")
Back to Journals » Psychology Research and Behavior Management » Volume 18
Relationship Between Sleep Time and Depressive Symptoms in Middle-Aged and Elderly Chinese: Mediating Role of Body Pain
Authors Yang Z, Li B, Ma D, Lv Y, Qiu X, Zhang W, Wang J, Zhang Y, Xu C, Deng Y, Li J, Zhen X, Zhang J
Received 13 June 2024
Accepted for publication 20 December 2024
Published 14 January 2025 Volume 2025:18 Pages 67—79
DOI https://doi.org/10.2147/PRBM.S482589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Ziqing Yang,1,* Bingsong Li,2,3,* Dan Ma,1,4 Yitong Lv,1 Xinhui Qiu,5 Wenge Zhang,6 Jianye Wang,7 Yanlin Zhang,8 Chunming Xu,9 Yuxin Deng,9 Jinyang Li,10 Xuemei Zhen,2,3 Jun Zhang1
1Department of Orthodontics, School and Hospital of Stomatology, Cheeloo College of Medicine, Shandong University & Shandong Key Laboratory of Oral Tissue Regeneration & Shandong Engineering Research Center of Dental Materials and Oral Tissue Regeneration & Shandong Provincial Clinical Research Center for Oral Diseases, Jinan, Shandong, People’s Republic of China; 2Centre for Health Management and Policy Research, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, 250012, People’s Republic of China; 3NHC Key Laboratory of Health Economics and Policy Research (Shandong University), Jinan, Shandong, 250012, People’s Republic of China; 4Department of Orthodontics, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, 250021, People’s Republic of China; 5The second Hospital of Shandong University, Jinan, Shandong, 250033, People’s Republic of China; 6School of Management, Shandong University, Jinan, Shandong, 250100, People’s Republic of China; 7Department of Obstetrics and Gynecology, Qilu Hospital of Shandong University, Jinan, Shandong, 250012, People’s Republic of China; 8School of Basic Medical Sciences, Shandong University, Jinan, Shandong, 250012, People’s Republic of China; 9Department of Pediatrics, Xinjiang Medical University, Urumqi, People’s Republic of China; 10Faculty of Nursing, Shihezi University, Shihezi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuemei Zhen; Jun Zhang, Email [email protected]; [email protected]
Objective: Existing research has yet to adequately examine the correlation between sleep time, body pain, and depressive symptoms. This study seeks to elucidate the interconnections between these three elements.
Methods: The study used 2020 CHARLS data for analysis. To assess the intricate association among sleep time, body pain, and depressive symptoms, the study employed Spearman correlation analysis, multiple logistic regression, restricted cubic splines, and mediation effect analysis based on bootstrap testing.
Results: Risk factors for depressive symptoms in middle-aged and elderly Chinese include physical pain and reduced sleep duration. Results from the RCS suggest that the lowest risk of depressive symptoms occurs when the sleep time for the middle-aged and elderly population is approximately 7.5 hours. Body pain accounts for a 19.05% mediating effect between sleep time and depressive symptoms, and even after controlling confounding factors, there remains a 7.5% mediating effect.
Conclusion: The research findings indicate that there is a significant correlation among sleep time, body pain, and depressive symptoms. Insufficient sleep time and body pain can lead to depressive symptoms. Body pain plays a partial mediating role between sleep time and depressive symptoms.
Keywords: middle-aged and elderly people, sleep time, body pain, depressive symptoms
Introduction
The World Health Organization reports that depression is a major contributor to global disability and a significant part of the worldwide disease burden, affecting over 350 million people.1,2 In China, the prevalence of depression among the elderly surpasses 20%, with many exhibiting symptoms without meeting full clinical diagnostic criteria.3,4 As a psychological disorder, depression can precipitate a range of health complications; research indicates that those with depression are substantially more likely to develop heart disease and chronic conditions than those without.5 In extreme cases, it can lead to suicidal behavior, highlighting depression’s status as a critical public health concern globally and within China. Findings from the China Health and Retirement Longitudinal Study point to a rising prevalence of depressive symptoms nationwide.6 With advancing urbanization and an increasing aging population, the determinants of depression among middle-aged and elderly Chinese are becoming more complex and varied.7
Some studies have shown a correlation between sleep and depression, but the dose-response relationship has not been clearly explained.8 Previous research has established a correlation between the duration of sleep and the manifestation of depressive symptoms in middle-aged and elderly individuals.9 Sleep duration, as a significant factor influencing the risk of depression, has now garnered considerable attention. Studies have indicated that insomnia or short sleep duration can increase the risk of developing depression.10 Additionally, sleep disturbances serve as a factor in the recurrence of depression and as a predictor of its onset.11 However, there are also studies suggesting that restricting sleep can alleviate negative moods, thereby reducing the likelihood of developing depression.12 Current research has predominantly focused on the effects of short sleep duration on depression, with fewer studies examining the impact of prolonged sleep duration. Therefore, the relationship between sleep duration and depression warrants further investigation.
