")
Back to Journals » Clinical Ophthalmology » Volume 19
Reproducibility and Screening Capability of Corneal Epithelial Thickness Measurement for Keratoconus Using Anterior Segment Optical Coherence Tomography
Authors Oshika T, Sawaki A, Nishida T, Nakamura T , Kojima T
Received 7 April 2025
Accepted for publication 14 June 2025
Published 30 June 2025 Volume 2025:19 Pages 2057—2065
DOI https://doi.org/10.2147/OPTH.S528630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Taro Oshika,1 Ayako Sawaki,2,3 Tomoya Nishida,3 Tomoaki Nakamura,3 Takashi Kojima2,3
1Department of Ophthalmology, Japanese Red Cross Gifu Hospital, Gifu, Japan; 2Department of Ophthalmology, Japanese Community Healthcare Organization Chukyo Hospital, Nagoya, Japan; 3Department of Ophthalmology, Nagoya Eye Clinic, Nagoya, Japan
Correspondence: Takashi Kojima, Department of Ophthalmology, Nagoya Eye Clinic, COLLECT MARK Kanayama 2F, 24-14 Namiyose-cho, Atsuta-ku, Nagoya, Aichi, 456-0003, Japan, Tel +81 52 872 0490, Fax +81 52 872 0491, Email [email protected]
Purpose: To investigate the reproducibility of corneal epithelial thickness measurements using anterior segment optical coherence tomography (AS-OCT, CASIA2, TOMEY) and evaluate its potential for the diagnosis of keratoconus.
Patients and Methods: This study included patients diagnosed with stage 1– 2 keratoconus (Amsler-Krumeich classification) at the Nagoya Eye Clinic and healthy controls. Corneal epithelial thickness was measured with the CASIA2 AS-OCT. Sixteen patients with keratoconus (16 eyes) and 11 healthy controls (11 eyes) underwent three consecutive measurements to determine the intraclass correlation coefficient (ICC). Measurements were taken for eight corneal sections in 40 keratoconus eyes (mean age: 25.5 ± 8.0 years) and 44 normal eyes (mean age: 24.2 ± 5.1 years). The mean corneal epithelial thickness, the upper-to-lower corneal epithelial thickness ratio, and the standard deviation of thickness across segments were compared between the two groups. Logistic regression analysis was used to evaluate corneal epithelial thickness-related parameters for the diagnosis of keratoconus. The cutoff value was determined using the Youden index derived from the receiver operating characteristic (ROC) curve.
Results: The ICC was ≥ 0.95 in all areas for both keratoconus and normal eyes. The superior paracentral corneal epithelium was significantly thicker in the keratoconus eyes, whereas the inferior paracentral area was thinner compared to normal eyes (p< 0.001). The standard deviation of corneal epithelial thickness was significantly higher in keratoconus eyes across all regions. Logistic regression analysis identified the standard deviation of corneal epithelial thickness (2– 5 mm) and the mean thickness ratio (0– 5 mm) as explanatory variables. The area under the ROC curve was 0.955, with sensitivity and specificity of 92.1% and 100%, respectively.
Conclusion: Corneal epithelial thickness measurements using the AS-OCT CASIA2 were highly reproducible and showed significant differences between early-stage keratoconus and normal corneas. These findings suggest its potential utility as a screening tool for keratoconus.
Keywords: keratoconus, corneal epithelial thickness, diagnosis, anterior segment optical coherence tomography
Introduction
Keratoconus is a corneal ectatic disorder primarily affecting individuals between 10 and 30 years of age. Progression of the disease leads to increased corneal irregular astigmatism and a decline in spectacle-corrected visual acuity.1–3 Corneal crosslinking (CXL), developed by Seiler et al, has been evaluated for its effectiveness in preventing the progression of keratoconus. Recently, the adoption of CXL has expanded as evidence of its safety and efficacy has grown.4,5 Consequently, early detection of keratoconus has become increasingly important.
