")
Back to Journals » Clinical Ophthalmology » Volume 19
Resveratrol Supplementation in Wet AMD: Association With Fewer Intravitreal Injections and Reduced Macular Fibrosis
Authors Datseris I, Rouvas A, Tzanidaki ME, Kardara M, Geros V, Gouliopoulos N
Received 2 October 2024
Accepted for publication 13 January 2025
Published 21 January 2025 Volume 2025:19 Pages 217—225
DOI https://doi.org/10.2147/OPTH.S494595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ioannis Datseris,1 Alexandros Rouvas,2 Malvina-Efthymia Tzanidaki,1 Marina Kardara,1 Vasileios Geros,2 Nikolaos Gouliopoulos2
1Ophthalmology Department, Ophthalmological Institute “OMMA”, Athens, Greece; 2 2nd Department of Ophthalmology, Medical School of University of Athens, “attikon” University Hospital, Athens, Greece
Correspondence: Ioannis Datseris, Ophthalmological Institute OMMA, Katehaki 74, Athens, 11525, Greece, Tel +302106755850, Fax +302106755851, Email [email protected]
Purpose: To evaluate the 2-year outcomes of resveratrol oral supplement given as an adjunctive treatment in patients with wet age-related macular degeneration (AMD) that were treated with intravitreal injections of aflibercept.
Patients and Methods: In our retrospective study, 50 treatment-naïve patients suffering from wet-AMD were included. They were assigned to two subgroups of 25 patients each. Every participant was treated according to “Pro Re Nata” protocol; 3 monthly intravitreal injections of 2.0 mg aflibercept were applied followed by injections according to need. The patients in the second group also consumed daily two tablets of resveratrol enriched oral supplement (60 mg of resveratrol in total). For 2 years, the patients were monthly assessed with best corrected visual acuity (BCVA) measurement, fundus autofluorescence, optical coherence tomography (OCT) scans and OCT-angiography. The main endpoints were the change of BCVA, the number of anti-VEGF injections, the change of central foveal thickness values, and the expansion or new development of fibrosis.
Results: Between the studied groups, no significant differences were detected in the baseline demographic and clinical data (p> 0.05 for all). Over the 24-month study period, both BCVA and central foveal thickness values did not differ significantly between the two groups. As for the number of applied injections, they were significantly fewer in the group of patients that were treated with the resveratrol supplement (9.32± 1.37 vs 7.40± 1.88, p< 0.001). Notably, the frequency of fibrosis progression was significantly lower in the resveratrol group (p=0.04).
Conclusion: In conclusion, our findings suggest that resveratrol oral supplement could be considered as a useful adjunctive aid to the established treatment in cases suffering from wet AMD, highlighting the superiority of the combination treatment regimen, since it was accompanied by lower rates of both intravitreal aflibercept injections and progression of macular fibrosis.
Keywords: wet AMD, Resvega, resveratrol, aflibercept, macular fibrosis, food supplement
Introduction
Age-related macular degeneration (AMD) is a progressive, degenerative, multifactorial disease, being the leading cause of irreversible vision impairment and even blindness in older adults in the Western world.1,2 AMD can be divided into two main categories: nonexudative or dry and neovascular or exudative or wet.3 Dry AMD is classified as early, intermediate and late when geographic atrophy is present, while wet AMD is always classified as late AMD.
Wet AMD represents the advanced stages of the disease and is characterized by the development of a choroidal neovascularization (CNV),4,5 which initiates from the choroidal vasculature and extends to the subretinal space, through Bruch’s membrane and the retinal pigment epithelium (RPE).4 The abnormal new vessels are prone to leakage and bleeding, leading to the accumulation of subretinal fluid (SRF) and/or intraretinal fluid (IRF), and in the development of intraretinal, subretinal, or subRPE hemorrhage.6,7 CNVs (either treated or not) gradually transform from a neovascular membrane to a mixed tissue consisting of both active and inactive choroidal fibrovascular tissues resulting in the development of subretinal fibrosis.4 Therefore, an irreversible damage occurs to the photoreceptors and the RPE, which is accompanied by a severe and rapid vision loss,8 and a downgrade of the patients’ quality of life.7,9,10 Treatments aim to control CNV and prevent further damage, but the degenerative nature of the disease poses a constant threat to vision.
