")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Relationship Between Body Composition and Hypertension in Postmenopausal Women with Osteoporosis—A Single-Center Cross-Sectional Study
Authors Jiang S , Fu Y, Chen L, Qiu Y
Received 3 January 2025
Accepted for publication 5 May 2025
Published 14 May 2025 Volume 2025:18 Pages 1587—1598
DOI https://doi.org/10.2147/DMSO.S515563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jae Woong Sull
Shu Jiang,1,* Yu Fu,2,* Lu Chen,2 Yi Qiu2
1Department of Echocardiography and Cardiology, The First People’s Hospital of Changzhou, Changzhou, Jiangsu Province, 213003, People’s Republic of China; 2Department of Clinical Nutrition, The First People’s Hospital of Changzhou, Changzhou, Jiangsu Province, 213003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lu Chen; Email [email protected] Yi Qiu, Email [email protected]
Objective: To research the association among body composition and the presence or absence of comorbid hypertension in postmenopausal women with osteoporosis.
Methods: Postmenopausal osteoporosis sufferers according to whether they are combined with hypertension or not were divided into two groups: hypertension-negative group and hypertension-positive group. Compare the indicators of the two groups, find out the independent influencing factors, and test the test effect of influencing factors. Establish a prediction model and analyse the relationship between the prediction model and blood pressure.
Results: There were statistical differences in age, 25-hydroxyvitamin D, uric acid, homocysteine, history of diabetes, high-density lipoprotein cholesterol, body mass index (BMI), waist circumference (WC), body fat mass (BFM), body fat percentage (PBF) and visceral fat area (VFA) between two groups. Logistic analysis showed that BFM and VFA were independent influencing factors for hypertension, with for BFM (OR, 0.46; 95% CI, 0.24– 0.90; p=0.024) and VFA (OR, 1.06; 95% CI, 1.01– 1.13; p=0.031). Based on the body composition parameters of BMI, WC, BFM, PBF and VFA, the area under the curve of the prediction model for detecting hypertension was 0.694 by receiver-operating characteristic test (p < 0.001). Using generalized additive model, the predictor were found to have a significant dose-response relationship with systolic blood pressure (SBP), but not with diastolic blood pressure.
Conclusion: BFM and VFA are independent influencing factors for hypertension in postmenopausal osteoporosis patients. In postmenopausal osteoporosis patients, the predictive model composed of body composition related parameters has certain significance in predicting whether postmenopausal osteoporosis is complicated with hypertension. The effect of the prediction model on blood pressure was mainly reflected in SBP.
Keywords: body composition, osteoporosis, hypertension, body fat mass, visceral fat area
Background
Osteoporosis can occur at all ages, with postmenopausal women and the elderly being the most prevalent groups. 2021 data from the 7th China Population Survey showed that older people ranked first in the world, with 264 million (18.7%) people aged 60+, and with over 190 million in the 65+ age group. With the increasing trend of population ageing, the incidence of osteoporosis is rapidly rising in China and has become a public health challenge that cannot be ignored. A comprehensive analysis of 5097 postmenopausal women in Morocco showed that the prevalence of osteoporosis in this group was 32%.1 This condition is closely linked to the decline in oestrogen levels in women after menopause, as well as increasing the risk of developing hypertension. The large-scale cross-sectional study of the NHANES (National Health and Nutrition Examination Survey) from 1999–2018 confirmed that the risk of osteoporosis in patients with hypertension is 1.69 folds greater compared to those without hypertension.2 It has also been noted that patients with osteoporosis have a markedly greater prevalence of hypertension and coronary heart disease.3
Currently, most studies have focused on osteoporosis. In this paper, postmenopausal women with osteoporosis were selected to study the risk of hypertension in this population. From the perspective of nutrition and body composition, the effect of body composition on whether postmenopausal women with osteoporosis complicated with hypertension was studied. And how to carry out reasonable lifestyle intervention to prevent the occurrence of hypertension was explored.
