")
Back to Journals » Clinical Optometry » Volume 17
Refitting Previous Presbyopic Contact Lens Dropouts with a Single Use Multifocal Contact Lens
Authors Fogt JS , Roth M , Travis BA, Bickle KM, Gardner HP
Received 28 March 2025
Accepted for publication 25 June 2025
Published 2 July 2025 Volume 2025:17 Pages 185—193
DOI https://doi.org/10.2147/OPTO.S526434
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Mr Simon Berry
Jennifer Swingle Fogt,1 Madison Roth,1 Beth A Travis,1 Katherine M Bickle,2 Hope Patterson Gardner1
1College of Optometry, The Ohio State University, Columbus, OH, USA; 2Procare Vision Center, Granville, OH, USA
Correspondence: Jennifer Swingle Fogt, The Ohio State University College of Optometry, 338 W 10th Avenue, Columbus, OH, 43210, USA, Tel +1 614 292 0882, Email [email protected]
Purpose: Contact lens dropout is known to occur frequently in presbyopic patients. The purpose of this study was to assess the rate of patient-reported success, defined by willingness to continue lens wear after the study, when fitting previous presbyopic contact lens dropout patients with a single-use multifocal contact lens.
Methods: Presbyopes who had previously discontinued contact lens wear due to poor vision were recruited and fit with delefilcon A multifocal contact lenses. Participants were prescribed lenses following the fitting guide, wore lenses for 1 week to allow for adaptation, and returned for a follow-up visit. After confirmation of optimized lens powers, lenses were dispensed for one month of wear. A final visit was completed to assess vision and respond to survey questions, including 0– 100 visual analog scale (VAS) surveys of lens wear experiences. Participants also scored their likelihood of continuing with study lenses upon study completion and whether the participant would recommend the study lenses to a friend. Success with fitting the study lenses was defined as those participants who selected “very likely” or “likely” to continue wearing the study lenses after the conclusion of the study.
Results: Twenty-five participants completed all study visits. Median (Interquartile range) binocular LogMAR acuity with the study lenses was − 0.10 (0.16) at distance (20/16 Snellen acuity equivalent) and 0.00 (0.12) at near (20/20 Snellen acuity equivalent). The median (IQR) satisfaction score was 84 (29.75) on a scale of 0– 100. Eighty percent of the participants said they were very likely or likely to continue wearing the multifocal lenses after the conclusion of the study. All twenty-five of the participants said they would recommend the study lenses to a friend.
Conclusion: The objective and subjective findings of this study suggest that presbyopic contact lens dropouts can be refit with the study multifocal contact lens.
Keywords: presbyopia, multifocal contact lens, dropout
Introduction
Presbyopia brings new challenges to vision correction, as people begin to experience the inability to see clearly at near without a change in vision correction.1–3 For spectacle wearers, this problem is frequently addressed by including an add power in glasses, requiring adaptation to either a progressive lens design or a lined bifocal.4 Acclimating to new spectacles for presbyopia can take several weeks, including adjustment to the new optics and compensating alterations in head position and head movement.5–10
Presbyopic contact lens wearers similarly need to be refit with a lens that is designed to focus more than one viewing distance.5 The use of soft multifocal lenses has increased over the last few decades, employing simultaneous image optics.5 Similar to the time required to adjust to presbyopic spectacles, adaptation to multifocal contact lenses has been proposed to occur from 4 to 15 days by various researchers.11–17
Despite the increasing use and known advantages of multifocal contact lenses, studies have shown that multifocal contact lenses are under-prescribed among presbyopic patients.5,18,19 Reluctance to introduce multifocal lenses can stem from difficulty predicting which patients will be successful, concerns over required chair time, and fear that the fitting is unlikely to succeed.18,20,21 Hesitation in pursuing multifocal lens fitting may be intensified by reported retention rates of 57 to 69% at 1 year.22,23 This dropout from lens wear further contributes to the low percentage of contact lens wearers in the presbyopic population, with poor vision and discomfort as primary causes of lens wear discontinuation.24–26 Presbyopic patients are more likely to cite poor distance and near vision, and less likely to cite discomfort, as a reason for discontinuing lens wear compared to non-presbyopic patients; this includes both presbyopes wearing multifocal lenses and those using reading glasses over single vision lenses.22,27,28 A 2002 study found that 11 of 20 (55%) of presbyopic contact lens dropouts were successful when refit with a soft bifocal contact lens.3 It is not well known whether attempts to refit presbyopic contact lens dropouts in modern multifocal lens designs could lead to satisfied contact lens wear.