Numerous studies have highlighted the utility of corneal topography and tomography in the early diagnosis of keratoconus, and these techniques are now widely applied in clinical practice.6–9 Recent advances in examination devices have enabled direct assessment of corneal biomechanical properties, providing insights into the structural vulnerability of keratoconus.10,11 Methods that integrate assessments of corneal biomechanical properties with corneal shape have demonstrated enhanced diagnostic utility.12–14
The corneal epithelium undergoes compensatory remodeling of its thickness in response to alterations in the anterior corneal surface. This adaptive mechanism may obscure early-stage anterior corneal protrusion in keratoconus.4 Efforts to detect keratoconus at its earliest stages have focused on identifying these epithelial thickness changes. Very high-frequency digital ultrasound (VHFDU) and anterior segment optical coherence tomography (AS-OCT) have been used to measure corneal epithelial thickness.15 However, VHFDU is a water immersion system that requires considerable skill, whereas noninvasive AS-OCT has gained broader acceptance in clinical settings due to its ease of use.5,16–19
OCT captures backscattered light from the boundary surfaces where the refractive index changes within the cornea. In normal corneal tissue, each layer maintains a relatively uniform refractive index, allowing boundary surfaces to appear distinct on OCT images due to differences in refractive indices.6,7 The interface between the corneal epithelium and the corneal stroma produces less backscatter compared to the anterior and posterior surfaces of the cornea, necessitating high-resolution OCT systems to accurately identify the corneal epithelium.
Although no direct comparative studies have been conducted between CASIA2 and other anterior segment OCT devices, its key advantage lies in the broad range of clinically useful analyses it offers. CASIA2 uses a 1310 nm swept-source and high-speed scanning to provide high-quality 3D imaging of the anterior segment. It enables preoperative assessment of total corneal astigmatism, higher-order aberrations, topography, and lens geometry including tilt and decentration. Recent advancements have allowed CASIA2 to segment the posterior surface of the corneal epithelium and measure corneal epithelial thickness. However, reports on the reproducibility of corneal epithelial thickness measurements or the evaluation of keratoconus using CASIA2 remain limited.
This study aimed to assess the reproducibility of corneal epithelial thickness measurements in normal and keratoconus eyes using CASIA2. Additionally, the study investigated the utility of corneal epithelial thickness as a parameter for diagnosing keratoconus.
Materials and Methods
Patients and Healthy Controls
This retrospective study was conducted at the Nagoya Eye Clinic. The inclusion criteria for keratoconus patients were as follows: keratoconus was diagnosed by a corneal specialist using slit-lamp microscopy, corneal topography, and corneal tomography. The severity of keratoconus was classified as stage 1 or 2 according to the Amsler-Krumeich classification. Eyes with diseases other than keratoconus or with corneal opacities were excluded from the study.For the normal control group, the inclusion criteria were no history of ocular surgery, no ocular diseases other than refractive error, and no abnormal findings on anterior segment optical coherence tomography (AS-OCT, CASIA2, TOMEY, Nagoya, Japan) or slit-lamp microscopy.
According to the inclusion and exclusion criteria, 16 eyes from 16 patients (mean age 29.2 ± 13.1 years) with keratoconus and 11 eyes from 11 healthy controls (mean age, 24.2 ± 5.1 years) were included for the reproducibility analysis. To evaluate corneal thickness and assess keratoconus screening, an additional 40 eyes from 40 keratoconus patients (mean age, 25.5 ± 8.0 years) and 44 eyes from 44 healthy controls (mean age, 24.2 ± 5.1 years) were included.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Nagoya Eye Clinic (2023–61). The ethics committee approved the use of an opt-out method, and the requirement for informed consent was waived due to the retrospective nature of the study.