Methods
Study Population
During 6/2020 to 6/2023, 164 hospitalised patients with osteoporosis were selected as study subjects in the First People’s Hospital of Changzhou. All of them were postmenopausal women. The bone mineral density of the patients was measured by dual-energy X-ray bone densitometry according to the criteria of the Chinese Guidelines for the Diagnosis and Treatment of Primary Osteoporosis (2022 edition). The clinical diagnosis of osteoporosis was confirmed if the patient’s bone mineral density T value was lower than −2.5. Subsequently, the patients were categorised into a non-hypertensive group (negative group) and a hypertensive group (positive group) according to whether they were accompanied by hypertension or not. The diagnosis of hypertension was based on the Chinese Guidelines for the Prevention and Control of Hypertension 2024 (Revised), which were as follows (in the absence of antihypertensive medication): three in-office blood pressure measurements on non-simultaneous days were ≥140/90 mmHg; or the average of home self-measurement of blood pressure for five to seven consecutive days was ≥135/85 mmHg; or the results of 24-hour ambulatory blood pressure monitoring showed an average value of ≥130/80 mmHg. Patients with a history of hypertension and currently taking antihypertensive medication were classified as hypertensive even if their blood pressure was below the above criteria.
Inclusion criteria were: (1) postmenopausal women, age ranged from 45 to 85 years; (2) patients with a clear diagnosis of osteoporosis; (3) patients with a body composition analysis; (4) the data were complete. Exclusion criteria were: (1) serious underlying diseases; (2) secondary hypertension; (3) thyroid and parathyroid diseases; (4) gastrointestinal and renal diseases affecting calcium and vitamin D absorption and metabolism; (5) malignancies; (6) had taken or were taking drugs affecting bone metabolism; (7) secondary osteoporosis and osteoporotic fractures. Figure 1 presents the flowchart for this study. This study was approved by the Ethics Committee of the First People’s Hospital of Changzhou, and the approval number was (2024) Department 167. The study was carried out in accordance with the guidelines of the Declaration of Helsinki.
 |
Figure 1 Flow chart of the study population. |
Data Collection
General information: Age, past medical history, personal habits, and blood pressure indicators were collected and recorded for all patients.
Laboratory tests: were performed in our hospital and all blood samples were centrifuged, separated to be analysed within one hour of collection. The following indices were measured by colorimetric method: serum uric acid (UA), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), apolipoprotein A1, apolipoprotein B, and homocysteine (HCY).
Bone metabolism index measurement: Four millilitres of venous blood was drawn early in the morning on an empty stomach and centrifuged at 4000 x g for 5 minutes and the supernatant was taken. Roche Electrochemiluminescence Immunoassay Analyser and its accompanying kit were used to detect procollagen type I N-terminal propeptide, type I collagen C-terminal cross-linking peptide, parathyroid hormone and osteocalcin. Dual-energy X-ray bone densitometry (Hologic Discovery, USA) was used to measure the bone density of the lumbar spine (L1-4), the left femoral neck, and the femoral trochanter, and to correct for osteophytes. Before the examination, subjects were asked to remove any high-density items they were wearing and to measure their height and weight. Bone density measurements were performed by the same technician to ensure data consistency.
Body composition analysis: Body composition analyser (Biospace Co., Ltd., Korea, Inbody 770 model) was used to measure in fasting state, including: body mass index (BMI), waist circumference (WC), hip circumference, muscle circumference of the upper arm, whole body water, intracellular water, extracellular water, minerals, protein content, bone mineral content, fat-free volume, muscle volume, limb skeletal muscle mass, body fat mass (BFM), percentage body fat (PBF), Inbody score, visceral fat area (VFA), and cell counts were recorded.
Statistical Analysis
Data are presented as  or as medians with interquartile ranges for continuous variables, while categorical variables are presented as frequencies and percentages. To assess statistical differences in means and proportions between the two groups, the Mann–Whitney U-test and chi-square test were employed. A multivariate logistic regression model was constructed to investigate the association between hypertension and various parameters. Additionally, multivariate logistic regression analysis was conducted to explore the link between body composition parameters and hypertension, with significant predictors being retained in the model. The diagnostic accuracy of these predictors for hypertension was evaluated using receiver operating characteristic (ROC) curves. Furthermore, generalized additive models were applied to examine the dose-response relationship between the predictors and systolic blood pressure (SBP) as well as diastolic blood pressure (DBP). All statistical analyses were performed using R software and EmpowerStats (http://www.empowerstats.com, X&Y Solutions,Inc.,Boston,MA), with a two-sided significance level of 0.05 used to determine statistical significance.
or as medians with interquartile ranges for continuous variables, while categorical variables are presented as frequencies and percentages. To assess statistical differences in means and proportions between the two groups, the Mann–Whitney U-test and chi-square test were employed. A multivariate logistic regression model was constructed to investigate the association between hypertension and various parameters. Additionally, multivariate logistic regression analysis was conducted to explore the link between body composition parameters and hypertension, with significant predictors being retained in the model. The diagnostic accuracy of these predictors for hypertension was evaluated using receiver operating characteristic (ROC) curves. Furthermore, generalized additive models were applied to examine the dose-response relationship between the predictors and systolic blood pressure (SBP) as well as diastolic blood pressure (DBP). All statistical analyses were performed using R software and EmpowerStats (http://www.empowerstats.com, X&Y Solutions,Inc.,Boston,MA), with a two-sided significance level of 0.05 used to determine statistical significance.
