")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Relationship of Hypothyroidism with Alopecia Areata and Androgenetic Alopecia: Insights from a Two-Sample Mendelian Randomization Study
Authors Zhang G, Huang X, Li H, Gong H, Zhou Y , Liu F
Received 17 June 2024
Accepted for publication 19 August 2024
Published 22 August 2024 Volume 2024:17 Pages 1865—1874
DOI https://doi.org/10.2147/CCID.S474168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Gongjie Zhang,1 Xinlyu Huang,1 Hanlin Li,1 Huizi Gong,1 Yabin Zhou,2 Fang Liu1
1Department of Dermatology, Venereology and Cosmetology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China; 2Department of Dermatology, Beijing Children’s Hospital, Capital Medical University, National Centre for Children’s Health, Beijing, 100045, People’s Republic of China
Correspondence: Yabin Zhou, Department of Dermatology, Beijing Children’s Hospital, Capital Medical University, National Centre for Children’s Health, No. 56 Nan Lishi Road, Xicheng District, Beijing, 100045, People’s Republic of China, Tel +86 10 59616884, Email [email protected] Fang Liu, Department of Dermatology, Venereology and Cosmetology, Beijing Chaoyang Hospital, Capital Medical University, No. 8 Gongti Nan Road, Chaoyang District, Beijing, 100020, People’s Republic of China, Tel +86 18611369216, Email [email protected]
Background: Hair loss is common in hypothyroidism patients. However, the link with alopecia areata (AA) and androgenetic alopecia (AGA) is unclear. Previous observational studies have presented completely opposite results. This study aims to causally link hypothyroidism with AA and AGA.
Methods: A two-sample Mendelian Randomization (MR) study, utilizing data from FinnGen Consortium, investigated the causal link between hypothyroidism and AA and AGA. We employed Inverse Variance Weighted (IVW), MR-Egger, Weighted Median, Simple Mode, and Weighted Mode to assess the risk association.
Results: The discovery samples included 13,429 hypothyroidism cases (94,436 controls), 767 alopecia areata cases (394,105 controls), and 220 androgenetic alopecia cases (219,249 controls). MR analysis showed a causal link between hypothyroidism and AA, with significant results from IVW (OR, 1.34; CI, 1.16– 1.56; P = 0.0001), MR-Egger (OR, 1.56; CI, 1.09– 2.23; P = 0.0240), and weighted median (OR, 1.34; CI, 1.06– 1.69; P = 0.0140). However, no clear causal relationship was found between genetically predicted hypothyroidism and AGA risk (p > 0.05).
Conclusion: The results show hypothyroidism causally associated with AA onset, but not AGA. These findings address contentious issues in observational studies. Comprehensive thyroid function assessments are crucial for AA patients, emphasizing thorough clinical examinations’ importance.
Keywords: hypothyroidism, alopecia areata, androgenetic alopecia, Mendelian randomization study, causality
Introduction
Alopecia areata (AA) manifests globally, with an estimated incidence of 1 in 1000 individuals, entailing a lifelong susceptibility of approximately 2%.1,2 It may occur in both children and adults, with no gender disparity in its incidence.1 The mechanism of AA remains unclear, with key events possibly involving the loss of immune privilege in hair follicles, leading to T-cell-mediated immune attacks on follicular cells.3 Genetic susceptibility also plays a role, as confirmed by GWAS establishing a link between AA and human leukocyte antigen (HLA) genes. Notably, the HLA-DQB1*03 allele may serve as a significant marker for the susceptibility to AA.4,5 AA predominantly presents on the scalp but can also occur in any area with hair growth, such as eyelashes, eyebrows, beard, limbs, or other regions. The most common clinical manifestation is patchy hair loss, characterized by scattered, smooth, and circular areas where hair is completely lost, evolving over several weeks. Less common patterns of hair loss include creeping alopecia, rare horseshoe-shaped baldness, and diffuse AA. The horseshoe-shaped alopecia may resemble male-pattern androgenetic alopecia (AGA), making differentiation challenging at times. The characteristic features of AGA in males include the distinctive phenomenon of hair follicle miniaturization to varying degrees in specific locations on the scalp, accompanied by a reduction in the density of terminal hair. The extent of scalp involvement may gradually evolve with the progression of the