Globally, physical pain is a prevalent issue among older adults, resulting in substantial health consequences.13–15 Prior research has established a link between sleep duration and physical pain, revealing that poor sleep quality can worsen chronic pain symptoms.16 A review study found a two-way effect between sleep and pain, with poor sleep quality exacerbating pain and pain disrupting sleep.17 The study of American showed, sleep-active basal cortical pathways were critical for the production and maintenance of chronic pain. Studies in China have also found that poor sleep duration and quality at night can lead to lower back pain.18 Furthermore, evidence suggests that physical pain can increase the likelihood of depressive symptoms in this demographic. The review of studies found that both physical and psychological pain significantly increased the risk of depression symptoms.19 Studies in China have found that lower back pain can worsen depressive symptoms.20 Significantly, chronic pain has been found to triple the risk of developing depression symptoms in comparison to individuals without chronic pain.21 It is evident that both sleep time and body pain significantly influence the prevalence of depressive symptoms in middle-aged and older adults. Additionally, a correlation exists between sleep duration and physical pain. Current research indicates that as individuals age and experience a decline in bodily functions, middle-aged and older adults encounter an increasing number of health challenges, with sleep disturbances and physical pain being common issues.22,23 A recent review study found that sleep disorders play a partial mediating role between depressive symptoms and chronic pain. Therefore, it is crucial for research to investigate the connections between sleep duration, physical pain, and depression. While studies have examined these relationships among middle-aged and older Chinese populations, there is a scarcity of research using large, recent national samples.24 Furthermore, the causal pathways linking sleep duration and physical pain to depression have yet to be fully elucidated.
This study utilized data from the 2020 China Health and Retirement Longitudinal Study (CHARLS) to investigate the association between sleep time and depressive symptoms among middle-aged and elderly Chinese, and to examine the mediating role of body pain in this relationship. The following hypotheses are proposed and tested in this study. First, sleep duration is hypothesized to influence depressive symptoms. Second, physical pain is posited to have an impact on depressive symptoms. Third, it is suggested that sleep duration affects physical pain, which subsequently influences depressive symptoms. The findings offer valuable insights for the development and implementation of mental health policies aimed at improving the well-being of China’s middle-aged and elderly population, thereby holding significant social importance.
Methods
Data Resource
The dataset utilized in this study is derived from the 2020 China Health and Retirement Longitudinal Study (CHARLS), which is dedicated to amassing high-quality micro-data that accurately represents individuals and households aged 45 and older in China. This dataset encompasses five waves of data collection, starting with the baseline survey in 2011 and extending through to the latest survey conducted in 2020. It spans 30 provinces or municipalities, encompassing 150 counties (districts) and 450 communities (villages) across China. After eliminating individuals younger than 45 years of age, and cases with missing values for key variables (such as depressive symptoms, sleep time, and body pain) as well as other control variables, the final sample comprised 5724 participants. The methodology for selecting the sample is illustrated in Figure 1.
 |
Figure 1 Sample selection process. |
Measurement
Depressive Symptoms
Depressive symptoms were measured using the CES-D scale in the questionnaire. The scale consists of four levels, “rarely or not at all =0”, “not much =1”, “sometimes or half the time =2”, “most of the time =3”, with a total score of 0 to 30. When an individual’s total score is greater than or equal to 10 points, they are considered to have depressive symptoms and are classified as depressed. When an individual’s total score is less than 10 points, they are considered to have no depressive symptoms and are classified as non-depressed. The scale has been widely used to measure depression symptoms in Chinese middle-aged and elderly people and has a good measurement effect.25
Sleep Time
Sleep time was measured using the questionnaire question “About how many hours did you actually sleep each night during the past month?(Probably less than the time spent in bed)”.The time to fill this question is between 0 and 24 hours. The reliability of self-reported nighttime sleep duration has been validated within the field of sleep epidemiology.26 According to previous research, continuous variables are often used to evaluate sleep duration in CHARLS databases.27,28
Body Pain
Body pain was measured using the questionnaire question “Do you often suffer from pain?” Is it nothing, a little, some, quiet a lot, or a lot?”. Self-reported measures of body pain have been used in most epidemiological studies of pain.29 Based on previous research, we divided these responses into two categories, with and without body pain.30 This study classified “not at all” as having no body pain, and “a little”, “some”, “quite a lot”, and “a lot” as having body pain.31,32
Control Variable
We referred to several previous research, considering that it was critical to control potential covariates that may affect results when using CHARLS databases.33 The study incorporated covariates grouped into three categories: sociodemographic factors, lifestyle factors, and health status.34,35 Sociodemographic factors encompassed gender, age, place of residence, marital status, and educational level. Places of residence were classified into rural, township, and urban areas. Both age and gender significantly influenced sleep time and pain prevalence.31,36 Education and residence indicated socioeconomic status. Different Marital status affects depressive symptoms differently36 Marital status was divided into married and not in a marital relationship. Educational levels were divided into three groups: primary or below, secondary, and tertiary. Lifestyle factors assessed included alcohol consumption and smoking habits. Smoking and drinking were risk factors for many diseases.37,38 Health status variables consisted of self-rated health, which was further categorized into good, fair, and poor, as well as the presence of chronic diseases. Self-rated health reflected an individual’s overall health assessment and influenced depression, pain, and sleep duration.31,36 Chronic diseases were linked to depression, making them a significant confounding variable.36
Statistical methods
Frequency and percentage statistics were used for categorical data, and chi-square test was used for component comparison. Mean and standard deviation statistics were used for measurement data, and T-test was used for inter group comparison. Spearman correlation analysis and variance inflation factors were used to check the collinearity of explanatory variables, and all variables passed the collinearity test.39 (Table S1 and Table S2 in supplementary) Spearman correlation analysis was employed to examine the relationships among depressive symptoms, sleep time, and body pain. Multiple logistic regression model was used to explore the influencing factors of depressive symptoms. We build a crude model and a fully tuned model. Restricted cubic spline was used to explore the nonlinear relationship between sleep time and depressive symptoms. Mediation analysis was further used to explore the role of body pain between sleep time and depressive symptoms, and bootstrap method was used to test the mediation effect. Finally, we performed binary logistic regression to verify the robustness of the main results by excluding samples with chronic diseases. (Table S3 in supplementary) This study used stata 17.0 for data processing and analysis. The threshold for statistical significance in this study was established at P values less than 0.05.