Vascular endothelial growth factor (VEGF) has a critical role in the pathogenesis of wet AMD, particularly in the development of CNV and the persistence of exudation.11,12 The administration of anti-VEGF agents intravitreally is pivotal in cases of wet AMD.13,14 Despite their undoubtful significant beneficial effects, their efficacy is occasionally suboptimal in preventing visual decline mainly due to the development of subretinal fibrosis, which occurs in almost half of the eyes even with ongoing application of anti-VEGF agents.15
Resveratrol (RSV) is a stilbenoid polyphenolic phytoalexin that can be found in several fruits and seeds but mainly in grapes, berries, and peanuts.16–22 It has antidiabetic, anticancer, cardioprotective, anti-inflammatory, antioxidant, and antiangiogenic properties via the activation of sirtuin-1.17–23 Several studies have suggested that RSV has a protective effect on RPE cells through the local inhibition of inflammation and oxidation, while it prevents the cell apoptosis and suppresses the expression of VEGF,16–21,24 indicating a possible favorable effect in cases of wet AMD.7,16–25 Moreover, it has been identified a favorable effect of RSV in improving contrast sensitivity through an improvement in retinal remodeling via many pathways that include decreased lipofuscin accumulation, increased choroidal perfusion, and increased macular pigment volume.26
Resvega® (Laboratoires Thea/Clermont-Ferrand, France) is a novel oral supplement, containing RSV (30 mg), omega-3 fatty acids (665 mg), lutein (10 mg), zeaxanthin crystalline (2 mg), vitamins C (120 mg), E (30 mg), and D (5 μg), zinc (12.5 mg), and copper (1 mg). Recent studies have demonstrated that daily oral intake of Resvega capsules results in improved retinal structure and visual function in eyes suffering from wet AMD.7,27,28
In previous research, we demonstrated that the complementary intake of Resvega by patients with wet AMD managed with intravitreal injections of aflibercept (IAIs) led to notable improvements in contrast sensitivity and overall quality of life (QoL) over a 12-month period.7 However, this supplementation did not significantly affect best-corrected visual acuity (BCVA) or reduce the number of IAIs.7
In light of the aforementioned points, we have now assessed the 2-year outcomes of Resvega supplementation combined with IAIs, comparing it with IAIs as monotherapy, in a separate population of patients. The aim of this study was to examine whether the daily intake of Resvega as an adjunctive treatment would have a favorable anatomical and functional effect in patients suffering from wet AMD. To the best of our knowledge, no prior studies have examined the extended effects of Resvega in this context, making our investigation unique in the existing literature.
Materials and Methods
This is a retrospective, interventional, monocentric, comparative study that took place at the Ophthalmological Institute “OMMA”, Athens, Greece. Fifty treatment-naïve patients suffering with wet AMD were assigned to two age- and sex-matched groups, each consisting of 25 subjects. The patients in the first group received three monthly intravitreal injections of 2.0 mg aflibercept (Eylea, Bayer Healthcare, Germany); afterwards, a pro re nata (PRN) treatment regimen was applied and injections were administered as needed based on clinical findings (“Eylea” group).29–31 The decision for reinjection was guided by optical coherence tomography (OCT) results, with criteria including the presence of SRF, IRF, and/or an increase in the height of retinal pigment epithelium (RPE) detachment (PED) The second group followed the same treatment modality, along with the daily consumption of two tablets of Resvega oral supplement (60 mg of resveratrol daily) (“Eylea & Resvega” group). Intravitreal injections were performed under standard sterile conditions, while topical antibiotics were applied 4 times per day for 2 days after the injection.32 The study followed the tenets of the Helsinki Declaration and was approved by the ethical committee of the Ophthalmological Institute “OMMA” (Protocol number:62, Date: 10/01/2022). Risks and benefits were thoroughly explained, and written informed consent was obtained from every participant.
All the patients underwent a complete ocular baseline examination, including evaluation of best-corrected visual acuity (BCVA), funduscopy, OCT (SPECTRALIS, Heidelberg Engineering, Heidelberg, Germany), fundus autofluorescence (FAF), fluorescein angiography, indocyanine green angiography, and OCT angiography (OCT-A) (Optovue, Inc., Freemont, CA). The participants were evaluated monthly for the next 24 months. At every examination, BCVA was measured, while FAF, OCT, and OCT-A were performed. OCT scans allow early detection as well as the evaluation of the volume and extent of fibrosis, which is defined as compact hyperreflective material beneath the neurosensory retina or the RPE accompanied by the degeneration of photoreceptors and RPE cells.33,34 Furthermore, central foveal thickness (CFT) was measured via OCT.
Patients that were previously treated for wet AMD were excluded from the study. Further exclusion criteria included the presence of any other macular disorders, like polypoidal choroidal vasculopathy, retinal angiomatous proliferation, diabetic retinopathy, and CNV secondary to any other disorder except for wet AMD.
Reinjections were applied according to the criteria we described above. No significant differences in patients’ visit intervals were present between the studied groups. The main endpoint outcomes included BCVA change, the number of anti-VEGF injections, the CFT change, and the expansion or new onset of fibrosis. “Expansion” was defined as the enlargement of already established fibrosis, by measuring the extension of the hyperreflective area on OCT. “Development” was defined as the detection of new onset fibrosis that was absent in previous examinations. “Progression” was defined as either “expansion” or “development” of fibrosis.