condition. Currently, it is acknowledged that AGA is a hereditary trait dependent on androgens. Dihydrotestosterone (DHT) stands as the pivotal androgen that induces and accelerates AGA in males.6 Several susceptibility loci associated with AGA have been identified,7,8 including AR/EDAR2 on the X chromosome,9 PAX1/FOXA2 on chromosome 20p11,10,11 and the HDAC9 gene on chromosome 7p21.1.12,13 Chromosome 3q26 may also play a certain role.14 Female pattern hair loss (FPHL) is a prevalent, non-scarring alopecia primarily occurring in adult women. Its hallmark is the progressive loss of terminal hairs in the frontal and vertex regions of the scalp, resulting in a noticeable reduction in hair density. In contrast to many cases of AGA in men (male pattern hair loss), the shedding of terminal hairs in affected areas of female pattern hair loss is typically incomplete and often does not involve the frontal hairline. The majority of women with FPHL exhibit normal levels of androgens, indicating that the understanding of the pathogenic mechanisms is still not comprehensive enough.15,16 The genetic basis and inheritance patterns of FPHL remain relatively less understood.17 The aromatase gene (CYP19A1) may be involved in the development of female pattern hair loss.18 Several diseases have been found to be associated with AA, including vitiligo, lupus erythematosus, psoriasis, atopic dermatitis, thyroid disease, and allergic rhinitis.19 Similarly, some diseases have been found to be associated with AGA, including psychosocial effects,20 cardiovascular disease and metabolic syndrome,21–26 prostate cancer.27
Hypothyroidism, characterized by an underactive thyroid gland, is a common endocrine disorder affecting various physiological processes. Hair loss frequently accompanies hypothyroidism.28 However, the relationship between hypothyroidism and specific types of hair loss, such as AA and AGA, remains unclear. Despite its common occurrence, only a limited number of studies have been published to evaluate the association of hypothyroidism with AA or AGA. While most studies suggest a correlation between hypothyroidism and AA, there are still some observational studies indicating the absence of a connection. This discrepancy could be influenced by factors like sample size, ethnic diversity, and other methodological considerations. Hence, the association between hypothyroidism and AA, as well as the nature of any potential relationship, remains uncertain. Observational studies exploring the relationship between hypothyroidism and AGA are currently scarce.
The Mendelian randomization (MR) research method is recognized as a robust tool in epidemiological studies, focusing on utilizing genetic variations to evaluate the causal link between risk factors and specific diseases. Confounding factors pose a significant challenge in causal inference within epidemiological studies. In the Mendelian randomization method, genetic variations adhere to the principle of random distribution of alleles to offspring, resembling the design of a randomized controlled trial. The strengths of the MR method lie in effectively addressing common issues in observational studies, including confounding factors, reverse causation, and issues related to representativeness and feasibility in randomized controlled trials.29 However, it is noteworthy that there is currently no research applying the MR method to evaluate the relationship of hypothyroidism with AA or AGA. Hence, this study utilizes a two-sample MR research approach to explore the potential causal connection of hypothyroidism with AA and AGA. The objective is to establish a theoretical foundation for understanding the interplay between the development of hypothyroidism and the onset of AA and AGA.
Methods
Study Design
We conducted two-sample MR analysis based on summary statistics from GWAS to investigate the association of hypothyroidism with AA and AGA. Valid instrumental variables (IVs) need to meet specific criteria: 1. The variant should be linked to the risk factor being studied; 2. The variant must be independent of any confounding factors that might influence the relationship between the risk factor and the outcome; 3. The variant should only influence the outcome through its impact on the risk factor.30 The comprehensive flowchart illustrating the methodology of this MR study is presented in Figure 1A, with the MR assumptions delineated in Figure 1B.
