")
Back to Journals » Clinical Ophthalmology » Volume 18
Refractive Prediction Accuracy Using Intraoperative Aberrometry versus Barrett True-K Formula Following Corneal Refractive Surgery
Authors Fram NR , Davidson J, Gu X , Babu RJ, Breen M
Received 20 July 2024
Accepted for publication 16 December 2024
Published 20 December 2024 Volume 2024:18 Pages 3871—3879
DOI https://doi.org/10.2147/OPTH.S487888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nicole R Fram,1,2 John Davidson,2 Xiaolin Gu,3 Raiju J Babu,3 Michael Breen3
1Advanced Vision Care, Los Angeles, CA, USA; 2Stein Eye Institute, UCLA, Los Angeles, CA, USA; 3Alcon Vision LLC, Fort Worth, TX, USA
Correspondence: Nicole R Fram, Advanced Vision Care, 2080 Century Park East, Suite 911, Los Angeles, CA, 90067, USA, Email [email protected]
Purpose: To compare the refractive prediction accuracy of the Optiwave Refractive Analysis (ORA) SYSTEM with the Barrett True-K (BTK) formula in calculating intraocular lens (IOL) power in eyes that underwent cataract surgery after previous myopic photorefractive keratectomy (PRK) or laser-assisted in situ keratomileusis (LASIK).
Methods: This retrospective study evaluated patients aged ≥ 22 years with prior myopic PRK or LASIK who underwent unilateral or bilateral cataract removal and monofocal IOL implantation using the ORA SYSTEM at 177 sites in the United States. Two datasets were analyzed: All Eyes (ie, all eligible eyes) and First Surgery Eyes (ie, each patient’s first implanted eye). All Eyes were subgrouped by axial length (AL) and further analyzed. The main outcomes included paired differences in absolute prediction errors (APEs) between the ORA SYSTEM and BTK and differences in the proportion of eyes with APEs of ≤ 0.25 diopter (D) and ≤ 0.50 D.
Results: 1067 eyes were analyzed, including 897 First Surgery Eyes. Significantly higher proportions of All Eyes had APEs of ≤ 0.25 D (P = 0.0128) and ≤ 0.50 D (P < 0.0001) using the ORA SYSTEM than the BTK formula. Similarly, significantly higher proportions of First Surgery Eyes had APEs of ≤ 0.25 D (P = 0.0037) and ≤ 0.50 D (P = 0.0004) using the ORA SYSTEM than the BTK formula. In both datasets, mean (P < 0.0001) and median (P ≤ 0.0005) APEs were significantly lower with the ORA SYSTEM than with the BTK formula. AL did not affect the differences in prediction accuracy between these IOL power calculations.
Conclusion: In post-myopic PRK or LASIK eyes undergoing cataract surgery, the ORA SYSTEM provided significantly more accurate refractive predictability than the BTK formula, as determined by mean and median APE.
Keywords: absolute prediction error, intraoperative aberrometry, Barrett True-K formula, post-myopic corneal refractive surgery
Introduction
An increasing number of patients develop age-related cataracts and present for cataract surgery after having undergone keratorefractive surgery.1,2 These patients generally seek to achieve some level of spectacle independence and tend to have heightened expectations of excellent uncorrected vision.1 However, accurate intraocular lens (IOL) power calculation remains challenging in patients with prior keratorefractive surgery. Laser vision correction alters the curvature of the cornea in the area of the ablation zone, as well as the anterior/posterior curvature ratio, making conventional lens power calculations less accurate.2 Current methods that have been proposed to improve the accuracy of IOL power calculation in post-refractive eyes include no clinical history post-laser refractive surgery formulas, such as the Haigis-L,3 Masket,4 Shammas,5 and Barrett True-K (BTK)6–8 formulas, and combinations of conventional formulas, such as the traditional Haigis9 and Emmetropia Verifying Optical (EVO)10 formulas, with total keratometry results obtained with the optical biometer IOLMaster 700 (Carl Zeiss Meditec).
