")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Response Time and Influencing Factors Among Emergency Nurses in Indonesian Hospital: A Scoping Review of Current Evidence
Authors Ramdani D , Kosasih CE, Emaliyawati E
Received 10 October 2024
Accepted for publication 22 November 2024
Published 13 January 2025 Volume 2025:18 Pages 133—145
DOI https://doi.org/10.2147/JMDH.S498227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Dadan Ramdani,1 Cecep Eli Kosasih,2 Etika Emaliyawati2
1Postgraduate Program of Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, 45363, Indonesia; 2Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, 45363, Indonesia
Correspondence: Etika Emaliyawati, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia, Email [email protected]
Background: The incidence of mass casualty incidents and severe emergencies such as cerebrovascular and motor vehicle accidents in Indonesia is increasing, leading to an increased burden on emergency services. The current literature on response times and associated factors in Indonesian emergency departments (EDs) is extensive yet lacks comprehensive national and regional analysis.
Objective: This study aimed to synthesize existing research on emergency nurse response times in Indonesian hospital settings and identify the factors influencing these times.
Methods: This study was guided by the PRISMA-ScR framework. This study systematically searched the PubMed/MEDLINE, CENTRAL/Cochrane, EBSCOhost, and Google Scholar databases for studies published between 2019 and 2024. The included studies focused on empirical measurements of response times, defined as the time from patient arrival to initial treatment, with a particular interest in examining variations across different hospital levels and regions within Indonesia. A thematic analysis was conducted in this study.
Results: The review included data from 1628 nurses across 13 provinces, highlighting significant variability in response times. Tertiary hospitals generally show faster response times than secondary hospitals. Key factors influencing response times included the demographic aspects of the nursing staff, work environment conditions, and the level of nurse training and education. Specific barriers such as inadequate infrastructure and cultural differences in healthcare-seeking behaviors also play a role.
Conclusion: There is a critical need for targeted improvements in hospital infrastructure and staff training programs to enhance response times across all hospital levels in Indonesia. Future policies should focus on equipping secondary healthcare services to efficiently meet emergency care demands.
Keywords: emergency department, emergency care, emergency nurse, healthcare infrastructure, intrahospital, nursing education, response time
Introduction
The number of mass casualty incidents (MCIs) has increased globally, leading to a significant increase in injuries. The number of cases of cerebrovascular disease and motor vehicle accidents in Indonesia, which are the main causes of early death and disability, is increasing.1 Concurrently, communicable diseases remain a major problem.2 In Indonesia, approximately 19.4% of all deaths are caused by strokes. It is higher than 10.5% in other high-income Asia-Pacific countries, and 9.8% in lower-middle-income countries in the region.1,3,4 To tackle these issues, the Indonesian government has increased its health budget to 5% of the total national expenditure, and now covers approximately 70% of the population with its national healthcare system.5 However, emergency care has not been a focus, and has been developing slowly.2 There are regulations for emergency departments (EDs), but no detailed studies have been conducted on how effective or well equipped these EDs are, particularly in terms of emergency response time.2
Nursing services are an essential part of healthcare. The ED serves as a critically important unit inside the hospital, acting as the primary entry point for managing emergency cases.6 Emergency department nurses are essential healthcare practitioners that significantly contribute to the triage process.7 Early identification of clinical decline and rapid mobilization of the rapid response team (RRT) are essential for enhancing patient outcomes, necessitating nurses to proactively initiate RRT activation upon the first signs of clinical deterioration.8 Previous studies have reported that the response time is low among nurses in a few hospitals in Indonesia. A delayed response time may negatively affect patient outcomes and is associated with a greater risk of ICU admission, hospital mortality, and overall healthcare quality.8,9
The response time as an emergency medical service (EMS) in the prehospital context is well documented. MCIs experienced pre-hospital delays exceeding two hours, with some delays lasting over eight hours.10 Prehospital emergency services in low- and middle-income countries (LMICs) suffer from poor funding and operational resources, including staffing issues.11,12 Additionally, challenges such as insufficient infrastructure and cultural differences in how people seek healthcare, communication, and coordination pose major obstacles to accessing EMS in these nations.13 However, studies have identified the pooled number of response times and comprehensively identified the factors associated with response time in Indonesia in the hospital setting, specifically in the ED.
While Indonesian literature on these topics is extensive, it lacks comprehensive analyses that delve into national and regional response times among nurses and the factors influencing them. The objective of this study was to estimate the response time and identify influencing factors among emergency nurses in Indonesian hospitals. This study aims to fill this gap by evaluating response times across Indonesia, mapping the factors that affect these times, providing a clearer picture of the state of emergency medical services, and identifying potential areas for improvement.