 |
Figure 1 (A) Detailed flowchart depicting the methodology employed in the current two-sample Mendelian randomization study. (B) Mendelian randomization assumptions. |
Study Samples and Measures
The summary statistics were obtained from the FinnGen Consortium.31 The FinnGen study is a large-scale genomics initiative that has analyzed over 500,000 Finnish biobank samples and correlated genetic variation with health data to understand disease mechanisms and predispositions. The project is a collaboration between research organizations and biobanks within Finland and international industry partners. The discovery sample for hypothyroidism included 13429 clinically diagnosed cases (94436 controls). Similarly, the discovery sample for AA included 767 clinically diagnosed cases (394105 controls). Additionally, the discovery sample for AGA included 220 clinically diagnosed cases (219249 controls). However, all single nucleotide polymorphisms (SNPs) were all derived from GWAS on European ancestry to minimize potential bias caused by population heterogeneity.
Instruments Selection
We selected SNPs with genome-wide significance (p < 5 × 10−8) as IVs for hypothyroidism in our study. Linkage disequilibrium (LD) was assessed to determine genetic linkage among SNPs, with a threshold set at r2 < 0.001 and a window size of 10,000 kb. SNPs associated with potential confounding factors of AA and AGA were excluded from the final MR analyses using data from the PhenoScanner V2 database (http://www.phenoscanner.medschl. cam.ac.uk/). Additionally, palindromic variants were excluded, and the effects of SNPs on hypothyroidism, AA, and AGA were harmonized. Ultimately, 25 eligible SNPs were included in the final MR analyses, with detailed information provided in Supplementary Table 1.
Statistical Analyses of the MR Study
We employed the inverse variance weighted (IVW), Mendelian randomization-Egger (MR-Egger), weighted median, simple mode, and weighted mode approaches to assess the risk association of hypothyroidism with AA and AGA. Among these methods, IVW emerged as the most commonly utilized variant-specific causal estimation method in two-sample MR analyses, particularly when all enrolled IVs exhibited robust validity. Consequently, IVW was chosen as the primary and most efficient analytical method for this study.32 If statistical significance was observed for heterogeneity in the research studies, a random effects IVW model was utilized; otherwise, a fixed effects IVW model was employed.
To further validate the consistency and effectiveness of the MR findings, additional supplementary methods were utilized. The MR-Egger regression estimates the causal effect by regressing the instrument-exposure association on the instrument-outcome association, allowing for an intercept term that represents potential pleiotropy. A significant intercept suggests the presence of horizontal pleiotropy, indicating that the instrument may not satisfy the exclusion restriction assumption.33 The weighted median estimation calculates a median estimate of the causal effect by giving more weight to IVs with smaller standard errors or larger statistical precision. Simple mode is a basic analytical approach where a straightforward statistical method is used to estimate causal effects without complex adjustments or weighting of genetic variants and it may overlook certain complexities inherent in causal inference, such as confounding or unmeasured variables. Weighted mode is an analysis approach where weights are assigned to each genetic variant based on their variance. Scatter, forest, and funnel plots were drawn to visualize the results and demonstrate the efficiency and stability of the MR study.
Sensitivity Analyses
We conducted sensitivity analyses to assess various aspects of our MR study, including heterogeneity, pleiotropy, and the influence of outliers. Heterogeneity among the IVs utilized in the IVW method was evaluated using Cochran’s Q test, with a significance level set at p < 0.05 indicating substantial heterogeneity. Interpretation of the MR results should be cautious in the presence of significant heterogeneity. Pleiotropy, the phenomenon where a single genetic locus affects multiple phenotypes, was assessed using the MR-Egger intercept analysis. A p-value greater than 0.05 suggests negligible directional pleiotropy.34 Furthermore, we conducted the MR-PRESSO analysis to identify and address the influence of outliers in our data. To assess the robustness of our results, we performed leave-one-out tests, systematically removing one SNP at a time and evaluating the impact on the overall results. Consistency in the direction and magnitude of the remaining results after SNP removal indicates stability and reliability of the causal relationship.
All statistical analyses were conducted using the “Two-Sample MR” and “MRPRESSO” packages within the R software environment (version 4.2.3).