Evaluation of Corneal Epithelial Thickness
Corneal epithelial thickness was analyzed using the AS-OCT CASIA2 (TOMEY). Measurements were performed thrice on the same day by a certified and experienced orthoptist, and the average of the three measurements was recorded. The analysis encompassed a 7-mm diameter area of the cornea, divided into three concentric zones: 0–2 mm, 2–5 mm, and 5–7 mm from the center. Each zone was further subdivided into eight 45-degree sections, yielding a total of 24 segments. The mean and standard deviation of corneal epithelial thickness in each segment were analyzed.
Corneal Epithelial Thickness Ratio Calculation Method
The corneal epithelial thickness ratio was defined as the ratio of the average corneal epithelial thicknesses of the upper and lower corneas (upper corneal thickness/lower corneal thickness). This ratio was calculated within the zones of 0–2 mm, 2–5 mm, 5–7 mm, and 0–5 mm. Comparisons of the corneal epithelial thickness ratio were conducted between the keratoconus and control groups.
Investigation of the Usefulness of Keratoconus Diagnosis
A logistic regression analysis was performed to evaluate the diagnostic utility for keratoconus. The dependent variable was a dummy variable, coded as 1 for keratoconus and 0 for normal. Independent variables included the mean corneal epithelial thickness, the standard deviation of corneal epithelial thickness, and the corneal epithelial thickness ratio.
Statistical Analysis
Comparisons of the corneal epithelial thickness, standard deviation of corneal epithelial thickness, and corneal epithelial thickness ratio between the keratoconus and control groups were conducted using the Mann–Whitney U-test. All statistical analyses were performed using SPSS (VER.29), with a significance level set at less than 5%.
Results
For the reproducibility analysis, the keratoconus group included 12 males and 4 females, with a mean keratometry of 49.4 ± 3.8 D. The healthy control group included 9 males and 2 females, with a mean keratometry of 43.2 ± 1.2 D. For the corneal thickness and keratoconus screening evaluations, the keratoconus group comprised 34 males and 6 females, with a mean keratometry of 45.11 ± 1.60 D. The healthy control group comprised 41 males and 3 females, with a mean keratometry of 42.77 ± 1.24 D. Table 1 summarizes the demographic characteristics of the study participants.
 |
Table 1 Demographic Information of Patients with Keratoconus and Healthy Controls |
Comparison of Reproducibility of Corneal Epithelial Thickness in Keratoconus and Normal Eyes Implant
Figure 1 shows the mean intraclass correlation coefficients (ICCs) for corneal epithelial thickness measurements in keratoconus and normal eyes. For the keratoconus group, the mean ICCs were 0.962, 0.961, and 0.970 for the 0–2 mm, 2–5 mm, and 5–7 mm zones, respectively. For the normal control group, the mean ICCs were 0.977, 0.985, and 0.985, respectively.