Methods
Study Design
This scoping review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension of the Scoping Reviews guidelines.14 This study aimed to review emergency nurse response times and related factors in hospital settings in Indonesia.
Search Strategy
We conducted a comprehensive search using keywords and Medical Subject Headings (MeSH) terms, focusing on ”emergency nursing”, ”response time”, ”Indonesia”, ”hospital emergency services”, ”nursing staff, hospital”, ”time factors”, and ”workload”.. The literature search included the PubMed/MEDLINE, CENTRAL/Cochrane, EBSCOhostt, and Google Scholar databases, covering studies published between 2019–2024. We did not conduct a manual search or search for reference lists. The detailed search strategy used for each database is provided in Supplementary File 1.
Eligibility Criteria
Using the Population, Concept, and Context (PCC) framework, the inclusion criteria were as follows: (1) studies focusing on the response times of nursing staff in Indonesian hospital emergency settings, where “response time” is defined as the average time from when a patient arrives at the treatment area after triage to when they receive initial treatment, with times of five minutes or less considered rapid and more than five minutes considered slow; (2) empirical research that quantitatively measures these response times; and (3) studies analyzing factors that affect these response times, published between 2019 and 2024. The exclusion criteria were as follows: (1) studies without accessible full texts; (2) non-empirical publications, such as reviews, editorials, and conference abstracts; and (3) studies not published in English or Bahasa Indonesia.
Data Collection and Analysis
Data extraction was independently conducted by two reviewers (DR and EMW), and discrepancies were resolved by consensus. The extracted information comprised (1) author(s) and publication year; (2) population details, including sample size and demographics; (3) study location and design; (4) specific response times recorded; and (5) factors identified as influencing these response times. We employed a thematic synthesis approach to amalgamate and interpret the findings from the included studies, organizing the data into key themes and categories relevant to our review objectives.
Results
Study Selection Results
The search initially yielded 1337 records from various sources, including PubMed (n = 523), Scopus (n = 32), EBSCOhost (n = 177), and Google Scholar (n = 605). Prior to screening, 17 duplicate records were removed, resulting in 1320 records for detailed screening. After excluding 1261 records for reasons that did not meet our criteria, 61 reports were identified for full retrieval. Of these, one report could not be retrieved. The remaining 60 studies were assessed for their eligibility. Exclusions at this stage included 11 reports where the full text was not available, 11 that were repository sources, one knowledge survey, one study where the sample in the analysis did not match, and one that focused on triage, leaving 35 studies included in the final review for both qualitative and quantitative analysis.15–49 Details of the study selection results are shown in Figure 1.
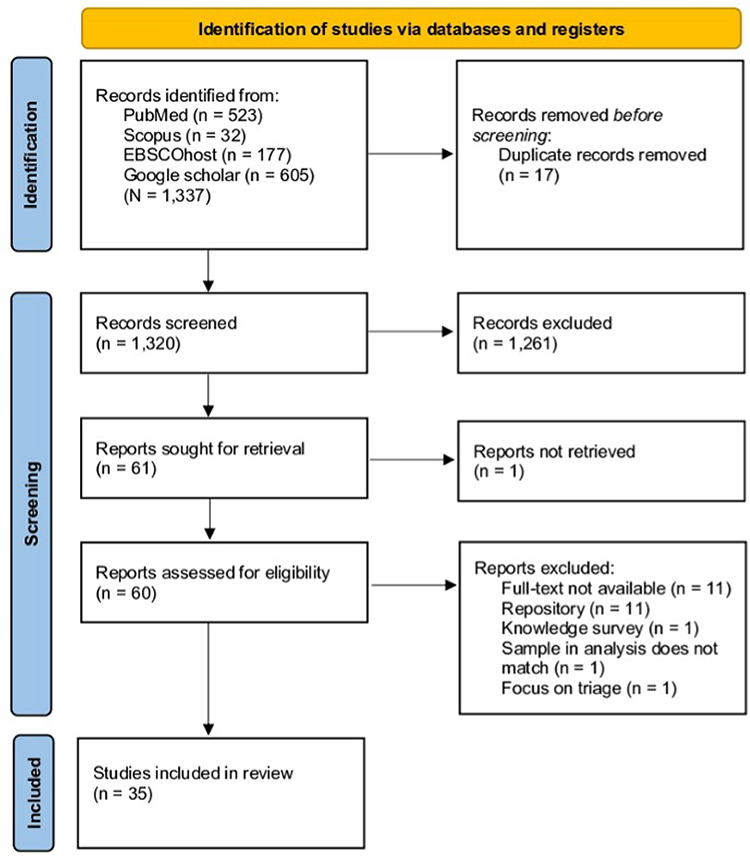 |
Figure 1 PRISMA flow diagram. Notes: Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372:n71. Creative Commons. |
Characteristic of Included Studies
This study included 1628 nurse participants across various levels of hospital services (A, B, C, D, and NA) from multiple provinces in Indonesia, reflecting the extensive geographical and healthcare setting diversity within the country. Most studies have utilized observational methods, although a significant number have relied on self-report instruments. The criteria for response times were largely consistent, with the majority defining fast response times as 5 min or less and slow as more than 5 min, which provides a uniform benchmark for assessing emergency response efficiency across studies. Moreover, the studies included data from 13 provinces representing both major islands and smaller archipelagos, thus offering a comprehensive snapshot of emergency care responsiveness across Indonesia. Among the hospitals studied, there were 8 hospitals classified as Level A (tertiary care), 15 as Level B, 12 as Level C, and 4 as Level D, indicating a varied level of resources and capabilities across the healthcare system. The characteristics of the included studies are presented in Table 1.