Results
Baseline Data
These 164 patients were included in this study and they were categorised into hypertension negative group (n=80) and hypertension positive group (n=84) according to whether they had hypertension. Table 1 and Table 2 show the comparison of each parameter between the two groups. There were significant differences in age, history of diabetes, 25-hydroxyvitamin D, UA, HDL-C and HCY. In addition, in terms of body composition, the two groups showed significant differences in BMI, WC, BFM, PBF, and VFA.
 |
Table 1 Subgroups Based on the Presence or Absence of Hypertension and Comparison of Baseline Data Between the Two Groups |
 |
Table 2 Comparison of Body Composition Parameters Between the Two Groups According to Whether They Were Divided Into Groups with or without Hypertension |
Relationship Between the Variables and Hypertension
Binary logistic regression was carried out with hypertension as the dependent variable and age, diabetes, UA, 25-hydroxyvitamin D, HCY, TG, TC, LDL-C, HDL-C, BMI, WC, BFM, PBF and VFA as the independent variable. The results are shown in Table 3. BFM and VFA were independent influencing factors for hypertension. In Figure 2, the risk ratios of each factor are presented in the form of forest plots.
 |
Table 3 Multivariate Logistic Regression Results |
 |
Figure 2 Risk ratios for factors associated with hypertension in postmenopausal women with osteoporosis. Abbreviations: OR, Odds ratios; UA, Uric acid; HCY, Homocysteine; BMI, Body mass index; TC, Total cholesterol; TG, Triglyceride; HDL-C, High density lipoprotein cholesterol; LDL-C,Low-density lipoprotein cholesterol; WC, Waist circumference; BFM, Body Fat Mass; PBF, Percent Body Fat; VFA, Visceral fat area. |
The results of binary logistic regression with hypertension as the dependent variable and BMI, WC, BFM, PBF, VFA as the independent variables in body composition are shown in Table 4. The predictive indicator composed of BMI, WC, BFM, PBF and VFA were saved (formula =0.256BMI+0.135WC-0.772BFM+0.161PBF+0.058VFA). The predictive indicator was analyzed by logistic regression. After adjusting for Age, Diabetes, UA, 25-hydroxyvitamin D, HCY, and HDL-C, the predictive indicator was found to be independent risk factors for hypertension. In Figure 3 ROC curve analysis of the predictors showed that the area under the curve for predicting hypertension was 0.694 (p < 0.001).
 |
Table 4 Logistic Regression with the Presence or Absence of Hypertension as the Dependent Variable and Parameters Related to Body Composition as Independent Variables |
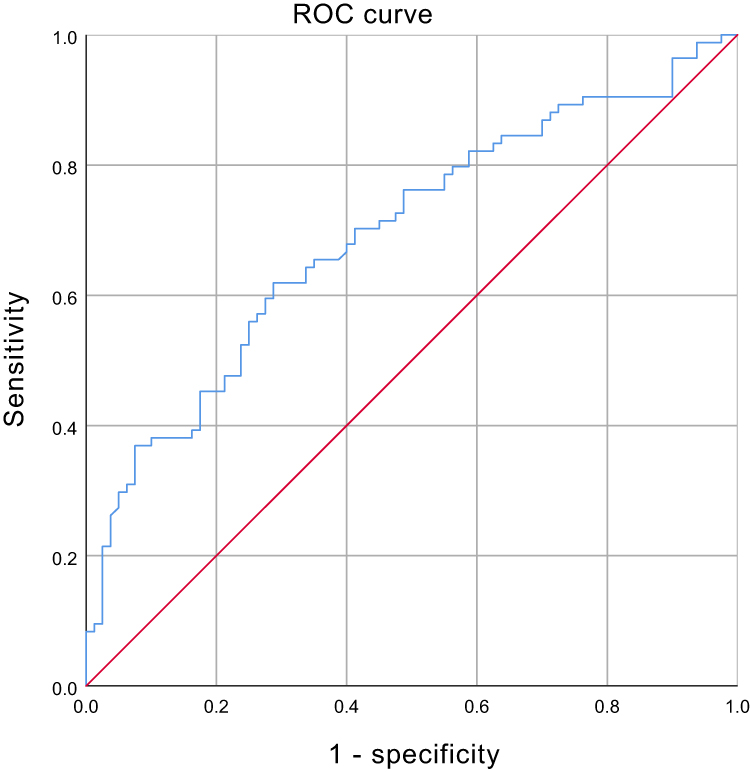 |
Figure 3 Test of the predictive value of the predictor composed of body composition parameters for whether postmenopausal women with osteoporosis have hypertension. |
Dose-Response Association Between Body Composition Predictor and SBP, DBP
The dose-response relationship between body composition predictors and SBP was investigated using a generalised additive model, and Figure 4 demonstrates the existence of a dose-response relationship between the two (p=0.004). However, there was no statistically significant relationship with DBP (p=0.488). With the increase of body composition predictor, SBP also increased, while DBP did not change significantly. Even so, it can be seen from the curve fitting that DBP showed an overall upward trend.
