with accelerated disease progression in RA.40,41 As well, ESR can predict the occurrence of co-morbidities in RA. A prior study revealed that changes in ESR could reflect the inflammatory activation state of RA patients prior to the combination of heart failure and that elevated ESR was correlated with the risk of heart failure in RA patients.42 Therefore, ESR can be utilized as one of the indicators for diagnosis and disease progression monitoring in RA. However, due to a study exhibiting that the assessment of inflammation or disease activity in RA patients with DAS28-ESR can be affected by anemia, DAS28-CRP may be more suitable than DAS28-ESR for assessing disease activity in RA patients with anemia.40
RBC Distribution Width (RDW)
Red cell distribution width (RDW) is part of the routine blood test used to estimate the size variability of RBCs.43 Lippi et al reported that RDW was positively associated with inflammatory markers including CRP and ESR in unselected outpatients,44 as observed in another study.45 In addition, elevated RDW has been detected in a variety of inflammatory diseases.46 According to a study by Al-Rawi et al, RDW was significantly higher in RA patients than in healthy controls.47 Increased RDW in RA is predominantly due not only to the fact that RA is an autoimmune chronic disease that is often combined with anemia, but also to the impact of inflammation. Of note, a previous study uncovered higher RDW values in RA patients without anemia than in healthy controls, underscoring that RDW in RA may be elevated by inflammation even in the absence of anemia.48 Moreover, through a large-sample prospective study, Perlstein et al49 found that anemia had no effect on the prediction of RDW for mortality risk. It is thus clear that although affected by anemia, RDW changes in RA patients essentially stem from the inflammatory state of RA. RA, as a chronic inflammatory disease, is associated with the imbalance of several cytokines including TNF-α, IL-1β, and IL-17 in patients. Cytokines may affect the production and apoptosis of RBCs, as well as their size and fragility, through different pathways,50 which in turn is reflected in changes in RDW values. For example, high levels of inflammatory cytokines such as IL-1, IL-6, and TNF-α inhibit the activity of EPO by desensitizing erythroid progenitor cells to EPO, which leads to an influx of immature blood cells into the bloodstream, resulting in high RDW.47 He et al found that RDW was elevated in RA patients compared to controls and correlated with inflammatory state and anti-inflammatory cytokines in RA patients, highlighting that RDW can be used as a laboratory parameter to monitor inflammation in RA.51 Despite mounting studies demonstrating RDW as a potential inflammatory marker for monitoring inflammation and disease progression in RA patients, some researchers also believed that this finding is only relevant in some groups and in specific situations. For instance, a cross-sectional study by Remalante et al revealed that RDW was weakly correlated with DAS-28 in Filipino RA patients with a P-value > 0.05. Hence, they concluded that the ability of RDW to reflect disease activity is not applicable to all racial populations.52 In conclusion, the specific mechanisms by which RDW changes reflect RA disease activity are uncertain and this ability of RDW is influenced by other factors, which calls for further large-sample, multi-control studies.
CVD is one of the common extra-articular damages of RA. Reportedly, the incidence of CVD in RA patients is twice as high as that in the general population, and CVD also leads to an increase of 60% in the mortality of RA patients.53 According to a study by Rodríguez-Carrio et al, RDW values at initial diagnosis had a moderate discriminative power for the occurrence of CV events in RA, with favorable performance of RDW changes accumulated in the first year after diagnosis, illustrating that RDW can be utilized as a predictor of CV events in RA patients.54 The results of another study exhibited that elevated RDW at admission, during hospitalization, or at discharge was significantly associated with increased all-cause mortality in patients with chronic heart failure and coronary heart disease.55 Over the past 10 years, effective antirheumatic therapy for early RA based on RDW changes has markedly decreased mortality from CV events in RA patients.56 Therefore, RDW monitoring in the first stage of RA can guide the management of inflammation and thus reduce the incidence of CV events.