Results
Sample Characteristics
The overall prevalence of depressive symptoms in the sample was 44.86%.Chi-square test and T test showed that the differences in gender, age, residence, education, marriage, drinking, smoking, self-rated health, chronic disease, body pain, and sleep time were statistically significant. (Table 1) In the depressive symptoms group, the prevalence of depressive symptoms in females was 87.58%, and that in males was 12.42%, with a significantly higher prevalence in females than in males. The average age of the non-depressive symptoms group was (58.87±9.08) years old, and that of the depressive symptoms group was (61.49±9.29) years old. There were 3476 individuals living in rural areas, 734 in towns and villages, and 1514 in cities. Most individuals had an education level of primary school or below and were married. Most individuals did not have smoking or drinking behaviors. In the depressive symptoms group, 86.57% of the individuals rated their self-rated health as general or poor. Most individuals had chronic diseases, especially in the depressive symptoms group, where 77.49% of the individuals had chronic diseases. The average sleep time of the non-depressive symptoms group was (6.40±1.63) hours, while the average sleep time of the depressive symptoms group was (5.50±2.03) hours. Most people had body pain, and 75.51% of the individuals in the depressive symptoms group had body pain.
 |
Table 1 Sample Characteristics Classified by Depressive Symptoms or Not |
Correlation Analysis
Spearman correlation analysis revealed significant associations among depressive symptoms, sleep duration, and body pain.(Table 2) Sleep duration exhibited a negative correlation with depressive symptoms (r=−0.25) and body pain (r=−0.21). Conversely, body pain showed a positive correlation with depressive symptoms (r=0.26). These results also satisfy the prerequisites for subsequent mediation analysis.
 |
Table 2 Correlation Analysis of Depressive Symptoms, Sleep Time and Body Pain |
Binary Logistic Regression Analysis
Table 3 presents the odds ratios (OR) and 95% confidence intervals (CI) for variables significantly associated with the onset of depressive symptoms in middle-aged and elderly individuals, as determined by univariate analysis. Model 1 and Model 2 show the binary logistic regression results of whether depressive symptoms occur in middle-aged and elderly people. Model 1 only includes two variables: sleep time and body pain. The results show that both sleep time and body pain are important influencing factors for the occurrence of depressive symptoms. Depression risk decreased with increasing sleep time. People with body pain were 2.67 times more likely to have depressive symptoms than people without body pain. Model 2 includes confounding variables for control, and the two variables of sleep time and body pain are still significant in the model. Specifically, the incidence of depressive symptoms in women is 1.52 times higher than that in men. Aging is a risk factor for developing depressive symptoms. Increasing sleep time may reduce the risk of depression symptoms. The incidence of depressive symptoms in people with body pain is 1.68 times higher than that in people without body pain. The incidence of depressive symptoms in people with chronic diseases is 1.24 times higher than that in people without chronic diseases. The incidence of depressive symptoms in people with general self-rated health and poor self-rated health is 1.87 times and 4.01 times higher than that in people with good self-rated health. The likelihood of exhibiting symptoms of depression among populations residing in towns and cities is 70.3% and 58.9% of that in rural populations, respectively. The risk of depressive symptoms was 64.6% for those with a secondary education and 47.8% for those with an associate’s degree or above, compared with those with a primary school education or less. The risk of depressive symptoms in married people was 0.78 times higher than People who are not in a marital relationship. Smoking and drinking did not have a significant effect on the occurrence of depressive symptoms in Model 2.
 |
Table 3 Multiple Model Binary Logistic Regression Analysis |
Nonlinear Analysis of Sleep Time and Depressive Symptoms
To further elucidate the association between sleep duration and depressive symptoms, the study employed the restricted cubic spline method to adjust for confounding factors and examine this relationship across three distinct groups: the entire middle-aged and elderly population, as well as the male and female cohorts within this demographic. For the general population, an optimal sleep time was identified at approximately 7.5 hours (OR=0.51, 95% CI: 0.44–0.59), beyond which the risk of depressive symptoms incrementally increased. (Figure 2) Subgroup analysis revealed that, for women, the risk of depressive symptoms significantly dropped at around 7.5 hours of sleep (OR=0.48, 95% CI: 0.41–0.57) and subsequently began a gradual ascent. (Figure 3) Conversely, for men, the trend between sleep time and depression risk paralleled the linear analytical results, indicating a higher risk of depressive symptoms with shorter sleep duration (Figure 4).
 |
Figure 2 Restriction cubic splines of sleep time and depression in the whole population. |
 |
Figure 3 Restriction cubic splines of sleep time and depression in the female. |
 |
Figure 4 Restriction cubic splines of sleep time and depression in the male. |
Mediating Effects of Body Pain on Sleep Time and Depressive Symptoms
Based on the aforementioned analysis, to further verify the relationship between physical pain, sleep duration, and the onset of depressive symptoms, the present study established Model 3 and Model 4, with the occurrence of depressive symptoms as the dependent variable, sleep duration as the independent variable, and physical pain as the mediating variable. Model 3 included only sleep duration and physical pain. (Table 4) The total effect of sleep duration on depressive symptoms was −0.063 (p<0.001), the direct effect was −0.051 (p<0.001), and the indirect effect was −0.012 (p<0.001), with the mediating effect accounting for 19.05%. Model 4, built upon Model 3, incorporated all control variables. At this point, the total effect of sleep duration on depressive symptoms was −0.040 (p<0.001), the direct effect was −0.038 (p<0.001), and the indirect effect was −0.003 (p<0.001), with the mediating effect accounting for 7.50%. Figure 5 presents a schematic diagram of the mediating effect without adjusting for all control variables. Path c in Figure 5 showed the total effect of sleep time on depressive symptoms as −0.063, path a showed the effect of sleep time on body pain as −0.052, path b showed the effect of body pain on depression symptoms as 0.225, and path C “showed the effect of sleep time on depressive symptoms as −0.051 when body pain acts as a mediator. With significant paths a and b, path C” remains significant, indicating that the mediation is partial.