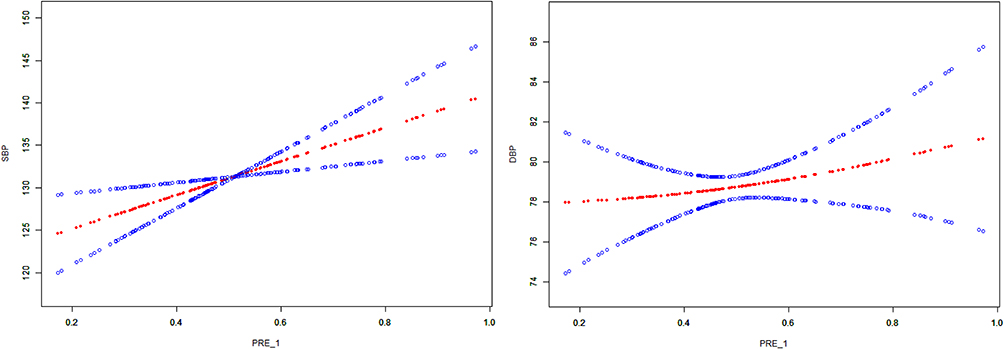 |
Figure 4 Examined dose-response relationships of the predictor with SBP and DBP using generalized additive models. The red dotted line corresponds to the smooth curve between the variables. Age, 25-hydroxyvitamin D, UA, Diabetes, HCY, HDL-C, TC, TG, LDL-C were adjusted. Abbreviations: SBP, Systolic blood pressure; DBP, Diastolic blood pressure; PRE_1, predictor composed of body composition parameters. |
Discussion
This study used a cross-sectional investigation, aiming at postmenopausal women with osteoporosis, which is special compared with the general population. Past researches found that hypertension prevalence was higher in osteoporosis patients than in non-osteoporosis patients.2 Similarly, in our study the prevalence of combined hypertension in patients with osteoporosis was about 51.2%, 24 of them were diagnosed after hospitalization, accounting for 28.6% of hypertensive patients. This indicates that many patients do not have the awareness of monitoring blood pressure, so they lack of timely and effective treatment for hypertension. Elevated blood pressure can induce structural or functional alterations in the arterial vascular system and its supply organs, ultimately resulting in target organ damage and subsequent cardiovascular and cerebrovascular events, which may lead to organ failure, including that of the heart and kidneys. A prospective observational study involving 61 populations globally (encompassing nearly 1 million individuals aged 40–89 years)4 revealed that both SBP and DBP exhibit a consistent, independent, and directly proportional relationship with the risk of stroke, coronary heart disease events, and cardiovascular mortality. Consequently, the accurate diagnosis and effective management of hypertension are of paramount importance.
