")
Back to Journals » Clinical Ophthalmology » Volume 19
Relative Behavior of Modern Intraocular Lens Power Calculation Formulas Across a Realistic Range of Biometry Values
Authors Rossip MG, Hastings J, Burwinkel H, Lavrova E, Steinbrenner R, Bensaid N, Cooke DL , Pantanelli SM
Received 22 April 2025
Accepted for publication 11 June 2025
Published 28 June 2025 Volume 2025:19 Pages 2037—2045
DOI https://doi.org/10.2147/OPTH.S529208
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Maxwell G Rossip,1 Jordan Hastings,1 Hendrik Burwinkel,2 Elizaveta Lavrova,2 Ronny Steinbrenner,2 Nicolas Bensaid,2 David L Cooke,3 Seth M Pantanelli1
1Department of Ophthalmology, Penn State College of Medicine, Hershey, PA, USA; 2Carl Zeiss Meditec AG, Oberkochen, Germany; 3Great Lakes Eye Care, St. Joseph, MI, USA
Correspondence: Seth M Pantanelli, Department of Ophthalmology, Penn State College of Medicine, 500 University Drive, HU19, Hershey, PA, 17033, Tel +1717.531.5690, Fax +1717.531.5009, Email [email protected]
Purpose: To investigate the relative performance of modern intraocular lens (IOL) power calculation formulas over a wide range of biometric parameters.
Patients and Methods: Through the concept of emmetropization there exists a mean keratometry, anterior chamber depth, lens thickness, and white-to-white for a given axial length (AL). Using a database of biometric values from 2721 surgery naïve eyes, these relationships were modeled and used to create an artificial dataset of 170 eyes with an anatomically realistic distribution of biometric parameters. Biometric values for each artificial eye were entered into the ESCRS IOL power calculation website. The emmetropic IOL power was calculated for Barrett Universal II, Cooke K6, Kane, PEARL-DGS, HofferQST, EVO v2.0, and Hill-RBF v3.0. Separately, emmetropic IOL powers were calculated for the Zeiss AI formula. The disparity between the formulas was evaluated to determine the ALs at which they diverged.
Results: For eyes with ALs between 22.5 and 28.1 mm, emmetropic IOL powers and spherical equivalent predictions differed by less than 0.25 D. Outside this range, spherical equivalent predictions differed by 0.25 D or more. At ALs < 19.5 mm the difference in emmetropic IOL power across the formulas exceeded 1.0 D.
Conclusion: This work helped to identify an implementation error in Pearl-DGS, which was corrected in collaboration with the formula’s author. Cataract surgeons should consider that formula choice still has a clinically meaningful impact on refractive outcomes in eyes with axial lengths of < 22.5 mm and > 28.1 mm. We estimate that this may represent more than 10% of the population.
Plain Language Summary: Cataract surgeons use IOL power calculation formulas to determine the optimal lens replacement for cataract surgery. These formulas rely on preoperative measurements such as the length of the eye and curvature of the cornea. Several modern formulas exist that can calculate IOL power and predict postoperative refraction accurately in eyes with average measurements. The purpose of this study was to investigate a broad range of eye measurements and show where these formulas still diverge in their predictions. The results of this study show that even modern formulas differ in their power calculations for eyes at extremes and reveal a degree of uncertainty for cataract surgeons when deciding the best-powered lens for patients with relatively long or short eyes.
Keywords: biometry, cataract, axial length, IOL
Introduction
Intraocular lens (IOL) power calculation formulas have evolved substantially over the past 40 years. The vergence-based IOL power calculation formulas of the 1980s and 90s performed well over a narrow range of axial lengths (AL), keratometries (K), and anterior chamber depths (ACD), and less well in eyes with eccentric biometric values (long and short AL, flat and steep K, etc).1 To manage these limitations, surgeons adopted guidelines that helped them to optimize outcomes for specific situations; for example, HofferQ was best for short eyes, Holladay1/2 for average eyes, and SRK/T for long eyes.2 As modern formulas were developed (eg Barrett Universal II, Hill-RBF etc) that worked well over a broader range of values, surgeons were able to eschew these rules-of-thumb.