Results
Hypothyroidism is Associated with Increased Risk of AA
Twenty five hypothyroidism-related SNPs meeting the three main assumptions of the study were retained after excluding SNPs associated with confounding factors and outcomes. SNPs with incompatible alleles or palindromic characteristics and intermediate allele frequencies were also removed. Scatter plots visually represented the effects of the selected 25 SNPs on both hypothyroidism and AA, while funnel plots illustrated the distribution of individual SNP effects (Figures 2A, B and 3A, B). Forest plots were employed to visualize the impact of each SNP on outcome estimations (Supplementary Figure 1). Heterogeneity analysis using the MR-Egger test indicated no clear evidence of heterogeneity among the hypothyroidism-related SNPs. The MR-Egger method reported a Cochran’s Q statistic of 23.45, with a p-value greater than 0.05 (p = 0.377) for AA (Table 1). Consequently, the IVW method with a fixed effects model was predominantly used for causal estimation.
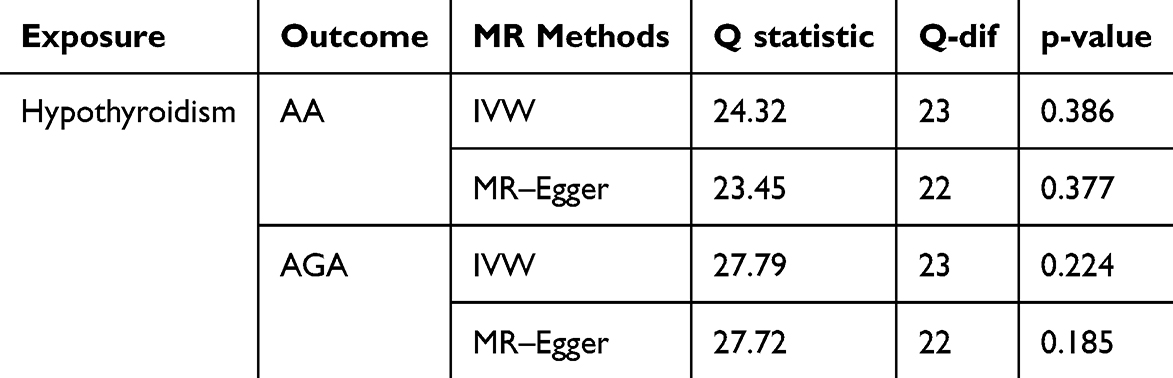 |
Table 1 Heterogeneity analysis of the hypothyroidism-related genetic variants in the AA and AGA GWAS datasets |
 |
Figure 2 Scatter plots illustrating the effects of SNPs on hypothyroidism, AA and AGA. The x-axis represents the impact of each SNP on hypothyroidism, while the y-axis represents the impact of each SNP on AA (A) and AGA (B). |
 |
Figure 3 Funnel plots of hypothyroidism SNPs for AA (A) and AGA (B). |
MR analysis indicates a causal relationship between hypothyroidism and AA. The main results are derived from the IVW method (OR, 1.34; CI, 1.16–1.56; P = 0.0001), MR-Egger (OR, 1.56; CI, 1.09–2.23; P = 0.0240), and the weighted median (OR, 1.34; CI, 1.06–1.69; P = 0.0140). Additionally, the results from the simple mode (OR, 1.23; CI, 0.80–1.89; P = 0.3600) and weighted mode (OR, 1.26; CI, 0.93–1.71; P = 0.1480) (Figure 4A) estimations show a similar trend in the impact of hypothyroidism on AA, although not reaching statistical significance. As mentioned earlier, the IVW method was adopted as the primary and most effective analytical approach in this study, leading to the conclusion that genetically predicted hypothyroidism is associated with an increased risk of AA.
 |
Figure 4 Forest plot of the association between hypothyroidism and AA (A) and AGA (B). |
However, the MR analysis did not reveal any association between hypothyroidism and AGA. No significant heterogeneity was observed, with a Q statistic of 27.72 (p = 0.185) obtained from the MR-Egger method (Table 1). The results of the fixed effects IVW, MR-Egger, weighted median, simple mode, and weighted mode analyses collectively reveal that there was no clear causal relationship between genetically predicted hypothyroidism and the risk of AGA, with all p-values greater than 0.05 (Figure 4B).