A study conducted previously among Asian women revealed an association between reduced bone mineral density and the incidence of atherosclerotic cardiovascular events.5 High blood pressure is also prone to osteoporosis, the pathophysiological mechanisms underlying osteoporosis in hypertensive patients may involve the following interrelated pathways. Primary Mechanism: Hyperactivation of the renin-angiotensin-aldosterone system (RAAS) elevates circulating angiotensin II levels, which promotes accelerated bone remodeling. This enhanced bone turnover disrupts the balance between bone resorption and formation, ultimately leading to progressive reduction in bone mineral density.2,6,7 Secondary Mechanism: Chronic hypertension promotes renal calcium wasting through pressure natriuresis, thereby disrupting calcium homeostasis and triggering compensatory secondary hyperparathyroidism. The resultant elevation of parathyroid hormone (PTH) levels stimulates bone resorption through increased osteoclastic activity while simultaneously enhancing renal 1α-hydroxylase activity to amplify calcium reabsorption - a paradoxical response that exacerbates skeletal calcium depletion.8 In this study, it was found that age, 25-hydroxyvitamin D, UA, HCY, history of diabetes, and HDL-C were statistically different between the two groups of women with and without hypertension. It is well established that UA is associated with the metabolic syndrome, and therefore has an effect on blood pressure.9 Wu et al discovered that postmenopausal women diagnosed with osteoporosis typically exhibited low levels of 25-hydroxyvitamin D. After in-depth discussion of hypertensive patients with osteoporosis, it was concluded that when 25-hydroxyvitamin D content was below 42 mmol/L, blood pressure increased significantly with the decrease of 25-hydroxyvitamin D content, but when it was above 42 mmol/L, 25-hydroxyvitamin D had no such effect on blood pressure.10
Postmenopausal women experience a range of body composition changes, including increased fat mass, redistribution of adipose tissue to visceral regions, and accelerated declines in muscle mass and strength.11,12 It is well known that fat, muscle, and bone tissues are anatomically and functionally closely related, and all are influenced by common factors.13 In the field of body composition analysis, a study involved 1285 patients found that osteoporosis was significantly associated with sarcopenia. In the non-obese sarcopenic population, the highest prevalence of osteoporosis was found at the lumbar spine, full hip, and femoral neck locations, while total adiposity was positively correlated with bone mineral density at the hip and femoral neck.14 What’s more, scholars have subdivided adiposity levels by location, with high leg fat levels independently associated with lower risk of hypertension and cardiovascular-metabolic disease.15 Yang et al showed that for every unit increase in leg fat levels, the prevalence of osteoporosis was reduced by 36.9%.16
In this study, BFM and VFA were identified as independent predictors of whether patients with osteoporosis had comorbid hypertension after controlling for other potential confounders. A large cohort study in Iran explored the relationship between body composition and hypertension and found that high PBF had been related to increased increased risk of new-onset hypertension.17 Previous studies have confirmed this finding that VFA was statistically significant (p < 0.05) in a comparison of body composition between healthy women and hypertensive female patients.18
Given the results of the NHANES study, which showed a nonlinear correlation between visceral adiposity index (VAI) and skeletal muscle loss, a VAI value of 1.51 was identified as the critical tipping point, and there was a significant positive association per unit increase in VAI with the likelihood of skeletal muscle loss (OR, 2.54; 95% CI, 1.74–3.79).19
One noteworthy finding of this study is that, in the univariate analysis, both BFM and VFA were identified as risk factors. However, following the multifactorial logistic regression analysis, it was observed that BFM acted as a protective factor, while VFA was identified as a risk factor. The reason for this condition may be that fat is divided into visceral fat and subcutaneous fat. The inclusion of both variables in the logistic regression analyses yielded disparate results from those observed in the univariate analyses, which can be attributed to the influence of subcutaneous fat. Many studies have shown that visceral fats are a risk factor for cardiovascular disease, whereas subcutaneous fat has been shown to exert a protective effect.20–22
The Obesity Paradox: Previous studies have demonstrated that obesity is a risk factor for the onset of disease, but that when the disease manifests, obesity becomes a protective factor.23,24 Fat distribution is different between men and women, in women have relatively less visceral fat and more subcutaneous fat. Excess visceral fat has been linked to the development of metabolic syndrome. People with more subcutaneous fat have a lower risk of cardiovascular disease regardless of whether they have excessive visceral fat.25 This is associated with the adipokines and pro-inflammatory cytokines produced by visceral fat, such as tumour necrosis factor and interleukin-6.26