Table 1 summarizes the literature on the correlation of RBC-related parameters with RA disease activity. In summary, anemia is typically associated with disease activity in RA and can be an indicator of the inflammatory response. It is therefore useful to guide the clinical management of RA by monitoring anemia in RA patients. Table 2 lists the literature on the correlation of RBC-related parameters with the co-morbidities and prognosis of RA. Low RBC counts, low Hb levels, and high RDW values are strongly associated with an increased risk of CV events, the aggravation of joint damage, and the decreased quality of life of patients, thereby affecting the daily life and working ability of RA patients. Additionally, long-term cohort studies are warranted to continually track the impact of RBC-related parameters on the long-term prognosis of RA patients.
 |
Table 1 RBC-Related Parameters and RA Disease Activity |
 |
Table 2 RBC-Related Parameters and the Co-Morbidities and Prognosis of RA |
Immunological Significance of RBCs in RA
Immune Function of RMPs in RA
With in-depth research on the immune function of RBCs, RBCs have been established to exert an immunomodulatory effect in multiple physiological and pathological models and play a critical role in the normal development of the organism and the development of diseases.57,58 RBCs can regulate the cell cycle of CD4+ and CD8+ T cell populations and release factors that favor their growth and survival.59–61 Accordingly, RBCs can be directly involved in the pathogenesis of RA through immunomodulation. A prior study elucidated that most cell-derived microparticles in the circulation and a few microparticles in the synovial space originate from RBCs and that RMPs can influence the expansion of the T-lymphocyte pool through antigen presentation.62 Unfortunately, an over-expanded T-lymphocyte pool may lead to immune system dysregulation and exacerbate RA. Meanwhile, another study unveiled that microparticles with bound C1q, C4, and C3 were abundant in RA synovial fluid, suggesting the involvement of RMPs in the formation of immune complexes during RA.63 Moreover, these immune complexes can be deposited in joints and other tissues, exacerbating the inflammatory response and tissue damage in RA.
Immunomodulation of RBC-Related Proteins in RA
Another important immunomodulatory property of RBCs is their tendency to bind to numerous chemokines. As reported, a major binding site on the surface of RBCs is the Duffy Ag Receptor (DARC) of chemokines, which binds to IL-8, thereby triggering IL-8-dependent gradient inactivation of chemokines and preventing neutrophil recruitment. Therefore, it can be believed that sequestration of inflammatory factors by RBC surface receptors depresses neutrophil signaling and thus curbs the immune response.64 Conversely, Darbonne et al concluded through a series of experiments that chemokine binding is readily reversible, illustrating that RBC receptors may have the potential of sustaining immune activation, as RBC receptors can alternatively bind and release their substrates in the tissue microenvironment, thereby maintaining the gradient of chemokines and promoting immune responses.65 In addition, the Duffy site binds to other immunomodulatory proteins with high affinity, including CXC and CC chemokines other than IL-8.66 In other words, RBCs bind to chemokines via DARC, thereby mediating neutrophil recruitment and immune activation. Available studies have unveiled that the role of DARC binding activity of RBCs depends on the environment, sometimes exacerbating the immune response and sometimes maintaining immune quiescence. Nevertheless, the exact mechanisms and environmental factors that regulate this duality remain unclear.12 Hence, the immunomodulatory role of RBCs in RA may be double-edged. It has also been found that some proteins in RBC, such as calpastatin, have the potential to stimulate the inflammatory activity of other cells or to become antigens in the autoimmune process of RA.67 Therefore, research on antigen systems targeted by immune cells may also shed light on the relationship between immunomodulation and RBCs in RA.68
Promoting Effect of RBC-Platelet (PLT) Interactions on Immune-Inflammatory Responses in RA