Sensitivity Analyses
No conclusive evidence of substantial statistical heterogeneity was observed among the hypothyroidism-related SNPs concerning their impact on AA, as mentioned previously. Additionally, the MR-Egger intercept analysis showed no signs of directional pleiotropy (intercept = −0.027, SE = 0.030, p = 0.38), suggesting that potential confounding factors through alternate pathways were unlikely to affect the relationship between exposure and outcome. MR-PRESSO analysis indicated the absence of directional pleiotropy and outliers for the IVs (p-global test = 0.371). The leave-one-out analysis yielded results consistent with the primary MR studies, suggesting that no individual SNP significantly influenced the outcomes and emphasizing the robustness and reliability of the MR studies (Supplementary Figure 2).
Discussion
Based on the findings of this study, there is evidence supporting a causal association between hypothyroidism and AA. These results are substantiated by a series of sensitivity analyses. However, no causal relationship was identified between hypothyroidism and AGA. This reaffirms the notion that the connection between AA and the immune system is more closely linked compared to AGA. Unfortunately, employing the most stringent Bonferroni correction with a “gold standard” threshold of 5e-8, no effective SNPs were identified in the genomic databases for AA and AGA. Hence, reverse MR tests could not be completed.
Some previous epidemiological cohort studies have proposed a potential association between hypothyroidism and AA. In one of the largest disease association studies, a nationwide investigation in Taiwan involving 4334 patients with AA revealed associations with thyroid disease (OR 1.89, 95% CI 1.68–2.13) among all patients compared to control subjects.19 According to Bakry et al’s study, 16% of patients with AA were diagnosed with subclinical hypothyroidism.35 Marahatta et al’s study revealed a statistically significant prevalence of subclinical hypothyroidism, specifically 16%, in the AA group. They strongly recommend considering thyroid function evaluation in patients with AA.36 Lyakhovitsky et al’s study revealed a significant association between AA and thyroid abnormalities (16% hypothyroidism).37 Park et al’s study also observed an increased incidence of thyroid dysfunction and thyroid autoimmunity in AA patients, particularly those with severe AA.38 However, possibly influenced by factors such as sample size and ethnicity, some studies present contrasting results. For instance, in Saylam Kurtipek et al’s study, they identified elevated anti-thyroglobulin (anti-TG) levels in 2.2% of AA patients, elevated anti-thyroid peroxidase antibodies (anti-TPO) in 14.1%, elevated thyroid-stimulating hormone (TSH) in 7.6%, elevated free thyroxine (fT4) in 1.1%, and elevated free triiodothyronine (fT3) levels in 5.4%. Unlike previous research, these findings indicate a lower incidence of impaired thyroid functions and thyroid autoantibodies in patients with AA. As a result, the researchers suggested that a detailed examination might not be necessary for patients with AA who lack a clinical history.39 Shrestha et al’s study suggested that there was no significant association between AA and thyroid function tests.40
In investigating the association between exposure factors and outcomes, limitations in experimental conditions or ethical considerations may preclude the possibility of conducting randomized controlled trials. Currently, no randomized controlled trials have been conducted regarding the association between hypothyroidism and AA. The use of genetic variations as IVs in MR can provide conclusions that are not only more reliable but also comparable to the results of randomized controlled trials, surpassing the outcomes of observational or retrospective studies. Our study proposes that hypothyroidism may play a causal role in the development of AA, but not in AGA. These results offer new perspectives on the mechanisms underlying AA and contribute to resolving contentious issues in observational studies. However, it remains crucial to conduct future high-quality randomized controlled studies with substantial sample sizes to further validate this association.