Subcutaneous fat, on the other hand, is a lower-grade inflammatory state. A retrospective study comprising 1102 participants conducted by Kim et al revealed that subcutaneous fat area is an independent prognostic indicator for femur fractures in the elderly. In addition, studies have shown that the greater the area of subcutaneous fat, the better the prognosis for elderly patients with proximal femur fractures.27 The redistribution of body fat with age reduces the amount of subcutaneous fat, which functions as a leptin-producing agent. Since leptin improves glucagon sensitivity and regulates sugar-lipid measurement and immune response, this may be the reason why subcutaneous fat reduces mortality and increases healthy longevity.28
This paper presents a study of the predictors of blood pressure in postmenopausal osteoporotic populations, with a focus on the role of body composition. The analysis revealed that predictors comprising BMI, WC, BFM, PBF, and VFA had a significant impact on SBP. There was no such effect on DBP. Kaess et al conducted a cross-sectional investigation (Framingham Heart Study 3223 participants) showing a significant correlation between visceral fat-subcutaneous fat ratio and SBP, DBP (p<0.001).29 A correlation between hypertension and visceral fat-subcutaneous fat ratio was observed in a 625-participant study in China (r=0.255).21 In the animal experiments of Nazari et al rats were fed with a moderate amount of high-fat chow and male rats were obtained to show a gradual increase in body weight, plasma triglycerides, and SBP at weeks 2, 4, and 5 of feeding, respectively.30 A cohort of specialised occupational pilots revealed a statistically significant inverse correlation between BMI, WC, PBF and SBP, DBP, mean arterial pressure (p < 0.001).31
The results of this study have implications for nutritional interventions. In older women, diets rich in meat, vegetables, dairy products, fruit and eggs have been linked to increased bone mineral density, whereas beverages and fried foods have been associated with decreased L1−432 In a Japanese study related to dietary intervention for visceral fat in male patients, it was found that Optimized Nutri-Dense Meals without strict control of total energy, limiting saturated fatty acids only to 6.2 grams per two meals is beneficial for visceral fat reduction.33 And the intake of polyphenol-rich foods has a role in controlling blood pressure in the postmenopausal female population.34 Although flaxseed is known to exert effect in lowering blood lipids, its effect on reducing volatile fatty acids remains to be demonstrated.35 In terms of probiotics, there are also studies in Poland showing that consuming the probiotic Lactobacillus acidophilus for 12 weeks can lead to significant reductions in body fat and visceral fat.36 Meanwhile the results of sedentary lifestyles on blood pressure were inconsistent, with women perhaps benefiting from exercise in comparison.37 Studies in the type 2 diabetes mellitus population have found aerobic or combined exercise to be more effective in reducing VFA, and there was no difference in visceral fat reduction with long-term interventions (>12 weeks) compared to short-term interventions.38
Conclusions
BFM and VFA are independent influencing factors for hypertension in postmenopausal osteoporosis patients. In postmenopausal osteoporosis patients, the predictive model composed of body composition related parameters has certain significance in predicting whether postmenopausal osteoporosis is complicated with hypertension. The effect of the prediction model on blood pressure was mainly reflected in SBP.
A limitation of this study is that it was a single-center retrospective study with a small sample size, which may have been influenced by selection bias and unmeasured confounding variables. Further validation through prospective cohort studies with rigorously controlled covariates is warranted to confirm the generalisability of these findings and mitigate confounding effects.
Data Sharing Statement
Raw data can be obtained upon request from the corresponding author.
Ethics Statement
This study was approved by the Ethics Committee of the First People’s Hospital of Changzhou, and the approval number was (2024) Department 167. Since our study was a retrospective observational study, the informed consent form was exempted from signing after approval from the Ethics Committee of The First People’s Hospital of Changzhou. All data were anonymized using unique study IDs, with access restricted to authorized researchers only. Original medical records remained securely stored in the hospital’s encrypted database.
Acknowledgments
We were very grateful that our study was funded by the Jiangsu Key Clinical Speciality Construction Unit (Clinical Nutrition Department), a government department from China. This work was also supported by the Applied and Basic Research Program of Changzhou Scientific and Technological Project (CJ20235089, CJ20245016), Changzhou Healthcare High-level Talent Cultivation Project (2024CZBJ004), the Major Scientific and Technological Project of Changzhou Health Commission of China (ZD202309), and Clinical Research Program of Changzhou First People’s Hospital(KY20252330).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kherrab A, Toufik H, Ghazi M, et al. Prevalence of postmenopausal osteoporosis in Morocco: a systematic review and meta-analysis. Arch Osteoporos. 2024;19(1):61. doi:10.1007/s11657-024-01421-3
2. Huang Y, Ye J. Association between hypertension and osteoporosis: a population-based cross-sectional study. BMC Musculoskelet Disord. 2024;25(1):434. doi:10.1186/s12891-024-07553-4
3. Chai H, Jirong G, Li L, et al. Hypertension is associated with osteoporosis: a case-control study in Chinese postmenopausal women. BMC Musculoskelet Disord. 2021;22(1):253. doi:10.1186/s12891-021-04124-9
