")
Back to Journals » Clinical Ophthalmology » Volume 19
Retinal Artery Occlusion Associated with Prepapillary Arterial Loop: An Isolated Ocular Disease? Case Report and Literature Review
Authors Mansour AM , Parodi MB, Casella AMB , Kheir WJ , Bashshur ZF
Received 28 November 2024
Accepted for publication 30 January 2025
Published 11 February 2025 Volume 2025:19 Pages 449—458
DOI https://doi.org/10.2147/OPTH.S509248
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ahmad M Mansour,1 Maurizio Battaglia Parodi,2 Antônio Marcelo Barbante Casella,3 Wajiha J Kheir,1 Ziad Fayez Bashshur1
1Department of Ophthalmology, American University of Beirut, Beirut, Lebanon; 2Department of Ophthalmology, University Vita-Salute Milan, Milan, Italy; 3Department of Ophthalmology, Universidade Estadual de Londrina, Paraná, Brazil
Correspondence: Ahmad M Mansour, Department of Ophthalmology, American University of Beirut, Beirut, Lebanon, Tel +961-337-7633, Email [email protected]
Purpose: When branch retinal artery occlusion is linked to prepapillary artery loop, is a systemic work-up necessary?
Methods: Case Report and literature review. The databases searched were MEDLINE OVID, Scopus, Web of Science, and Embase. The search was for all relevant articles published from inception until October 31, 2024.
Results: A total of 33 cases of prepapillary artery loop with retinal artery occlusion were reviewed. Median age at diagnosis was 24 years (range 10– 64). Twenty five cases had no systemic disease while 9 had unrelated systemic disorder. Systemic workup was carried in 17 cases and was negative. The location of the branch retinal artery occlusion was inferior in 21 cases, superior in 6 cases, and combined superior and inferior in 2 cases. Paracentral acute middle maculopathy was noted in 2 cases. Precipitating factors included exercise in 4 cases, head trauma in 2 cases, blunt ocular trauma, severe sneezing, ocular rubbing and sun exposure in 1 case each.
Conclusion: A branch retinal artery occlusion linked to a prepapillary loop appears as a distinct ocular condition in young healthy individuals. There is no definite need for additional diagnostic testing in such patients with a negative systemic history.
Keywords: prepapillary arterial loop, branch retinal artery occlusion, systemic workup
Introduction
Prepapillary arterial loop is a rare congenital vascular1–34 anomaly originating from a branch retinal artery and ending at the optic disc with projection into the vitreous cavity. Distinguishing it from other pathologies such as optic disc collaterals or neovascularization is crucial. There is no known association between prepapillary capillary loops and specific systemic illness. This variant of normal retinal vasculature, occurs when a developing retinal artery diverges into the vitreous cavity within Cloquet’s canal and returns back to the retina. It is usually unilateral in 80% of cases and the number of loops can vary from 1 to 10.15 Prepapillary arterial loops, also known as spirals, are classified based on their morphological appearances.15 The majority are detected on routine fundus exam and cause no symptoms. The most dreaded complication is occlusion of the branch retinal artery emanating from the loop.1–32 Many such cases undergo extensive workup to find the cause of the vascular occlusion.3,7,13,16,19,24–26,28,29,34 The laboratory vascular workup has included complete blood count, platelet count, erythrocyte sedimentation rate, lipid profile, antiphospholipid antibodies, and coagulation screen. In addition, imaging studies have included echocardiography and carotid Doppler ultrasonography.35 We present such a case and wonder whether any workup is obligatory based on an extensive literature review.
Case Report
A 29-year-old Caucasian man complained of a sudden right superior visual field loss at noon time 10 days prior to presentation at a major eye facility overseas. Corrected visual acuity (from myopic astigmatism) was 20/20 in both eyes with a normal intraocular pressure. Funduscopy revealed sectorial whitening of the inferior temporal retina sparing the foveal region (Figures 1 and 2). Fluorescein angiography confirmed obstruction of the inferotemporal arteries sparing the macula with nonperfusion of the prepapillary arterial loop (Figure 3). The branch retinal artery occlusion spared the fovea by optic coherence tomography (Figure 4). A right superior visual field was documented (Figure 4). Extensive blood work-up (complete blood count, platelet count, fasting blood sugar level, lipid profile, coagulation profile, anti-nuclear antibody, anti-cardiolipin, lupus anticoagulant), as well as electrocardiogram, echocardiography, and carotid duplex ultrasound were unrevealing. The patient denied intravenous drug abuse. He was placed on acetyl salicylic acid and clopidogrel. A second opinion was sought, and a CT angiography of the brain was negative based on the differential diagnosis of arteriovenous anastomoses. A third opinion attested to the entity of branch retinal artery occlusion from prepapillary arterial loop with no need for further diagnostic tests. The visual status was unchanged at the one-month follow-up, before leaving the country.