A study was designed to enroll presbyopic patients who previously discontinued lens wear for unsatisfactory vision and refit them with a single-use multifocal contact lens. It was hypothesized that this population could become successful contact lens wearers again by allowing time for lens adaptation and over-refracting lenses with specific criteria to ensure the least minus power distance correction and the lowest add power that provides near correction were used. This study sought to determine the frequency of patient-reported satisfaction with the study multifocal lenses when fit by following the manufacturer fitting guide and given adequate time for adaptation, similar to adaptation required for successful progressive addition spectacle wear.29
Methods
This prospective, open-label, noncomparative study was conducted under the tenants of the Declaration of Helsinki and the Institutional Review Board (2023H0245) at The Ohio State University in Columbus, Ohio, USA. The study was registered on Clinicaltrials.gov (NCT06053463) before enrollment of participants. A diagram of the study design can be found in Figure 1. An IRB-approved prescreening questionnaire was used to determine if potential participants met specific eligibility criteria. Potential participants were required to be at least 38 years of age and have a spectacle prescription between +6.00 and −10.00 diopters; less than 1.00 diopter of astigmatism; and an add power of +0.50 D or greater. Potential participants who reported previously discontinuing contact lens wear due to discomfort issues were excluded to eliminate possible dry eye or tear film complications. Presbyopic participants who had previously dropped out of contact lens wear due to unsatisfactory vision were recruited at two sites. After completing the informed consent process, vision was assessed to ensure participants had best-corrected acuity of 0.1 (equivalent to 20/25) or better in each eye. Visual acuity was obtained using a LogMAR lightbox throughout the study. Slit lamp biomicroscopy was completed to further evaluate eligibility. Exclusion criteria included: current ocular inflammation or infection; presence of corneal ectasia or keratoconus; history of eye surgery; pregnancy or lactation; poor systemic health that could preclude contact lens wear; and the presence of strabismus or a lack of binocular vision.
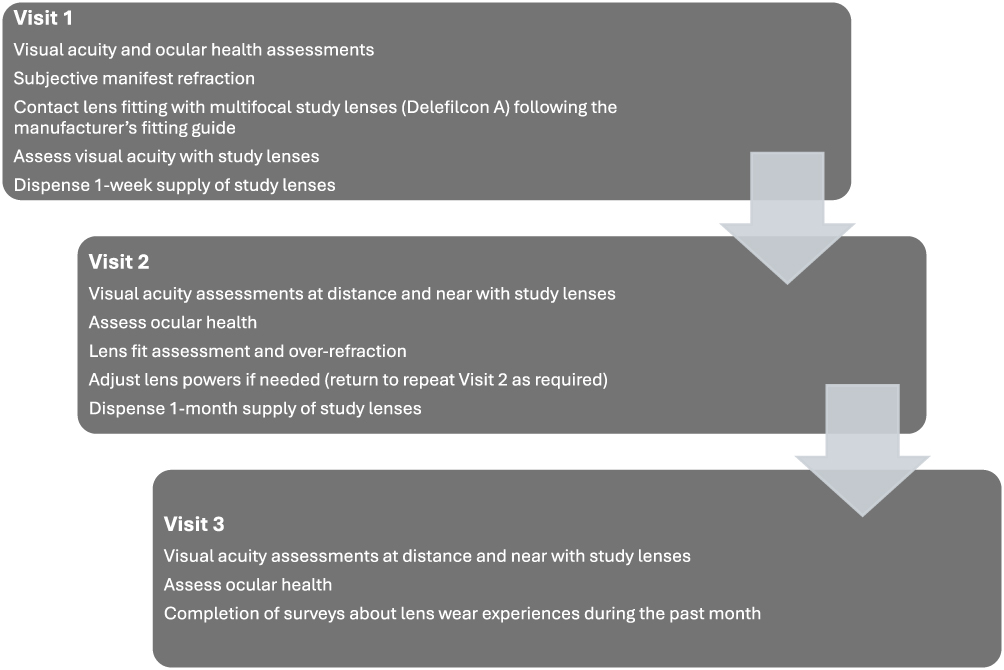 |
Figure 1 Study Design. |
Participants were refracted, determining the least minus prescription required for optimized distance vision and the lowest add power that provided satisfactory near vision. A single use multifocal lens design (Dailies TOTAL1 Multifocal, delefilcon A, Alcon, Inc, Fort Worth, TX, USA) was selected to be used in the study. A single use lens eliminates any concerns of poor compliance due to lens solution or storage, and the lens material has a high comfort profile.30–34 Participants were fit with the study lens following the manufacturer’s fitting guide (Dailies TOTAL1 Multifocal, delefilcon A, Alcon, Inc, Fort Worth, TX, USA). The fitting guide instructs practitioners to use an initial lens with +0.25D power added to the spherical equivalent of the vertexed manifest refraction. Initial add power to be used is based on the “lowest acceptable add” obtained during the manifest refraction as it falls in the following groupings: LO (up to +1.25 D), MED (+1.50 to +2.00 D), or HI (+2.25 or +2.50 D).