4. Lewington S, Clarke R, Qizilbash N, et al. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913.
5. Park J, Elizabeth Yoon Y, Min Kim K, et al. Prognostic value of lower bone mineral density in predicting adverse cardiovascular disease in Asian women. Heart. 2021;107(13):1040–1046. doi:10.1136/heartjnl-2020-318764
6. Gao Y, Tian X, Zhang G, et al. The low bone mass density in adults with hypertension: a meta-analysis. J Orthop. 2025;63:70–76. doi:10.1016/j.jor.2024.10.041
7. Harrison DG, Coffman TM, Wilcox CS, et al. Pathophysiology of hypertension: the mosaic theory and beyond. Circ Res. 2021;128(7):847–863. doi:10.1161/CIRCRESAHA.121.318082
8. Song S, Cai X, Junli H, et al. Correlation between plasma aldosterone concentration and bone mineral density in middle-aged and elderly hypertensive patients: potential impact on osteoporosis and future fracture risk. Front Endocrinol. 2024;15:1373862. doi:10.3389/fendo.2024.1373862
9. Gómez-de-Tejada-Romero M-J, Murias-Henríquez C, Saavedra-Santana P, et al. Influence of serum uric acid on bone and fracture risk in postmenopausal women. Aging Clin Exp Res. 2024;36(1):156. doi:10.1007/s40520-024-02819-2
10. Tianlong W, Lin Z, Wang C, et al. Correlation between vitamin D levels and blood pressure in elderly hypertensive patients with osteoporosis. Front Med. 2024;11:1396254. doi:10.3389/fmed.2024.1396254
11. Marlatt KL, Pitynski-Miller DR, Gavin KM, et al. Body composition and cardiometabolic health across the menopause transition. Obesity. 2022;30(1):14–27. doi:10.1002/oby.23289
12. Khalafi M, Habibi Maleki A, Sakhaei MH, et al. The effects of exercise training on body composition in postmenopausal women: a systematic review and meta-analysis. Front Endocrinol. 2023;14:1183765. doi:10.3389/fendo.2023.1183765
13. Tencerova M, Ferencakova M, Kassem M. Bone marrow adipose tissue: role in bone remodeling and energy metabolism. Best Pract Res Clin Endocrinol Metab. 2021;35(4):101545. doi:10.1016/j.beem.2021.101545
14. Yan L, Zhenbin X. The relationship of body composition with bone mineral density and 10-year probability of hip fracture in postmenopausal women. Geriatr Nurs. 2024;59:250–255. doi:10.1016/j.gerinurse.2024.07.001
15. Shi J, Yang Z, Niu Y, et al. Large thigh circumference is associated with lower blood pressure in overweight and obese individuals: a community-based study. Endocr Connect. 2020;9(4):271–278. doi:10.1530/EC-19-0539
16. Yang L, Deng H, Pan W, et al. The inverse association of leg fat mass and osteoporosis in individuals with type 2 diabetes independent of lean mass. Diabetes Metab Syndr Obes. 2022;15:1321–1330. doi:10.2147/DMSO.S358717
17. Ali Nematollahi M, Jahangiri S, Asadollahi A, et al. Body composition predicts hypertension using machine learning methods: a cohort study. Sci Rep. 2023;13(1):6885. doi:10.1038/s41598-023-34127-6
18. Wang R, Wang Q. A differential study into body fat in healthy and hypertensive populations using multiple indexes. Diabetes Metab Syndr Obes. 2021;14:279–284. doi:10.2147/DMSO.S267366
19. Jianzhao L, Lin Y, Deng H, et al. Association of visceral adiposity index with sarcopenia based on NHANES data. Sci Rep. 2024;14(1):21169. doi:10.1038/s41598-024-72218-0
20. Yun Hwan O, Hyun Moon J, Ju Kim H, et al. Visceral-to-subcutaneous fat ratio as a predictor of the multiple metabolic risk factors for subjects with normal waist circumference in Korea. Diabetes Metab Syndr Obes. 2017;10:505–511. doi:10.2147/DMSO.S150914
21. Chiyanika C, Wai-Sun Wong V, Wong GL-H, et al. Implications of abdominal adipose tissue distribution on nonalcoholic fatty liver disease and metabolic syndrome: a Chinese general population study. Clin Transl Gastroenterol. 2021;12(2):e00300. doi:10.14309/ctg.0000000000000300
22. Abe Y, Urakami T, Hara M, et al. The characteristics of abdominal fat distribution in Japanese adolescents with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2019;12:2281–2288. doi:10.2147/DMSO.S223049