In RA, the inflammatory response in the body can contribute to a hypercoagulable state,69 which is closely related to the stimulation of inflammatory factors and the abnormal activation of the NF-κB pathway.70 There are several reports revealing that RBCs may be implicated in the hypercoagulable state. For instance, Sun et al found that in normal humans, RBCs and PLTs facilitated the process of thrombin generation in a phosphatidylserine (PS)-dependent manner and that PS-positive RBCs also complemented cross-linked collagen-related peptide-induced procoagulant activity of PLTs.71 There are many circulating extracellular vesicles from PLTs and RBCs in RA patients,72 which can recruit mediators of the coagulation cascade and initiate clot formation by exposure to PS, further exacerbating the inflammatory response.73–75 Therefore, this interaction may account for the thrombotic events observed in the vessels of RA patients. In addition, platelet integrin αIIbβ3 (GPIIb-IIIa) is central to coagulation, fibrinogenesis, and PLT interactions.76 αIIbβ3 directly binds to intercellular adhesion molecule 4 on the surface of RBCs,77,78 which may also be a factor contributing to thrombotic events in RA. Since neovascularization is one of the progressive manifestations of RA, the interaction between RBCs and platelets may present exponentially in RA. A former study displayed the RBC-PLT ratio was significantly associated with disease activity in RA.7 Obviously, RBC-PLT interactions in RA promote immune-inflammatory responses, accelerating the progression and causing poor prognosis of RA.
Summary and Prospects
In our review, we summarise the solid evidence that erythrocytes, as the most common blood cells in human blood, play an important role in patients with RA. The current guidelines for RA recommend early targeted treatment of RA with DMARDs in order to reduce disease activity as quickly as possible and minimise joint and organ damage.79,80 Given that targeted therapeutic approaches require close monitoring of disease activity, the need for long-term, objective, reliable, and easily accessible indicators of response to disease activity is undeniable. As a series of easily accessible and cost-effective biomarkers, RBCs and their related parameters have a crucial role in the clinical assessment and management of RA. By testing erythrocyte-related parameters, we can tell that the presence of anaemia is strongly associated with disease progression, imaging progression and joint damage in RA; RDW is positively correlated with inflammatory markers in RA patients and may be able to be used as a potential marker for assessing the disease progression of RA, as well as being correlated with the risk of developing cardiovascular disease in RA patients. Erythrocytes themselves can also play an immunomodulatory role, as evidenced by the fact that the Duffy Ag Receptor (DARC) on their surface binds to a variety of chemokines and regulates neutrophil recruitment and immune activation, which may exacerbate immune responses or maintain immune quiescence in different environments, and also interacts with PLT to promote immune-inflammatory responses in RA patients. In the future, further studies are warranted to continuously investigate the pathophysiological and immunological mechanisms underlying changes in these parameters in RA, thus providing additional support for the clinical management of RA.
This review highlights the potential of erythrocyte parameters as a cost-effective indicator of RA disease activity monitoring, risk assessment for the development of comorbidities, and provides a basis for further investigation. Future studies should aim to assess the diagnostic and evaluative performance of erythrocyte parameters and their possible advantages in terms of cut-off values, specificity and sensitivity compared with established standards, including biomarkers such as DAS-28 and CRP. Only then can the clinical validity and utility of erythrocyte-related parameters as a means of assessing disease activity and predicting the development of comorbidities in patients with RA be determined. Specifically, in the future, multi-center, large-sample, multi-ethnic randomized controlled trials should be conducted to clarify the specific RBC-related parameter that has definite independent value for the clinical evaluation of disease activity, co-morbidities, and prognosis in RA, the optimal cut-off values, sensitivity, and specificity of RBC-related parameters for assessing disease activity, co-morbidities, and prognosis in RA, molecular biological mechanisms of RBC immunity in the development of RA, and whether RBC-related parameters can be combined with other biomarkers to create a comprehensive assessment system for RA.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
High-level key discipline of Traditional Chinese Medicine by the State Administration of Traditional Chinese Medicine (Teaching Letter of Traditional Chinese Medicine [2023] NO.85); National Traditional Chinese Medicine Inheritance and Innovation Center (Development and Reform Office Society [2022] No. 366); the National Nature Fund Program (No. 82074373). The grantees of the three funded projects were all Jian Liu. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no conflicts of interest regarding the publication of this paper. All the authors had no financial relationship with the organizations that funded the study.
