")
Back to Journals » Clinical Ophthalmology » Volume 18
Relationship Between Postoperative Oxidative Stress Levels and Corneal Endothelial Cell Loss After Phacoemulsification in Diabetic Patients with Cataract
Authors Gao Y, Yang N, Wei L, Yan Y, Li L
Received 20 September 2024
Accepted for publication 26 November 2024
Published 25 December 2024 Volume 2024:18 Pages 3957—3965
DOI https://doi.org/10.2147/OPTH.S497133
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yuan Gao,* Ning Yang,* LiJuan Wei, YiJie Yan, Lei Li
Department of Ophthalmology, Hainan General Hospital (Hainan Affiliated Hospital of Hainan Medical University), Haikou City, Hainan Province, 570311, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lei Li, Department of Ophthalmology, Hainan General Hospital (Hainan Affiliated Hospital of Hainan Medical University), No. 19 Xiuhua Road, Xiuying District, Haikou City, Hainan Province, 570311, People’s Republic of China, Email [email protected]
Objective: To investigate the relationship between postoperative oxidative stress and corneal endothelial cell loss in diabetic patients with cataract.
Methods: One hundred and twenty patients who underwent phacoemulsification were selected, including 80 diabetic patients with cataract and 40 patients with ordinary cataracts. Corneal endothelial cell loss was recorded, and the endothelial cell density (ECD), the proportion of hexagonal cells, and the corneal thickness within the central corneal area were compared. According to the severity of endothelial cell loss, the diabetic patients with cataract were divided into a general loss group (n = 37) and a serious loss group (n = 43), and the postoperative serum superoxide dismutase (SOD), malonaldehyde (MDA), and glutathione peroxidase (GSH-Px) were measured. The relationship between oxidative stress factors and corneal endothelial cell loss in diabetic patients with cataract was analyzed, and the predictive value of MDA, SOD, and GSH-Px was investigated by using receiver operating characteristic (ROC) curve.
Results: Diabetic patients with cataract had higher serum MDA and lower SOD and GSH-px, and higher fasting blood glucose concentration, glycosylated hemoglobin level, and low-density lipoprotein cholesterol (P < 0.05). The mean change in ECD in diabetic patients with cataract was 10.95%, which was greater than the 6.11% in non-diabetic patients with cataract (P < 0.05), and the proportion of hexagonal cells decreased and corneal thickness increased. MDA levels was negatively correlated with corneal endothelial cell loss in diabetic patients with cataract (rs = 0.509), and SOD and GSH-px were negatively correlated (rs = − 0.361, rs = − 0.482). The area under the ROC curve of MDA, SOD, and GSH-px in corneal endothelial cell loss was 0.719, 0.773, and 0.752, respectively.
Conclusion: The degree of postoperative corneal endothelial cell loss in diabetic patients with cataract was greater and positively correlated with MDA, and negatively correlated with SOD and GSH-px.
Keywords: diabetic cataract, phacoemulsification, oxidative stress, corneal endothelial cell loss, correlation
Introduction
Cataract is one of the common malignant ophthalmic diseases in clinical practice, and is the main cause of global blindness.1 Clinical studies have shown that cataracts occur more frequently and at a shorter age in diabetic patients than in non-diabetic patients.2,3 Despite the current revolution in surgical approaches to cataract treatment, postoperative damage to the corneal endothelium, remains an unavoidable problem. When the loss of corneal endothelial cells reaches a certain level, corneal endothelial dysfunction occurs, leading to persistent corneal edema, which seriously affects postoperative vision. The mechanism by which diabetes leads to corneal endothelial cell damage has not yet been clarified.
Oxidative stress is involved in the metabolism of corneal endothelial cells in diabetic patients4 and is related to diabetic cataractogenesis.5,6 Acoustic cavitation of ultrasound waves in aqueous solution during cataract phacoemulsification operation also induces oxidative stress in endothelial cells7 that leads to corneal endothelial cell damage. Superoxide dismutase (SOD), malondialdehyde (MDA), and glutathione (GSH) are known to be important indicators of oxidative stress. Hyperglycemia in diabetic patients may lead to autoxidation and non-enzymatic glycosylation, resulting in overproduction of free radicals in the lens.3 Excessive production of free radicals causes increased lipid peroxidation, and MDA, a breakdown product of polyunsaturated fatty acids under peroxidative conditions, is a standard marker of lipid peroxidation, which is significantly elevated in lenses of diabetic patients with cataract.8 SOD is the main antioxidant enzymes9 and has a protective effect on cataract.10 However, high glucose can directly inhibit SOD and trigger cataract formation in the course of diabetes.11
Based on this, this study intends to investigate the relationship between postoperative oxidative stress levels and corneal endothelial cell loss in diabetic patients with cataract, and to provide direction for the treatment of corneal endothelial cell loss caused by phacoemulsification.