In 2013 the Optiwave Refractive Analysis SYSTEM with VerifEye (ORA SYSTEM; Alcon, Inc., Fort Worth, TX), which integrates a Talbot-Moiré aberrometer, was launched.11 The ORA SYSTEM is capable of measuring the refractive power of aphakic and pseudophakic eyes during cataract surgery, allowing for intraoperative IOL power calculation through a proprietary process that accounts for the contribution of the anterior and posterior corneal curvatures/powers to the overall refractive power of the eye.11,12 Aphakic measurements are designed to refine/confirm the IOL power (ie, sphere and total astigmatism), whereas pseudophakic readings help to adjust the orientation of an IOL in the case of a toric implantation.13 Furthermore, by including postoperative refractive data, the ORA SYSTEM can optimize IOL specific lens constants and regression coefficients used in IOL power calculations, which enable improved refractive outcomes.14
Although most studies of post-refractive eyes have reported that the ORA SYSTEM provides equal or better refractive outcomes compared with other IOL power calculation formulas, those studies included small patient populations.1,15–18 The purpose of this study was to retrospectively compare the refractive prediction accuracy of the ORA SYSTEM with the BTK formula in a large cohort of patients who underwent cataract surgery with the ORA SYSTEM after myopic photorefractive keratectomy (PRK) or laser-assisted in situ keratomileusis (LASIK). Real-world data from multiple sites in the United States were extracted from the ORA SYSTEM AnalyzOR database, and a secondary sensitivity analysis using the first surgery eye set was performed to control for bias that might have occurred when selecting the IOL power of the second eye knowing the outcome of the first eye. The effects of axial length (AL) on post-refractive outcomes were also evaluated.
Methods
Study Design
This retrospective study utilized data entered into the ORA SYSTEM AnalyzOR database from multiple sites in the United States (N = 177 sites and N = 267 surgeons) between October 2016 and February 2021. The study was conducted in accordance with the principles of the Declaration of Helsinki and in compliance with Good Clinical Practice, the US Food and Drug Administration 21 Code of Federal Regulations 812, as well as laws and regulations of foreign countries, whichever afforded greater protection to patients, and all other applicable regulations. The study protocol was approved by the Institutional Review Board of Salus, which waived the requirement for informed consent, with data collected only from sites specified in the waiver. The defined dataset was anonymized according to US HIPAA §164.514(a)-(b) privacy laws and guidelines for deidentification of personal information prior to analysis.19
Eligibility Criteria
At the time of data extraction, the ORA SYSTEM AnalyzOR database included a total of 2,096,029 eyes. The data set was limited by the specific inclusion/exclusion criterion in the planned analysis. Eligible patients in the database had to be aged ≥22 years, had to have a history of undergoing myopic PRK or LASIK, and had to have been implanted with AcrySof monofocal IOLs (models SN60WF, SA60WF, SN60AT, or SA60AT; Alcon, Inc., Fort Worth, TX) at the time of cataract surgery. Refined ORA regression coefficients and global or personalized surgeon factors had been assigned to all IOLs. All included patients had undergone cataract extraction by phacoemulsification in at least one eye, with the ORA SYSTEM providing assistance with IOL power selection. Eyes with a history of ocular disease, an absolute prediction error (APE) of ≥ 2.75 diopters (D), a history of radial keratotomy, or unavailable preoperative, intraoperative, and/or postoperative data (with at least 10 days follow-up) were excluded from the study.
Data Collection
The ORA AnalyzOR database includes data recorded by surgeons regarding the IOL power calculation formula used during pre-operative planning and the IOL power suggested by the formula. During the study period between October 2016 and February 2021, the database did not record the BTK version used or lens constant information.