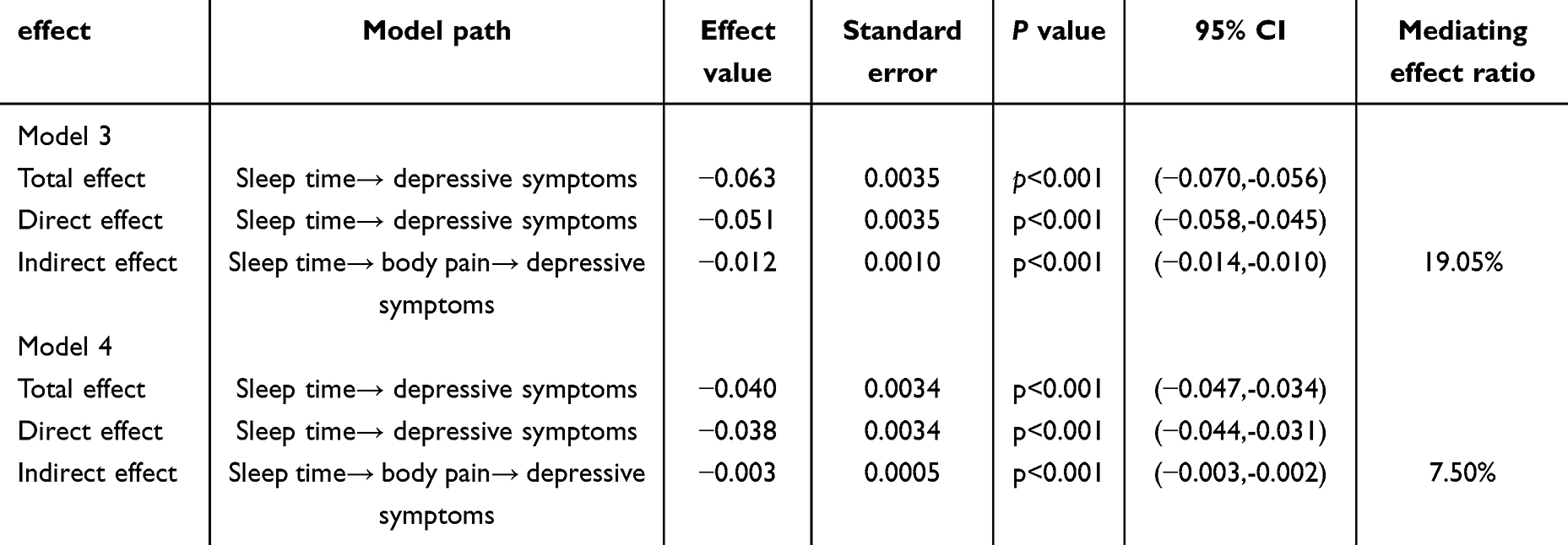 |
Table 4 Mediation Effect Model |
 |
Figure 5 Schematic diagram of the mediating effect. Note:** indicates P<0.001. |
Sensitivity Analysis
Finally, we performed a sensitivity check. We removed samples with chronic conditions, which can affect depression symptoms. Then, we built two models. Model 1 is the crude model, showing that both pain (OR=2.24, 95% CI: 1.83–2.75) and sleep duration (OR=0.82, 95% CI: 0.78–0.88) influence depressive symptoms. Model 2, a fully adjusted model, showed that sleep duration (OR=0.85, 95% CI: 0.80–0.91) had a protective effect on depressive symptoms, while pain (OR=1.84, 95% CI: 1.49–2.30) exacerbated depressive symptoms. Both models agree with the main results (Table S3 in supplementary).
Discussion
To our knowledge, this is the first study to explore the relationship between sleep duration, physical pain, and depressive symptoms in middle-aged and older adults using the 2020 CHARLS database. Our study found that Chinese middle-aged and elderly people are at greater risk of depressive symptoms, and 7.5 hours of sleep may help reduce the risk of depressive symptoms. At the same time, physical pain plays a partial mediating role between sleep duration and depressive symptoms.
The results of this study indicate that the relationship between sleep duration and depression symptoms is complex. Firstly, short sleep duration is associated with an increased risk of depression symptoms, consistent with previous research findings. This may be due to insufficient sleep leading to a decrease in the levels of neurotransmitters that regulate mood, disruption of the circadian rhythm, thereby impacting mental health and causing depression symptoms.40 Additionally, lack of sleep can increase the body’s stress response, leading to an overproduction of stress hormones, which in turn can lead to depression symptoms.41,42
Further analysis revealed a nonlinear relationship between sleep duration and the risk of depression symptoms among the general population of middle-aged and older adults, as well as among female middle-aged and older adults, exhibiting an “L” shape. Approximately 7.5 hours of sleep can significantly reduce the risk of depression symptoms, which aligns with the findings of previous studies.43 Moreover, some research has explored the relationship between long sleep duration and depression symptoms, suggesting that long sleep duration may also increase the risk of depression symptoms.44 However, in this study, the association between long sleep duration and depressive symptoms was not significant. This could be due to certain limitations of the study itself, such as potential bias in self-reported sleep duration.