Materials and Methods
Patient Information
A prospective analysis was performed with 120 cases (120 eyes) of cataract patients who underwent phacoemulsification operation in Hainan General Hospital from December 2022 to December 2023. They were 80 diabetic patients with cataract and 40 non-diabetic patients with cataract according to whether they were accompanied by diabetes or not.
Inclusion criteria: (1) Diabetic patients with cataract met the WHO criteria for non-insulin-dependent diabetes mellitus; (2) Cataracts of grade II or III (nuclear cataract grading); (3) Diabetic patients with fasting glucose less than 7 mmol/L or postprandial glucose less than 11 mmol/L.
Exclusion criteria: (1) patients with a history of ocular surgery, dry eye syndrome, uveitis, ocular inflammation, corneal clouding, glaucoma, and ocular trauma; (2) Both groups were free of keratitis, uveitis, and glaucoma; (3) There was no retinal detachment in ultrasound examination, the intraocular pressure was normal, and there were no serious intra-operative or postoperative complications; (4) patients with contraindications to phacoemulsification operation; (5) patients with severe cardiopulmonary, hepatic, and renal dysfunctions; and (6) patients with psychiatric or neurological disorders. Informed consent was obtained from the patients and the study was approved by the Ethics Committee of Hainan General Hospital.
Surgical Methods
Preoperatively, all patients underwent a complete ophthalmic evaluation including slit lamp examination, non-contact tonometer, and mydriasis examination. All patients underwent cataract extraction by phacoemulsification combined with posterior chamber intraocular lens implantation under topical anesthesia, and the procedures were performed by the same experienced ophthalmologist using the standard technique of the same machine.
Clinical Data Collection
Patients’ age, gender, body mass index (BMI), duration of cataract, hypertension, hyperlipidemia, and axial length were collected. 3 mL of preoperative fasting venous blood was collected for routine biochemical tests such as fasting blood glucose (FBG), glycosylated hemoglobin albumin (HbA1c), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C).
Detection of Oxidative Stress Level
3 mL of elbow venous blood was collected one week postoperatively, left to stand for 20 min, and centrifuged with a radius of 10 cm at 3000 r/min for 20 min. The serum to be examined was extracted. SOD, MDA, and GSH-Px were detected by enzyme-linked immunosorbent assay kits (Nanjing Jianjian Bioengineering Institute, Nanjing, China) and Bio-Tek ELX800 technique.
Determination of Corneal Endothelial Cell Loss
One week postoperatively, non-contact corneal endothelial microscopy (SP 3000P; Topcon, Tokyo, Japan) was applied to examine the surgical eye, including the density of endothelial cells in the central zone, the proportion of hexagonal cells, and the corneal thickness, and the average value was taken from three consecutive shots. Endothelial cell loss rate = (preoperative cell count - postoperative cell count/preoperative cell count) × 100%. Based on the mean value of the cell loss rate, patients with greater than the mean value were included in the serious loss group, and patients with less than or equal to the mean value were included in the general loss group.
Statistical Analysis
Statistical analysis of the study data was performed using SPSS 24.0 software, and Shapiro-Wilk test was used to test the normality of the data. Count data were expressed as % and differences between groups were compared using the χ2 test; measure data were expressed as mean ± standard deviation after the normality test, and differences between groups were compared using the t test; Mann–Whitney U was used for independent samples that were not normally distributed. The relationship between oxidative stress factors and corneal endothelial cell loss in diabetic patients with cataract was analyzed by using Spearman correlation, and the predictive value of MDA, SOD, and GSH-px in the degree of corneal endothelial cell loss in diabetic patients with cataract was explored by using receiver operating characteristic (ROC) curves. P < 0.05 was considered as a statistically significant difference. The analysis results were visualized using Graph Pad Prism 8.0.