All variables were tested for a normal distribution with the Kolmogorov‒Smirnov test. Normally distributed data are expressed as the means ± standard deviations. Comparisons of mean values between groups for continuous and normally distributed variables were performed with Student’s t test, whereas nonparametric data were tested with the Mann‒Whitney U-test. BCVA values, evaluated by Snellen charts (measured in decimals), were converted to a logarithm of the minimum angle of resolution (logMAR) scale for statistical purposes. A paired sample t test was used to test intra- and inter-group differences between the means of logMAR BCVA and CFT. P values <0.05 indicated statistical significance. The statistical calculations were performed using SPSS software (version 20.0; SPSS, Chicago, IL).
Results
In Table 1 are presented the participants’ demographic and baseline clinical characteristics. No significant differences existed between the studied groups in terms of the mean age or sex status (p>0.05 for both). Moreover, we did not identify any significant differences between the baseline values of BCVA, CFT, or the frequency of established fibrosis (p>0.05 for all).
 |
Table 1 Demographic and Baseline Clinical Characteristics of the Participants |
The outcomes for both treatment regimens, as summarized in Table 2, show that after the completion of our study, no significant differences were detected between the two groups in terms of mean logMAR BCVA or mean CFT values between the groups (p>0.05). Additionally, the mean changes in logMAR BCVA and CFT during the study period did not differ significantly at any stage between the two groups (Table 3). However, despite the lack of significant differences between the two groups, both treatment regimens achieved a statistically significant improvement from baseline in logMAR BCVA (−0.10±0.17, p=0.007 for “Eylea” and −0.07±0.16, p=0.03 for “Eylea & Resvega”) and CFT values (−64.00±20.21 μm, p<0.001 for “Eylea” and −62.80±38.46 μm p<0.001 for “Eylea & Resvega”).
 |
Table 2 Clinical Outcomes of Treatment Regimens |
 |
Table 3 Changes From Baseline Values According to the Applied Treatment |
With respect to the number of applied IAIs, the patients in the “Eylea & Resvega” group required significantly fewer injections throughout the 24-month period (9.32±1.38 vs 7.40±1.87, p<0.001). It is noteworthy that at 12 months, the number of IAIs did not differ significantly (5.60±1.00 vs 5.16±0.85, p=0.10), whereas a significant difference was first noted at 18 months (7.68±1.11 vs 6.48±1.56, p=0.003) in favor of the “Eylea & Resvega” group (Figure 1). Interestingly, the frequency of both “progression” and “expansion” fibrosis was significantly greater in the “Eylea” group (p=0.04 for both), whereas the rate of “development” fibrosis did not differ significantly between the studied groups (p=0.33) (Figure 2). Notably, no cases of fibrosis development or enlargement were identified among the patients of the “Eylea & Resvega” group.
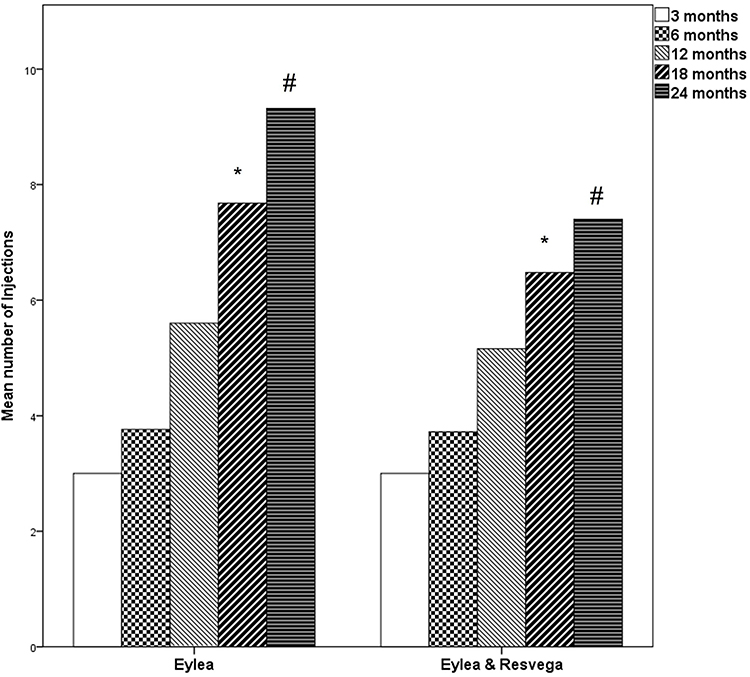 |
Figure 1 Bars representing the differences in mean number of intravitreal aflibercept injections between the “Eylea” and “Eylea & Resvega” group at 3, 6, 12, 18, and 24 months. |
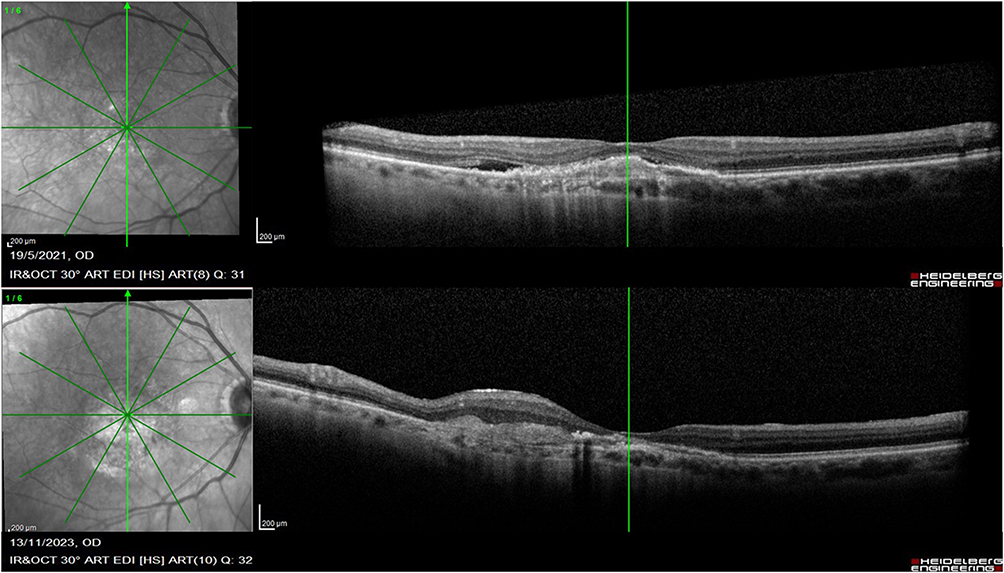 |
Figure 2 Optical coherence tomography scans of patient that was treated with intravitreal injections of aflibercept as a monotherapy, that experienced an expansion of fibrosis. |
Discussion