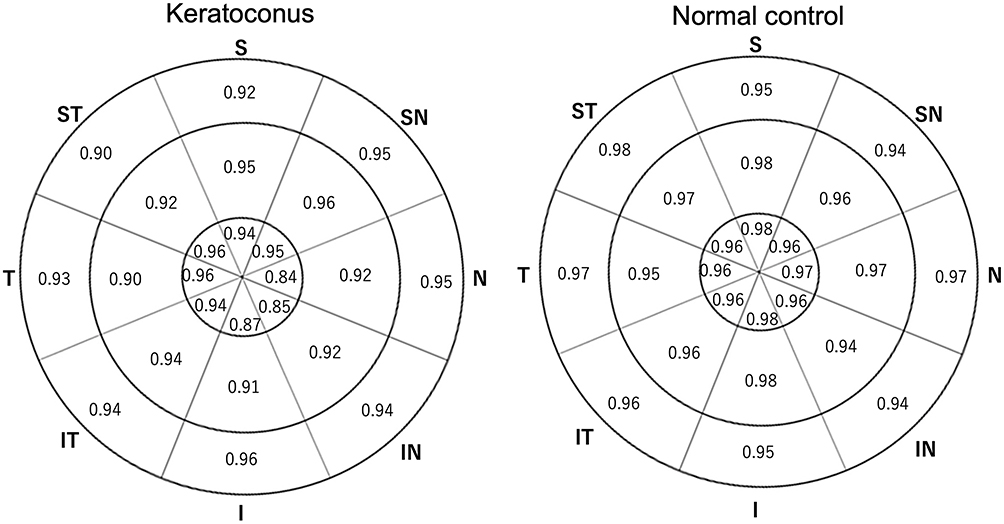 |
Figure 1 Mean intraclass correlation coefficient (ICC) of corneal thickness measurements for keratoconus and normal eyes. The keratoconus group exhibited slightly lower ICC values compared to the normal group; however, both groups had ICC values above 0.8 in all measured areas. |
Mean Corneal Epithelial Thickness
Table 2 presents the mean corneal epithelial thickness results. In the nasal (N), inferonasal (IN), inferior (I), inferotemporal (IT), and temporal (T) areas, the keratoconus group exhibited significantly lower thickness values compared to the control group (p<0.05). In the superior (S) and superotemporal (ST) areas, the keratoconus group showed significantly higher thickness values than the control group (p<0.05).
 |
Table 2 Comparison of Mean Corneal Epithelial Thickness Between the Keratoconus and Control Groups |
Standard Deviation of Corneal Epithelial Thickness
The standard deviation of corneal epithelial thickness is shown in Table 3. In all regions, the keratoconus group showed significantly higher values than the control group (p<0.05 across all areas).
 |
Table 3 Comparison of the Standard Deviation of Corneal Epithelial Thickness Between the Keratoconus and Control Groups |
Corneal Epithelial Thickness Ratio
Table 4 shows the mean corneal epithelial thickness ratios for the keratoconus and control groups. In the keratoconus group, the mean ratios (95% confidence interval) were 1.05 (1.04–1.06) for the 0–2 mm zone, 1.07 (1.05–1.09) for the 2–5 mm, and 1.02 (1.00–1.02) for the 5–7 mm zone. For the control group, the corresponding values were 0.99 (0.99–1.00), 0.99 (0.98–0.99), and 0.98 (0.98–0.99), respectively. The keratoconus group exhibited significantly higher ratios across all zones compared to the control group (p<0.001).
 |
Table 4 Comparison of the Mean Corneal Epithelial Thickness Ratio Between the Keratoconus and Control Groups |
Investigation of the Usefulness of Keratoconus Diagnosis
Logistic regression analysis identified the standard deviation of corneal epithelial thickness in 2–5 mm and 0–5 mm ranges as explanatory variables. The area under the receiver operating characteristic curve (AUROC) was 0.955, with a cut-off value of 0.494, and the sensitivity and specificity were 92.1% and 100%, respectively (Figure 2).