Results
General Clinical Data
The demographic and clinical characteristics of the patients in both groups are shown in Table 1. The mean age, male to female ratio, and BMI were similar in both groups (p > 0.05). There was no significant difference between the two groups in terms of intraocular pressure, percentage of patients suffering from hypertension or hyperlipidemia, and duration of cataract (p > 0.05). Regarding ocular clinical characteristics, there were also no significant differences between the two groups in terms of axial length, anterior chamber depth, and nuclear cataract grading (p > 0.05). Unsurprisingly, FBG and HbA1c were significantly higher in the diabetic patients with cataract (p < 0.05). Diabetic patients with cataract had higher LDL-C levels compared to non-diabetic patients with cataract (p < 0.05), whereas there was no statistical difference between the two groups in terms of TC, TG, and HDL-C (p > 0.05).
 |
Table 1 Analysis of General Clinical Data of Patients in Diabetic Group and Non-Diabetic Group |
Endothelial Cell Density, Proportion of Hexagonal Cells, and Corneal Thickness
Postoperatively, endothelial cell density, hexagonal cell percentage decreased and corneal thickness increased in both groups. The mean postoperative corneal endothelial cell loss in diabetic patients with cataract was 10.95%, which was significantly greater than (p < 0.05) that in non-diabetic patients with cataract (6.11%) (corneal endothelial cell loss rates are expressed as medians in Table 2).
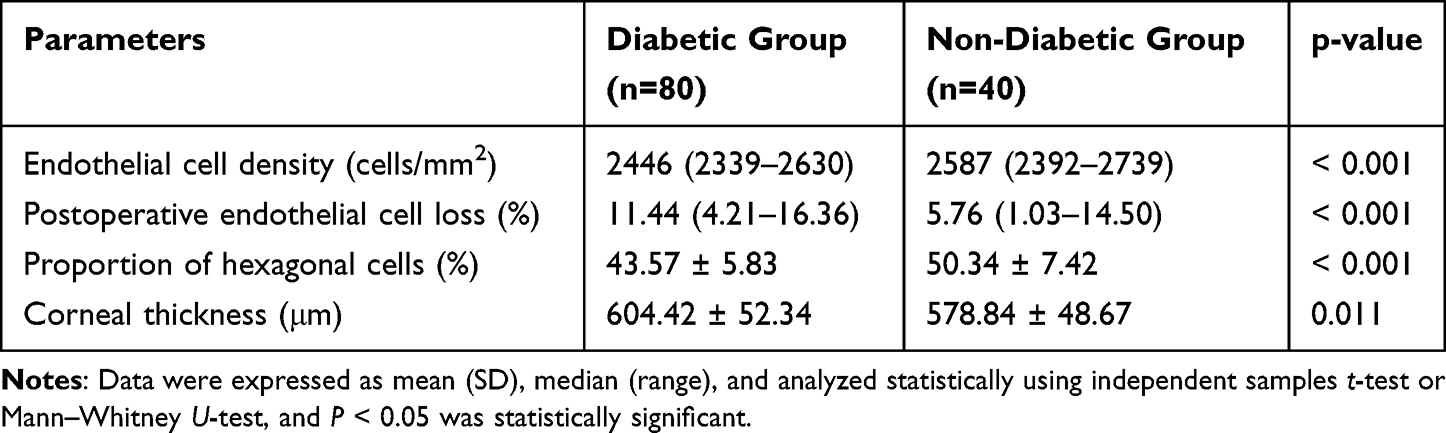 |
Table 2 Comparison of Endothelial Cell Density, Proportion of Hexagonal Cells, and Corneal Thickness in the Diabetic Group and the Non-Diabetic Group |
Postoperative Serum Levels of Oxidative Stress
As shown in Figure 1, postoperative serum SOD and GSH-px levels in diabetic patients with cataract were lower than those in non-diabetic patients with cataract, whereas MDA was higher than those in non-diabetic patients with cataract (P < 0.001). Based on the mean of the postoperative endothelial cell loss rates in the diabetic patients described above, diabetic patients with cataract were categorized into a general loss group (≤ 10.95%, n = 37) and a serious loss group (> 10.95%, n = 43) according to the magnitude of postoperative corneal endothelial cell loss. Patients in the serious loss group had lower serum SOD and GSH-px than those in the general loss group, while MDA levels were higher than those in the general loss group (P < 0.001).