 |
Figure 1 Widefield pseudocolor fundus of the right eye showing inferotemporal branch retinal artery occlusion (arrow). |
 |
Figure 2 Prepapillary arterial loop takes the figure of eight configuration (arrow). |
 |
Figure 3 Venous phase of the right eye shows nonperfusion of the loop (arrow) and of the inferior temporal retina (star). |
 |
Figure 4 (A)- Vertical raster of the right prepapillary loop (arrow). (B)- Vertical raster through the fovea revealed hyperreflectivity and increased thickness of the inner retinal layers in the superior (arrow) compared to inferior retina. (C)- Superior visual field defect of the right eye. |
Literature Review
The databases searched were MEDLINE OVID, Scopus, Web of Science, and Embase. The search was for all relevant articles published from inception until October 31, 2024 following the Prisma guidelines. No limitation was placed on language, year of publication, or study design. MEDLINE was used with the following MeSH (Medical Subject Headings): prepapillary arterial loop or prepapillary vascular loop AND vascular occlusion or retinal vascular occlusion. All interventional and observational studies (case report, case series) were included. A manual search was also conducted to ensure the inclusion of potentially missing relevant articles. We searched for 1) similar articles of the finally included articles in our review, 2) reference list of finally included articles in our review, and 3) Google scholar as grey literature. The following data was collected using an Excel (Microsoft, Redmond, WA, USA) extraction sheet: baseline characteristics (year of publication, country of corresponding author, age, gender, systemic disease, possible etiology of arterial occlusion), initial best corrected visual acuity and workup for retinal vascular occlusion.
Results
A total of 33 cases (31 articles) were collected from 1901 to 2024 (including the current case report and after deleting 2 duplicates) (Tables 1 and 2). The median age was 24 (range 10–64), with equal gender distribution 15 vs15 and more involvement of the right eye (19 right vs11 left). The occlusion was inferior in 21, superior in 6, and both in 2 cases. The median presenting best corrected visual acuity was 20/20. Three cases had secondary vitreous hemorrhage and two had paracentral acute middle maculopathy. Twenty-five patients had no known systemic disease while 4 had unrelated systemic disorder. Workup for retinal vascular occlusion (complete blood count, platelet count, erythrocyte sedimentation rate, coagulation screen, carotid ultrasound, echocardiogram, and brain imaging) (Table 3) was done in 17 and turned up to be negative in all such cases while work-up was deemed unnecessary in 12. Precipitating factors included Valsalva maneuvers (strenuous exercise in 4 and severe sneezing in 1) and some kind of trauma (head trauma in 2, blunt trauma in 1 and strong ocular rubbing in 1).
 |
Table 1 Summary of a Literature Review of Branch Retinal Artery Occlusion (BRAO) with Prepapillary Arterial Loop |
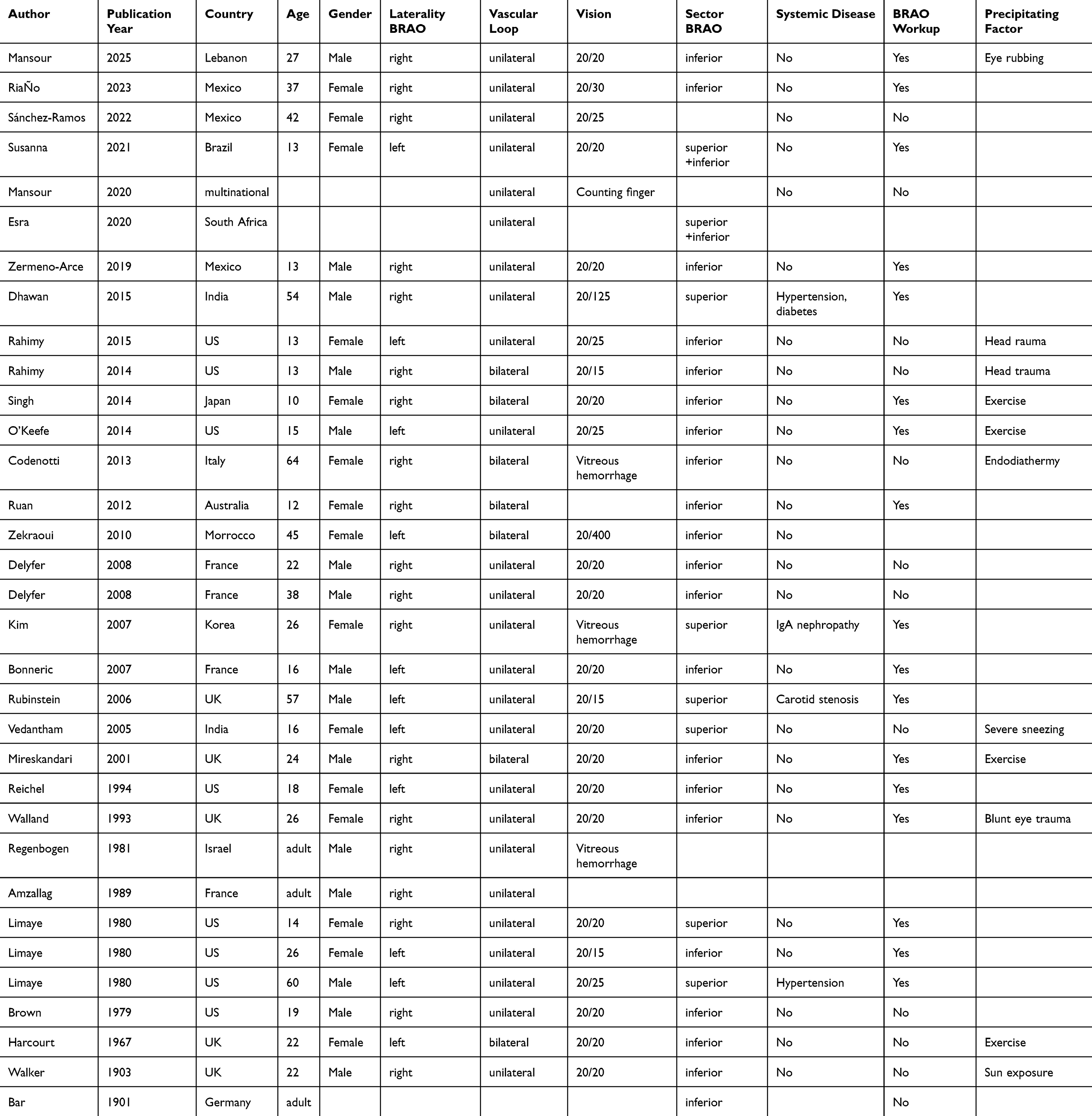 |