Today, Barrett Universal II is among the most commonly used IOL power calculation formulas because of its high predictive accuracy over a broad range of biometric values.1,3–5 However, other formulas have since been introduced, most notably, Cooke K6, EVO v2.0, Hill-RBF v3.0, HofferQST, Kane, PEARL-DGS, and Zeiss AI IOL Calculator.6–13 Although these formulas are expected to perform similarly in eyes with average AL, K, and ACD, it is plausible that they might still diverge in their spherical equivalent (SE) predictions with eccentric biometric values. Moreover, because these contemporary formulas are unpublished, it is more challenging to compare their relative performance with that of legacy formulas. In this study, we examined the relative behavior of eight modern IOL power calculation formulas using a synthetic dataset covering the complete medically realistic biometric parameter range.
Methods
Creating the Dataset
Using regression analysis of a larger database of cataract cases, it is possible to determine the representative relationships between the given K, ACD, lens thickness (LT), and AL values. Our intention was to elucidate these relationships and use them to create a dataset of artificial eyes covering the complete range of medically realistic ALs and other corresponding biometric parameters. To that end, the Zeiss’ Veracity database was queried for arrays of real eye biometrics measured preoperatively by one of two optical biometers (IOLMaster 700, Carl Zeiss Meditec AG, Jena, Germany or Lenstar LS 900, Haag-Streit AG, 3098 Köniz, Switzerland) between 04/20/2022 and 09/27/2023. Measurements had to be “Successful” based on the devices’ internal metrics and without AL or K quality assurance warnings. The inclusion criteria required eyes to have a postoperative best-corrected visual acuity (BCVA) of 20/40 or better. This reduces the likelihood of comorbid conditions or prior surgeries that might affect the refractive outcome and nullify biological emmetropization (eg, no history of laser vision correction, congenital glaucoma, keratoconus, pseudophakia, amblyopia, strabismus, pellucid marginal degeneration, retinopathy of prematurity, etc).14–16 Since these data were fully anonymized, the study was not considered human subjects research, and was deemed exempt by the Penn State College of Medicine Institutional Review Board.
Linear regressions were elucidated for ACD, LT, flat (Kmin) and steep (Kmax) keratometry, central corneal thickness (CCT), and white-to-white (WTW) as function of AL. This resulted in regression equations for each parameter. The resultant data clouds with the regression lines are shown in Figure 1.
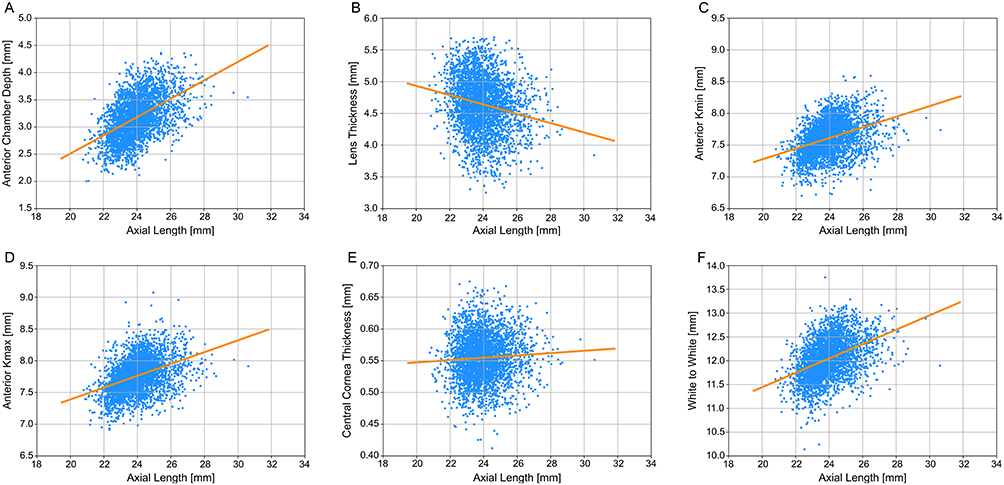 |
Figure 1 Synthetic biometric data (Orange) for anterior chamber depth (A), lens thickness (B), flat Kmin (C), steep Kmax (D), central cornea thickness (E), and white-to-white (F) was derived by linear regression of true eye measurements (blue) relative to axial length. |
An array of AL values ranging from 18.0 to 35.0 mm in 0.1 mm steps was constructed to cover the broad range of potential values. Using the regression coefficients, Kmin, Kmax, ACD, LT, WTW, and CCT were calculated for each corresponding AL. Therefore, the parameter values of this synthetic dataset were linearly correlated with AL and followed the trends provided by the real dataset. This resulted in the parameter coverage listed in Table 1.
 |
Table 1 Biometry Ranges for Dataset of Real Eyes and Dataset of Synthetic Eyes |
The synthetic dataset was created in this manner to fulfill the two necessary requirements for our analysis.