Clinical data recorded included preoperative keratometry, AL, and white-to-white measurement. Preoperative data also included the IOL power calculated using the preoperative measurements and the BTK formula, as well as the predicted postoperative spherical equivalent as determined by the calculation of preoperative IOL power. The primary endpoints for comparison were the differences in the percentages of eyes in which the APEs for the IOLs implanted were ≤ 0.50 D and ≤ 0.25 D, as determined by the ORA SYSTEM and the BTK formula, and the differences in means and medians of the APEs obtained with the ORA SYSTEM and the BTK formula. The absolute ORA SYSTEM prediction error for the IOL implanted was defined as the absolute value of the difference between the manifest refraction spherical equivalent (MRSE) predicted intraoperatively by the ORA SYSTEM for the IOL implanted and the actual MRSE achieved by the IOL implanted. The APE for the IOL power calculated preoperatively using the BTK was back calculated by taking the difference between the MRSE predicted by the formula and the MRSE that would have been achieved if the preoperatively planned IOL had been implanted, taking into account the difference between the power of the IOL implanted and the power of the IOL calculated preoperatively at the spectacle plane. Postoperative MRSE was included in the analysis if it was determined ≥10 days after surgery.
The primary end points were assessed using two analysis sets: All Eyes and First Surgery Eyes. The All Eyes set contained all eligible eyes and was also used for subgroup analyses by AL (< 26 mm vs ≥ 26 mm). The First Surgery Eyes set contained each eligible patient’s first implanted eye according to the earliest surgery date in the case of bilateral implantation and was considered secondary as a supportive sensitivity analysis. No safety or follow-up data were included, as the data collection was retrospective in nature and based on real-world data entered into the ORA SYSTEM AnalyzOR database.
Statistical Analysis
Statistical analysis was performed using SAS software (SAS Institute Inc., Cary, NC). No sample size calculation was conducted for this analysis. Differences between the refractive outcomes of the ORA SYSTEM and BTK formula were tested with paired Chi-squared tests (for proportions), paired t-tests (for means), and Wilcoxon signed-rank tests (for medians). The superiority of the ORA SYSTEM over the BTK formula in the All Eyes and First Eye sets and in subgroups stratified by AL was tested by applying one-sided tests, with statistical significance defined as a P value of < 0.025.
Results
The All Eyes set consisted of 1067 eyes, with refractive results collected an average 44.9 days postoperatively (Table 1). All patients had a history of myopic PRK or LASIK and had undergone unilateral or bilateral IOL implantation. The First Surgery Eyes set consisted of 897 (84.1%) of the 1067 eyes. The most commonly implanted IOL model was SN60WF (79.1%; 844/1067), followed by SA60WF (18.2%; 194/1067), SA60AT (1.8%; 19/1067), and SN60AT (0.9%; 10/1067).
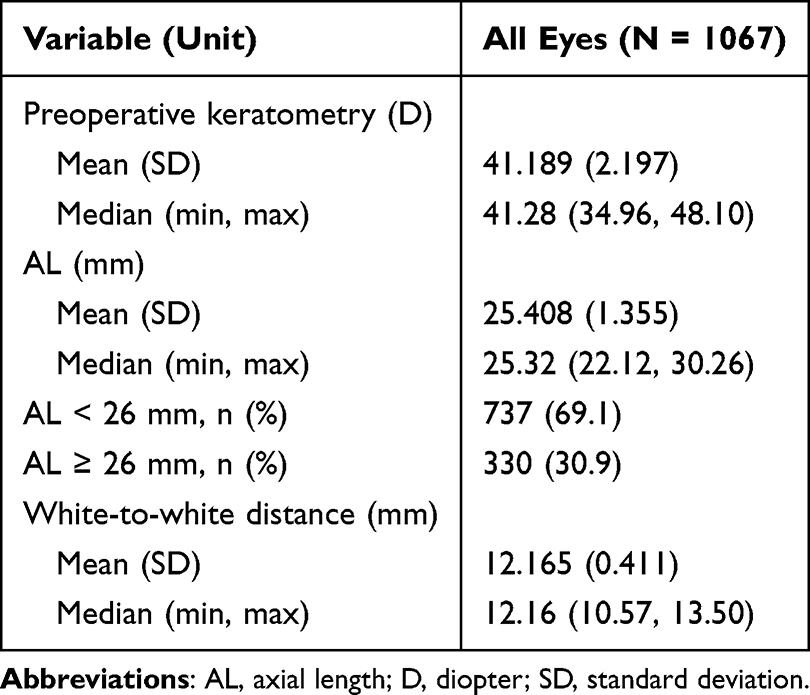 |
Table 1 Ocular Baseline Characteristics in the All Eyes Set (N = 1067) |
Analyses of the All Eyes set showed that, compared with the BTK formula, use of the ORA SYSTEM resulted in significantly higher proportions of eyes with APEs of ≤0.25 D (47.2% vs 42.5%, P = 0.0128) and ≤0.50 D (76.2% vs 69.3%, P < 0.0001), resulting in differences of 4.7% and 6.9%, respectively (Figure 1A). In addition, significantly lower mean and median APEs were achieved with the ORA SYSTEM than the BTK formula, with paired differences of –0.060 D (0.36 D vs 0.42 D, P < 0.0001) and –0.020 D (0.27 D vs 0.32 D, P = 0.0001), respectively (Figure 1B). The mean arithmetic prediction errors determined by the ORA SYSTEM and the BTK formula for All Eyes did not differ significantly (Table 2).