 |
Table 1 Characteristic of Included Studies |
Outcome of Included Studies
Rate of National and Regional Response Time in Emergency Department
East Java, leading to a fast response efficiency of approximately 93.69%. This is significantly higher than the national average of 66.24%. South Sumatra and Bengkulu also showed robust emergency service capabilities, with fast response rates of 85.00% and 84.85%, respectively, both well above the national average. In contrast, South Sulawesi reported the lowest percentage of fast responses (33.82%), substantially below the national threshold. The inclusion of the national average highlights that more than half of the provinces had fast response rates above the national average, demonstrating variability in emergency response efficiency across the country. These data underscore the importance of regional assessments and targeted interventions to enhance emergency care outcomes in Indonesia and to identify specific areas where improvements are needed to achieve more uniform standards of emergency care. Figure 2 depicts the distribution of fast and slow response times in emergency departments across various Indonesian provinces from 2019 to 2024.
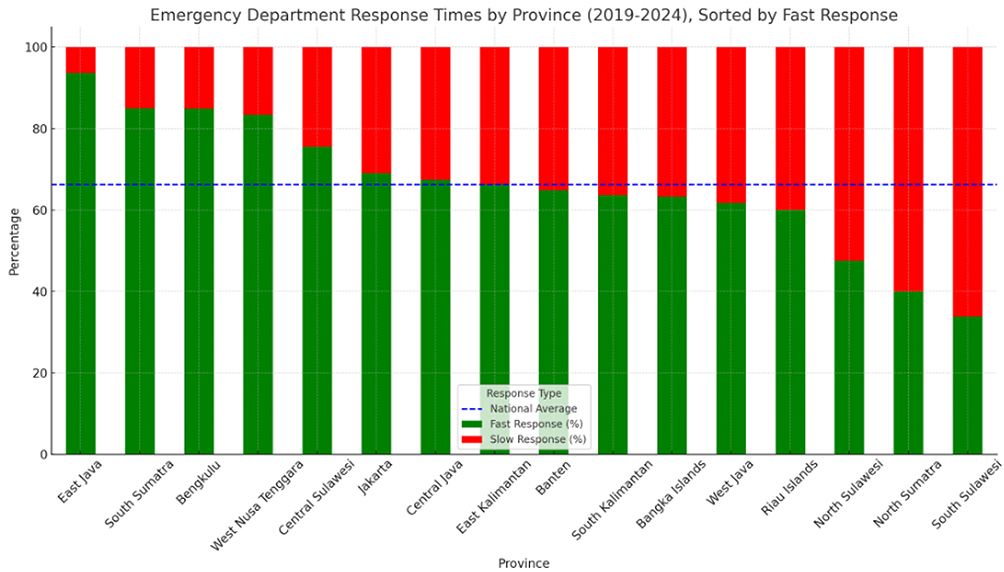 |
Figure 2 Emergency department response time by province (2019–2024). |
Response Time Based on Hospital Level
The analysis of emergency department response times in Indonesian hospitals revealed distinct patterns across different hospital levels (A, B, C, and D) and when aggregated into secondary and tertiary healthcare services. The Figure 3, which details response times by specific hospital levels, shows that Level A hospitals, classified as tertiary healthcare services, generally exhibit higher percentages of fast responses. This indicates their advanced capabilities and resources, which are characteristic of tertiary care facilities that handle more complex cases and have better infrastructure and staff. In contrast, Levels B, C, and D, grouped together as secondary healthcare services, show a combined performance that, while competitive, suggests greater variability in response efficiency.