- It should reflect the general linear dependencies between the different biometric parameters using AL as a reference to allow for an assessment of formula behavior across a broad range of medically realistic eyes. This was ensured by modifying all the parameter values across the synthetic dataset.
- It should provide regular increments for all parameters to enable the identification of formula-specific trends which would be lost in statistical variations of arbitrary parameter value combinations or complex fitting models. This was achieved via a strict linear dependency in the fitting process.
Calculations and Formula Selection
The array of artificial biometric values was entered into the European Society of Cataract and Refractive Surgery (ESCRS) IOL calculator (https://iolcalculator.escrs.org) between 01/25/2024 and 03/22/2024, which allowed us to simultaneously calculate IOL power and expected postoperative SEs for seven modern IOL formulas.17 To keep powers and outcomes consistent, we utilized a K-index of 1.3375 and the website’s pre-specified lens constants for each formula corresponding to the Alcon Clareon SY60WF, and assumed the left eye of a 70-year-old female.
The seven formulas for which calculations were performed using the ESCRS IOL calculator were as follows: Barrett Universal II (BU2),5 Cooke K6 (K6),6 Emmetropia Verifying Optical Formula (EVO v2.0),7 Hill Radial Basis Function (Hill-RBF v3.0),9 HofferQST,8 Kane,10 and Pearl-DGS.11 Some formulas have internal constraints, wherein they do not produce a result for highly eccentric biometric values. EVO v2.0, Kane, and Pearl-DGS did not accept ACD values ≥ 5.00 mm, which corresponded to ALs 34.8–35.0 mm. Furthermore, Pearl-DGS would not output IOL powers ≥ 34.0 D. Hill-RBF v3.0 would not accept AL ≤ 19.0 mm. The BU2 and HofferQST formulas accept 170 sets of data spanning the entire data range.
Using the same array of artificial biometric values, K-index, age, gender, and IOL model, IOL powers and predicted postoperative SEs were separately calculated for the Zeiss AI IOL Calculator (ZAIC) by authors H.B., L.L., and R.S. Given the internal parameter constraints, ZAIC provided results for ALs from 19.5 mm to 31.8 mm.
Analysis
For the eight formulas described above, the IOL powers and corresponding predicted postoperative SEs between 0.0 and −0.5 D were recorded. Through extrapolation, the IOL power required to achieve exact emmetropia (0.00 D) was calculated for each artificial eye and formula.
Next, for each synthetic data point and formula, the change in IOL power corresponding to a 0.25 and 0.5 D change in predicted postoperative SE was calculated. For example, for the BU2 formula, 0.3378 D and 0.3906 D changes in IOL power were required to invoke 0.25 D changes in the predicted postoperative SE for eyes with an AL of 22.0 and 28.0 mm, respectively. To show the data points for which the formulas diverged in a clinically meaningful way, the median (across all eight formulas) change in IOL power required to invoke a 0.25 D, 0.5 D, and 1.0 D change in predicted postoperative SE was plotted, as was the difference between the strongest and weakest IOL powers targeting emmetropia, across all eight formulas.
Results
From an initial dataset of 7292 eyes, 2721 eyes met the inclusion criteria for regression derivation. The resultant regression equations and R2 values for each parameter are presented in Table 2. ACD, WTW, Kmin, and Kmax were most strongly correlated with AL, and there was no meaningful correlation between LT and AL or CCT and AL.