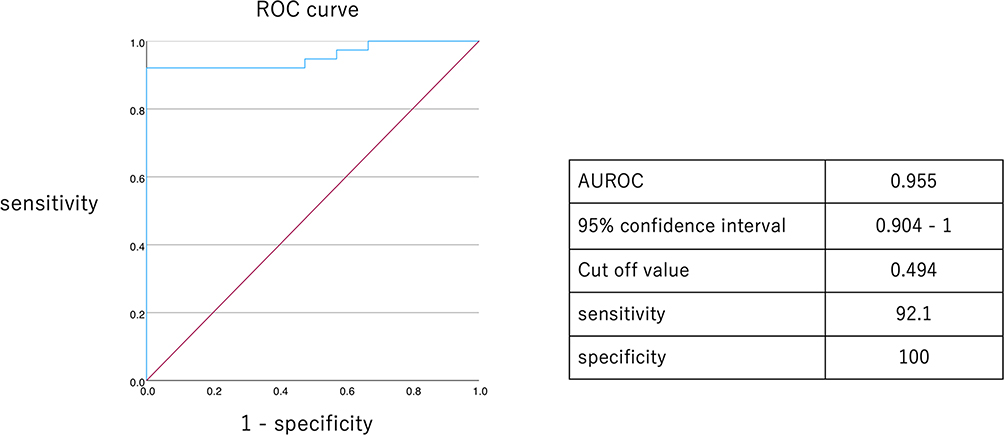 |
Figure 2 Receiver operating characteristic (ROC) analysis illustrating the sensitivity and specificity of keratoconus screening using corneal epithelial thickness. Abbreviation: AUROC, area under the ROC curve. |
Discussion
The CASIA2 AS-OCT system has gained widespread use in evaluating anterior segment structures.20–22 This study employed CASIA2 to evaluate the reproducibility of corneal epithelial thickness measurement in keratoconus eyes and compared corneal epithelial thickness between keratoconus and normal eyes. Additionally, the study explored the usefulness of corneal epithelial thickness parameters for diagnosing keratoconus. To our knowledge, this represents the first study evaluating keratoconus eyes using corneal epithelial thickness measurements obtained with CASIA2.
Firstly, in this study, the reproducibility of three consecutive measurements in keratoconus eyes was comparable to that in normal eyes, suggesting sufficient reliability for clinical application. However, the ICC showed a slight tendency to be lower in the central and lower regions of keratoconus eyes. This discrepancy may stem from the pronounced fluctuation in epithelial thickness observed in keratoconus eyes. A minor shift in the center of measurement could lead to variability in the recorded values due to these fluctuations.
Compensatory changes in corneal epithelial thickness are a hallmark of keratoconus, reflecting the thinning and steepening of the cornea.3,23 Consistent with previous reports, corneal epithelial thickness in keratoconus eyes was thinner at the inferior region and the inferior temporal region compared to normal eyes.24 Additionally, another study reported a significantly larger standard deviation of corneal epithelial thickness in keratoconus eyes compared to normal eyes.25 These results suggest that assessing corneal epithelial thickness may enable the detection of subtle changes on the anterior corneal surface associated with localized steepening. Such changes may be masked by epithelial remodeling, particularly in the early stages of keratoconus.
In this study, the standard deviation was employed as an index to assess intra-sectoral variations in corneal epithelial thickness. The findings demonstrated that the standard deviation of corneal epithelial thickness increased across all regions within the 0–2 mm, 2–5 mm, and 5–7 mm ranges. This likely reflects more pronounced local corneal stromal shape changes in keratoconus eyes. Previous studies using RTVue have shown heterogeneity in corneal epithelial thickness in patients with keratoconus,26 and other reports using SD-OCT (Spectralis Heidelberg) have shown an increased standard deviation of corneal epithelial thickness in keratoconus compared to normal corneas.27 The present results were consistent with previous reports.
In this study, the mean corneal epithelial thickness ratio in keratoconus was greater than that in normal corneas, with a value of 1.07 for the 2–5 mm region. A previous study reported that in keratoconus (mean K: 46.44 ± 4.13), the corneal epithelial thickness ratio increased with disease severity, as indicated by worsening logMAR visual acuity.8 In that report, the corneal epithelial thickness ratio was below 0.95 in normal eyes and exceeded 1.00 in severe keratoconus. Although direct comparison is limited due to differences in the measurement areas between the two studies, a similar trend of increased corneal epithelial thickness ratio in keratoconus compared to normal corneas was observed.