The main finding of our study is that in cases of wet AMD, the daily intake of Resvega along with the established treatment of IAIs is associated with significantly fewer IAIs in the 24-month study period. Furthermore, the addition of the aforementioned food supplement was related to significantly lower rates of “fibrosis progression” compared to patients who were treated with IAIs alone, suggesting that Resvega may have a protective role in reducing the development of subretinal fibrosis in wet AMD patients. However, its consumption did not lead to further functional and/or anatomical improvements, as they are expressed by the means of BCVA and CFT.
The application of intravitreal injections of anti-VEGF agents is currently the gold standard treatment for eyes suffering from wet AMD.5 They exert their biological action by blocking the activation of the VEGF downstream pathway; thus, they suppress CNV growth and activity, ameliorating the exudative phenomena and improving visual acuity.5,35 Among anti-VEGF agents, aflibercept is a recombinant fusion protein that binds to all isomers of the VEGF-A and VEGF-B families and to the placental growth factor (PGF).36,37 Aflibercept has gained ground as a first option treatment in cases of wet AMD since it has a longer duration compared to ranibizumab, resulting in fewer injections.38 Despite this, the frequency of recurrent episodes is relatively high, requiring a relatively high number of injections.39 It should be underlined that recurrences have a deleterious effect on visual acuity due to the higher frequency of fibrosis development.30 Moreover, a greater number of intravitreal injections per se has been recognized as a significant risk factor for the development of fibrosis,40 while their psychological and economic burden for the patients is extremely higher.7 Therefore, it is of great importance to identify therapeutic options that would minimize recurrences and the concomitant number of injections, as well as the frequency and extend of fibrosis.
The role of RSV as an adjunctive treatment in cases of wet AMD has attracted attention recently.7,22,26 In our study, the intake of Resvega, an RSV and omega-3 fatty acid-enriched oral supplement, was associated with significantly fewer IAIs (almost 2) over the 24-month study period. A plausible examination of our findings is that RSV in retinal cells can suppress VEGF-A and -C secretion induced by inflammatory cytokines, transforming growth factor-β (TGF-β), and hypoxia through disruption of the PI3K-AKT-mTOR signaling axis and NF-κB pathways.17,26 The aforementioned mechanisms have been associated with a prolonged antiangiogenic effect of bevacizumab.26 It could be hypothesized that RSV may similarly enhance the action of aflibercept, extending the treatment intervals and decreasing as a result the number of the required IAIs. In accordance with our findings, in a previous study conducted in a cohort of patients suffering from diabetic macular edema, Resvega intake was followed by significantly fewer intravitreal injections of anti-VEGF agents over a 12-month period.41 In contrast, we have previously shown that Resvega did not affect the number of injections in patients with wet AMD within a period of 1 year. This discrepancy could be attributed to the fact that the 12-month study period is possibly too short to draw safe conclusions concerning the influence of Resvega on this parameter. In support of this theory, in our study at 12 months, there was no difference between the studied groups regarding the number of IAIs, while a significant difference was first noted at 18 months and became even more prominent at 24 months.