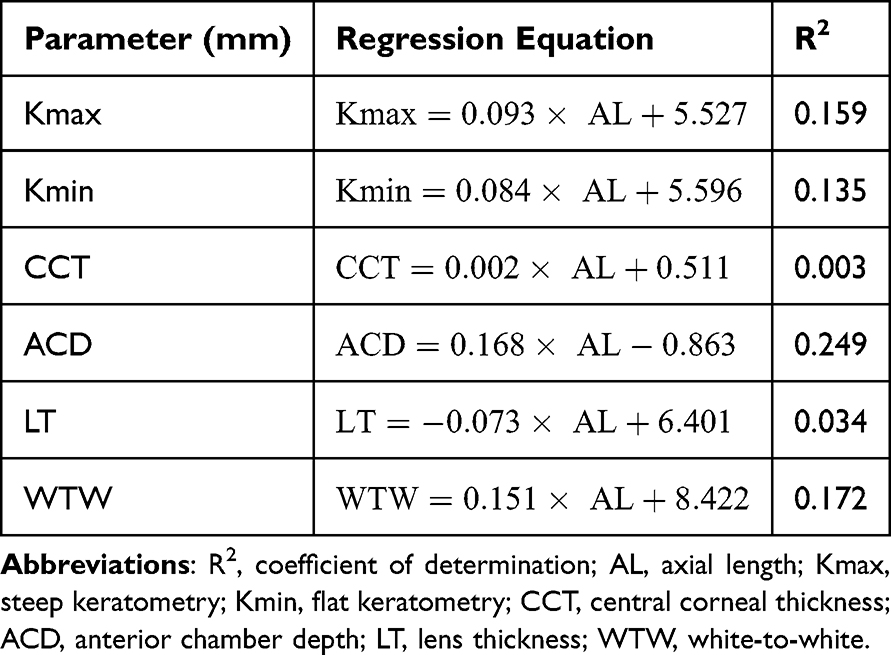 |
Table 2 Linear Regression Equations and Coefficients of Determination for Various Biometric Parameters as a Function of Axial Length |
Figure 2 shows the predicted IOL powers required for an emmetropic outcome for each formula, plotted as a function of AL (A). Figures 2B and C highlight the relative behavior of formulas at the extremes of AL below 21.0 and above 28.0 D, respectively. The eight formulas perform similarly and predict congruent emmetropic IOL powers in the central area of the synthetic dataset. The formulas diverge at extreme values in both directions. For short eyes, the BU2 and Pearl-DGS formulas predicted the most myopic (strongest emmetropic IOL power) outcomes, and Hill-RBF v3.0 and HofferQST predicted the most hyperopic (weakest emmetropic IOL power) outcomes. At ALs of 21.0, 20.0, and 19.0 mm, the eight formulas had a spread of 0.60 D, 0.91 D, and 1.97 D, respectively, with regard to emmetropic IOL power. For long eyes, ZAIC and HofferQST predicted the most myopic outcomes, whereas the Cooke K6 formula predicted the most hyperopic outcomes. At ALs of 28.0, 30.0, and 32.0 mm, the formulas had a spread of 0.36 D, 0.40 D, and 0.61 D, respectively, with regard to emmetropic IOL power. Although the results were plotted as a function of AL to be visualized in 2D graphs, all biometric parameters were propagated according to their correlation with AL through a medically realistic range.
 |
Figure 2 Predicted emmetropic IOL powers for eight modern IOL power calculation formulas over a range of axial lengths from 18.0–35.0 mm (A). Barrett Universal II (red), Cooke K6 (yellow), EVO v2.0 (light green), Hill-RBF v3.0 (dark green), HofferQST (light blue), Kane (dark blue), PEARL-DGS (purple), and Zeiss AI (Orange) are shown in greater detail at short axial lengths from 18.0 −21.0 mm (B) and long axial lengths from 28.0–35.0 mm (C). |
Figure 3 helps elucidate when the formula choice might have a clinically meaningful impact. The difference between the strongest and weakest emmetropic IOL powers (across all eight formulas) is shown in blue. Also shown is the median change in IOL power required to induce a 0.25 (yellow), 0.5 (orange), and 1.0 D (red) change in predicted SE. Between ALs of 22.5 and 28.0 mm, all eight formulas calculate emmetropic IOL powers within 0.4 D and predicted postoperative SEs within 0.25 D of each other. In other words, formula choice is unlikely to have a clinically meaningful impact over this range. However, for ALs ≤ 22.4 mm or ≥ 28.1 mm, emmetropic IOL powers diverge enough to result in more than a 0.25 D difference in predicted SE. In a separate database of eye biometrics of 10,793 patients (Penn State College of Medicine, Hershey, PA, USA), this represented 10.99% of the eyes. For ALs ≤ 20.1 or ≥ 32.9 mm, emmetropic IOL powers diverge enough to result in a difference of more than 0.5 D in the predicted SE. For AL ≤ 19.4 mm, emmetropic IOL powers diverge enough to result in more than 1.0 D difference in predicted SE. At 18.0 and 35.0 mm, emmetropic IOL powers diverge by 3.50 and 1.60 D, respectively.