 |
Table 2 Mean Arithmetic Prediction Errors Determined by the ORA SYSTEM and the BTK Formula for All Eyes and for First Surgery Eyes |
 |
Figure 1 Proportion of eyes with postoperative APE ≤ 0.25 D or ≤ 0.50 D (A) and mean and median (B) APEs in the All Eyes set (N = 1067) with the BTK formula and the ORA SYSTEM. Abbreviations: APE, absolute prediction error; BTK, Barrett True-K; D, diopter; ORA, Optiwave Refractive Analysis. |
Similarly, analyses of the First Surgery Eyes set showed that, compared with the BTK formula, use of the ORA SYSTEM resulted in significantly higher proportions of eyes with APEs of ≤0.25 D (46.8% vs 40.9%, P = 0.0037) and ≤0.50 D (75.5% vs 69.1%, P = 0.0004) using the ORA SYSTEM than the BTK formula, resulting in differences of 5.9% and 6.4%, respectively (Figure 2A). In addition, mean and median APEs were significantly lower when using the ORA SYSTEM than the BTK formula, with paired differences of –0.058 D (0.37 D vs 0.42 D, P < 0.0001) and –0.025 D (0.28 D vs 0.33 D P = 0.0005), respectively (Figure 2B). Similar to results observed for All Eyes, the mean arithmetic prediction errors determined by the ORA SYSTEM and the BTK formula for First Surgery Eyes did not differ significantly (Table 2).
 |
Figure 2 Proportion of eyes with postoperative APE ≤ 0.25 D or ≤ 0.50 D (A) and mean and median APEs (B) in the First Surgery Eyes set (n = 897) with the BTK formula and the ORA SYSTEM. Abbreviations: APE, absolute prediction error; BTK, Barrett True-K; D, diopter; ORA, Optiwave Refractive Analysis. |
Statistically significant differences between the ORA SYSTEM and the BTK formula were also observed when eyes from the All Eyes dataset were subgrouped by AL (Figure 3). The proportion of eyes with an AL of < 26 mm and APE of ≤ 0.50 D was significantly higher using the ORA SYSTEM than the BTK formula (78.2% vs 71.2%, P = 0.0002; Figure 3A). Compared with the BTK formula, the ORA SYSTEM resulted in significantly lower mean (0.34 D vs 0.39 D, paired difference of –0.049 D, P = 0.0002) and median (0.26 D vs 0.30 D, paired difference of –0.025 D, P = 0.0005) APEs (Figure 3B). Similarly, the proportion of eyes with an AL of ≥ 26 mm and APE of ≤ 0.50 D was significantly higher using the ORA SYSTEM than the BTK formula (71.8% vs 64.8%, P = 0.0279; Figure 3C). Compared with the BTK formula, the ORA SYSTEM resulted in significantly lower mean (0.40 D vs 0.49 D, paired difference of –0.091 D, P = 0.0006) and marginally lower median (0.31 D vs 0.37 D, paired difference of –0.010 D, P = 0.0817) APEs (Figure 3D).