The research also found that in the male middle-aged and older adult population, the results of the nonlinear analysis of sleep duration and depression symptoms were close to those of the linear analysis. The shorter the sleep duration, the greater the risk of depression symptoms. Studies have shown that there are indeed differences in the relationship between sleep duration and depression symptoms between male and female populations45 Men and women may exhibit different psychological reactions and coping strategies when faced with insufficient sleep. The research suggests that inadequate sleep may exacerbate stress responses in men, while women may demonstrate more difficulty with emotional regulation46. This may be one reason for their differing responses. Overall, the study concludes that interventions targeting sleep duration can reduce the risk of depression symptoms in middle-aged and older adults. We need to actively intervene using appropriate methods to help this population achieve approximately 7.5 hours of sleep.
Sleep duration can directly affect the risk of depressive symptoms and can also indirectly affect the risk of depressive symptoms through body pain. Sleep time can affect body pain. Studies have shown that insufficient sleep can lead to an increase in inflammatory responses in the body, which may lead to body pain.47 Sleep time also affects hormone levels, especially hormones that promote the feeling of pain.37 Therefore, insufficient sleep duration may increase body pain, which in turn affects the occurrence of depressive symptoms. Studies have shown that the greater the degree of body pain, the greater the risk of depression symptoms.48 This may be because body pain can cause a decline in quality of life, which may lead to depressive emotions.49,50 Previous studies have found that depressive symptoms can play an intermediary role between sleep duration and body pain.51 However, this study found that body pain also played a mediating role between sleep duration and depression symptoms. It can be seen that there may be a bidirectional effect between body pain and depression symptoms.
The study indicates that the prevalence of depressive symptoms among middle-aged and elderly individuals in China is 44.86%, corroborating prior research findings and underscoring the need to address depression symptoms in this demographic.52 Identified risk factors for depression symptoms in this group include gender, age, place of residence, education level, marital status, self-rated health, chronic disease, sleep time, and body pain. The data reveals that women have a 1.52-fold higher risk of developing depressive symptoms compared to men, a disparity that may be attributed to greater emotional sensitivity in women.53 Advancing age is associated with an increased risk of depression symptoms, as is a lower level of education, particularly in rural areas, likely due to reduced health literacy and poorer coping mechanisms for negative events.54,55 Married individuals have a lower risk (0.775 times) of depression than people who not in the marriage, possibly due to the greater social and emotional support marriage provides.56 Poor self-rated health significantly elevates the risk of depression symptoms, with individuals perceiving their health as poor being 4.009 times more likely to experience depressive symptoms. Therefore, self-rated health is an important factor in the occurrence of depression symptoms. Although self-rated health is a person’s subjective assessment of their own health status, it is based on objective physical and mental health status. In this study, the risk of developing depression symptoms was 1.237 times higher with chronic conditions than without chronic conditions, which is consistent with previous research suggesting that many chronic conditions, such as diabetes and high blood pressure, increase the risk of depression symptoms in middle-aged and older adults.57–59
Finally, although this study found a significant association between sleep time, body pain, and depressive symptoms, it is necessary to consider the potential impact of lifestyle factors on these relationships. Studies have shown that physical activity was linked to sleep quality and depression symptoms, with regular physical activity helping to relieve pain symptoms and reduced the risk of depression and sleep disorders.60,61 Dietary habits also played a crucial role in sleep and mood regulation, as a healthy diet could improve sleep quality and have a positive impact on mental health.62,63 Furthermore, the interplay between sleep and immune function significantly impacted the recovery process and overall mental health of individuals experiencing pain. Adequate sleep has been found to bolster immune function, which subsequently may expedite pain recovery and contribute to improved mental health outcomes.64 Therefore, while the analysis in this study was limited to survey data and did not include lifestyle and physiological factors such as diet, immune factors, etc, it is important to carefully consider these potential confounding variables when interpreting the results. Future studies are needed to further control for these factors to explore the interrelationship between sleep time, body pain, and depression symptoms.
The study utilized cross-sectional data obtained from the 2020 China Health and Retirement Longitudinal Study (CHARLS). Although it is the latest data, it is still limited in causal inference. Secondly, the sleep duration used in the study was self-reported, which may have certain memory biases, causing bias problems. Third, there may be a two-way relationship between sleep duration, body pain, and depression symptoms that needs further study. However, the study used data from the CHARLS database, and the sample has a certain degree of representativeness, and the results can be extrapolated to the middle-aged and elderly population in China. In the future, the study will consider using longitudinal data to further explore the relationship between sleep time, body pain, and depressive symptoms in the middle-aged and elderly population in China.
Conclusion
The study, based on a nationally representative survey, revealed a significant correlation between sleep duration, physical pain, and depression among middle-aged and elderly individuals in China. It established that shorter sleep time significantly increases the risk of depression symptoms, although the link between longer sleep time and increased depression symptoms risk was not statistically significant in this research. Optimal sleep, around 7.5 hours, appears to effectively mitigate depression symptoms risk in this demographic. Nonetheless, gender differences introduce additional layers to the sleep-depression dynamic, suggesting the need for further research into these nuances. The study also highlighted the considerable influence of physical pain on depression symptoms, noting its partial mediating effect on the relationship between sleep duration and depression symptoms. Consequently, strategies to prevent depression symptoms in middle-aged and elderly populations should prioritize ensuring adequate sleep and addressing physical pain.