Over-refraction of the initial trial lenses was completed by following the fitting guide, with plus lenses presented over each eye, while binocular to determine how much additional plus power the participant would accept. The lens powers were updated if a change was found.
Participants returned for a follow-up visit after wearing the lenses for 1 week, which included assessments of visual acuity at distance and near, over-refraction of contact lenses, and assessments of lens fit and ocular health. Those participants who had further improvement of vision with a change in lens power were dispensed the new prescription and returned for a repeated follow-up visit in one week. Those who did not benefit from any changes in lens power were dispensed enough lenses to wear for one month and scheduled for their final visit. The final study visit consisted of assessments of distance and near visual acuity, lens fit, and ocular health. Participants also completed survey questions sent to their smartphones, while present at the visit. REDCap (Research Electronic Data Capture) was used to deploy the questions and capture participant responses.35,36 Survey questions regarding the participant wear experience over 1 month of study lens wear were scored on a 0–100 visual analog scale (VAS), with “Unacceptable” anchored at 0 and “Excellent” anchored at 100. The same scales were used for VAS surveys used to grade subjective overall vision, comfort, and satisfaction with the study lenses. Participants also responded to a Likert-scale question about willingness to continue wearing the study contact lenses after the study, and a “yes/no” question asking if they would recommend the study contact lenses to a friend. Success with fitting the study lenses was defined as selecting “very likely” or “likely” to continue wearing the study lenses after the conclusion of the study. Survey questions used at the end of the study are presented in Box 1.
 |
Box 1 Surveys Deployed at the Final Study Visit Using REDCap |
Statistical Analysis
Data analysis was completed with Minitab Version 21.3.1 (Minitab, LLC, State College, PA). Normality of data distribution was analyzed using Anderson–Darling testing for visual acuity and VAS survey responses. Data not distributed normally is reported as median and interquartile range. Comparisons of visual acuity with habitual spectacles and with study contact lenses were completed using Mann–Whitney analysis. Multiple linear regression was conducted to evaluate the impact of participant age, final add power, and type of lens worn when dropout previously occurred upon the VAS satisfaction score, quality of vision score, and comfort score.
Results
Twenty-five participants completed all visits of the study, wore the study lenses for 30 days after the final follow-up visit, and completed the wear experience survey. The mean ± standard deviation age of participants was 54.3 ± 6.6 years (Min, 43; Max, 69). Twenty-three participants were female. At the time that these participants previously dropped out of lens wear, 9 of the participants (36%) wore single vision spherical contact lenses and 16 wore multifocal contact lenses. Five additional eligible participants were enrolled but did not complete one month of lens wear for varying reasons: one was lost to follow-up, one exited due to an ocular adverse event unrelated to the study lens, and three voluntarily exited the study due to concerns of potential unsatisfactory vision over the required one month of wear.
Wear Time
During the 30 days between Visit 2 and Visit 3, the mean wear time of participants was 11.5 ± 2.5 hours per day. Participants wore the lenses 26 ± 4 days.