 |
Figure 3 Proportion of eyes with postoperative APE ≤ 0.25 D or ≤ 0.50 D (A and C) and mean and median APEs (B and D) of All Eyes for AL < 26 mm (A and B) or AL ≥ 26 mm (C and D). P values of < 0.025 demonstrated statistical significance in favor of the ORA SYSTEM being superior to the BTK formula. Abbreviations: AL, axial length; APE, absolute prediction error; BTK, Barrett True-K; D, diopter; ORA, Optiwave Refractive Analysis. |
Discussion
Patients who have undergone successful keratorefractive surgery, resulting in excellent uncorrected vision and spectacle independence, also have high expectations for a similarly successful cataract surgery.1 Nevertheless, calculating the optimal IOL power is challenging in post-refractive eyes.2 After corneal tissue ablation via keratorefractive surgery, conventional keratometry methods assuming a fixed ratio of anterior to posterior corneal curvature to extrapolate corneal power are subject to inaccuracy. A hyperopic refractive result after myopic LASIK is primarily due to an overestimation of the corneal power, whereas a myopic refractive result after hyperopic LASIK is primarily due to underestimation of corneal power.2
The errors inherent in conventional keratometry methods in post-refractive eyes have led to the development of advanced IOL power calculation formulas, such as the Haigis-L,3 Masket,4 Shammas,5 and BTK6–8 formulas, and the introduction of intraoperative aberrometry during cataract surgery.9–11 In post-refractive eyes, the Haigis-L, Masket, Shammas, and BTK formulas have been shown to achieve an APE ≤0.50 D in 45.5% to 93.3% of eyes.3,4,16,20 The BTK formula incorporates a modified double-K method with separate algorithms for previous hyperopic and myopic procedures. Not only can this formula incorporate measurements of keratometry and refraction before and after laser correction,3,4,20 but also calculate the required power of the IOL in the absence of pre-refractive surgery measurements (no-history formula).6 BTK has been shown to achieve equal or better refractive predictability than other formulas including the Shammas and Haigis-L formulas.6 The ORA SYSTEM was found to provide refractive outcomes in post-refractive eyes that were equal to or better than outcomes obtained with the Haigis-L, Shammas, and Masket formulas.1,16 For example, a study of 116 eyes from 79 patients reported that a higher proportion of post-myopic eyes achieved refractive outcomes with an APE ≤0.50 D following keratorefractive surgery using the ORA SYSTEM (73%) than using the BTK formula (69%), although the difference was not statistically significant.16
To our knowledge, the present study is the largest investigation to date to retrospectively compare the refractive prediction accuracy of the ORA SYSTEM with the BTK formula to determine IOL power in post-myopic PRK and LASIK eyes. The primary outcome measures were the proportion of eyes with APEs of ≤ 0.25 and ≤ 0.50 D and the mean and median APEs. Similar to a previous study,16 reasonably accurate refractive outcomes were observed using the BTK formula and ORA SYSTEM. Additionally, significantly higher proportions of eyes had APEs ≤ 0.25 D and ≤ 0.50D with the ORA SYSTEM than with the BTK formula, with the ORA SYSTEM resulting in lower mean and median APEs.
This study also evaluated the mean arithmetic prediction errors in both groups. Not surprisingly, the between-group differences in these errors were not statistically significant. Using the mean arithmetic prediction errors (signed values) usually results in means that are very close to 0.00 because both hyperopic and myopic errors are included. Inasmuch as the numbers and magnitudes of minus errors are usually similar to the numbers and magnitudes of plus errors, the means are generally very close to 0.00. Thus, the absolute values of the prediction errors are usually used when measuring and comparing prediction errors, as these absolute values are more accurate than arithmetic values in representing the magnitude of the error. Interestingly, the range of errors reported in the present study were smaller for ORA than for the BTK formula.