Ethical
We conducted research using the CHARLS database. During the research process, our study did not cause harm to human subjects, did not involve sensitive personal information or commercial interests, and utilized publicly available and anonymized data. The CHARLS database has been approved by the Biomedical Ethics Committee of Peking University (IRB00001052-11015), and all participants provided written informed consent.According to Article 32, Items 1 and 2 of the “Ethical Review Measures for Life Science and Medical Research Involving Human Subjects” issued on February 18, 2023, in China:
1. Item 1: Research involving human subjects that only uses de-identified data from public databases and does not involve direct information related to individuals may generally be exempt from ethical review.
2. Item 2: If the research data comes from a project that has obtained informed consent and the use of the data conforms to the scope of the original informed consent, it may also be considered exempt from ethical review.
Therefore, our research meets the criteria outlined above and can be exempt from further ethical review.
Disclosure
We declare that we have no conflict of interest.
References
1. Global. regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Fortschritte Der Neurologie Psych. 2022;90(09):390–391.
2. Herrman H, Patel V, Kieling C, et al. Time for united action on depression: a Lancet-World Psychiatric Association Commission. Lancet. 2022;399(10328):957–1022. doi:10.1016/S0140-6736(21)02141-3
3. Tang T, Jiang JL, Tang XF. Prevalence of depressive symptoms among older adults in mainland China: a systematic review and meta-analysis. J Affective Disorders. 2021;293:379–390. doi:10.1016/j.jad.2021.06.050
4. Li D, Zhang DJ, Shao JJ, Qi XD, Tian L. A meta-analysis of the prevalence of depressive symptoms in Chinese older adults. Arch Gerontol Geriatrics. 2014;58(1):1–9. doi:10.1016/j.archger.2013.07.016
5. Shiga T. Depression and cardiovascular diseases. J Cardiol. 2023;81(5):485–490. doi:10.1016/j.jjcc.2022.11.010
6. Li XY. Stability and transitions of depressive symptoms among Chinese older adults over a 5-year follow up. Curr Psychol. 2023.
7. Fan XW, Guo X, Ren Z, et al. The prevalence of depressive symptoms and associated factors in middle-aged and elderly Chinese people. J Affective Disorders. 2021;293:222–228. doi:10.1016/j.jad.2021.06.044
8. Karimi R, Mallah N, Scherer R, Rodríguez-Cano R, Takkouche B. Sleep quality as a mediator of the relation between depression and chronic pain: a systematic review and meta-analysis. Br J Anaesth. 2023;130(6):747–762. PMID: 37059623. doi:10.1016/j.bja.2023.02.036
9. Chaput JP, Dutil C, Featherstone R, et al. Sleep timing, sleep consistency, and health in adults: a systematic review. Appl Physiol Nutr Metab. 2020;45(10):S232–S247. doi:10.1139/apnm-2020-0032
10. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affective Disorders. 2011;135(1–3):10–19. doi:10.1016/j.jad.2011.01.011
11. Mirchandaney R, Asarnow LD, Kaplan KA. Recent advances in sleep and depression. Curr Opin Psychiatry. 2023;36(1):34–40. doi:10.1097/YCO.0000000000000837
12. Lorenz N, Sander C, Ivanova G, Hegerl U. Temporal Associations of Daily Changes in Sleep and Depression Core Symptoms in Patients Suffering From Major Depressive Disorder: idiographic Time-Series Analysis. Jmir Mental Health. 2020;7(4):e17071. doi:10.2196/17071
13. Solovev A, Watanabe Y, Kitamura K, et al. Total physical activity and risk of chronic low back and knee pain in middle-aged and elderly Japanese people: the Murakami cohort study. Eur JPain. 2020;24(4):863–872. doi:10.1002/ejp.1535
14. Martins LB, Ribeiro JS, Rodrigues AMD, Dos Santos LC, Teixeira AL, Ferreira AVM. High resting energy expenditure in women with episodic migraine: exploring the use of predictive formulas. Front Nutri. 2023;10.
15. Derry-Vick HM, Johnston CD, Brennan-Ing M, et al. Pain Is Associated With Depressive Symptoms, Inflammation, and Poorer Physical Function in Older Adults With HIV. Psychosomatic Med. 2022;84(8):957–965. doi:10.1097/PSY.0000000000001119
16. Nordstoga AL, Adhikari S, Skarpsno ES. The joint association of insomnia disorder and lifestyle on the risk of activity-limiting spinal pain: the HUNT Study. Sleep Med. 2024;114:244–249. doi:10.1016/j.sleep.2024.01.016
17. Seiger AN, Penzel T, Fietze I. Chronic pain management and sleep disorders. Cell Rep Med. 2024;5(10):101761. PMID: 39413729. doi:10.1016/j.xcrm.2024.101761
18. Yang J, Liu C, Wu G, Zhao S. Association between nighttime sleep duration and quality with low back pain in middle-aged and older Chinese adults. Exp Gerontol. 2024;197:112602. PMID: 39357806. doi:10.1016/j.exger.2024.112602
19. Conejero I, Olié E, Calati R, Ducasse D, Psychological Pain CP. Depression, and Suicide: recent Evidences and Future Directions. Curr Psychiatry Rep. 2018;20(5):33. PMID: 29623441. doi:10.1007/s11920-018-0893-z
20. Huang J, Wang X. Association of depressive symptoms with risk of incidence low back pain in middle-aged and older Chinese adults. J Affect Disord. 2024;354:627–633. PMID: 38522815. doi:10.1016/j.jad.2024.03.081
21. Meda RT, Nuguru SP, Rachakonda S, Sripathi S, Khan MI, Patel N. Chronic Pain-Induced Depression: a Review of Prevalence and Management. Cureus J Med Sci. 2022;14(8).