23. Guglin M. The fiction of the obesity paradox. Eur Heart J. 2023;44(39):4199. doi:10.1093/eurheartj/ehad504
24. Yuxin L, Huang Z, Gong Y, et al. Retrospective analysis of the relationship between bone mineral density and body composition in a health check-up Chinese population. Front Endocrinol. 2022;13:965758. doi:10.3389/fendo.2022.965758
25. Zhang B, Jiangshan H, Guo P, et al. Ratio of visceral fat area to body fat mass (VBR) is a superior predictor of coronary heart disease. Chin Med J. 2023;136(19):2380–2382. doi:10.1097/CM9.0000000000002601
26. Kim J-M, Chung E, Cho E-S, et al. Impact of subcutaneous and visceral fat adiposity in patients with colorectal cancer. Clin Nutr. 2021;40(11):5631–5638. doi:10.1016/j.clnu.2021.10.001
27. Kim Y-J, Seo D-W, Yousun K, et al. Subcutaneous fat area at the upper thigh level is a useful prognostic marker in the elderly with femur fracture. J Cachexia Sarcopenia Muscle. 2021;12(6):2238–2246. doi:10.1002/jcsm.12845
28. Ebadi M, Tandon P, Moctezuma-Velazquez C, et al. Low subcutaneous adiposity associates with higher mortality in female patients with cirrhosis. J Hepatol. 2018;69(3):608–616. doi:10.1016/j.jhep.2018.04.015
29. Kaess BM, Pedley A, Massaro JM, et al. The ratio of visceral to subcutaneous fat, a metric of body fat distribution, is a unique correlate of cardiometabolic risk. Diabetologia. 2012;55(10):2622–2630. doi:10.1007/s00125-012-2639-5
30. Nazari S, Mostafa Shid Moosavi S. Temporal patterns of alterations in obesity index, lipid profile, renal function and blood pressure during the development of hypertension in male, but not female, rats fed a moderately high-fat diet. Arch Physiol Biochem. 2022;128(4):897–909. doi:10.1080/13813455.2020.1739713
31. Wilson D, Driller M, Johnston B, et al. The relationship between cardiorespiratory fitness and blood pressure among airline pilots: a mediation analysis of body composition. J Hypertens. 2024;42(2):344–349. doi:10.1097/HJH.0000000000003605
32. Zhao N, Yin X, Chen L, et al. Associations of different dietary patterns, bone mineral density, and fracture risk among elderly women: the China osteoporosis prevalence study. Front Endocrinol. 2024;15:1378158. doi:10.3389/fendo.2024.1378158
33. Shobako N, Shimada H, Yamato T, et al. Visceral fat-reducing effect of novel dietary intervention program: a randomized controlled trial in Japanese males. Nutrients. 2024;16(18):3202. doi:10.3390/nu16183202
34. Sánchez-Martínez L, González-Barrio R, García-Alonso J, et al. Assessing the impact of (Poly)phenol-rich foods on cardiometabolic risk in postmenopausal women: a dietary trial. Antioxidants. 2024;13(8):973. doi:10.3390/antiox13080973
35. Lenártová P, Gažarová M, Kopčeková J, et al. Effect of crushed flaxseed consumption on cardiovascular risk indicators in menopausal women. Life. 2024;14(7):849. doi:10.3390/life14070849
36. Azmy Harahap I, Moszak M, Czlapka-Matyasik M, et al. Effects of daily probiotic supplementation with Lactobacillus acidophilus on calcium status, bone metabolism biomarkers, and bone mineral density in postmenopausal women: a controlled and randomized clinical study. Front Nutr. 2024;11:1401920. doi:10.3389/fnut.2024.1401920
37. Pinto AJ, Bergouignan A, Dempsey PC, et al. Physiology of sedentary behavior. Physiol Rev. 2023;103(4):2561–2622. doi:10.1152/physrev.00022.2022
38. Kazeminasab F, Bahrami Kerchi A, Behzadnejad N, et al. The effects of exercise interventions on ectopic and subcutaneous fat in patients with type 2 diabetes mellitus: a systematic review, meta-analysis, and meta-regression. J Clin Med. 2024;13(17):5005. doi:10.3390/jcm13175005
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Dietary Patterns and All-Cause Mortality in Individuals with Hypertension and Osteoporosis: A Retrospective Cohort Study
Guan J, Ding L, Wang Y, Zhu Z, Pan M, Du L, Yin N
Journal of Multidisciplinary Healthcare 2025, 18:3781-3791
Published Date: 30 June 2025