Fibrosis is generally regarded as a pathological wound healing response to tissue damage.42 It is remarkable that fibrosis in wet AMD shares common pathogenetic mechanisms with the development of fibrosis in other organs, including the lung, liver, kidney, heart, and skin.43,44 In wet AMD, CNV culminates in subretinal fibrosis through a process that involves multiple types of cells, including RPE cells, glia, fibroblasts, myofibroblast-like cells, and macrophages.43,45,46 They interact with inflammatory cytokines, growth factors, and matricellular proteins, resulting in cell proliferation, migration, and substantial changes in the extracellular matrix structure.43,45,46 Among growth factors, platelet-derived growth factor (PDGF) is a profibrotic mediator, while its BB subunit (PDGF-BB) has been recognized as having a crucial role in fibrosis development via the induction of migration and signaling in RPE cells.47
The advanced stages of wet AMD are characterized by the degeneration of photoreceptors and RPE cells and the consequent development/progression of subretinal fibrosis, which is followed by irreversible visual decline.4,48 Since fibrosis is the most important predictor of final visual acuity,49 significant efforts have been made to recognize therapeutic approaches that either inhibit fibrosis or limit its extent. To date, no antifibrotic treatment has been identified with the ability to prevent the development or to decelerate the enlargement of subretinal fibrosis.45 In the past, several trials have shown promising results in preventing fibrosis in cases of wet AMD that are promptly treated in a timely manner with intravitreal anti-VEGF agents alone; however, in clinical practice, these trials have been proven rather inefficient.48,50
According to our study, Resvega may play a key role in hindering the extension of fibrosis in cases of wet AMD and has a favorable effect on retinal remodeling. None of the patients in the combination group experienced an expansion of fibrosis, whereas 3 out of the 6 patients in the other group encountered an enlargement of the initially established fibrosis. The aforementioned finding could be explained by the antifibrotic action of RSV, which is apparent in multiple organs.51,52 Regarding the possible role of RSV in restricting the promotion of macular fibrosis it could be attributed to its involvement in the inhibition of PDGF-BB-induced migration and signaling in RPE-19 cells.47 Anti-PDGF therapy may increase the susceptibility of CNV to the effects of anti-VEGF therapy,53,54 providing another explanation for the associations detected in our study. Indeed, the patients in the “Eylea & Resvega” group needed significantly fewer IAIs, suggesting that anti-VEGF treatment was more efficient. Moreover, it should be taken into account that a lower number of IAIs is, on the one hand, indicative of fewer recurrences and, consequently, of a decreased frequency of fibrosis,30 whereas on the other hand, it has by itself a protective effect against fibrosis.40
Despite the interesting findings of our study, several inherent limitations are present. The 24-month study period may have been too short to accurately assess the effectiveness of Resvega in wet AMD, and prospective studies with longer follow-up periods, using also higher RSV doses are needed to efficiently determine the impact of the aforementioned oral supplement in wet AMD. Future studies will also evaluate the possible impact of RSV supplements on further visual outcomes that are associated with QoL indices, including contrast sensitivity and reading ability. Moreover, the relatively small sample size limits the generalizability of our conclusions; thus, larger studies are needed to validate our results. Since multiple factors are implicated in the development of fibrosis, it should be underlined that our results have to be interpreted with caution. Furthermore, we did not examine whether the impact of the treatment regimens was influenced by the type of CNV (“classic” or “occult”), since the “classic” ones are more likely to develop fibrosis.43 We should also mention that our findings could be affected by the relatively high frequency of established fibrosis in our patients before study initiation. Finally, our patients were treated only with IAIs; it would be of great interest to examine whether our findings are replicated in patients treated with other anti-VEGF agents, especially with the ones with longer duration of action.
Conclusion
In conclusion, our study suggested that the daily oral consumption of Resvega in patients suffering from wet AMD could be identified as a useful supplementary aid to the established treatment, highlighting superiority of the combination treatment modality may be superior to the monotherapy of IAIs, since this regimen yielded better outcomes regarding the number of IAIs, having also a significantly favorable effect in preventing the progression of fibrosis. The aforementioned attributes classify Resvega as a promising supplement in the battle against wet AMD.