The improved refractive predictive accuracy of the ORA SYSTEM may be due to its ability to measure the refractive error of the aphakic eye intraoperatively, thus improving the IOL power calculation by incorporating the aphakic spherical equivalent.11,12,21 With ORA, the aphakic spherical equivalent is calculated using the aphakic sphere and the total refractive astigmatism of the eye, taking into account the total corneal power. Adapting total keratometry (TK) measurements has shown benefits within the existing framework of post-refractive IOL power calculation methods. For example, calculation of IOL power in post-myopic LASIK or PRK eyes using a combination of the Haigis formula and TK measurement resulted in a greater proportion of eyes having an APE ≤ 0.50 D compared with calculations using the Haigis formula alone (N =53; 58.5% vs 35.8%, respectively).9 The Barrett True-K formula was recently updated (BTK-TK) to incorporate measurements of posterior corneal astigmatism (PCA). A recent study of 40 eyes showed that a statistically significantly higher percentage of eyes that had undergone post-myopic keratorefractive surgery had APEs ≤ 0.50 D with the BTK TK formula than the BTK formula (75% vs 62.5%).7 Similarly, another study reported that the BTK TK formula, when compared with the BTK formula, increased the proportion of eyes with APEs ≤ 0.50 D in patients who had previously undergone myopic keratorefractive surgery (N = 116 eyes; 72% vs 69%, respectively).16 Similar proportions of eyes using ORA (73%) were reported to have APE ≤0.50 D, although the difference in mean APE was not statistically significant when determined by either BTK or BTK-TK.16
According to the manufacturer, the ORA SYSTEM AnalyzOR database allows for optimization of the lens constants and lens-specific regression coefficients used in the SYSTEM’s proprietary IOL power formula, with postoperative data input into the database. The present study included data of patients implanted with four IOL models from the same platform, for which refined regression coefficients and global or personalized lens constants were utilized. This feature may have also contributed to the improved refractive outcomes observed with the ORA SYSTEM calculations and resulted in statistically significant differences in mean APE as well as the distributions of APEs, when compared with the BTK formula.
Despite advances in IOL power calculation methods, residual refractive errors still occur following cataract surgery due to difficulties in predicting effective lens position and ocular surface considerations. Confounding factors, such as unstable tear film during preoperative biometry measurements, can also alter the accuracy of IOL calculations.22,23 An APE ≤0.50 D is generally regarded as being on target, whereas an APE >0.50 D has been associated with a refractive miss and an undesired patient outcome, possibly needing further refractive enhancements.24
A retrospective analysis of 32,189 eyes found that the mean (0.30 D ± 0.26 vs 0.36 ± 0.32 D, P < 0.0001) and median (0.24 D vs 0.29 D, P < 0.0001) APEs were significantly lower, and that the percentage of eyes with APEs ≤0.50 D was significantly higher (81.9% vs 75.9%, P < 0.0001), using intraoperative aberrometry than conventional preoperative planning.24 In addition, evaluation of the 12,779 eyes in which the power of the preoperative planned and actually implanted IOLs showed that the percentage with APEs ≤0.50 D was significantly higher using intraoperative aberrometry than conventional preoperative planning alone (81.3% vs 68.8%, P < 0.0001). These findings suggested that the introduction of intraoperative aberrometry to the surgical cataract procedure may be beneficial, not only to surgeons concerned about missing the refractive target, but also to patients seeking emmetropia following myopic keratorefractive surgery. No formula, however, including that of the ORA System, can currently achieve 100% accuracy in calculating optimal IOL following myopic keratorefractive surgery.
Errors in preoperative estimation of effective lens position, postoperative manifest refraction, and inaccurate preoperative AL measurements have been reported to be the largest contributors to errors in IOL power calculations (35%, 27%, and 17%, respectively).25 In the present study, AL did not affect the difference in refractive accuracy observed between the two IOL power calculation approaches, with the ORA SYSTEM having statistically significantly better results in all study end points in eyes with an AL of < 26 mm (except in a proportion of eyes with APEs ≤ 0.25 D), and in mean APE in eyes with an AL of ≥ 26 mm. These findings suggest that intraoperative aberrometry may enhance the accuracy of IOL power calculations in post-myopic keratorefractive eyes, especially those with an AL < 26 mm. However, care should be taken when extrapolating these results to real-world practice, as subgroup analysis by AL was not weighted.
The main limitation of this study was its retrospective design, which did not allow for full monitoring of data captured in the database, as would a prospective study. The numbers of eyes that underwent PRK and LASIK could not be determined in the database extraction, and access to patients’ raw clinical data was not possible. Furthermore, the AnalyzOR Database used in this study currently cannot distinguish between with-History and No-History methods or between with and without PCA measurements for the BTK formula.