Visual Acuity
The median (Interquartile range) binocular distance visual acuity when wearing the study multifocal lenses was −0.10 (0.16), which is equivalent to 20/16 Snellen acuity. The median (IQR) binocular near visual acuity with the study lenses was 0 (0.12), which is equivalent to 20/20 Snellen acuity.
Binocular acuities with the participants’ habitual spectacles were compared to the binocular study lens acuities. The median (IQR) binocular visual acuity when wearing habitual spectacles was −0.14 (0.12) at distance and 0.04 (0.13) at near. There was not a statistically significant difference between the binocular acuities of the spectacles and study lenses with Mann–Whitney analysis at distance (P = 0.08) or at near (P = 0.3).
Study Multifocal Lenses
The mean ± standard deviation sphere power of the final study lenses was −1.75 ± 2.01 (range −5.00 to +3.25) D in the right eyes and −1.60 ± 1.98 (range −5.00 to +3.00) D in the left eyes.
Fifteen participants (60%) did not require any changes in sphere power or add at the 1-week follow-up visit. A total of 10 participants benefited from changes in power (4), add (1), or both (5) at follow-up visits to optimize prescriptions. All sphere power changes, whether at Visit 1 or at a follow-up visit, were increases in plus power. The median optimized final lens prescriptions were approximately +0.25 D greater (+0.18 in the right eyes and +0.31 in the left eyes) than the initial lens recommended by the fitting guide. This equates to +0.43 in the right eyes and +0.57 in the left eyes relative to the vertexed manifest refraction. The distribution of additional plus power accepted in the optimized lens powers is shown in Table 1. This additional plus-power improved distance and near acuity with the study lenses.
 |
Table 1 Additional Sphere Power Accepted in Optimized Contact Lens vs Fitting Guide-Advised Initial Lens |
Wear Experience Surveys
Visual analog scale (VAS) survey responses were collected from participants after one month of study lens wear and are presented in Table 2. Participants were permitted to skip a question if they did not complete the task in the question. Participants responded to the question “How willing are you to continue wearing these contact lenses after the study?” with 12 (48%) reporting they were “very likely”, 8 (32%) reporting “likely”, 3 reporting “neither unlikely nor likely”, 1 “unlikely”, and 1 “very unlikely”, all twenty-five participants selected “yes” when asked, “Would you recommend your current contact lenses to a friend?”
 |
Table 2 Median and Interquartile Ranges for Visual Analog Scale Surveys Deployed After One month of Wear with Study Lenses |
Multiple linear regression found that participant age, lens power, add power, and the previous type of contact lens worn when dropout occurred (single vision or multifocal), had no statistically significant impact upon the VAS satisfaction score, quality of vision score, or comfort score outcomes.
Discussion
Because this study population consisted of contact lens dropouts, it is reasonable to say that these individuals were potentially harder to please than the general presbyopic population. Many practitioners fear that a patient who has failed at wearing lenses previously is not a good candidate to fit with lenses again. This may be a reasonable assumption for patients who specifically dropped out of contact lens wear due to discomfort, which can be caused by ocular surface disease or other inflammatory conditions. This study enrolled patients who discontinued previous lens wear due to poor vision, and 80% of the participants who wore the lenses for 1 month said they were very likely or likely to wear the lenses after the study was complete, despite having previously discontinued wearing contact lenses. Of this group of successful participants, 13 had dropped out of multifocal lenses previously, and 7 had dropped out of single vision lens wear when unable to see adequately at both distance and near. It is unknown why this smaller cohort had not tried multifocal lenses in the past, whether individuals were reluctant to try multifocal lenses or not given the opportunity, as practitioners are known to be hesitant about fitting multifocal contact lenses.37 Interestingly, all participants – including those who were noncommittal, “unlikely” or “very unlikely” to continue wearing the study lenses - said they would recommend the lenses to a friend. It is possible that these participants view themselves as “harder to please” than their friends if they still find the lenses favorable for recommending to others.