References
1. Di Matteo A, Bathon JM, Emery P. Rheumatoid arthritis. Lancet. 2023;402(10416):2019–2033. doi:10.1016/S0140-6736(23)01525-8
2. Finckh A, Gilbert B, Hodkinson B, et al. Global epidemiology of rheumatoid arthritis. Nat Rev Rheumatol. 2022. doi:10.1038/s41584-022-00827-y
3. Radu A, Bungau SG. Management of rheumatoid arthritis: an overview. Cells. 2021;10(11):2857. doi:10.3390/cells10112857
4. Scott IC, Seegobin SD, Steer S, et al. Predicting the risk of rheumatoid arthritis and its age of onset through modelling genetic risk variants with smoking. PLoS Genetics. 2013;9(9):e1003808. doi:10.1371/journal.pgen.1003808
5. Bergström U, Jacobsson L, Nilsson J, et al. Smoking, low formal level of education, alcohol consumption, and the risk of rheumatoid arthritis. Scand J Rheumatol. 2012;42(2):123–130. doi:10.3109/03009742.2012.723744
6. Luquita A, Urli L, Svetaz MJ, et al. Erythrocyte aggregation in rheumatoid arthritis: cell and plasma factor’s role. Clin Hemorheol Microcirc. 2009;41(1):49–56. doi:10.3233/CH-2009-1154
7. Xue L, Tao L, Sun H, et al. Association between blood PLT and RBC related indices and disease activity in patients with rheumatoid arthritis. International Journal of General Medicine. 2022;15:573–581. doi:10.2147/IJGM.S351505
8. Olumuyiwa-Akeredolu OO, Pretorius E. Platelet and red blood cell interactions and their role in rheumatoid arthritis. Rheumatol Int. 2015;35(12):1955–1964. doi:10.1007/s00296-015-3300-7
9. Bernard NJ. Another function for red blood cells. Nat Immunol. 2021;22(12):1469. doi:10.1038/s41590-021-01081-2
10. Siegel I, Lin Liu T, Gleicher N. THE RED-CELL IMMUNE SYSTEM. Lancet. 1981;318(8246):556–559. doi:10.1016/S0140-6736(81)90941-7
11. Elahi S, Mashhouri S. Immunological consequences of extramedullary erythropoiesis: immunoregulatory functions of CD71+ erythroid cells. Haematologica. 2020;105(6):1478–1483. doi:10.3324/haematol.2019.243063
12. Anderson HL, Brodsky IE, Mangalmurti NS. The evolving erythrocyte: red blood cells as modulators of innate immunity. J Immunol. 2018;201(5):1343–1351. doi:10.4049/jimmunol.1800565
13. Minasyan HA. Erythrocyte and leukocyte: two partners in bacteria killing. Int Rev Immunol. 2014;33(6):490–497. doi:10.3109/08830185.2014.956359
14. Minasyan H. Erythrocyte and blood antibacterial defense. Eur J Microbiol Immunol. 2014;4(2):138–143. doi:10.1556/EuJMI.4.2014.2.7
15. Karsten E, Breen E, Herbert BR. Red blood cells are dynamic reservoirs of cytokines. Sci Rep. 2018;8(1). doi:10.1038/s41598-018-21387-w
16. Minton K. Red blood cells join the ranks as immune sentinels. Nat Rev Immunol. 2021;21(12):760–761. doi:10.1038/s41577-021-00648-2
17. Canny SP, Orozco SL, Thulin NK, et al. Immune mechanisms in inflammatory anemia. Ann Rev Immunol. 2023;41(1):405–429. doi:10.1146/annurev-immunol-101320-125839