The logistic regression analysis in this study revealed that the standard deviation of corneal epithelial thickness and the corneal epithelial thickness ratio effectively distinguished keratoconus from normal corneas with high accuracy. A previous study analyzing corneas approximately 10 mm in diameter reported that the thickness of the corneal epithelium and Bowman’s layer successfully differentiated subclinical keratoconus from normal corneas, achieving an AUC of 0.984, with sensitivity and specificity values of 100% and 90.5%, respectively.28 Another study analyzing corneas with an 8 mm diameter used the standard deviation of corneal epithelial thickness and the corneal epithelial thickness ratio to identify keratoconus, reporting an AUC of 0.92, sensitivity of 74.0%, and specificity of 96.7% for the corneal epithelial thickness ratio.29 The AUROC in our study was 0.955, which was similar to that in previous studies, indicating that the corneal epithelial thickness parameters measured by CASIA2 provide robust utility in diagnosing keratoconus.
This study had several limitations. Although this study demonstrated high intra-operator reproducibility, inter-operator reproducibility was not evaluated. As the anterior segment OCT used in this study includes an automatic parameter measurement function, inter-operator reproducibility is presumed to be high; however, further investigation is warranted. The diagnostic accuracy for early suspected keratoconus or forme fruste keratoconus (FFK) remained unknown, as the analysis included only cases already diagnosed with keratoconus. Future research should focus on evaluating even earlier cases than those assessed in this study. Previous reports have indicated an association between corneal epithelial thickness and corneal stromal thickness.10,30 One study suggested that incorporating changes in the thickness of Bowman’s layer could enhance the accuracy of diagnosing suspected FFK or keratoconus.11 These findings indicate that comprehensive evaluations considering corneal epithelial thickness, corneal stromal thickness, and posterior corneal shape may improve screening accuracy.13
In laser corneal refractive surgery, thorough preoperative screening is essential to ensure the safety and stability of postoperative outcomes. One of the most critical aspects of this screening process is the identification and exclusion of keratoconus and other forms of corneal ectatic disorders, as undetected subclinical keratoconus is a major risk factor for the development of postoperative keratectasia—a potentially sight-threatening complication. Although conventional corneal topography and tomography are widely used to detect keratoconus, these modalities may not always identify early or subclinical forms of the disease with sufficient sensitivity. In this context, evaluating the corneal epithelial thickness profile, which can reflect subtle biomechanical or morphological changes in the cornea, may offer additional diagnostic value. The use of anterior segment OCT to assess epithelial thickness has the potential to enhance the screening protocol by providing complementary information to traditional imaging techniques. Future studies should explore whether integrating epithelial thickness measurements with topographic and tomographic indices can lead to improved sensitivity and specificity in detecting early keratoconus, thereby contributing to safer refractive surgical practices.
Conclusion
In conclusion, corneal epithelial thickness measurements using CASIA2 demonstrated high reproducibility and may aid in the accurate diagnosis of keratoconus.
Data Sharing Statement
All data generated or analyzed during this study are included in the Supplementary Data 1. Further enquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
Study approval statement:
This retrospective study was approved by the Institutional Review Board of the Nagoya Eye Clinic (2023-61). The study was performed in accordance with the tenets of the Declaration of Helsinki.
Consent to participate statement:
An opt-out method was approved, and the need for obtaining written informed consent was waived.
Acknowledgments
This study was orally presented at the 127th Annual Meeting of the Japanese Ophthalmological Society, held in Tokyo, Japan, on April 6–9, 2023.
Author Contributions
All authors made a significant contribution to the work reported, including either the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any funding relevant to this study.
Disclosure
Dr. Nakamura reports receiving personal fees from Staar Surgical, HOYA, and Carl Zeiss Meditec, outside of the submitted work. Dr. Kojima reports receiving personal fees from Staar Surgical, Santen Pharmaceutical, HOYA, SEED, Ophtecs and Alcon Japan, outside of the submitted work. The authors report no other conflicts of interest in this work.