 |
Figure 3 Response times by level of healthcare service in Indonesia. |
Figure 4 consolidates these findings by directly comparing the grouped secondary services with a singular tertiary level. This clearly illustrates that tertiary healthcare services outperform secondary services in terms of their fast response rates, highlighting the potential disparity in resource allocation and operational efficiency. This comparative analysis underscores the critical need for targeted improvements in secondary hospitals to improve their response capabilities and match those observed in tertiary institutions. Such enhancements are crucial for improving patient outcomes and ensuring that the quality of emergency care is uniform across hospitals in Indonesia.
 |
Figure 4 Response times by level of healthcare service (primary vs secondary level). |
Factor Associated with Response Time in the Emergency Department
In the following analysis, we explored six crucial factors that directly impact the response times in emergency departments. These factors encompass the demographic characteristics of healthcare providers, work environment conditions, professional training and knowledge, skill levels, clinical urgency of patients, and additional systemic variables. Each of these elements plays a distinct role in how quickly healthcare professionals react to emergencies, reflecting both individual capabilities and a broader operational context.
Demographic factors influencing response time included sex, age, and educational level. Male nurses often exhibited faster response times than female nurses.24 A younger age was associated with shorter response times.18 Nurses with a diploma (D3) responded faster than those with a bachelor’s degree (S1) did.24 Conversely, other studies indicate that bachelor’s degree nurses have quicker response times than diploma nurses do.18,46
The work environment factors affecting response times included facilities, workload, length of employment, and nurse-to-patient ratio. Adequate facilities support faster response times.41 A lighter workload allows quicker responses.16,17,19,21,23,26,28,36,41,42,45 Moreover, the length of employment also influences the speed of nurses’ responses to patients.19,21,23,24,28,33–37,46 Additionally, nurse-to-patient ratio was linked to the level of nurse responsiveness.
Adequate knowledge related to Basic Trauma Life Support (BTCLS), triage, and initial assessment is associated with quick nurse responses.32,37,38,40,43,49 Specialized training, such as BTCLS and Advanced Cardiac Life Support (ACLS), enhances response times.24,46
Greater skill proficiency contributed to faster response times.27,45 Patients with more critical conditions receive priority and respond quickly.26,35,44,45 Moreover, Proper use of the Emergency Severity Index (ESI) during the triage process accelerates response times.20
Discussion
This study represents the first scoping review of response times in intrahospital settings in Indonesia, shedding light on a critically under-explored area of emergency care. The findings indicate that the average national response time for emergency nurses is approximately 66.24%, with notable variations, such as East Java exhibiting exceptionally rapid response rates of 93.69%, while others, such as South Sulawesi, lag behind, with rates as low as 33.82%. Key factors identified include the demographic characteristics of nursing staff, such as age and education level, as well as work environment conditions, such as facility adequacy and workload. These variations are influenced by several critical factors identified in our findings: (1) demographic characteristics of the nursing staff (such as age and gender), (2) educational attainment and the extent of professional training, (3) environmental factors such as the adequacy of hospital facilities and workload intensity, (4) clinical and emergency level of the patient, and (5) skills development.
Despite the significant strides in emergency care in Indonesia, this study revealed a concerning national average rapid response rate of only 66.24%, indicating that a substantial portion of emergency responses fall short of the desired speed. Such delays in response times are not merely statistical concerns but also have profound implications for clinical outcomes. Slow response times in emergency situations can drastically affect patient survival rates and likelihood of recovery without long-term disability. In acute medical conditions such as strokes, heart attacks, and trauma, the principle of “time is tissue” underscores the urgency; delays can lead to irreversible damage, significantly increasing the risk of mortality and morbidity (Hui et al, 2024; Sachdeva et al, 2023; Chhabra et al, 2022).50–52 The suboptimal response rate highlighted by this study could contribute to higher rates of fatality and disability following emergencies, particularly in regions with slowest response times. This is particularly critical in areas such as South Sulawesi, where response rates are markedly below the national average. Delayed intervention in these cases likely exacerbates patient outcomes, leading to an increased burden of care post-emergency, higher healthcare costs, and greater strain on healthcare resources and families.53,54
The importance of continuous education and training to improve response times in medical emergency services cannot be overstated. Educational initiatives and ongoing training programs are pivotal for equipping healthcare professionals, especially emergency nurses, with the skills necessary to respond efficiently and effectively to emergencies.55 This is crucial not only for enhancing the speed of response but also for improving the overall quality of care provided to patients. Continuing education and targeted training programs help bridge gaps in the knowledge and skills of healthcare staff. Advanced training in specific emergency care protocols, such as Advanced Cardiac Life Support (ACLS) and Basic Life Support (BLS), has been shown to improve outcomes in critical care situations.56,57
The findings of this study have significant implications for clinical practice and health policy in Indonesia. For practitioners, variability in response times highlights the necessity for continuous training and adherence to standardized protocols. Emergency departments should focus on refining triage procedures and optimizing nurse-to-patient ratios to facilitate quicker response times. Implementing routine drills and simulation exercises could also enhance nurses’ ability to manage patients under pressure efficiently. This review highlights the urgent need for policymakers to enhance infrastructure and resource allocation in emergency services. Policies should aim to improve the availability of essential medical equipment and ensure that emergency departments are adequately staffed and equipped to handle peak loads. Moreover, establishing clear benchmarks for response times based on international standards and monitoring compliance through regular audits could help to maintain high levels of care. Policymakers should also consider incentivizing hospitals to consistently meet or exceed these benchmarks to encourage improvements across the board. Finally, fostering a culture of continuous professional development and learning in hospital settings can empower nurses and other health care professionals to deliver prompt and effective care. By addressing these practices and policy issues, health care leaders in Indonesia can significantly enhance the efficiency and quality of emergency responses, ultimately improving patient outcomes in critical care settings.