Conclusion
This large retrospective analysis of post-myopic PRK or LASIK eyes implanted with AcrySof monofocal IOLs at multiple centers showed that the ORA SYSTEM produces refractive outcomes with significantly greater accuracy than the BTK formula alone, as demonstrated by the achievement of lower APEs. However, prospective studies are needed to more thoroughly evaluate the refractive predictability of IOL power calculation compared with multiple formulae, including the BTK-TK, EVO, and emerging AI formulae, in post-myopic keratorefractive surgery patients. The use of large database analyses and optimization and future artificial intelligence-based formulae may offer significant advances and promise to improve IOL calculations in patients who have undergone myopic keratorefractive surgery.
Acknowledgments
The authors thank BelMed Professional Resources for editorial assistance in the preparation of the manuscript, with funding from Alcon Research LLC.
Disclosure
Nicole R. Fram and John Davidson are ophthalmological surgeons who contributed to the data cited in this study, as well as being consultants and speakers for Alcon; Xiaolin Gu and Raiju J Babu are employees of Alcon, and Michael Breen was an employee of Alcon at the time of this study.
Presented at: the American Academy of Ophthalmology Meeting, November 12–15, 2021; New Orleans, Louisiana; and the American Society of Cataract and Refractive Surgery, July 23–27, 2021, Las Vegas, Nevada.
References
1. Ianchulev T, Hoffer KJ, Yoo SH, et al. Intraoperative refractive biometry for predicting intraocular lens power calculation after prior myopic refractive surgery. Ophthalmology. 2014;121(1):56–60. doi:10.1016/j.ophtha.2013.08.041
2. Savini G, Hoffer KJ. Intraocular lens power calculation in eyes with previous corneal refractive surgery. Eye Vis. 2018;5:18. doi:10.1186/s40662-018-0110-5
3. Haigis W. Intraocular lens calculation after refractive surgery for myopia: Haigis-L formula. J Cataract Refract Surg. 2008;34(10):1658–1663. doi:10.1016/j.jcrs.2008.06.029
4. Masket S, Masket SE. Simple regression formula for intraocular lens power adjustment in eyes requiring cataract surgery after excimer laser photoablation. J Cataract Refract Surg. 2006;32(3):430–434. doi:10.1016/j.jcrs.2005.12.106
5. Shammas HJ, Shammas MC. No-history method of intraocular lens power calculation for cataract surgery after myopic laser in situ keratomileusis. J Cataract Refract Surg. 2007;33(1):31–36. doi:10.1016/j.jcrs.2006.08.045
6. Abulafia A, Hill WE, Koch DD, Wang L, Barrett GD. Accuracy of the Barrett True-K formula for intraocular lens power prediction after laser in situ keratomileusis or photorefractive keratectomy for myopia. J Cataract Refract Surg. 2016;42(3):363–369. doi:10.1016/j.jcrs.2015.11.039
7. Lawless M, Jiang JY, Hodge C, Sutton G, Roberts TV, Barrett G. Total keratometry in intraocular lens power calculations in eyes with previous laser refractive surgery. Clin Exp Ophthalmol. 2020;48(6):749–756. doi:10.1111/ceo.13760
8. Lanza M, Ruggiero A, Ha J, Simonelli F, Kane JX. Accuracy of formulas for intraocular lens power calculation after myopic refractive surgery. J Refract Surg. 2022;38(7):443–449. doi:10.3928/1081597X-20220602-01
9. Wang L, Spektor T, de Souza RG, Koch DD. Evaluation of total keratometry and its accuracy for intraocular lens power calculation in eyes after corneal refractive surgery. J Cataract Refract Surg. 2019;45(10):1416–1421. doi:10.1016/j.jcrs.2019.05.020
10. Yeo TK, Heng WJ, Pek D, Wong J, Fam HB. Accuracy of intraocular lens formulas using total keratometry in eyes with previous myopic laser refractive surgery. Eye. 2021;35(6):1705–1711. doi:10.1038/s41433-020-01159-5