This study’s notable strength lies in being the first, to our knowledge, to employ a two-sample MR analysis to explore the causal association between hypothyroidism and both AA and AGA. Simultaneously, we utilized the latest data from the FinnGen database for analysis.31 In comparison to observational studies, this analytical method is less susceptible to confounding, reverse causation, and measurement exposure errors. By adopting a more conservative and iterative approach, we minimized heterogeneity, confirmed the consistency of point estimates pre- and post-removal of outliers, thereby reinforcing the evidence. A series of sensitivity analyses further validated the robustness of the results. The findings appear unaffected by pleiotropy, as consistent results were obtained in sensitivity analyses, and no outliers were detected using both the IVW and MR-PRESSO methods. However, it is essential to note that the study results are based on data from patients of European descent, potentially limiting generalizability to other ethnicities.
Conclusions
In this MR study, the results indicate a causal association between hypothyroidism and the onset of AA, but no association with AGA. The findings are of utmost importance as they address contentious issues observed in observational studies. They contribute to an enhanced understanding of the pathogenic mechanisms underlying AA and raise awareness among clinicians about the potential risk of AA in individuals with hypothyroidism, thereby improving patient prognostic outcomes. This study suggests that comprehensive thyroid function assessments are necessary for patients with AA, emphasizing the importance of thorough clinical examinations. Future research at the basic level is warranted to elucidate the pathophysiological mechanisms of AA in patients with hypothyroidism.
Data Sharing Statement
The data that support the findings of this study are openly available in the FinnGen Consortium (https://storage.googleapis.com/finngen-public-data-r10/summary_stats/R10_manifest.tsv).
Ethics Declaration
The data utilized in this study were sourced from publicly available genome-wide association studies (GWAS). The original studies obtained ethical approval and consent from participants, and no further ethical review was required for this analysis. Beijing Chaoyang Hospital Review Board granted an exemption for this study, as it was considered minimal risk. The review board adheres to the Declaration of Helsinki and International Ethical Guidelines for Health-related Research Involving Humans. All GWAS data used in this study are from publicly accessible summary databases, meeting the criteria for exemption from additional review as outlined in the “Ethical Review Measures for Life Sciences and Medical Research Involving Humans”.
Acknowledgments
We want to acknowledge the participants and investigators of the FinnGen study. Additionally, we appreciate Yiting Xia’s assistance from Beijing Cangfeng Shigan Technology Co., Ltd. with optimizing the figures and tables in this paper.
Funding
This work was supported by the National Natural Science Foundation of China (Fund No. 82273551).
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Strazzulla LC, Wang EHC, Avila L, et al. Alopecia areata: disease characteristics, clinical evaluation, and new perspectives on pathogenesis. J Am Acad Dermatol. 2018;78(1):1–12. doi:10.1016/j.jaad.2017.04.1141
2. Safavi KH, Muller SA, Suman VJ, Moshell AN, Melton LJ. Incidence of alopecia areata in Olmsted County, Minnesota, 1975 through 1989. Mayo Clin Proc. 1995;70(7):628–633. doi:10.4065/70.7.628
3. Rajabi F, Drake LA, Senna MM, Rezaei N. Alopecia areata: a review of disease pathogenesis. Br J Dermatol. 2018;179(5):1033–1048. doi:10.1111/bjd.16808