22. Wang XR, Wang R, Zhang D. Bidirectional associations between sleep quality/duration and multimorbidity in middle-aged and older people Chinese adults: a longitudinal study. Bmc Public Health. 2024;24(1).
23. Qiu YD, Li H, Yang ZY, et al. The prevalence and economic burden of pain on middle-aged and elderly Chinese people: results from the China health and retirement longitudinal study. BMC Health Serv Res. 2020;20(1). doi:10.1186/s12913-020-05461-6
24. Ye X, Wang XF. Associations of multimorbidity with body pain, sleep duration, and depression among middle-aged and older adults in China. Health Qual Life Ou. 2024;22(1). doi:10.1186/s12955-024-02238-x
25. Chen HJ, Mui AC. Factorial validity of the Center for Epidemiologic Studies Depression Scale short form in older population in China. Intl Psych. 2014;26(1):49–57. doi:10.1017/S1041610213001701
26. Schokman A, Bin YS, Simonelli G, et al. Agreement between subjective and objective measures of sleep duration in a low-middle income country setting. Sleep Health. 2018;4(6):543–550. PMID: 30442323. doi:10.1016/j.sleh.2018.08.008
27. Pan L, Li L, Peng H, et al. Association of depressive symptoms with marital status among the middle-aged and elderly in Rural China-Serial mediating effects of sleep time, pain and life satisfaction. J Affect Disord. 2022;303:52–57. PMID: 35124113. doi:10.1016/j.jad.2022.01.111
28. Shang Q, Zhou J, Yao J, Feng C, Lou H, Cong D. Sleep duration and the risk of new-onset arthritis in middle-aged and older adult population: results from prospective cohort study in China. Front Public Health. 2024;12:1321860. PMID: 38873298; PMCID: PMC11169742. doi:10.3389/fpubh.2024.1321860
29. Qiu Y, Li H, Yang Z, et al. The prevalence and economic burden of pain on middle-aged and elderly Chinese people: results from the China health and retirement longitudinal study. BMC Health Serv Res. 2020;20(1):600. doi:10.1186/s12913-020-05461-6
30. Zhang N, Wang C, Li Y, Chen F, Yan P. Hypothetical interventions on risk factors for depression among middle-aged and older community-dwellers in China: an application of the parametric g-formula in a longitudinal study. J Affect Disord. 2023;327:355–361. doi:10.1016/j.jad.2023.01.113
31. Ai Z, Tang C, Peng P, Wen X, Tang S. Prevalence and influencing factors of chronic pain in middle-aged and older adults in China: results of a nationally representative survey. Front Public Health. 2023;11:1110216. PMID: 37139366. doi:10.3389/fpubh.2023.1110216
32. Jia Z, Gao Y, Zhao L, Han S. Effects of pain and depression on the relationship between household solid fuel use and disability among middle-aged and older adults. Sci Rep. 2022;12(1):21270. PMID: 36481918. doi:10.1038/s41598-022-25825-8
33. You Y, Mo L, Tong J, Chen X, You Y. The role of education attainment on 24-hour movement behavior in emerging adults: evidence from a population-based study. Front Public Health. 2024;12:1197150. PMID: 38292911. doi:10.3389/fpubh.2024.1197150
34. Furihata R, Uchiyama M, Suzuki M, et al. Association of short sleep duration and short time in bed with depression: a Japanese general population survey. Sleep Biol Rhythms. 2015;13(2):136–145. doi:10.1111/sbr.12096
35. Yu WJ, Gong YJ, Lai XZ, Liu JP, Rong HG. Sleep Duration and Risk of Depression: empirical Evidence from Chinese Middle-Aged and Older Adults. Sustainability. 2023;15(7).
36. Ye X, Wang X. Associations of multimorbidity with body pain, sleep duration, and depression among middle-aged and older adults in China. Health Qual Life Outcomes. 2024;22(1):23. PMID: 38413940. doi:10.1186/s12955-024-02238-x
37. You Y, Liu J, Li X, Wang P, Liu R, Ma X. Relationship between accelerometer-measured sleep duration and Stroop performance: a functional near-infrared spectroscopy study among young adults. PeerJ. 2024;12:e17057. PMID: 38436025. doi:10.7717/peerj.17057
38. You Y, Li J, Zhang Y, Li X, Li X, Ma X. Exploring the potential relationship between short sleep risks and cognitive function from the perspective of inflammatory biomarkers and cellular pathways: insights from population-based and mice studies. CNS Neurosci Ther. 2024;30(5):e14783. PMID: 38797980. doi:10.1111/cns.14783
39. Bayman EO, Dexter F. Multicollinearity in Logistic Regression Models. Anesth Analg. 2021;133(2):362–365. PMID: 34257197. doi:10.1213/ANE.0000000000005593
40. Feng ZQ, Chen Q, Li YJ, Xue Z, Hao XN. The association between falls and depressive symptoms among older adults: evidence from the China Health and Retirement Longitudinal Study. Front Public Health. 2023;11.