References
1. Santodomingo-Rubido J, Carracedo G, Suzaki A, Villa-Collar C, Vincent SJ, Wolffsohn JS. Keratoconus: an updated review. Cont Lens Anterior Eye. 2022;45(3):101559. doi:10.1016/j.clae.2021.101559
2. Deshmukh R, Ong ZZ, Rampat R, et al. Management of keratoconus: an updated review. Front Med. 2023;10:1212314.
3. Gomes JA, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359–369. doi:10.1097/ICO.0000000000000408
4. Ng SM, Hawkins BS, Kuo IC. Transepithelial versus epithelium-off corneal crosslinking for progressive keratoconus: findings from a cochrane systematic review. Am J Ophthalmol. 2021;229:274–287. doi:10.1016/j.ajo.2021.05.009
5. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627. doi:10.1016/S0002-9394(02)02220-1
6. Sedghipour MR, Sadigh AL, Motlagh BF. Revisiting corneal topography for the diagnosis of keratoconus: use of Rabinowitz’s KISA% index. Clin Ophthalmol. 2012;6:181–184. doi:10.2147/OPTH.S24219
7. Nicula CA, Bulboacă AE, Nicula D, Nicula AP, Horvath KU, Bolboacă SD. Performances of corneal topography and tomography in the diagnosis of subclinical and clinical keratoconus. Front Med. 2022;9:904604. doi:10.3389/fmed.2022.904604
8. Fukuda S, Beheregaray S, Hoshi S, et al. Comparison of three-dimensional optical coherence tomography and combining a rotating Scheimpflug camera with a Placido topography system for forme fruste keratoconus diagnosis. Br J Ophthalmol. 2013;97(12):1554–1559. doi:10.1136/bjophthalmol-2013-303477
9. Maeda N, Klyce SD, Smolek MK, Thompson HW. Automated keratoconus screening with corneal topography analysis. Invest Ophthalmol Vis Sci. 1994;35(6):2749–2757.
10. Elham R, Jafarzadehpur E, Hashemi H, et al. Keratoconus diagnosis using Corvis ST measured biomechanical parameters. J Curr Ophthalmol. 2017;29(3):175–181. doi:10.1016/j.joco.2017.05.002
11. Yang K, Xu L, Fan Q, et al. Evaluation of new Corvis ST parameters in normal, Post-LASIK, Post-LASIK keratectasia and keratoconus eyes. Sci Rep. 2020;10(1):5676. doi:10.1038/s41598-020-62825-y
12. Hashemi H, Seyedian MA, Miraftab M, Fotouhi A, Asgari S. Corneal collagen cross-linking with riboflavin and ultraviolet a irradiation for keratoconus: long-term results. Ophthalmology. 2013;120(8):1515–1520. doi:10.1016/j.ophtha.2013.01.012
13. Kato N, Konomi K, Shinzawa M, et al. Corneal crosslinking for keratoconus in Japanese populations: one year outcomes and a comparison between conventional and accelerated procedures. Jpn J Ophthalmol. 2018;62(5):560–567. doi:10.1007/s10384-018-0610-9
14. Aixinjueluo W, Usui T, Miyai T, Toyono T, Sakisaka T, Yamagami S. Accelerated transepithelial corneal cross-linking for progressive keratoconus: a prospective study of 12 months. Br J Ophthalmol. 2017;101(9):1244–1249. doi:10.1136/bjophthalmol-2016-309775
15. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ. Repeatability of layered corneal pachymetry with the Artemis very high-frequency digital ultrasound arc-scanner. J Refract Surg. 2010;26(9):646–659. doi:10.3928/1081597X-20091105-01
16. Abicca I, Schiano-Lomoriello D, Gilardi M, et al. Repeatability of automatic measurements by an anterior segment swept-source OCT biometer in patients with keratoconus. J Refract Surg. 2024;40(7):e445–e452. doi:10.3928/1081597X-20240514-03