4. Barahmani N, de Andrade M, Slusser JP, et al. Human leukocyte antigen class II alleles are associated with risk of alopecia areata. J Invest Dermatol. 2008;128(1):240–243. doi:10.1038/sj.jid.5700973
5. Megiorni F, Pizzuti A, Mora B, et al. Genetic association of HLA-DQB1 and HLA-DRB1 polymorphisms with alopecia areata in the Italian population. Br J Dermatol. 2011;165(4):823–827. doi:10.1111/j.1365-2133.2011.10466.x
6. Kaufman KD. Androgens and alopecia. Mol Cell Endocrinol. 2002;198(1–2):89–95. doi:10.1016/s0303-7207(02)00372-6
7. Heilmann-Heimbach S, Herold C, Hochfeld LM, et al. Meta-analysis identifies novel risk loci and yields systematic insights into the biology of male-pattern baldness. Nat Commun. 2017;8(1):14694. doi:10.1038/ncomms14694
8. Hagenaars SP, Hill WD, Harris SE, et al. Genetic prediction of male pattern baldness. PLoS Genet. 2017;13(2):e1006594. doi:10.1371/journal.pgen.1006594
9. Hillmer AM, Hanneken S, Ritzmann S, et al. Genetic variation in the human androgen receptor gene is the major determinant of common early-onset androgenetic alopecia. Am J Hum Genet. 2005;77(1):140–148. doi:10.1086/431425
10. Hillmer AM, Brockschmidt FF, Hanneken S, et al. Susceptibility variants for male-pattern baldness on chromosome 20p11. Nat Genet. 2008;40(11):1279–1281. doi:10.1038/ng.228
11. Richards JB, Yuan X, Geller F, et al. Male-pattern baldness susceptibility locus at 20p11. Nat Genet. 2008;40(11):1282–1284. doi:10.1038/ng.255
12. Heilmann-Heimbach S, Hochfeld LM, Paus R, Nöthen MM. Hunting the genes in male-pattern alopecia: how important are they, how close are we and what will they tell us? Exp Dermatol. 2016;25(4):251–257. doi:10.1111/exd.12965
13. Brockschmidt FF, Heilmann S, Ellis JA, et al. Susceptibility variants on chromosome 7p21.1 suggest HDAC9 as a new candidate gene for male-pattern baldness. Br J Dermatol. 2011;165(6):1293–1302. doi:10.1111/j.1365-2133.2011.10708.x
14. Hillmer AM, Flaquer A, Hanneken S, et al. Genome-wide scan and fine-mapping linkage study of androgenetic alopecia reveals a locus on chromosome 3q26. Am J Hum Genet. 2008;82(3):737–743. doi:10.1016/j.ajhg.2007.11.014
15. Futterweit W, Dunaif A, Yeh HC, Kingsley P. The prevalence of hyperandrogenism in 109 consecutive female patients with diffuse alopecia. J Am Acad Dermatol. 1988;19(5):831–836. doi:10.1016/s0190-9622(88)70241-8
16. Schmidt JB, Lindmaier A, Trenz A, Schurz B, Spona J. Hormone studies in females with androgenic hairloss. Gynecol Obstet Invest. 1991;31(4):235–239. doi:10.1159/000293166
17. Yip L, Rufaut N, Sinclair R. Role of genetics and sex steroid hormones in male androgenetic alopecia and female pattern hair loss: an update of what we now know. Australas J Dermatol. 2011;52(2):
18. Yip L, Zaloumis S, Irwin D, et al. Gene-wide association study between the aromatase gene (CYP19A1) and female pattern hair loss. Br J Dermatol. 2009;161(2):289–294. doi:10.1111/j.1365-2133.2009.09186.x
19. Chu SY, Chen YJ, Tseng WC, et al. Comorbidity profiles among patients with alopecia areata: the importance of onset age, a nationwide population-based study. J Am Acad Dermatol. 2011;65(5):949–956. doi:10.1016/j.jaad.2010.08.032
20. Cash TF. The psychosocial consequences of androgenetic alopecia: a review of the research literature. Br J Dermatol. 1999;141(3):
21. Ahouansou S, Le Toumelin P, Crickx B, Descamps V. Association of androgenetic alopecia and hypertension. Eur J Dermatol. 2007;17(3):220–222. doi:10.1684/ejd.2007.0152
22. Hirsso P, Rajala U, Hiltunen L, Jokelainen J, Keinänen-Kiukaanniemi S, Näyhä S. Obesity and low-grade inflammation among young Finnish men with early-onset alopecia. Dermatology. 2007;214(2):125–129. doi:10.1159/000098570