18. Wolfe F, Michaud K. Anemia and renal function in patients with rheumatoid arthritis. J Rheumatol. 2006;33(8):1516.
19. Ferrucci L, Guralnik JM, Woodman RC, et al. Proinflammatory state and circulating erythropoietin in persons with and without anemia. Am J Med. 2005;118(11):1211–1288. doi:10.1016/j.amjmed.2005.06.039
20. Grigorakaki C, Morceau F, Chateauvieux S, et al. Tumor necrosis factor alpha-mediated inhibition of erythropoiesis involves GATA-1/GATA-2 balance impairment and PU.1 over-expression. Biochem Pharmacol. 2011;82(2):156–166. doi:10.1016/j.bcp.2011.03.030
21. Voulgari PV, Kolios G, Papadopoulos GK, et al. Role of cytokines in the pathogenesis of anemia of chronic disease in rheumatoid arthritis. Clin Immunol. 1999;92(2):153–160. doi:10.1006/clim.1999.4736
22. Masson C. Rheumatoid anemia. Joint Bone Spine. 2011;78(2):131–137. doi:10.1016/j.jbspin.2010.05.017
23. Raj DSC. Role of interleukin-6 in the anemia of chronic disease. Semin Arthritis Rheumatism. 2009;38(5):382–388. doi:10.1016/j.semarthrit.2008.01.006
24. Nita E, Bairaktari E, Kolios G, et al. Role of hepcidin in anemia of chronic disease in rheumatoid arthritis. J Lab Phys. 2021;13(04):317–322. doi:10.1055/s-0041-1732827
25. Möller B, Scherer A, Förger F, et al. Anaemia may add information to standardised disease activity assessment to predict radiographic damage in rheumatoid arthritis: a prospective cohort study. Ann Rheumatic Dis. 2014;73(4):691–696. doi:10.1136/annrheumdis-2012-202709
26. van Steenbergen HW, van Nies JAB, van der Helm-Van Mil AHM. Anaemia to predict radiographic progression in rheumatoid arthritis. Ann Rheumatic Dis. 2013;72(7):e16. doi:10.1136/annrheumdis-2013-203718
27. Chen Y, Xu S, Xu Y, et al. Inflammatory anemia may be an indicator for predicting disease activity and structural damage in Chinese patients with rheumatoid arthritis. Clin Rheumatol. 2020;39(6):1737–1745. doi:10.1007/s10067-019-04873-y
28. Padjen I, Öhler L, Studenic P, et al. Clinical meaning and implications of serum hemoglobin levels in patients with rheumatoid arthritis. Semin Arthritis Rheumatism. 2017;47(2):193–198. doi:10.1016/j.semarthrit.2017.03.001
29. Smyrnova G. Relação entre o nível de hemoglobina e a atividade da doença em pacientes com artrite reumatoide. Revista Brasileira de Reumatologia. 2014;54(6):437–440. doi:10.1016/j.rbr.2014.06.002
30. Pereira ICP, Sousa NCF, Pereira DMS, et al. Treatment with either leflunomide or Adalimumab reduces anaemia in patients with rheumatoid arthritis. Anais da Academia Brasileira de Ciências. 2018;90(2 suppl 1):2161–2166. doi:10.1590/0001-3765201820170091
31. Furst DE, Chang H, Greenberg JD, et al. Prevalence of low hemoglobin levels and associations with other disease parameters in rheumatoid arthritis patients: evidence from the CORRONA registry. Clin Experim Rheumatol. 2009;27(4):560.
32. Bray C, Bell LN, Liang H, et al. Erythrocyte sedimentation rate and C-reactive protein measurements and their relevance in clinical medicine. WMJ. 2016;115(6):317–321.
33. Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med. 1999;340(6):448–454. doi:10.1056/NEJM199902113400607
34. Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis. JAMA. 2018;320(13):1360. doi:10.1001/jama.2018.13103
35. Singh G. C-reactive protein and erythrocyte sedimentation rate in inflammatory lesions: erythrocyte sedimentation rate test is essential in a subset of patients. Am J Clin Pathol. 2023;161(3):311.
36. Meyer PWA, Hodkinson B, Ally M, et al. Circulating cytokine profiles and their relationships with autoantibodies, acute phase reactants, and disease activity in patients with rheumatoid arthritis. Mediators Inflammation. 2010;2010:1–10. doi:10.1155/2010/158514
37. Saldanha C, Freitas T, Almeida JP. Fibrinogen effects on erythrocyte nitric oxide mobilization in presence of acetylcholine. Life Sci. 2012;91(21–22):1017–1022. doi:10.1016/j.lfs.2012.06.035
38. Kumsishvili T, Varazashvili M, Mchedlishvili G. Local hemorheological disorders during chronic inflammation. Clin Hemorheol Microcirc. 2004;30(3–4):427–429.
39. Weng X, Cloutier G, Beaulieu R, et al. Influence of acute-phase proteins on erythrocyte aggregation. Am J Physiol Heart Circ Physiol. 1996;271(6):H2346–H2352. doi:10.1152/ajpheart.1996.271.6.H2346
40. Mohammadi-Kebar Y, Azami A, Pourfarzi F, et al. Comparative study of DAS-28 ESR and DAS-28 CRP in determining the severity of disease activity in patients with rheumatoid arthritis. Int J Community Med Public Health. 2022;9(2):626. doi:10.18203/2394-6040.ijcmph20220218
41. Alvarez-Hernandez E, Marin SR, Alvarez-Etchegaray S. SAT0142 Comparison of the Patient’s Assessment Measure (RADAI) and the Physician’s Assessment Measure (DAS 28-ESR AND CDAI) of Disease Activity in Rheumatoid Arthritis (RA) in an open label clinical study. Ann Rheumatic Dis. 2014;73(Suppl 2):642. doi:10.1136/annrheumdis-2014-eular.6080
42. Maradit-Kremers H, Nicola PJ, Crowson CS, et al. Raised erythrocyte sedimentation rate signals heart failure in patients with rheumatoid arthritis. Ann Rheumatic Dis. 2006;66(1):76–80. doi:10.1136/ard.2006.053710
43. Danese E, Lippi G, Montagnana M. Red blood cell distribution width and cardiovascular diseases. J Thorac Dis. 2015;7(10):E402–E411. doi:10.3978/j.issn.2072-1439.2015.10.04
44. Lippi G, Targher G, Montagnana M, et al. Relation between red blood cell distribution width and inflammatory biomarkers in a large cohort of unselected outpatients. Arch Pathol Lab Med. 2009;133(4):628–632. doi:10.5858/133.4.628
45. Vayá A, Sarnago A, Fuster O, et al. Influence of inflammatory and lipidic parameters on red blood cell distribution width in a healthy population. Clin Hemorheol Microcirc. 2015;59(4):379–385. doi:10.3233/CH-141862
46. Song CS, Park DI, Yoon MY, et al. Association between red cell distribution width and disease activity in patients with inflammatory bowel disease. Dig Dis Sci. 2012;57(4):1033–1038. doi:10.1007/s10620-011-1978-2
47. Al-Rawi Z, Gorial F, Al-Bayati AA. Red cell distribution width in rheumatoid arthritis. Mediterranean J Rheumatol. 2018;29(1):38–42. doi:10.31138/mjr.29.1.38
48. Tecer D, Sezgin M, Kanık A, et al. Can mean platelet volume and red blood cell distribution width show disease activity in rheumatoid arthritis?. Biomarkers Med. 2016;10(9):967–974. doi:10.2217/bmm-2016-0148
49. Perlstein TS, Weuve J, Pfeffer MA, et al. Red blood cell distribution width and mortality risk in a community-based prospective cohort. Arch Internal Med. 2009;169(6):588. doi:10.1001/archinternmed.2009.55
50. Weiss G, Goodnough LT. Anemia of chronic disease. N Engl J Med. 2005;352(10):1011–1023. doi:10.1056/NEJMra041809