17. Mencucci R, Paladini I, Virgili G, Giacomelli G, Menchini U. Corneal thickness measurements using time-domain anterior segment OCT, ultrasound, and Scheimpflug tomographer pachymetry before and after corneal cross-linking for keratoconus. J Refract Surg. 2012;28(8):562–566. doi:10.3928/1081597X-20120703-02
18. Said OM, Kamal M, Tawfik S, Saif AT. Comparison of corneal measurements in normal and keratoconus eyes using anterior segment optical coherence tomography (AS-OCT) and pentacam HR topographer. BMC Ophthalmol. 2023;23(1):194. doi:10.1186/s12886-023-02946-w
19. Seiler TG, Mueller M, Mendes Baiao T. Repeatability and comparison of corneal tomography in mild to severe keratoconus between the anterior segment OCT MS-39 and pentacam HR. J Refract Surg. 2022;38(4):250–255. doi:10.3928/1081597X-20220114-02
20. Saito A, Kamiya K, Fujimura F, Takahashi M, Shoji N. Comparison of angle-to-angle distance using three devices in normal eyes. Eye. 2020;34(6):1116–1120. doi:10.1038/s41433-019-0653-2
21. Weller JM, Hübner L, Kruse FE, Tourtas T. Characterisation of ectasia after penetrating keratoplasty in keratoconus eyes using anterior segment optical coherence tomography. Br J Ophthalmol. 2024;108(4):506–512. doi:10.1136/bjo-2022-322859
22. Langenbucher A, Hoffmann P, Cayless A, Wendelstein J, Szentmáry N. Evaluation of statistical correction strategies for corneal back surface astigmatism with toric lenses: a vector analysis. J Cataract Refract Surg. 2024;50(4):385–393. doi:10.1097/j.jcrs.0000000000001370
23. Franco J, White CA, Kruh JN. Analysis of compensatory corneal epithelial thickness changes in keratoconus using corneal tomography. Cornea. 2020;39(3):298–302. doi:10.1097/ICO.0000000000002156
24. Toprak I, Vega A, Del Barrio JL, Espla E, Cavas F, Alió JL. Diagnostic value of corneal epithelial and stromal thickness distribution profiles in forme fruste keratoconus and subclinical keratoconus. Cornea. 2021;40(1):61–72. doi:10.1097/ICO.0000000000002435
25. Santhiago MR, Stival LR, Araujo DC, Kara-Junior N, Toledo MC. Role of corneal epithelial measurements in differentiating eyes with stable keratoconus from eyes that are progressing. Ophthalmol Sci. 2023;3(1):100256. doi:10.1016/j.xops.2022.100256
26. Maeda N, Nakagawa T, Higashiura R, Fuchihata M, Koh S, Nishida K. Evaluation of corneal epithelial and stromal thickness in keratoconus using spectral-domain optical coherence tomography. Jpn J Ophthalmol. 2014;58(5):389–395. doi:10.1007/s10384-014-0338-0
27. Salomão MQ, Hofling-Lima AL, Gomes Esporcatte LP, et al. Corneal ectasia detection by epithelial pattern standard deviation from OCT. J Cataract Refract Surg. 2023;49(2):190–194. doi:10.1097/j.jcrs.0000000000001066
28. Hu L, Li Y, Liu Q, et al. Corneal vertical and horizontal thickness profiles generated by UHR-OCT for suspected and subclinical keratoconus diagnosis. J Refract Surg. 2021;37(7):438–445. doi:10.3928/1081597X-20210330-01
29. Vega-Estrada A, Mimouni M, Espla E, Del Barrio JA, Alio JL. Corneal epithelial thickness intrasubject repeatability and its relation with visual limitation in keratoconus. Am J Ophthalmol. 2019;200:255–262. doi:10.1016/j.ajo.2019.01.015
30. Reinstein DZ, Gobbe M, Archer TJ, Silverman RH, Coleman DJ. Epithelial, stromal, and total corneal thickness in keratoconus: three-dimensional display with artemis very-high frequency digital ultrasound. J Refract Surg. 2010;26(4):259–271. doi:10.3928/1081597X-20100218-01
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.