Funding
This work was supported by an unrestricted Grant from Laboratoires Thea®, France.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Klein R, Chou CF, Klein BE, Zhang X, Meuer SM, Saaddine JB. Prevalence of age-related macular degeneration in the US population. Arch.Ophthalmol. 2011;129:75–80. doi:10.1001/archophthalmol.2010.318
2. Flaxman SR, Bourne RRA, Resnikoff S; Vision Loss Expert Group of the Global Burden of Disease Study, et al. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Glob Health. 5;2017:e1221–e1234. doi:10.1016/S2214-109X(17)30393-5
3. Rouvas A, Theodossiadis P, Georgalas I, Gouliopoulos N. Complete resolution of subretinal fluid of the fellow eye following aflibercept injection in wet AMD. Retin Cases Brief Rep. 2023;7.
4. Wu J, Zhang J. Neovascular Remodeling and Subretinal Fibrosis as Biomarkers for Predicting Incomplete Response to Anti-VEGF Therapy in Neovascular Age-Related Macular Degeneration. Front Biosci. 2022;27:135. doi:10.31083/j.fbl2704135
5. Rouvas A, Bouratzis N, Georgalas I, Gouliopoulos N. Is there any association between the frequency of wet age-related macular degeneration recurrences and the seasons of the year? Int Ophthalmol. 2023;43:3287–3295. doi:10.1007/s10792-023-02732-z
6. Bird AC, Bressler NM, Bressler SB, et al. An international classification and grading system for age-related maculopathy and age-related macular degeneration. The International ARM Epidemiological Study Group. Surv Ophthalmol. 1995;39:39367–39374. doi:10.1016/S0039-6257(05)80092-X
7. Datseris I, Bouratzis N, Kotronis C, et al. One-year outcomes of resveratrol supplement with aflibercept versus aflibercept monotherapy in wet age-related macular degeneration. Int J Ophthalmol. 2023;16:1496–1502. doi:10.18240/ijo.2023.09.17
8. Wong TY, Chakravarthy U, Klein R, et al. The natural history and prognosis of neovascular age-related macular degeneration: a systematic review of the literature and meta-analysis. Ophthalmology. 2008;115:16–26. doi:10.1016/j.ophtha.2007.03.008
9. Lindblad AS, Clemons TE. Responsiveness of the National Eye Institute Visual Function Questionnaire to progression to advanced age-related macular degeneration, vision loss, and lens opacity: AREDS Report no. 14. Arch Ophthalmol. 2005;123(14):1207–1214. AREDS Report.
10. Vu KV, Mitchell P, Detaram HD, Burlutsky G, Liew G, Gopinath B. Risk factors for poorer quality of life in patients with neovascular age-related macular degeneration: a longitudinal clinic-based study. Eye (Lond). 2023;2736–2743. doi:10.1038/s41433-023-02407-0
11. Miller JW, Adamis AP, Shima DT, et al. Vascular endothelial growth factor/vascular permeability factor is temporally and spatially correlated with ocular angiogenesis in a primate model. Am J Pathol. 1994;145:574–584.
12. Sato T, Takeuchi M, Karasawa Y, Enoki T, Ito M. Intraocular inflammatory cytokines in patients with neovascular age-related macular degeneration before and after initiation of intravitreal injection of anti-VEGF inhibitor. Sci Rep. 2018;8:1098. doi:10.1038/s41598-018-19594-6
13. Servillo A, Zucchiatti I, Sacconi R, et al. The state-of-the-art pharmacotherapeutic management of neovascular age-related macular degeneration. Expert Opin Pharmacother. 2023;24:197–206. doi:10.1080/14656566.2022.2154145
14. Kim LA, D’Amore PA. A brief history of anti-VEGF for the treatment of ocular angiogenesis. Am J Pathol. 2012;181:376–379. doi:10.1016/j.ajpath.2012.06.006
15. Chakravarthy U, Armendariz BG, Fauser S. 15 years of anti-VEGF treatment for nAMD: success or failure or something in between? Eye (Lond). 2022;36:2232–2233. doi:10.1038/s41433-022-02153-9
16. Koskela A, Reinisalo M, Petrovski G, et al. Nutraceutical with Resveratrol and Omega-3 Fatty Acids Induces Autophagy in ARPE-19 Cells. Nutrients. 2016;8(5):284. doi:10.3390/nu8050284