This study had several limitations that may affect the generalizability and robustness of the findings. First, none of the included studies was sourced from reputed journals, which may have affected the reliability of the reported data. Additionally, there was considerable inconsistency in the standards of response time across studies, which could complicate the synthesis of data and lead to variations in the interpretation of the response efficiencies. A significant number of studies relied on self-report methods rather than direct observation, introducing potential bias and questioning the accuracy of the response times reported. A limited database was included, and the small sample sizes of several studies further limit the generalizability of the findings across broader populations. Furthermore, the absence of a clear theoretical framework underpinning this research may weaken the depth of analysis and interpretation of the results. Finally, the review is restricted to studies published between 2019 and 2024, which may not fully represent emergency response practices across all Indonesian provinces, potentially overlooking regional disparities and developments prior to 2019.
Conclusion
The study concluded that the national average rapid response rate of emergency nurses in Indonesian hospitals was 66.24%, demonstrating significant regional variations. East Java resulted in a relatively high response rate of 93.69%, whereas South Sulawesi demonstrated a relatively low rate of 33.82%. Response times were influenced by the demographic attributes of nursing personnel (including age, gender, and educational attainment), environmental factors (such as hospital infrastructure and task intensity), and the degree of professional education and training.
These findings emphasize the need for focused measures to enhance the response times at all hospital levels. In clinical practice, ongoing professional development and specialized emergency training programs are crucial for equipping nurses with the skills necessary for a rapid and efficient response. Hospitals should prioritize optimizing nurse-to-patient ratios and improving triage procedures to increase their response efficiency. From a policy standpoint, it is imperative to invest in the hospital infrastructure, assign sufficient resources, and establish defined targets for response times in accordance with internationally accepted standards. Policies need to encourage hospitals to reach or exceed these goals and underscore the necessity of regular audits to ensure compliance. By emphasizing these areas, healthcare leaders in Indonesia may substantially enhance emergency response capabilities, thereby decreasing patient mortality and morbidity, and improving overall healthcare quality.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sari EF, Johnson NW, McCullough MJ, Cirillo N. Global Burden of Disease Data for Indonesia. Lancet Glob Health. 2023;11(3):e336. doi:10.1016/S2214-109X(23)00004-9
2. Yusvirazi L, Sulistio S, Wijaya Ramlan AA, Camargo Jr CA Jr. Snapshot of emergency departments in Jakarta, Indonesia. Emerg Med Australasia. 2020;32(5):830–839. doi:10.1111/1742-6723.13570
3. Brice SN, Boutilier JJ, Gartner D, et al. Emergency services utilization in Jakarta (Indonesia): a cross-sectional study of patients attending hospital emergency departments. BMC Health Serv Res. 2022;22(1). doi:10.1186/s12913-022-08061-8