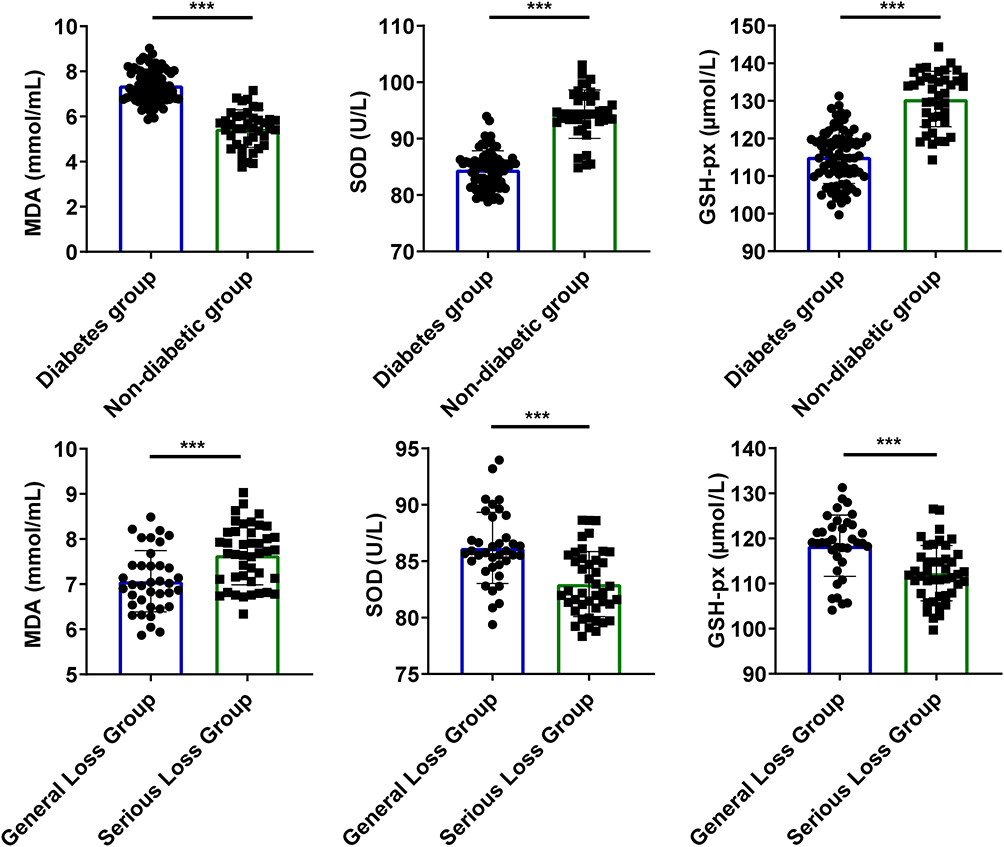 |
Figure 1 Comparison of oxidative stress levels in each group of patients (*** P < 0.001 serious loss group vs general loss group). |
Correlation Analysis Between Oxidative Stress and the Rate of Corneal Endothelial Cell Loss
To further explore the relationship between MDA, SOD, and GSH-px and corneal endothelial cell loss in diabetic patients with cataract, we performed Spearman correlation analyses of MDA, SOD, and GSH-px with the rate of corneal endothelial cell loss. The results, as shown in Figure 2, showed that MDA was positively correlated with corneal endothelial cell loss in diabetic patients with cataract (rs = 0.509), and SOD and GSH-px were negatively correlated with corneal endothelial cell loss (rs = −0.361, rs = −0.482).
 |
Figure 2 Correlation analysis of postoperative oxidative stress levels and corneal endothelial cell loss rate in diabetic patients with cataract. |
Predictive Value of Oxidative Stress Levels on Postoperative Corneal Endothelial Cell Loss in Diabetic Patients with Cataract
The ROC curves of serum MDA, SOD, and GSH-px levels in predicting postoperative corneal endothelial cell loss in diabetic patients with cataract were plotted, and the area under the curve was calculated. The area under the ROC curve of serum MDA, SOD, and GSH-px levels in predicting the degree of corneal endothelial cell loss was 0.719, 0.773, and 0.752, respectively (Table 3 and Figure 3).