 |
Figure 3 Largest difference between formulas’ predicted emmetropic IOL powers versus axial length (blue). Also shown is the median change in IOL power required to induce a 0.25 (yellow), 0.5 (Orange), and 1.0 D (red) change in predicted spherical equivalent. |
Supplemental Figure 1 is included as ancillary results because of its significance in the evolution of this project and our field. This figure is similar to Figure 2, except that 1) a different real eye dataset was used to develop the regressions, and 2) emmetropic IOL powers and predicted postoperative SEs span ALs from 17.0 mm to 35.0 mm and were obtained from the ESCRS calculator between 05/10/2023 and 05/27/2023 (before the aforementioned). In this earlier version of the analysis, the Pearl-DGS formula diverged significantly from all other formulas as the AL increased. These results were presented at the IOL Power Club meeting in Palm Springs, CA, in November 2023 and discussed with Dr. Guillaume Debellemanière. This prompted the identification of a sign error in the implementation of the Pearl-DGS formula (personal communication, December 4, 2023), which was promptly corrected. After this correction, the calculations were repeated and the divergence was resolved (as shown in the present study). In essence, this analysis served as a litmus test for formula validity. Therefore, readers should consider that IOL power calculations using the ESCRS IOL Calculator and Pearl-DGS formula performed prior to December 2023 may have been susceptible to this error.
Discussion
The present study confirms what we already know about modern IOL power calculation formulas: they perform more similarly over a broader range of parameter values than the legacy formulas of the 20th century. At the same time, our work adds to the existing body of literature by giving us a glimpse of how different these formulas are from one another at parameter value extremes. Given the paucity of data on real eyes with extremely short and long ALs, it was difficult to determine the relative performance and overall accuracy of these formulas in these subpopulations. As a starting point, the present study provides information about formulas that are likely to produce more myopic (stronger powered IOLs) and hyperopic (weaker powered IOLs) outcomes. When ALs are less than 22.5 mm or greater than 28.0 mm, we suggest that an average of several modern formulas may still be the best strategy.
Although the present study does not allow us to compare the accuracy of modern IOL power calculation formulas, it sheds light on how formulas have evolved and converged relative to legacy formulas such as HofferQ, Holladay1/2, and SRK/T. For example, in the 2018 landmark paper by Melles et al, they found that legacy formulas diverged in their predicted postoperative SE by more than 0.5 D for ALs < 21.0 mm and > 27.0 mm.1 In the present study, with modern formulas, this magnitude of divergence did not occur until ALs were < 20.4 mm or > 32.6 mm. If we accept that formula agreement and convergence are correlated with accuracy, we may have greater confidence when operating over this AL range.
The implications of this study for the patient are several-fold. First, the information herein may be used by surgeons to inform patients that have eccentric biometric values of a less predictable refractive outcome. Second, where the formulas diverge and there are limited data to inform proper formula choice, the results of this study can be used to target a more myopic / hyperopic outcome depending on the goal. For example, if a pathologic hyperope with an AL of 20 mm seeks cataract surgery and the surgeon wishes to maximize the chance of a myopic outcome, this would be most likely to occur if Pearl-DGS or BU2 were used. Likewise, if a surgeon wishes to minimize the chance of a hyperopic outcome in a pathologic myope with an AL of 34 mm, ZAIC or HofferQST would be most likely to succeed in that goal.