While 80% of the study population who wore lenses during the 1-month wear period reported being likely or very likely to continue wear, the calculated success of refitting presbyopic dropouts in this study is lower if participants who did not complete the study or surveys are considered. If the three participants who chose to discontinue the study during the fitting process due to subjective concerns about vision are included, the success rate is 71%. This is higher than the 53% success rate at 1 month previously reported for refitting dropouts in soft bifocal contacts, suggesting that current optical designs can yield better refitting success than found historically.3 It is also higher than the overall intent to purchase at 1 week reported as 55% for 4 modern single use multifocal contact lenses fit on existing wearers.38
Median scores for all the quality of vision VAS survey questions were relatively high, with the lowest median score (70 out of 100) being assessed for quality of vision with smart phone use. It was surprising that this was lower than other scores, as the font size of smart phones can be enlarged. The size of the letters on the participant smartphones were not measured, so it is unknown whether participants were aware of this feature. It is likely that the font size was not enlarged in general, since quality of vision when viewing a book or magazine was ranked 7 points higher. The median scores of other quality of vision questions were even higher, however it is interesting to note that there are larger interquartile ranges for using a computer and for reading a book or magazine, indicating more variability among participant experiences in these more demanding visual tasks. The median score of 84 out of 100 for satisfaction with lenses reflects the high rate of participants who were likely to continue wearing the lenses after the study.
In this study, a follow-up visit was conducted after 1 week of wear to allow time for adaptation before an additional opportunity to check for an over-refraction. Although a majority of participants did not have any lens changes after the initial trial lenses were dispensed, 40% of participants benefitted from a change in sphere power and/or add. New multifocal lens wearers without adequate follow-up may not see optimally when adapting to the lenses and may mistakenly believe that the vision they experience with their lenses is the best this modality offers. A review paper by Pucker on contact lens dropout suggests that lack of follow-up with multifocal fitting may be the cause for a large number of multifocal dropouts.39 The success found in this study supports Pucker’s suggestion, as follow-up visits were completed to assure lenses were optimized before lenses were dispensed for 1 month. Interestingly, this study brings attention to the importance of over-refracting presbyopic patients with plus powers at distance. Experienced practitioners know that extra plus is not well tolerated with spectacle wear,40,41 and this mindset may create a tendency to assume minus powers will remedy complaints of distance blur. Giving presbyopic patients additional plus power if distance vision improves or is “the same” can benefit a multifocal contact lens wearer at both distance and near.
Poor vision has been found to contribute equally or slightly more than discomfort to contact lens dropout in presbyopic patients.42,43 The visual acuity obtained in this study at distance and near, coupled with the high subjective comfort scores, is likely a primary reason for the success rate found with the study lenses. Previous studies have also found high comfort scores with lenses made of delefilcon A.31,44 This is reflected in the current study by the median comfort score of 97 out of 100. This is compelling, since discomfort is the most common cause for overall contact lens dropout.27 The daily disposable, single-use modality was also a possible contributor to success, as previous studies reported convenience important to presbyopic patients and ranked more important than lens cost.42,45 A larger study of multifocal lens fitting, which recruited neophytes or existing contact lens wearers found higher levels of satisfaction in participants wearing low add powers compared to high add powers and higher subjective vision scores in patients with higher ametropia compared to emmetropes.46 While the analyses of subjective findings in the current study did not find a relationship between these factors and subjective VAS scores, the population of the current study only enrolled presbyopic individuals who had previously discontinued lens wear and the sample size was smaller as a result of the narrow enrollment criteria. Additional limitations of this study include the ability of participants to skip VAS survey questions, since this resulted in less than 25 responses for some questions. Potential bias may have existed due to non-random sampling, since the participants elected to participate in a study to try contact lens wear again. The use of only one lens design is a limitation of the study; it is not known if other multifocal lenses fit with attention to adaptation and over-refraction would yield similar outcomes. A longer surveillance period in addition to the surveys given after 1 month of wear may have yielded different findings in terms of the percentage of participants willing to continue lens wear.