 |
Table 3 Diagnostic Analysis of MDA, SOD, and GSH-Px in Postoperative Corneal Endothelial Cell Loss in Diabetic Patients |
 |
Figure 3 Receiver operating characteristic curves of MDA, SOD, and GSH-px in postoperative corneal endothelial cell loss in diabetic patients with cataract. |
Discussion
Diabetic patients are two to five times more likely to develop cataracts than non-diabetic patients.12 Impaired fasting glucose in prediabetes has also been studied as a risk factor for cataracts.13 Phacoemulsification is a common modality for the treatment of cataracts although the intraoperative ultrasound energy damages the corneal cells, leading to loss of corneal endothelial cells.14,15 Endothelial cell density (ECD) loss is greater in diabetic patients with cataract compared to non-diabetic patients.14,16,17 The present study found that in diabetic patients with cataract, their ECD loss rate was higher, reaching 10.95%, compared to only 6.11% in non-diabetic patients with cataract. Diabetic patients with cataract had thicker corneal thickness and lower percentage of hexagonal cells postoperatively compared to non-diabetic patients with cataract.
Opacity of the lens is the main manifestation of cataracts.3 Maintaining lens transparency requires a balance of the redox state, and oxidative stress induced by hyperglycemia and an increase in intracellular mitochondrial reactive oxygen species (ROS) are now considered to be central to the pathogenesis of chronic complications of diabetes mellitus.18 The enzymatic activity of GSH may be reduced in the lens of diabetic patients. GSH levels are significantly reduced in the Diabetic lens as compared to non-diabetic samples.8 SOD activity is significantly reduced in the lens of diabetic patients.19,20 MDA has been found to be an important component of the lipid profile of cataractous lenses. Several studies have found that MDA, a major product of lipid peroxidation, is expressed at higher levels in the lens and plasma of diabetic patients with cataract.21,22 Our findings showed similar results, indicating that SOD and GSH-px were significantly lower in diabetic patients with cataract, whereas MDA was significantly higher compared with non-diabetic patients with cataract. In a subgroup of diabetic patients with cataract, we found that patients with severe loss of corneal endothelial cells had higher levels of MDA and lower levels of SOD and GSH-px than patients with general loss.
In the corneal endothelium, oxidative stress may lead to corneal endothelial cell damage and apoptosis. Some investigators have used antioxidants for anterior chamber flushing during ultrasonic emulsification, which is effective in reducing endothelial cell loss.23,24 It suggests that oxidative stress has a close relationship with corneal endothelial cell loss. Spearman correlation analysis showed that in diabetic patients with cataract, MDA level was positively correlated with corneal endothelial cell loss, and SOD and GSH-px were negatively correlated with corneal endothelial cell loss. In addition, we also investigated the predictive value of MDA, SOD, and GSH-px in the degree of corneal endothelial cell loss by ROC, and all three showed some predictive value in this. Currently, there are no studies that have examined the predictive value of these three in the degree of corneal endothelial cell loss. Therefore, the conduct of this study provides a new direction for the prediction of the degree of postoperative corneal endothelial cell loss in diabetic patients with cataract and provides a basis for the treatment of corneal endothelial cell loss in postoperative patients.
In conclusion, there is a close relationship between the level of oxidative stress and corneal endothelial cell loss after phacoemulsification in diabetic patients with cataract. This study suggests to us that careful preoperative control of the duration of diabetes mellitus to minimize intraoperative oxidative stress and postoperative clearance time is of great importance to surgeons. By using a combination of antioxidant therapy and preoperative glycemic control, corneal endothelial cell loss can be effectively ameliorated and surgical outcomes improved. Nevertheless, the present study has some limitations. First, the levels of oxidative stress markers in cataract-free control patients were not included in this study, which limits our ability to investigate the pathogenesis of diabetic patient with cataract. Second, the sample size of this study was still small. Changes in MDA, SOD, and GSH-px levels were not dynamically examined in patients in the preoperative and postoperative periods. For a longer period of time postoperatively, hypoglycemic medications in diabetic patients may further affect the changes in these indices. Then, the anterior chamber depth (net ACD), the distance of the echo-emulsification probe from the cornea, as well as the power and duration of the echo-emulsification, all of which affect corneal endothelial cell loss and the duration of postoperative corneal edema. Finally, we were unable to analyze ultrasound energy which plays an important role in ECD loss.