17. Nagineni CN, Raju R, Nagineni KK, et al. Resveratrol Suppresses Expression of VEGF by Human Retinal Pigment Epithelial Cells: potential Nutraceutical for Age-related Macular Degeneration. Aging Dis. 2014;5:88–100. doi:10.14366/AD.2014.050088
18. Pop R, Daescu A, Rugina D, Pintea A. Resveratrol: its Path from Isolation to Therapeutic Action in Eye Diseases. Antioxidants. 2022;11:2447. doi:10.3390/antiox11122447
19. Pervaiz S, Holme AL. Resveratrol: its biologic targets and functional activity. Antioxid Redox Sig. 2009;11:2851–2893. doi:10.1089/ars.2008.2412
20. Nashine S, Nesburn AB, Kuppermann BD, Kenney MC. Role of Resveratrol in Transmitochondrial AMD RPE Cells. Nutrients. 2020;12:159. doi:10.3390/nu12010159
21. Berman AY, Motechin RA, Wiesenfeld MY, Holz MK. The therapeutic potential of resveratrol: a review of clinical trials. NPJ Precision Onc. 2017;1:35. doi:10.1038/s41698-017-0038-6
22. Courtaut F, Aires V, Acar N, et al. RESVEGA, a Nutraceutical Omega-3/Resveratrol Supplementation, Reduces Angiogenesis in a Preclinical Mouse Model of Choroidal Neovascularization. Int J mol Sci. 2021;22:11023. doi:10.3390/ijms222011023
23. Bhattarai N, Korhonen E, Toppila M, et al. Resvega Alleviates Hydroquinone-Induced Oxidative Stress in ARPE-19 Cells. Int J mol Sci. 2020;21:2066. doi:10.3390/ijms21062066
24. Lançon A, Frazzi R, Anti-Oxidant LN. Anti-Inflammatory and Anti-Angiogenic Properties of Resveratrol in Ocular Diseases. Molecules. 2016;21:304. doi:10.3390/molecules21030304
25. Subramani M, Ponnalagu M, Krishna L, et al. Resveratrol reverses the adverse effects of bevacizumab on cultured ARPE-19 cells. Sci Rep. 2017;7:12242. doi:10.1038/s41598-017-12496-z
26. Sghaier R, Perus M, Cornebise C, et al. Resvega, a Nutraceutical Preparation, Affects NFκB Pathway and Prolongs the Anti-VEGF Effect of Bevacizumab in Undifferentiated ARPE-19 Retina Cells. Int J mol Sci. 2022;23:11704. doi:10.3390/ijms231911704
27. Richer S, Stiles W, Ulanski L, Carroll D, Podella C. Observation of human retinal remodeling in octogenarians with a resveratrol based nutritional supplement. Nutrients. 2013;5:1989–2005. doi:10.3390/nu5061989
28. Richer S, Patel S, Sockanathan S, Ulanski LJ 2nd, Miller L, Podella C. Resveratrol based oral nutritional supplement produces long-term beneficial effects on structure and visual function in human patients. Nutrients. 2014;6:4404–4420. doi:10.3390/nu6104404
29. Lalwani GA, Rosenfeld PJ, Fung AE, et al. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: year 2 of the PrONTO Study. Am J Ophthalmol. 2009;148:43–58. doi:10.1016/j.ajo.2009.01.024
30. Rouvas A, Gouliopoulos N, Douvali M, et al. One year outcomes of treat and extend and pro re nata (PRN) treatment regimens with aflibercept for polypoidal choroidal vasculopathy. Eur J Ophthalmol. 2021;31:2868–2875. doi:10.1177/11206721211014717
31. Kim BH, Chang IB, Yu HG, Hong IH. Volumetric fluid analysis of fixed monthly anti-VEGF treatment in patients with neovascular age-related macular degeneration. Int J Ophthalmol. 2023;16:909–914. doi:10.18240/ijo.2023.06.12
32. Rouvas A, Gouliopoulos NS, Moschos MM, Theodossiadis P. Optic disk melanocytoma associated with polypoidal choroidal vasculopathy lesions, after combination treatment of photodynamic therapy and intavitreal aflibercept (Eylea), a case report. BMC Ophthalmol. 2018;18:267. doi:10.1186/s12886-018-0927-7
33. Schranz M, Sacu S, Reiter GS, et al. Structure-Function Correlation of Retinal Fibrosis in Eyes with Neovascular Age-Related Macular Degeneration. J Clin Med. 2024;13:1074. doi:10.3390/jcm13041074
34. Bachmeier I, Armendariz BG, Yu S, et al. Fibrosis in neovascular age-related macular degeneration: a review of definitions based on clinical imaging. Surv Ophthalmol. 2023;68:835–848. doi:10.1016/j.survophthal.2023.03.004
35. Song D, Liu P, Shang K, Ma Y. Application and mechanism of anti-VEGF drugs in age-related macular degeneration. Front Bioeng Biotechnol. 2022;10:943915. doi:10.3389/fbioe.2022.943915
36. Rosenfeld PJ, Brown DM, Heier JS, et al. MARINA Study Group. N Engl J Med. 2006;355:1419–1431. doi:10.1056/NEJMoa054481