One strength of this study lies in the uniform parameters used across IOL formulas. This includes comparing the behavior of the formulas for a single IOL model, the Alcon Clareon SY60WF IOL, using each formula’s respective version of this IOL model. It is known that there can be changes in IOL behavior and power prediction accuracy along the power spectrum and that some formulas are better at adapting to the individual specifics of an IOL than others. Therefore, it can be assumed that IOL-specific formulas, such as Zeiss AI, might show stronger differences in behavior than other formulas optimized via the A-constant.
This study is not without limitations. First, the Zeiss Veracity database does not contain detailed clinical histories of all the eyes contained within. As such, it is plausible that some eyes with previous ocular surgery (eg, scleral buckle) or comorbid conditions (eg, keratoconus) were included in the data clouds used to derive the linear regressions. This could have resulted in some unusual combinations of values, which might have impacted the linear regressions in minor ways. To improve this, eyes with BCVA > 20/40 were excluded, increasing our confidence in the internal validity of the dataset. Second, the dataset of real eyes from which the linear regressions were developed did not contain biometrics with ALs < 19.5 mm or > 31.8 mm. Thus, extrapolations above and below these marks might not accurately correlate with real eyes at these AL extremes. Third, we created a synthetic dataset based on the linear dependency of all biometric parameters from AL. Therefore, although this dataset allows the analysis of the formula behavior across a broader range of parameter values, not all parameters show extreme values or unusual combinations in the covered interval. As described above, this was a deliberate design choice to enable a clear depiction of the formula trends. Finally, the results do not enable one to conclude which formulas are better or more accurate for a given eye biometry; rather, they show relative agreement or disagreement. For physicians, the results shed light on the biometric values for which the formula choice still matters. For researchers and formula creators, the results illustrate the need for refinement among eyes with eccentric values.
It is worth mentioning, perhaps as another limitation, that the present study represents a snapshot in time of relative formula performance. Formula creators are constantly updating their formulas and formula version numbers are not always prominently displayed or disclosed. In fact, as discussed above, the results from this study impacted the implementation of Pearl-DGS for axial myopes, but did not result in a new formula name or version number. It is plausible that even at the time of publication, the formulas mentioned above evolved in minor ways. Future work might include repeating this analysis with additional formulas (eg, Castrop, Oculix), or with respect to mean K or ACD, or in other special populations (eg, post-laser vision correction or keratoconus).
Conclusion
While modern IOL power calculation formulas behave similarly over normal eye biometric measurements, even today these formulas diverge with eccentric measurements. We recommend that cataract surgeons be cautious with formula selection for extreme eye measurements and consider the average prediction of multiple IOL power calculation formulas. These extreme eyes represent a clinically significant proportion of the population, and the formulas’ postoperative predicted SE can vary as much as 1.0 D in these eyes. There remains a need for further research in IOL power calculation formulas for eyes with AL < 21.0 mm and > 27.0 mm.
Data Sharing Statement
Data supporting the results can be obtained upon request from the corresponding author.
Ethics Statement
All data queried from the above study were fully anonymized, and thus were not considered human subject research and were deemed exempt by the Pennsylvania State University College of Medicine Institutional Review Board.
Acknowledgments
The authors thank Guillaume Debellemanière for his correspondence. This paper was presented in part at the IOL Power Club, Palm Springs CA, November 2023 and at the Association of Research and Vision in Ophthalmology (ARVO) Annual Meeting, Seattle WA, May 2024. The abstract of this paper was presented in part at the Association for Research in Vision and Ophthalmology 2024 conference as a poster with interim findings. The poster’s abstract was published in “ARVO Annual Meeting Abstracts” in Investigative Ophthalmology and Visual Science: Relative Behavior of Modern IOL Power Calculation Formulas with Regard to Axial Length.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
HB, NB, EL, and RS are employees of Carl Zeiss Meditec AG. In addition, HB has a patent US2023057389 AA pending to Carl Zeiss Meditec AG. DC received speaker fees from Heidelberg Engineering and royalties from Moptim for use with the Shammas-Cooke formula. SMP received research support from Bausch & Lomb, and Carl Zeiss Meditec AG, all unrelated to the present work. SMP is also a consultant for Bausch & Lomb and Carl Zeiss Meditec AG. The other authors report no conflicts of interest for this work.