Conclusion
Diabetic patients with cataract have a greater loss of corneal endothelial cells than non-diabetic patients with cataract after phacoemulsification operation. In oxidative stress analysis, diabetic patients with cataract have higher serum MDA levels and lower SOD and GSH-px. MDA levels are positively correlated with corneal endothelial cell loss after surgery in diabetic patients with cataract, while SOD and GSH-px are negatively correlated with the degree of loss. Serum MDA, SOD, and GSH-px levels also predict to some extent the degree of postoperative corneal endothelial cell loss in diabetic patients with cataract. This study may provide a means for surgeons to ameliorate corneal endothelial cell loss by adding antioxidants to aqueous humor.
Data Sharing Statement
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Ethics Approval
The present study was approved by the Ethics Committee of Hainan General Hospital and written informed consent was provided by all patients prior to the study start. All procedures were performed in accordance with the ethical standards of the Institutional Review Board and The Declaration of Helsinki, and its later amendments or comparable ethical standards.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Mohammadi SF, Hashemi H, Mazouri A, et al. Outcomes of cataract surgery at a referral center. J Ophthalmic Vis Res. 2015;10(3):250–256. doi:10.4103/2008-322X.170358
2. Memon AF, Mahar PS, Memon MS, Mumtaz SN, Shaikh SA, Fahim MF. Age-related cataract and its types in patients with and without type 2 diabetes mellitus: a Hospital-based comparative study. J Pak Med Assoc. 2016;66(10):1272–1276.
3. Mrugacz M, Pony-Uram M, Bryl A, Zorena K. Current approach to the pathogenesis of diabetic cataracts. Int J Mol Sci. 2023;24(7):6317. doi:10.3390/ijms24076317
4. Kaji Y, Usui T, Oshika T, et al. Advanced glycation end products in diabetic corneas. Invest Ophthalmol Vis Sci. 2000;41(2):362–368.
5. Kiziltoprak H, Tekin K, Inanc M, Goker YS. Cataract in diabetes mellitus. World J Diabetes. 2019;10(3):140–153. doi:10.4239/wjd.v10.i3.140
6. Chen YY, Wu TT, Ho CY, et al. Blocking of SGLT2 to eliminate NADPH-induced oxidative stress in lenses of animals with fructose-induced diabetes mellitus. Int J Mol Sci. 2022;23(13):7142.
7. Vaiciuliene R, Rylskyte N, Baguzyte G, Jasinskas V. Risk factors for fluctuations in corneal endothelial cell density (Review). Exp Ther Med. 2022;23(2):129. doi:10.3892/etm.2021.11052
8. Govindaswamy S, Prabhakar S, Prabhakar S. Evaluation of antioxidative enzymes levels and lipid peroxidation products levels in diabetic and non diabetic senile cataract patients. J Diabetes Metab Disord. 2022;21(1):697–705. doi:10.1007/s40200-022-01033-z
9. Manikandan R, Thiagarajan R, Beulaja S, Sudhandiran G, Arumugam M. Effect of curcumin on selenite-induced cataractogenesis in Wistar rat pups. Curr Eye Res. 2010;35(2):122–129. doi:10.3109/02713680903447884
10. Olofsson EM, Marklund SL, Behndig A. Enhanced diabetes-induced cataract in copper-zinc superoxide dismutase-null mice. Invest Ophthalmol Vis Sci. 2009;50(6):2913–2918. doi:10.1167/iovs.09-3510
11. Babizhayev MA. Mitochondria induce oxidative stress, generation of reactive oxygen species and redox state unbalance of the eye lens leading to human cataract formation: disruption of redox lens organization by phospholipid hydroperoxides as a common basis for cataract disease. Cell Biochem Funct. 2011;29(3):183–206. doi:10.1002/cbf.1737
12. Somaiya M, Burns JD, Mintz R, Warren RE, Uchida T, Godley BF. Factors affecting visual outcomes after small-incision phacoemulsification in diabetic patients. J Cataract Refract Surg. 2002;28(8):1364–1371. doi:10.1016/S0886-3350(02)01319-6