4. GBD. Global Burden of Disease 2021 Findings from the GBD 2021 Study; 2021.
5. Agustina R, Dartanto T, Sitompul R, et al. Universal health coverage in Indonesia: concept, progress, and challenges. Lancet. 2019;393(10166):75–102. doi:10.1016/S0140-6736(18)31647-7
6. Tartila DYR, Wahyudi AS, Qona’ah A. Determinant of Nurses’ Response Time in Emergency Department When Taking Care of A Patient. Indonesian Nurs J Edu Clin. 2020;5(2):125. doi:10.24990/injec.v5i2.305
7. Mulyadi M, Dedi B, Hou W, Huang I, Lee B. Nurses’ experiences of emergency department triage during the COVID‐19 pandemic in Indonesia. J Nurs Scholarsh. 2022;54(1):15–23. doi:10.1111/jnu.12709
8. Tilley M, Spencer K. Perceived Barriers to Rapid Response Team Activation Among Nurses. AJN, Ame J Nurs. 2020;120(7):52–60. doi:10.1097/01.NAJ.0000688220.05900.7c
9. McIntyre D, Chow CK. Waiting Time as an Indicator for Health Services Under Strain: a Narrative Review. Inquiry. 2020;57. doi:10.1177/0046958020910305
10. Alruqi F, Aglago EK, Cole E, Brohi K. Factors Associated with Delayed Pre-Hospital Times during Trauma-Related Mass Casualty Incidents: a Systematic Review. Dis Med Public Health Prep. 2023;17(2). doi:10.1017/dmp.2023.187
11. Hooper C, Ranse J, Hutton A. How is ambulance patient care and response time data collected and reported in Malaysia and Indonesia? Austr J Paramed. 2019;16:1–8. doi:10.33151/ajp.16.683
12. Obermeyer Z, Abujaber S, Makar M, et al. Emergency care in 59 low- and middle-income countries: a systematic review. Bull World Health Organ. 2015;93(8):577–586. doi:10.2471/BLT.14.148338
13. Kironji AG, Hodkinson P, De Ramirez SS, et al. Identifying barriers for out of hospital emergency care in low and low-middle income countries: a systematic review. BMC Health Serv Res. 2018;18(1). doi:10.1186/s12913-018-3091-0
14. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
15. Farilya M, Alfian A, Sulahsuningsih E, Syahril S. Pengaruh Penerapan ESI (Emergency Severity Index) Terhadap Response Time Triage di Instalasi Gawat Darurat RSUD Sumbawa. J Riset Kajian Teknologi Lingkungan. Indonesian. 2023;6(2):172–181.
16. Wahyuni S, Latjui SA. Hubungan Beban Kerja Perawat dengan Response Time Perawat di Instalasi Gawat Darurat RSUD Bitung. J Sisthana. Indonesian. 2020;2(1):1–5.
17. Dareda K, Yahya IM, Cawangi P. Hubungan Beban Kerja Dengan Waktu Tanggap Perawat di Instalasi Gawat Darurat RSUD. M.W. Marawis Minahasa Utara. J Ilmu Kedokteran Dan Kesehatan Indonesia. Indonesian. 2021;1(3):84–90.
18. Ra’uf M, Analysis of Factors That Related To Respond Time and Treating Emergency Patients In Banjarmasin Regional Public Hospital. Health Media. 2021;3(1):28–38. doi:10.55756/hm.v3i1.80
19. Nurzaman A, Windiyaningsih C, Hubungan Antara Kompetensi WS, Kerja B. Dan Masa Kerja Dengan Waktu Tanggap Perawat Di Instalasi Gawat Darurat Rumah Sakit Medirossa Cikarang. J Manajemen Dan Administrasi Rumah Sakit Indonesia. Indonesian. 2021;5(1):108–14.
20. Bahari ZK, Agina P, Suwaryo W, Setyaningsih E. Penerapan ESI (Emergency Severity Index) Terhadap Response Time Pasien di IGD PKU Muhammadiyah Gombong. In: The 10th University Research Colloquium 2019. 2019:307–319.
21. Bahriadi M, Garming AL, Firdaus R. The Relationship between Workload and Working Period with Nurse Response Time in Patient Handling at the Emergency Room of RSUD Dr. Abdul Rivai. Formosa J Multidiscip Res. 2023;2(5):887–894. doi:10.55927/fjmr.v2i5.4030
22. Fernalia F, Pawaliyah P, Trianingsih K. The Relationship of Knowledge and Long Work to Emergency Team Response Time in Emergency Installations Emergency (ER) RSUD Dr. M. YunusvCity of Bengkulu. J Kesehatan Medika Saintika. Indonesian. 2023;14(1). doi:10.30633/jkms.v14i1.1914
23. Karokaro TM, Hayati K, Sitepu SDEU, Sitepu AL. Faktor – faktor Yang Berhubungan Dengan Waktu Tanggap (Response Time) Pasien di Instalasi Gawat Darurat Rumah Sakit Grandmed. J Keperawatan Dan Fisioterapi. Indonesian. 2020;2(2):172–180. doi:10.35451/jkf.v2i2.356
24. Fathia NA, Kurdaningsih SV. Karakteristik Perawat Terhadap Waktu Tanggap dalam Penanganan Kegawatan Pasien di Instalasi Gawat Darurat. J ‘Aisyiyah Medika. 2022;7(2):89–98.