51. He Y, Liu C, Zeng Z, et al. Red blood cell distribution width: a potential laboratory parameter for monitoring inflammation in rheumatoid arthritis. Clin Rheumatol. 2018;37(1):161–167. doi:10.1007/s10067-017-3871-7
52. Remalante PPM, Salido EO, Penserga EG, et al. Red cell distribution width and neutrophil–lymphocyte ratio in rheumatoid arthritis. Rheumatol Int. 2020;40(10):1631–1637. doi:10.1007/s00296-020-04685-3
53. Meyer PW, Anderson R, Ker JA, et al. Rheumatoid arthritis and risk of cardiovascular disease. Cardiovasc J Africa. 2018;29(5):317–321. doi:10.5830/CVJA-2018-018
54. Rodriguez-Carrio J, Alperi-Lopez M, Lopez P, et al. Red cell distribution width is associated with cardiovascular risk and disease parameters in rheumatoid arthritis. Rheumatology. 2015;54(4):641–646. doi:10.1093/rheumatology/keu345
55. Li S, Zhang W, Liang X. Red blood cell distribution width and mortality risk in critically ill cardiovascular patients. Heliyon. 2023;9(11):e22225. doi:10.1016/j.heliyon.2023.e22225
56. Hansildaar R, Vedder D, Baniaamam M, et al. Cardiovascular risk in inflammatory arthritis: rheumatoid arthritis and gout. Lancet Rheumatol. 2021;3(1):e58–e70. doi:10.1016/S2665-9913(20)30221-6
57. Hotz MJ, Qing D, Shashaty MGS, et al. Red blood cells homeostatically bind mitochondrial DNA through TLR9 to maintain quiescence and to prevent lung injury. Am J Respir Crit Care Med. 2018;197(4):470–480. doi:10.1164/rccm.201706-1161OC
58. Neote K, Darbonne W, Ogez J, et al. Identification of a promiscuous inflammatory peptide receptor on the surface of red blood cells. J Biol Chem. 1993;268(17):12247–12249. doi:10.1016/S0021-9258(18)31379-6
59. Antunes RF, Brandão C, Maia M, et al. Red blood cells release factors with growth and survival bioactivities for normal and leukemic T cells. Immunol Cell Biol. 2011;89(1):111–121. doi:10.1038/icb.2010.60
60. Profumo E, Buttari B, Petrone L, et al. Redox imbalance of red blood cells impacts T lymphocyte homeostasis: implication in carotid atherosclerosis. Thrombosis Haemostasis. 2017;106(12):1117–1126.
61. Arosa FA, Pereira CF, Fonseca AM. Red blood cells as modulators of T cell growth and survival. Curr Pharm Des. 2004;10(2):191–201. doi:10.2174/1381612043453432
62. Danesh A, Inglis HC, Jackman RP, et al. Exosomes from red blood cell units bind to monocytes and induce proinflammatory cytokines, boosting T-cell responses in vitro. Blood. 2014;123(5):687–696. doi:10.1182/blood-2013-10-530469
63. Biro E, Nieuwland R, Tak PP, et al. Activated complement components and complement activator molecules on the surface of cell-derived microparticles in patients with rheumatoid arthritis and healthy individuals. Ann Rheumatic Dis. 2007;66(8):1085–1092. doi:10.1136/ard.2006.061309
64. Darbonne WC, Rice GC, Mohler MA, et al. Red blood cells are a sink for interleukin 8, a leukocyte chemotaxin. J Clin Investig. 1991;88(4):1362–1369. doi:10.1172/JCI115442
65. Fukuma N, Akimitsu N, Hamamoto H, et al. A role of the Duffy antigen for the maintenance of plasma chemokine concentrations. Biochem Biophys Res Commun. 2003;303(1):137–139. doi:10.1016/S0006-291X(03)00293-6
66. Lee JS, Wurfel MM, Matute-Bello G, et al. The Duffy Antigen modifies systemic and local tissue chemokine responses following lipopolysaccharide stimulation. J Immunol. 2006;177(11):8086–8094. doi:10.4049/jimmunol.177.11.8086
67. Iwaki-Egawa S, Matsuno H, Yudoh K, et al. High diagnostic value of anticalpastatin autoantibodies in rheumatoid arthritis detected by ELISA using human erythrocyte calpastatin as antigen. J Rheumatol. 2004;31(1):17–22.