37. Schmidt-Erfurth U, Kaiser PK, Korobelnik JF, et al. Intravitreal aflibercept injection for neovascular age-related macular degeneration: ninety-six-week results of the VIEW studies. Ophthalmology. 2014;121:193–201. doi:10.1016/j.ophtha.2013.08.011
38. Hernandez L, Lanitis T, Cele C, Toro-Diaz H, Gibson A, Kuznik A. Intravitreal Aflibercept Versus Ranibizumab for Wet Age-Related Macular Degeneration: a Cost-Effectiveness Analysis. J Manag Care Spec Pharm. 2018;24:608–616. doi:10.18553/jmcp.2018.24.7.608
39. Nishikawa K, Oishi A, Hata M, et al. Four-Year Outcome of Aflibercept for Neovascular Age-Related Macular Degeneration and polypoidal choroidal vasculopathy. Sci Rep. 2019;9:3620. doi:10.1038/s41598-019-39995-5
40. Romano F, Cozzi E, Airaldi M, et al. Ten-Year Incidence of Fibrosis and Risk Factors for Its Development in Neovascular Age-Related Macular Degeneration. Am J Ophthalmol. 2023;252:170–181. doi:10.1016/j.ajo.2023.03.033
41. Chatziralli I, Dimitriou E, Chatzirallis A, et al. Efficacy and safety of vitamin supplements with resveratrol in diabetic macular edema: long-term results of a comparative study. Eur J Ophthalmol. 2022;32(5):2735–2739. doi:10.1177/11206721211057682
42. Wynn TA. Common and unique mechanisms regulate fibrosis in various fibroproliferative diseases. J Clin Invest. 2007;117:524–529. doi:10.1172/JCI31487
43. Ishikawa K, Kannan R, Hinton DR. Molecular mechanisms of subretinal fibrosis in age-related macular degeneration. Exp Eye Res. 2016;142:19–25. doi:10.1016/j.exer.2015.03.009
44. Friedlander M. Fibrosis and diseases of the eye. J Clin Invest. 2007;117(3):576–586. doi:10.1172/JCI31030
45. Tenbrock L, Wolf J, Boneva S, et al. Subretinal fibrosis in neovascular age-related macular degeneration: current concepts, therapeutic avenues, and future perspectives. Cell Tissue Res. 2022;387:361–375. doi:10.1007/s00441-021-03514-8
46. Kent D, Sheridan C. Choroidal neovascularization: a wound healing perspective. Mol Vis. 2003;9:747–755.
47. Chan CM, Chang HH, Wang VC, Huang CL, Hung CF. Inhibitory effects of resveratrol on PDGF-BB-induced retinal pigment epithelial cell migration via PDGFRβ, PI3K/Akt and MAPK pathways. PLoS One. 2013;8:e56819.
48. Bloch SB, Lund-Andersen H, Sander B, Larsen M. Subfoveal Fibrosis in Eyes with Neovascular Age-Related Macular Degeneration Treated with Intravitreal Ranibizumab. Am J Ophthalmol. 2013;156:116–124.e1. doi:10.1016/j.ajo.2013.02.012
49. Cheung CMG, Grewal DS, Teo KYC, et al. The Evolution of Fibrosis and Atrophy and Their Relationship with Visual Outcomes in Asian Persons with Neovascular Age-Related Macular Degeneration. Ophthalmol Retina. 2019;3:1045–1055. doi:10.1016/j.oret.2019.06.002
50. Roberts PK, Zotter S, Montuoro A, et al. Identification and Quantification of the Angiofibrotic Switch in Neovascular AMD. Invest Ophthalmol Vis Sci. 2019;60:304–311. doi:10.1167/iovs.18-25189
51. Liu N, Fan X, Shao Y, et al. Resveratrol attenuates inflammation and fibrosis in rheumatoid arthritis-associated interstitial lung disease via the AKT/TMEM175 pathway. J Transl Med. 2024;22:457. doi:10.1186/s12967-024-05228-1
52. Huo R, Huang X, Yang Y, Yang Y, Lin J. Potential of resveratrol in the treatment of interstitial lung disease. Front Pharmacol. 2023;14:1139460. doi:10.3389/fphar.2023.1139460
53. Erber R, Thurnher A, Katsen AD, et al. Combined inhibition of VEGF and PDGF signaling enforces tumor vessel regression by interfering with pericyte-mediated endothelial cell survival mechanisms. FASEB J. 2004;18:338–340. doi:10.1096/fj.03-0271fje
54. Jo N, Mailhos C, Ju M, et al. Inhibition of platelet-derived growth factor B signaling enhances the efficacy of anti-vascular endothelial growth factor therapy in multiple models of ocular neovascularization. Am J Pathol. 2006;168:2036–2053. doi:10.2353/ajpath.2006.050588
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.