25. Rachma S, Hidayat E, Situmorang BHL. Efektivitas Penerapan ESI (Emergency Severity Index) Terhadap Response Time Triage di Instalasi Gawat Darurat RSUD Undata Provinsi Sulawesi Tengah. J Kesehatan Tambusai. 2023;4(3):4278–4280.
26. Darma E, Windiyaningsih C, Lutfie SH. Pengaruh Pengantar Pasien, Kondisi Pasien, Dan Beban Kerja Tenaga Kesehatan IGD Terhadap Waktu Tanggap Di IGD RSIA Bunda Aliyah Jakarta Tahun 2020. J Manajemen Dan Administrasi Rumah Sakit Indonesia. 2021;5(1):50–60 Indonesian.
27. Rumampuk JF, Katuuk ME. Hubungan Ketepatan Triase Dengan Response Time Perawat di Instalasi Gawat Darurat Rumah Sakit Tipe C. E-Journal Keperawatan. 2019;7(1):1. Indonesian.
28. Ramadani KF, Satriana A. Faktor-Faktor Yang Berhubungan dengan Waktu Tanggap (Response Time) Pasien di Instalasi Gawat Darurat di RSUD Tenriawaru Kabupaten Bone. J Keperawatan Lapatau. 2021;1(1):23–35. Indonesian.
29. Rossy M, Ilmi B, Hiryadi H. Analisis Faktor yang Berhubungan dengan response time Perawat dalam Melakukan Triage di Instalasi Gawat Darurat. J Kesmas Asclepius. 2023;5(2):209–223. Indonesian. doi:10.31539/jka.v5i2.7648
30. Afifah R, Wreksagung H, Sari RP, Tangerang SY. Relationship of nurse workload with response time in handling of patients in ER (emergency room) general hospital of Tangerang Regency in 2021. Nusantara Hasana Journal. 2022;1(9):35–40.
31. Bintang A, megawati M, Madamang I. Hubungan Tingkat Pengetahuan Perawat Dengan Response Time Instalasi Gawat Darurat RS Dr.M.Yasin Bone. Journal Keperawatan Lapatau. 2021;2021:1. Indonesian.
32. Afrina L, Kusumajaya H, Meilando Program Studi Ilmu Keperawatan R, et al. Faktor Faktor Yang Berhubungan dengan Response Time Perawat pada Kasus Kecelakaan Lalu Lintas di IGD. J Penelitian Perawat Profesional. 2023;5(2):645–656.
33. Marota SJ, Muzakkir M, Sabil FA. Hubungan Beban Kerja Perawat Dengan Waktu Tanggap Darurat Di Ruangan Instalasi Gawat Darurat Rumah Sakit Bhayangkara. JIMPK. 2024;4(2):152–6. Indonesian. doi:10.35892/jimpk.v4i2.1431
34. Surani W, Pujianto A, Artikel I. Faktor-Faktor yang Berhubungan dengan response time Tenaga Kesehatan di Ruang Instalasi Gawat Darurat (IGD). Pena Nursing. 2023;1:1–14. Indonesian.
35. Norhidayat M, Hamzah H, Hubungan Pelatihan SS. Lama Kerja dan Kondisi Pasien dengan response Time Perawat di Instalasi Gawat Darurat. J Kesmas Asclepius. 2023;5(2):176–182. Indonesian. doi:10.31539/jka.v5i2.7700
36. Kodja A, Syahrir S. Beban Kerja Perawat Dengan Response Time Pada Penanganan Pasien di Instalasi Gawat Darurat. ASHOLISCARE Journal. 2024;1(2):10–18.
37. Yulia R, Hubungan Lama Kerja dan Pelatihan dengan Ketepatan Waktu Tanggap Penanganan Pasien Di IGD RSHB Batam. Ahmar Metastasis Health J. 2022;2(3):166–173. Indonesian. doi:10.53770/amhj.v2i3.142
38. Nursanti DMY, Dinaryanti RS. Hubungan Tingkat Pengetahuan Tentang Triage dengan Pelaksanaan Respon Time Perawat Dalam Pelaksanaan Triage di IGD Rumah Sakit Dr Suyoto. J Ilmiah Keperawatan. 2022;8(1):193–199. Indonesian.
39. Cahyono A, Siswoyo S, A’la MZ. Hubungan beban kerja dengan response time perawat instalasi gawat darurat (IGD) pada rumah sakit tipe C Di Kabupaten Jember. Pustaka Kesehatan. 2020;8:183. Indonesian. doi:10.19184/pk.v8i3.12724
40. Yustilawati E, Pramana Putra A. The relationship of nurse’s knowledge about BTCLS with response time at the IGD RS Bhayangkara Makassar. J Media Keperawatan. 2023;14(1):2087–2122.