Table 2 Excel Sheet of the Detailed Literature Review of Branch Retinal Artery Occlusion (BRAO) with Prepapillary Arterial Loop |
 |
Table 3 Detailed Laboratory Investigations in 17 Patients with Branch Retinal Artery Occlusion (BRAO) and Prepapillary Arterial Loop Reported in the Literature |
Discussion
Generally, patients with branch retinal artery occlusion need an urgent stroke workup. However in the case of prepapillary arterial loop, as in both this case report and literature review attest to, there is no need for systemic workup. Occlusion in this entity is intrinsic to the loop physiology and pathology. Pathologically, prepapillary vascular loop does not have an internal elastic lamina and is supported by a connective tissue sheath lined by a cellular lamina.36 This weakened vessel wall is hence more prone to vasoocclusion. Physiologically, it is known that twisted vessels are more prone to occlusion with several cases of twisted cerebrovascular vessels reported to lead to occlusion of blood flow.37,38 Prepapillary loops, and more so the coil-like structures, appear to alter the hemodynamics and increase the risk of thromboembolic events due to turbulent blood flow.15 Prepapillary loops can assume several shapes: figure of eight, corkscrew, or hairpin turn.15 It seems that the torsional forces accompanied by turbulence lead to twisting and strangulation of the loop. Hemodynamic turbulence inside the loop results in endothelial damage with secondary intraarterial clot. Occasionally there is vitreous traction on the loop.39 There is no known association between prepapillary capillary loops and specific systemic illness.
Conclusions
In conclusion, the presence of a prepapillary arterial loop in a young healthy patient with branch retinal artery occlusion does not necessitate a thorough and multidisciplinary approach to diagnosis and management. Detailed systemic evaluation and proactive management strategies are not crucial to optimizing patient outcomes. This entity is a local ocular problem with inherent tendency of the loop to twist occurring mostly in young subjects probably initiated by exercise, Valsalva and ocular trauma or rubbing.
Ethics Approval and Informed Consent
This case report was conducted in accordance with the declaration of Helsinki. Written informed consent was provided by the patient to have the case details and accompanying images published. Institutional approval was not required to publish the case details.
Acknowledgments
Dr Ola Zein, Souha Yazbek, and Sally Naalbandian helped conduct the review and supply the references for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship and publication of this article.
Disclosure
The authors report no financial competing interests.
References
1. Amzallag T, Rouland JF, Ryckewaert M, Hustin B. Ischémie artérielle rétinienne par malformation vasculaire papillaire (French). Bull Soc Ophtalmol Fr. 1989;89(12):1437–1439.
2. Bar C. Ein Fall von in den Glaskorper vordringender Arteriesnschlinge in einem durch Embolic der Centralarterie erblindenten (German). Klin Monatsbl Augenh. 1901;39:307.