References
1. Melles RB, Holladay JT, Chang WJ. Accuracy of intraocular lens calculation formulas. Ophthalmology. 2018;125(2):169–178. doi:10.1016/j.ophtha.2017.08.027
2. Aristodemou P, Knox Cartwright NE, Sparrow JM, Johnston RL. Formula choice: Hoffer Q, Holladay 1, or SRK/T and refractive outcomes in 8108 eyes after cataract surgery with biometry by partial coherence interferometry. J Cataract Refract Surg. 2011;37(1):63–71. doi:10.1016/j.jcrs.2010.07.032
3. Wang L, Shirayama M, Ma XJ, Kohnen T, Koch DD. Optimizing intraocular lens power calculations in eyes with axial lengths above 25.0 mm. J Cataract Refract Surg. 2011;37(11):2018–2027. doi:10.1016/j.jcrs.2011.05.042
4. Abulafia A, Barrett GD, Rotenberg M, et al. Intraocular lens power calculation for eyes with an axial length greater than 26.0 mm: comparison of formulas and methods. J Cataract Refract Surg. 2015;41(3):548–556. doi:10.1016/j.jcrs.2014.06.033
5. Barrett Universal II Formula V1.05. Available from: https://calc.apacrs.org/barrett_universal2105/.
6. K6 Formula. Available from: https://cookeformula.com/.
7. EVO IOL Calculator v2.0. Available from: https://www.evoiolcalculator.com/calculator.aspx.
8. Hoffer® QST. Available from: https://hofferqst.com/.
9. Hill-RBF Calculator for IOL Power Calculations. Available from: https://rbfcalculator.com/online/index.html.
10. Formula K. Available from: https://www.iolformula.com/.
11. Solver. Available from: https://iolsolver.com/.
12. Debellemanière G, Dubois M, Gauvin M, et al. The PEARL-DGS formula: the development of an open-source machine learning-based thick IOL calculation formula. Am J Ophthalmol. 2021;232:58–69. doi:10.1016/j.ajo.2021.05.004
13. ZEISS AI IOL Calculator data-driven IOL power calculation formula. Available from: https://www.zeiss.com/meditec/en/products/veracity/ai-iol-calculator.html.
14. Mutti DO, Mitchell GL, Jones LA, et al. Axial growth and changes in lenticular and corneal power during emmetropization in infants. Investigative Ophthalmology & Visual Science. 2005;46(9):3074–3080. doi:10.1167/iovs.04-1040
15. Harrie RP. Factors in emmetropization. In: Ossoinig KC, ed.
16. Wong CW, Ang M, Tsai A, Phua V, Lee SY. A prospective study of biometric stability after scleral buckling surgery. Am J Ophthalmol. 2016;165:47–53. doi:10.1016/j.ajo.2016.02.023
17. IOL Calculator. Available from: https://iolcalculator.escrs.org/.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optical Biometry and Lens Power Calculations in 500 Phakic Patients: Axial Length and Corneal Curvature in the Fellow Eye
Kristianslund O, Hassaf SE, Drolsum L
Clinical Ophthalmology 2022, 16:2775-2780
Published Date: 23 August 2022
Efficacy of a One-Piece Aberration Neutral Hydrophobic Acrylic Toric Intraocular Lens
Buckhurst PJ, Lau G, Williams JI, Packer M
Clinical Ophthalmology 2022, 16:3763-3774
Published Date: 15 November 2022
Impact of Cataract Surgery on IOP and Ocular Structures in Normotensive Patients and Primary and Exfoliation Open-Angle Glaucoma Patients
Xirou V, Xirou T, Siganos C, Ntonti P, Georgakopoulos C, Stavrakas P, Makri OE, Kanakis M, Tsapardoni F, Fragkoulis I, Garnavou-Xirou C, Kozobolis V
Clinical Ophthalmology 2023, 17:1047-1055
Published Date: 5 April 2023
Optical Biometry Changes Throughout Childhood and Adolescence in Patients Wearing Ortho-K Lenses
Mahmoud O, Andrews C, Soeken T, Nallasamy S, Nallasamy N
Clinical Ophthalmology 2023, 17:1919-1927
Published Date: 4 July 2023