41. Herawati T, Djubaedah S, Hardiyanti A. Faktor-Faktor yang berhubungan dengan lamanya waktu tanggap (Response Time) Perawat di IGD RSUD DR. Chasbullah Abdulmadjid Kota Bekasi. J Kesehatan Masyarakat Perkotaan. 2022;2:59–71. Indonesian. doi:10.37012/jkmp.v2i2.1556
42. Muti RT, Dwilingga Z. Relationship between workload with response time at nurses Er IGD RSI Banjarnegara. Menara Journal of Health Science. 2023;2(2):265–275.
43. Ramadhan MF, Wiryansyah OA, Ari Wiryansyah O. Hubungan tingkat pengetahuan perawat tentang response time dalam menentukan triase diruang igd. J Kesehatan Dan Pembangunan. 2020;10(19):56–62. Indonesian. doi:10.52047/jkp.v10i19.61
44. Sutriningsih A, Ardiyani VM. Faktor yang berhubungan dengan ketepatan waktu tanggap (response time) Perawat Di IGD RSUD Bangil. J NursCare Biomol. 2023;8(2):1–9. Indonesian.
45. Silitonga JM, Anugrahwati R. The factors related to nurse time response to COVID 19 suspect patients in Hermina Jatinegara Hospital IGD: respon time Perawat Pada Pasien Suspek COVID 19. J Ilmiah Keperawatan Altruistik. 2021,4;4:20–26. doi:10.48079/Vol4.Iss1.67
46. Rochani S Correlation Between Level of Education and Years of Service to the Nurse Respond Time in Emergency Instalation of RSUD Dr. Adjidarmo Rangkasbitung 221 | JKSP 2021 4. doi:10.32524/jksp.v4i2.269
47. Wiyadi W, Rahman G, Analisis faktor yang berhubungan dengan waktu tanggap pada pasien gawat darurat di instalasi gawat darurat (IGD) RSUD A. Wahab sjahranie samarinda. Husada Mahakam. 2020;10:1. Indonesian.
48. Khotimah HH, Jundiah RS, Muliani R, Megawati S, Efek fatigue terhadap respon time penanganan penderita gawat darurat kategori australasian triage scale 1-5 versi indonesia. Faletehan Health J. 2022;9(2):209–219. Indonesian. doi:10.33746/fhj.v9i02.433
49. Khairari ND. The initial assessment of nurse knowledge to response time in traffic accident case. Media Keperawatan Indonesia. 2021;4(2):127. doi:10.26714/mki.4.2.2021.127-132
50. Sachdeva P, Kaur K, Fatima S, et al. Advancements in myocardial infarction management: exploring novel approaches and strategies. Cureus. 2023;15:1. doi:10.7759/cureus.45578
51. Hui C, Tadi P, Khan Suheb MZ, Patti L Ischemic Stroke. StatPearls. 2024.
52. Chhabra HS, Sharawat R, Vishwakarma G. In-hospital mortality in people with complete acute traumatic spinal cord injury at a tertiary care center in India—a retrospective analysis. Spinal Cord. 2022;60(3):210–215. doi:10.1038/s41393-021-00657-x
53. Shere-Wolfe RF, Galvagno SM, Grissom TE. Critical care considerations in the management of the trauma patient following initial resuscitation. Scand J Trauma Resusc Emerg Med. 2012;20:20. doi:10.1186/1757-7241-20-68
54. Rasouli HR, Aliakbar Esfahani A, Abbasi Farajzadeh M. Challenges, consequences, and lessons for way-outs to emergencies at hospitals: a systematic review study. BMC Emerg Med. 2019;19(1):62. doi:10.1186/s12873-019-0275-9
55. Proehl JA. Developing Emergency Nursing Competence. Nurs Clin North Ame. 2002;37(1):89–96. doi:10.1016/S0029-6465(03)00085-9
56. Sodhi K, Singla M, Shrivastava A. Impact of advanced cardiac life support training program on the outcome of cardiopulmonary resuscitation in a tertiary care hospital. Indian J Crit Care Med. 2011;15(4):209–212. doi:10.4103/0972-5229.92070
57. Pareek M, Parmar V, Badheka J, Lodh N. Study of the impact of training of registered nurses in cardiopulmonary resuscitation in a tertiary care centre on patient mortality. Indian J Anaesth. 2018;62(5):381–384. doi:10.4103/ija.IJA_17_18
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.