Despite its limitations, this study demonstrates that it is possible to refit presbyopic contact lens dropouts. This is valuable because presbyopic spectacle wearers have been shown to desire contact lens correction more than non-presbyopic spectacle wearers,47 and practitioners across the globe recognize the opportunity that exists with multifocal contact lenses to enhance both patient satisfaction and clinic revenue.48 Clinical implications resulting from the study include the importance of basing contact lens powers upon a manifest refraction that minimizes minus power at distance and minimizes the add power needed for best near vision. Because these participants were willing to spend the time attending multiple visits and adapting to lenses, it is reasonable to conclude that successful fits can be attributed to those patients who begin the refitting (or fitting) process with a willingness to wear the lenses to adapt and to return for a follow-up visit. Previous publications on fitting presbyopic patients with contact lenses suggest that motivation is important to successful fitting of multifocal contact lenses.13,21,43 Reproducing the results of this study in a clinical setting would require eye care practitioners to educate new multifocal lens wearers on the need for adaptation and follow-up to optimize their lens wear experience.
In this study, 80% of participants were very likely or likely to continue wearing the study multifocals after the investigation concluded. This rate of success likely benefited from median acuities of 20/20 at near and 20/16 at distance and positive subjective assessments, including the median VAS satisfaction score of 84. These findings--coupled with the study design allowing for lens adaptation and follow-up over-refraction--demonstrate that practitioners can successfully fit presbyopic patients with the study multifocal contact lens, even among those who have previously dropped out of lens wear.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, [JSF], upon reasonable request.
Acknowledgments
Funding for this investigator-initiated trial was provided by Alcon, Inc., Fort Worth, TX, USA. Study design and execution was completed by the investigators. The project described was supported in part by Award Number Grant UM1TR004548 from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
Disclosure
Dr Jennifer Fogt reports grants from CooperVision, Alcon, Bausch+Lomb, Eyenovia, Myoptechs, Vyluma, VizionFocus; personal fees from Hoya, outside the submitted work. Dr Katherine Bickle is a clinical investigator for Johnson and Johnson Vision Care, CooperVision, Sightglass Vision, Ophtecs, Pegavision, and Hoya, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Markoulli M, Fricke TR, Arvind A, et al. BCLA CLEAR presbyopia: epidemiology and impact. Contact Lens Anterior Eye. 2024;47(4):102157. doi:10.1016/j.clae.2024.102157
2. Wolffsohn JS, Davies LN. Presbyopia: effectiveness of correction strategies. Prog Retin Eye Res. 2019;68:124–143. doi:10.1016/j.preteyeres.2018.09.004
3. Young G, Veys J, Pritchard N, Coleman S. A multi-centre study of lapsed contact lens wearers. Ophthalmic Physiol Opt. 2002;22(6):516–527. doi:10.1046/j.1475-1313.2002.00066.x
4. Wolffsohn JS, Berkow D, Chan KY, et al. BCLA CLEAR presbyopia: evaluation and diagnosis. Cont Lens Anterior Eye. 2024;47(4):102156. doi:10.1016/j.clae.2024.102156
5. Morgan PB, Efron N, Papas E, et al. BCLA CLEAR presbyopia: management with contact lenses and spectacles. Cont Lens Anterior Eye. 2024;47(4):102158. doi:10.1016/j.clae.2024.102158
6. Sullivan CM, Fowler CW. Analysis of a progressive addition lens population. Ophthalmic Physiol Opt. 1989;9(2):163–170. doi:10.1111/j.1475-1313.1989.tb00837.x
7. Muždalo NV, Mihelčič M. Individually designed PALs vs. power optimized PALs adaptation comparison. Coll Antropol. 2015;39(1):55–61.