11. Wiley WF, Bafna S. Intra-operative aberrometry guided cataract surgery. Int Ophthalmol Clin. 2011;51(2):119–129. doi:10.1097/IIO.0b013e31820f226d
12. Woodcock MG, Lehmann R, Cionni RJ, Breen M, Scott MC. Intraoperative aberrometry versus standard preoperative biometry and a toric IOL calculator for bilateral toric IOL implantation with a femtosecond laser: one-month results. J Cataract Refract Surg. 2016;42(6):817–825. doi:10.1016/j.jcrs.2016.02.048
13. Blaylock JF, Hall B. Astigmatic results of a diffractive trifocal toric IOL following intraoperative aberrometry guidance. Clin Ophthalmol. 2020;14:4373–4378. doi:10.2147/OPTH.S285711
14. Davidson J, Gu X, Breen M, Babu RJ. Impact of global optimization of lens constants on absolute prediction error for final IOL power selection when using intraoperative aberrometry. Clin Ophthalmol. 2022;16:3155–3164. doi:10.2147/OPTH.S369797
15. Fram NR, Masket S, Wang L. Comparison of intraoperative aberrometry, OCT-based IOL formula, Haigis-L, and Masket formulae for IOL power calculation after laser vision correction. Ophthalmology. 2015;122(6):1096–1101. doi:10.1016/j.ophtha.2015.01.027
16. Christopher KL, Patnaik JL, Miller DC, Lynch AM, Taravella MJ, Davidson RS. Accuracy of intraoperative aberrometry, Barrett True-K with and without posterior cornea measurements, Shammas-PL, and Haigis-L formulas after myopic refractive surgery. J Refract Surg. 2021;37(1):60–68. doi:10.3928/1081597X-20201030-02
17. Sandoval HP, Serels C, Potvin R, Solomon KD. Cataract surgery after myopic laser in situ keratomileusis: objective analysis to determine best formula and keratometry to use. J Cataract Refract Surg. 2021;47(4):465–470. doi:10.1097/j.jcrs.0000000000000472
18. Soifer M, Passi SF, Wisely CE, et al. Refractive outcomes using intraoperative aberrometry for highly myopic, highly hyperopic, and post-refractive eyes. J Refract Surg. 2021;37(9):609–615. doi:10.3928/1081597X-20210609-03
19. Department of Health and Human Services. HIPAA privacy rule; Title 45, Part 164; 2020. National Archives, Code of Federal Regulations. Available from: https://www.ecfr.gov/current/title-45/subtitle-A/subchapter-C/part-164.
20. Zhang Q, Hou Y, Cao X, et al. Predictors of visual recovery in patients with macular edema secondary to central retinal vein occlusion after treatment with Conbercept. BMC Ophthalmol. 2021;21(1):402. doi:10.1186/s12886-021-02174-0
21. Gouvea L, Sioufi K, Brown CE, Waring G, Chamon W, Rocha KM. Refractive accuracy of Barrett True-K vs intraoperative aberrometry for IOL power calculation in post-corneal refractive surgery eyes. Clin Ophthalmol. 2021;15:4305–4315. doi:10.2147/OPTH.S334489
22. Hiraoka T, Asano H, Ogami T, et al. Influence of dry eye disease on the measurement repeatability of corneal curvature radius and axial length in patients with cataract. J Clin Med. 2022;11(3):710. doi:10.3390/jcm11030710
23. Kim J, Kim MK, Ha Y, Paik HJ, Kim DH. Improved accuracy of intraocular lens power calculation by preoperative management of dry eye disease. BMC Ophthalmol. 2021;21(1):364. doi:10.1186/s12886-021-02129-5
24. Cionni RJ, Dimalanta R, Breen M, Hamilton C. A large retrospective database analysis comparing outcomes of intraoperative aberrometry with conventional preoperative planning. J Cataract Refract Surg. 2018;44(10):1230–1235. doi:10.1016/j.jcrs.2018.07.016
25. Norrby S. Sources of error in intraocular lens power calculation. J Cataract Refract Surg. 2008;34(3):368–376. doi:10.1016/j.jcrs.2007.10.031
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.