41. Silverstein B, Ajdacic-Gross V, Rossler W, Angst J. The gender difference in depressive prevalence is due to high prevalence of somatic depression among women who do not have depressed relatives. J Affect Disord. 2017;210:269–272. doi:10.1016/j.jad.2017.01.006
42. Zhong WJ, Wang F, Chi LL, Yang XY, Yang YX, Wang ZH. Association between Sleep Duration and Depression among the Elderly Population in China. Experimental Aging Research. 2022;48(4):387–399. doi:10.1080/0361073X.2021.2008755
43. Pengpid S, Peltzer K. Mental morbidity and its associations with socio-behavioural factors and chronic conditions in rural middle- and older-aged adults in South Africa. J Psychol Afr. 2020;30(3):257–263. doi:10.1080/14330237.2020.1767956
44. Li J, Wang Q, Zhou XC. Spousal religious difference, marital satisfaction, and psychological well-being of Chinese older adults. Family Relat. 2023.
45. Lin WJ, Zhang DL, Wang YM, Zhang L, Yang JC. Analysis of depression status and influencing factors in middle-aged and elderly patients with chronic diseases. Frontiers in Psychology. 2024;15.
46. Cho YJ, Kim B, Kwon HS, Han K, Kim MK. Diabetes severity and the risk of depression: a nationwide population-based study. J Affective Disorders. 2024;351:694–700. doi:10.1016/j.jad.2024.01.181
47. Qiu WD, Cai AP, Li LW, Feng YQ. Association of depression trajectories and subsequent hypertension and cardiovascular disease: findings from the CHARLS cohort. Journal of Hypertension. 2024;42(3):432–440. doi:10.1097/HJH.0000000000003609
48. Pandi-Perumal SR, Monti JM, Burman D, et al. Clarifying the role of sleep in depression: a narrative review. Psychiatry Res. 2020;291.
49. Zuloaga DG, Lafrican JJ, Zuloaga KL. Androgen regulation of behavioral stress responses and the hypothalamic-pituitary-adrenal axis. Horm Behav. 2024;162:105528. doi:10.1016/j.yhbeh.2024.105528
50. Lis M, Miluch T, Majdowski M, Zawodny T. A link between ghrelin and major depressive disorder: a mini review. Front Psych. 2024;15.
51. You YW, Chen YQ, Liu RD, et al. Inverted U-shaped relationship between sleep duration and phenotypic age in US adults: a population-based study. Sci Rep. 2024;14(1). doi:10.1038/s41598-024-56316-7
52. Short MA, Booth SA, Omar O, Ostlundh L, Arora T. The relationship between sleep duration and mood in adolescents: a systematic review and meta-analysis. Sleep Med Rev. 2020;52.
53. Alcalde E, Rouquette A, Wiernik E, Rigal L. How do men and women differ in their depressive symptomatology? A gendered network analysis of depressive symptoms in a French population-based cohort. J Affect Disord. 2024;353:1–10. doi:10.1016/j.jad.2024.02.064
54. Sen B, Kurtaran NE, Öztürk L. The effect of 24-hour sleep deprivation on subjective time perception. Int J Psychophysiol. 2023;192:91–97. doi:10.1016/j.ijpsycho.2023.08.011
55. Costa AN, Coman A, Musich M, et al. Sleep characteristics and pain in middle-aged and older adults: sex-specific impact of physical and sitting activity. Sleep Med. 2023;111:180–190. doi:10.1016/j.sleep.2023.09.030
56. Khalil NFW, Hassan MM, Elshatby NM. The interplay of body composition, pain intensity, and psychological status in Egyptian patients with knee osteoarthritis. Egyptian Rheum Rehabil. 2024;51(1). doi:10.1186/s43166-024-00248-7
57. Petrelis M, Soultanis K, Michopoulos I, Nikolaou V. Efficacy of a conservative physical treatment regimen on psychological status and quality of life in Greek patients with chronic low back pain. Psychiatrike. 2024;35(1):54–65. doi:10.22365/jpsych.2023.027
58. Zhou H, Han D, Zhou HS, Ke XF, Jiang DD. Influencing factors of psychological pain among older people in China: a cross-sectional study. Heliyon. 2023;9(10).
59. Naughton F, Ashworth P, Skevington SM. Does sleep quality predict pain-related disability in chronic pain patients? The mediating roles of depression and pain severity. Pain. 2007;127(3):243–252. doi:10.1016/j.pain.2006.08.019
60. You Y, Chen Y, Zhang Q, Yan N, Ning Y, Cao Q. Muscle quality index is associated with trouble sleeping: a cross-sectional population based study. BMC Public Health. 2023;23(1):489. PMCID: PMC10012435. doi:10.1186/s12889-023-15411-6
61. You Y, Chen Y, Zhang Y, Zhang Q, Yu Y, Cao Q. Mitigation role of physical exercise participation in the relationship between blood cadmium and sleep disturbance: a cross-sectional study. BMC Public Health. 2023;23(1):1465. PMCID: PMC10391747. doi:10.1186/s12889-023-16358-4
62. You Y, Chen Y, Wei M, et al. Mediation Role of Recreational Physical Activity in the Relationship between the Dietary Intake of Live Microbes and the Systemic Immune-Inflammation Index: a Real-World Cross-Sectional Study. Nutrients. 2024;16(6):777. PMCID: PMC10974920. doi:10.3390/nu16060777
63. You Y, Wang R, Li J, Cao F, Zhang Y, Ma X. The role of dietary intake of live microbes in the association between leisure-time physical activity and depressive symptoms: a population-based study. Appl Physiol Nutr Metab. 2024;49(8):1014–1024. PMID: 38569203. doi:10.1139/apnm-2023-0550
64. You Y. Accelerometer-measured physical activity and sedentary behaviour are associated with C-reactive protein in US adults who get insufficient sleep: a threshold and isotemporal substitution effect analysis. J Sports Sci. 2024;42(6):527–536. doi:10.1080/02640414.2024.2348906
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.