23. Sasmaz S, Senol M, Ozcan A, et al. The risk of coronary heart disease in men with androgenetic alopecia. J Eur Acad Dermat Vene. 1999;12(2):123–125. doi:10.1111/j.1468-3083.1999.tb01001.x
24. Matilainen V, Koskela P, Keinänen-Kiukaanniemi S. Early androgenetic alopecia as a marker of insulin resistance. Lancet. 2000;356(9236):1165–1166. doi:10.1016/S0140-6736(00)02763-X
25. Arias-Santiago S, Gutiérrez-Salmerón MT, Castellote-Caballero L, Buendía-Eisman A, Naranjo-Sintes R. Androgenetic alopecia and cardiovascular risk factors in men and women: a comparative study. J Am Acad Dermatol. 2010;63(3):420–429. doi:10.1016/j.jaad.2009.10.018
26. Su LH, Chen LS, Lin SC, Chen HH. Association of androgenetic alopecia with mortality from diabetes mellitus and heart disease. JAMA Dermatol. 2013;149(5):601–606. doi:10.1001/jamadermatol.2013.130
27. Amoretti A, Laydner H, Bergfeld W. Androgenetic alopecia and risk of prostate cancer: a systematic review and meta-analysis. J Am Acad Dermatol. 2013;68(6):937–943. doi:10.1016/j.jaad.2012.11.034
28. Chiovato L, Magri F, Carlé A. Hypothyroidism in context: where we’ve been and where we’re going. Adv Ther. 2019;36(Suppl 2):47–58. doi:10.1007/s12325-019-01080-8
29. Sekula P, Del Greco MF, Pattaro C, Köttgen A. Mendelian randomization as an Approach to Assess Causality Using observational data. J Am Soc Nephrol. 2016;27(11):3253–3265. doi:10.1016/j.jaad.2017.04.1141
30. Hernán MA, Robins JM. Instruments for causal inference: an epidemiologist’s dream? Epidemiology. 2006;17(4):360–372. doi:10.1097/01.ede.0000222409.00878.37
31. FinnGen provides genetic insights from a well-phenotyped isolated population - PubMed. https://pubmed.ncbi.nlm.nih.gov/36653562/.
32. Burgess S, Scott RA, Timpson NJ, Davey Smith G, Thompson SG. Using published data in Mendelian randomization: a blueprint for efficient identification of causal risk factors. Eur J Epidemiol. 2015;30(7):543–552. doi:10.1007/s10654-015-0011-z
33. Bowden J, Del Greco MF, Minelli C, Davey Smith G, Sheehan NA, Thompson JR. Assessing the suitability of summary data for two-sample Mendelian randomization analyses using MR-Egger regression: the role of the I2 statistic.. Int J Epidemiol. 2016;45(6):1961–1974. doi:10.1093/ije/dyw220
34. Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32(5):377–389. doi:10.1007/s10654-017-0255-x
35. Bakry OA, Basha MA, El Shafiee MK, Shehata WA. Thyroid disorders associated with alopecia areata in Egyptian patients. Indian J Dermatol. 2014;59(1):49–55. doi:10.4103/0019-5154.123494
36. Marahatta S, Agrawal S, Mehata KD. Alopecia areata and thyroid dysfunction association- A study from eastern Nepal. Kathmandu Univ Med J. 2018;16(62):161–165.
37. Lyakhovitsky A, Shemer A, Amichai B. Increased prevalence of thyroid disorders in patients with new onset alopecia areata. Australas J Dermatol. 2015;56(2):103–106. doi:10.1111/ajd.12178
38. Park S-M, Oh Y-J, Lew B-L, Sim W-Y. The association among thyroid dysfunction, thyroid autoimmunity, and clinical features of alopecia areata: a retrospective study. J Am Acad Dermatol. 2019;81(2):602–605. doi:10.1016/j.jaad.2018.04.051
39. Saylam Kurtipek G, Cihan FG, Erayman Demirbaş Ş, Ataseven A. The frequency of autoimmune thyroid disease in alopecia areata and vitiligo patients. Biomed Res Int. 2015;2015:435947. doi:10.1155/2015/435947
40. Shrestha P, Shrestha M, Gurung S. Association between alopecia areata and thyroid dysfunction in western Nepal. Nepal J Med Sci. 2023;8(1):38–42. doi:10.3126/njms.v8i1.54303
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Causal Link of Distinct Mental Disorders with Androgenetic Alopecia and Alopecia Areata: A Bidirectional Two-Sample Mendelian Randomization Study
Hu C, Cheng Z, Tao Y, Zhang L, Zhang Y, Chen Z
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1727-1736
Published Date: 11 July 2025