8. Krause K. Acceptance of progressive lenses. Klin Monbl Augenheilkd. 1996;209(2–3):94–99. doi:10.1055/s-2008-1035285
9. Pedrono C, Obrecht G, Stark L. Eye-head coordination with laterally “modulated” gaze field. Am J Optom Physiol Opt. 1987;64(11):853–860. doi:10.1097/00006324-198711000-00009
10. Hutchings N, Irving EL, Jung N, Dowling LM, Wells KA. Eye and head movement alterations in naive progressive addition lens wearers. Ophthalmic Physiol Opt. 2007;27(2):142–153. doi:10.1111/j.1475-1313.2006.00460.x
11. Fernandes P, Amorim-de-Sousa A, Queirós A, Escandón-Garcia S, McAlinden C, González-Méijome JM. Light disturbance with multifocal contact lens and monovision for presbyopia. Cont Lens Anterior Eye. 2018;41(4):393–399. doi:10.1016/j.clae.2018.03.006
12. Fernandes PR, Neves HI, Lopes-Ferreira DP, Jorge JM, Gonzalez-Meijome JM. Adaptation to multifocal and monovision contact lens correction. Optom Vis Sci. 2013;90(3):228–235. doi:10.1097/OPX.0b013e318282951b
13. Pérez-Prados R, Piñero DP, Pérez-Cambrodí RJ, Madrid-Costa D. Soft multifocal simultaneous image contact lenses: a review. Clin Exp Optom. 2017;100(2):107–127. doi:10.1111/cxo.12488
14. Wolffsohn JS, Dumbleton K, Huntjens B, et al. CLEAR - Evidence-based contact lens practice. Cont Lens Anterior Eye. 2021;44(2):368–397. doi:10.1016/j.clae.2021.02.008
15. Jong M, Tilia D, Sha J, Diec J, Thomas V, Bakaraju RC. The relationship between visual acuity, subjective vision, and willingness to purchase simultaneous-image contact lenses. Optometry Vision Sci. 2019;96(4):283–290. doi:10.1097/OPX.0000000000001359
16. Diec J, Tilia D, Naduvilath T, Bakaraju RC. Predicting short-term performance of multifocal contact lenses. Eye Contact Lens. 2017;43(6):340–345. doi:10.1097/ICL.0000000000000286
17. Papas EB, Decenzo-Verbeten T, Fonn D, et al. Utility of short-term evaluation of presbyopic contact lens performance. Eye Contact Lens. 2009;35(3):144–148. doi:10.1097/ICL.0b013e3181a20361
18. Morgan PB, Efron N, Woods CA. An international survey of contact lens prescribing for presbyopia. Clin Exp Optom. 2011;94(1):87–92. doi:10.1111/j.1444-0938.2010.00524.x
19. Morgan PB, Efron N. Global contact lens prescribing 2000-2020. Clin Exp Optom. 2022;105(3):298–312. doi:10.1080/08164622.2022.2033604
20. Sivardeen A, Laughton D, Wolffsohn JS. Investigating the utility of clinical assessments to predict success with presbyopic contact lens correction. Cont Lens Anterior Eye. 2016;39(5):322–330. doi:10.1016/j.clae.2016.05.002
21. Bennett ES. Contact lens correction of presbyopia. Clin Exp Optom. 2008;91(3):265–278. doi:10.1111/j.1444-0938.2007.00242.x
22. Sulley A, Young G, Hunt C. Factors in the success of new contact lens wearers. Contact Lens Anterio. 2017;40(1):15–24. doi:10.1016/j.clae.2016.10.002
23. Sulley A, Young G, Hunt C, McCready S, Targett M-T, Craven R. Retention rates in new contact lens wearers. Eye & Contact Lens. 2018;44(1):S273–S282. doi:10.1097/ICL.0000000000000402
24. Naroo SA. Contact lens dropouts – ‘must try harder’. Contact Lens Anterior Eye. 2012;35(5):195. doi:10.1016/j.clae.2012.08.002
25. Naroo SA, Nagra M, Retallic N. Exploring contact lens opportunities for patients above the age of 40 years. Contact Lens Anterior Eye. 2022;45(6):101599. doi:10.1016/j.clae.2022.101599
26. Young G. Why one million contact lens wearers dropped out. Cont Lens Anterior Eye. 2004;27(2):83–85. doi:10.1016/j.clae.2004.02.006
27. Dumbleton K, Woods CA, Jones LW, Fonn D. The impact of contemporary contact lenses on contact lens discontinuation. Eye Contact Lens. 2013;39(1):93–99. doi:10.1097/ICL.0b013e318271caf4
28. Novillo-Díaz E, Villa-Collar C, Narváez-Peña M, Martín JLR. Fitting success for three multifocal designs: multicentre randomised trial. Cont Lens Anterior Eye. 2018;41(3):258–262. doi:10.1016/j.clae.2017.12.012