68. Kontos S, Kourtis IC, Dane KY, et al. Engineering antigens for in situ erythrocyte binding induces T-cell deletion. Proc Natl Acad Sci. 2013;110(1). doi:10.1073/pnas.1216353110
69. Maas C, Renné T. Coagulation factor XII in thrombosis and inflammation. Blood. 2018;131(17):1903–1909. doi:10.1182/blood-2017-04-569111
70. Zhang P, Liu J, Tan B, et al. Hypercoagulable state is associated with NF-kappa B activation and increased inflammatory factors in patients with rheumatoid arthritis. Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi. 2016;32(3):364–368.
71. Sun S, Campello E, Zou J, et al. Crucial roles of red blood cells and platelets in whole blood thrombin generation. Blood Adv. 2023;7(21):6717–6731. doi:10.1182/bloodadvances.2023010027
72. Alghamdi M, Alamry SA, Bahlas SM, et al. Circulating extracellular vesicles and rheumatoid arthritis: a proteomic analysis. Cell Mol Life Sci. 2022;79(1).
73. Kim Y, Xia BT, Jung AD, et al. Microparticles from stored red blood cells promote a hypercoagulable state in a murine model of transfusion. Surgery. 2018;163(2):423–429. doi:10.1016/j.surg.2017.09.028
74. Lipets EN, Antonova OA, Shustova ON, et al. Use of Thrombodynamics for revealing the participation of platelet, erythrocyte, endothelial, and monocyte microparticles in coagulation activation and propagation. PLoS One. 2020;15(5):e227932. doi:10.1371/journal.pone.0227932
75. Tripisciano C, Weiss R, Eichhorn T, et al. Different potential of extracellular vesicles to support thrombin generation: contributions of phosphatidylserine, tissue factor, and cellular origin. Sci Rep. 2017;7(1). doi:10.1038/s41598-017-03262-2
76. Vallés J, Santos MT, Aznar J, et al. Platelet-erythrocyte interactions enhance αIIbβ3 integrin receptor activation and P-selectin expression during platelet recruitment: down-regulation by aspirin ex vivo. Blood. 2002;99(11):3978–3984. doi:10.1182/blood.V99.11.3978
77. Hermand P, Gane P, Huet M, et al. Red Cell ICAM-4 Is a novel ligand for platelet-activated αIIbβ3 integrin. J Biol Chem. 2003;278(7):4892–4898. doi:10.1074/jbc.M211282200
78. Du V, Huskens D, Maas C, et al. New insights into the role of erythrocytes in thrombus formation. Semin Thromb Hemost. 2014;40(1):72–80. doi:10.1055/s-0033-1363470
79. Smolen JS, Breedveld FC, Burmester GR, et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheumatic Dis. 2015;75(1):3–15. doi:10.1136/annrheumdis-2015-207524
80. Nagy G, Roodenrijs NMT, Welsing PMJ, et al. EULAR points to consider for the management of difficult-to-treat rheumatoid arthritis. Ann Rheumatic Dis. 2022;81(1):20–33. doi:10.1136/annrheumdis-2021-220973
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.