13. Saxena S, Mitchell P, Rochtchina E. Five-year incidence of cataract in older persons with diabetes and pre-diabetes. Ophthalmic Epidemiol. 2004;11(4):271–277. doi:10.1080/09286580490510733
14. Joo JH, Kim TG. Comparison of corneal endothelial cell changes after phacoemulsification between type 2 diabetic and nondiabetic patients. Medicine. 2021;100(35):e27141. doi:10.1097/MD.0000000000027141
15. Hugod M, Storr-Paulsen A, Norregaard JC, Nicolini J, Larsen AB, Thulesen J. Corneal endothelial cell changes associated with cataract surgery in patients with type 2 diabetes mellitus. Cornea. 2011;30(7):749–753. doi:10.1097/ICO.0b013e31820142d9
16. Galgauskas S, Laurinaviciute G, Norvydaite D, Stech S, Asoklis R. Changes in choroidal thickness and corneal parameters in diabetic eyes. Eur J Ophthalmol. 2016;26(2):163–167. doi:10.5301/ejo.5000677
17. El-Agamy A, Alsubaie S. Corneal endothelium and central corneal thickness changes in type 2 diabetes mellitus. Clin Ophthalmol. 2017;11:481–486. doi:10.2147/OPTH.S126217
18. Vinson JA. Oxidative stress in cataracts. Pathophysiology. 2006;13(3):151–162. doi:10.1016/j.pathophys.2006.05.006
19. Kowluru RA, Chan PS. Oxidative stress and diabetic retinopathy. Exp Diabetes Res. 2007;2007:43603. doi:10.1155/2007/43603
20. Ozmen B, Ozmen D, Erkin E, Guner I, Habif S, Bayindir O. Lens superoxide dismutase and catalase activities in diabetic cataract. Clin Biochem. 2002;35(1):69–72. doi:10.1016/S0009-9120(01)00284-3
21. Hashim Z, Zarina S. Antioxidant markers in human senile and diabetic cataractous lenses. J Coll Physicians Surg Pak. 2006;16(10):637–640. doi:10.2006/JCPSP.637640
22. Donma O, Yorulmaz E, Pekel H, Suyugul N. Blood and lens lipid peroxidation and antioxidant status in normal individuals, senile and diabetic cataractous patients. Curr Eye Res. 2002;25(1):9–16. doi:10.1076/ceyr.25.1.9.9960
23. IRM Padua, Valdetaro PG, Lima BT, et al. Effects of intracameral ascorbic acid on the corneal endothelium of dogs undergoing phacoemulsification. Vet Ophthalmol. 2018;21(2):151–159. doi:10.1111/vop.12490
24. Rubowitz A, Assia EI, Rosner M, Topaz M. Antioxidant protection against corneal damage by free radicals during phacoemulsification. Invest Ophthalmol Vis Sci. 2003;44(5):1866–1870. doi:10.1167/iovs.02-0892
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Refractive and Visual Outcomes of a Monofocal Non-Constant Aberration Aspheric Intraocular Lens
Hernández-Martínez A, Díaz-del-Rio MA, Ruiz-Santos M, Ruiz-Mesa R, Tañá-Rivero P
Clinical Ophthalmology 2022, 16:2521-2530
Published Date: 10 August 2022
Comparison of Phacoemulsification Grooving Efficiency in Longitudinal vs Transversal Handpieces
Wilkinson SW, Ungricht EL, West WB, Harris JT, Zaugg B, Olson RJ, Pettey JH
Clinical Ophthalmology 2023, 17:191-195
Published Date: 11 January 2023
Prospective Randomized Single-Masked Study of Bilateral Isofocal Optic-Design or Monofocal Intraocular Lenses
Ang RET, Stodulka P, Poyales F
Clinical Ophthalmology 2023, 17:2231-2242
Published Date: 4 August 2023
Clinical Outcomes of a Monofocal, Optimized, Aspheric, Hydrophobic Acrylic Intraocular Lens Implant
García-Tomás B, Marín-Sánchez JM, García-Elskamp C, Alcon-Ruiz E, Montesinos-López L, García Martínez-Lozano B
Clinical Ophthalmology 2023, 17:3215-3224
Published Date: 27 October 2023
Clinical Outcomes of a Bi-Aspheric Trifocal Diffractive Intraocular Lens
Tañá-Sanz S, Tañá-Sanz P, Rodríguez-Carrillo MD, Ruiz-Santos M, Álvarez de Toledo C, Tañá-Rivero P
Clinical Ophthalmology 2024, 18:27-40
Published Date: 4 January 2024