29. Gresset J. Subjective evaluation of a new multi-design progressive lens. J Am Optom Assoc. 1991;62(9):691–698.
30. Insua Pereira E, Lira M. Comfort, ocular dryness, and equilibrium water content changes of daily disposable contact lenses. Eye Contact Lens. 2018;44 Suppl 2(2):S233–s240. doi:10.1097/ICL.0000000000000441
31. Varikooty J, Keir N, Richter D, Jones LW, Woods C, Fonn D. Comfort response of three silicone hydrogel daily disposable contact lenses. Optom Vis Sci. 2013;90(9):945–953. doi:10.1097/OPX.0b013e31829d8dbf
32. Michaud L, Forcier P. Comparing two different daily disposable lenses for improving discomfort related to contact lens wear. Cont Lens Anterior Eye. 2016;39(3):203–209. doi:10.1016/j.clae.2015.11.002
33. Guthrie SE, Luensmann D, Schulze MM, Woods J, Jones L. Investigation of delefilcon A contact lenses for symptomatic daily disposable contact lens wearers with dry eye disease: a prospective comparative study. Clin Ophthalmol. 2024;18:2999–3008. doi:10.2147/OPTH.S482568
34. Lievens C, Pucker AD, Rayborn E, et al. Refitting contact lens dropouts into a modern daily disposable contact lens. Ophthalmic Physiol Opt. 2024;44(4):686–692. doi:10.1111/opo.13299
35. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
36. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
37. Walsh K, Lyndon J, Moody K. Addressing common myths and misconceptions in soft contact lens practice. Clin Exp Optometry. 2022;105(5):459–473. doi:10.1080/08164622.2021.2003693
38. Lazon de la Jara P, Sulley A, Pepe P, Walsh K, Guillon M. Multifocal contact lens success predictability. Cont Lens Anterior Eye. 2024;47(2):102105. doi:10.1016/j.clae.2023.102105
39. Pucker AD, Jones-Jordan LA, Marx S, et al. Clinical factors associated with contact lens dropout. Cont Lens Anterior Eye. 2019;42(3):318–324. doi:10.1016/j.clae.2018.12.002
40. Atchison DA, Schmid KL, Edwards KP, Muller SM, Robotham J. The effect of under and over refractive correction on visual performance and spectacle lens acceptance. Ophthalmic Physiol Opt. 2001;21(4):255–261. doi:10.1046/j.1475-1313.2001.00588.x
41. Miller AD, Kris MJ, Griffiths AC. Effect of small focal errors on vision. Optom Vis Sci. 1997;74(7):521–526. doi:10.1097/00006324-199707000-00020
42. Rueff EM, Varghese RJ, Brack TM, Downard DE, Bailey MD. A survey of presbyopic contact lens wearers in a university setting. Optom Vis Sci. 2016;93(8):848–854. doi:10.1097/OPX.0000000000000881
43. Zeri F, Di Censi M, Livi S, Ercoli A, Naroo SA. Factors that influence the success of contact lens fitting in presbyopes: a multicentric survey. Eye & Contact Lens. 2019;45(6):382–389. doi:10.1097/ICL.0000000000000606
44. Fogt JS, Weisenberger K, Fogt N. Visual performance with multifocal contact lenses and progressive addition spectacles. Cont Lens Anterior Eye. 2021;45(4):101472. doi:10.1016/j.clae.2021.101472
45. Hutchins B, Huntjens B. Patients’ attitudes and beliefs to presbyopia and its correction. J Optom. 2021;14(2):127–132. doi:10.1016/j.optom.2020.02.001
46. McParland M, Walsh K, Comoroda D, Sulley A. Wearer experience and eye care professional acceptance with a 1 day multifocal contact lens. Clin Optom. 2022;14:223–235. doi:10.2147/OPTO.S375133
47. Rueff EM, Bailey MD. Presbyopic and non-presbyopic contact lens opinions and vision correction preferences. Cont Lens Anterior Eye. 2017;40(5):323–328. doi:10.1016/j.clae.2017.03.010
48. Thite N, Desiato A, Shinde L, et al. Opportunities and threats to contact lens practice: a global survey perspective. Cont Lens Anterior Eye. 2021;44(6):101496. doi:10.1016/j.clae.2021.101496
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.