3. Bonneric JG, Boissonnot M, Rovira JC, Dighiero P. Une boucle artérielle prépapillaire compliquée d’occlusion de branche artérielle rétinienne (French). J Fr Ophtalmol. 2007;30(3):e8. doi:10.1016/s0181-5512(07)89592-1
4. Brown GC, Magargal L, Augsberger JJ, Shields JA. Preretinal arterial loops and retinal arterial occlusion. Am J Ophthalmol. 1979;87(5):646–651. doi:10.1016/0002-9394(79)90298-8
5. Codenotti M, Fogliato G, De Benedetto U, et al. Simultaneous vitreous hemorrhage and branch retinal artery occlusion after prepapillary arterial loop rupture (French). J Fr Ophtalmol. 2013;36(4):e63–65. doi:10.1016/j.jfo.2012.07.005
6. Delyfer MN, Rougier MB, François L, Korobelnik JF, Occlusion de branche artérielle rétinienne chez deux jeunes patients présentant une boucle vasculaire pré-papillaire congénitale (French). J Fr Ophtalmol. 2008;31(1):126–127. doi:10.1016/S0181-5512(08)70344-9
7. Dhawan A, Shukla D. Combined occlusion of branch retinal artery and vein secondary to prepapillary arterial loops. Indian J Ophthalmol. 2015;63(12):917–918. doi:10.4103/0301-4738.176027
8. Esra N, Makgotloe A. Simultaneous superior and inferior temporal branch retinal arterial occlusion caused by a prepapillary vascular loop: a case report and review of the literature. South Afr Ophthalmol J. 2020;15(4):30–33.
9. Godel V, Regenbogen L, Lazar M, Coscas G. Vascular accidents in preretinal arterial loops. Int Ophthamol. 1980;2(3):151–155. doi:10.1007/BF00137960
10. Harcourt RB, Locket NA. Occlusion of a pre-retinal arterial loop. Br J Ophthalmol. 1967;51(8):562–565. doi:10.1136/bjo.51.8.562
11. Huang Y. Prepapillary arterial loop. Report of 2 cases (Chinese). Chinese Med J. 1988;101(7):510–512.
12. Khan MA, Shahlaee A, Kaiser RS. Two-year follow-up of a prepapillary vascular loop–related branch retinal artery occlusion. JAMA Ophthalmol. 2016;134(2):e153670. doi:10.1001/jamaophthalmol.2015.3670
13. Kim S-K, Kwon S-K. Prepapillary vascular loops associated with branch retinal artery occlusion and vitreous hemorrhage. J Korean Ophthalmol Soc. 2007;48:1001–1006.
14. Limaye SR, Tang RA, Pilkerton AR. Cilioretinal circulation and branch arterial occlusion associated with preretinal arterial loops. Am J Ophthalmol. 1980;89(6):834–839. doi:10.1016/0002-9394(80)90175-0
15. Mansour AM, Kozak I, Saatci AO, et al. Prepapillary vascular loop-a new classification. Eye. 2021;35(2):425–432. doi:10.1038/s41433-020-0859-3
16. Mireskandari K, Bentley C, Aclimandos WA. Bilateral prepapillary loops with unilateral branch retinal artery occlusion following thrombus at the loop apex. Retina. 2001;21(1):66–67. doi:10.1097/00006982-200102000-00012
17. Misra A, Flanagan DW, Martin KR. Recurrent transient visual loss due to intermittent occlusion of a prepapillary vascular loop. Brit J Ophthalmol. 2008;92(3):431–432. doi:10.1136/bjo.2007.124073
18. Oderinlo OO, Hassan AO, Okonkwo ON. Optical coherence tomography angiography features of paracentral acute middle maculopathy in a young female in sub-Saharan Africa: a case report. J Case Rep Images Ophthalmol. 2018;1:1. 100002Z17OO2018
19. O’Keefe GAD, Sadda SVR. A pre-retinal arterial loop causing a branch retinal artery occlusion. Ophthalmic Surg Lasers Imaging Retina. 2014;45(1):66–68. doi:10.3928/23258160-20131114-01
20. Rahimy E, Rayess N, Kaiser RS. Prepapillary vascular loop and associated branched retinal arterial occlusion (letter). JAMA Ophthalmol. 2015;133(3):363. doi:10.1001/jamaophthalmol.2014.4642
21. Rahimy E, Rayess N, Talamini CL, Kaiser RS. Traumatic prepapillary loop torsion and associated branch retinal artery occlusion. JAMA Ophthalmol. 2014;132(11):1376–1377. doi:10.1001/jamaophthalmol.2014.2415
22. Regenbogen L, Godel V, Spierer A, Lazar M. Retinal arterial loop occlusion. Ann Ophthalmol. 1981;13(6):729–732.
23. Reichel E, Duker JS, Puliafito CA, Hedges TR
24. Riaño CV, Mariscal HG, Guerra JF, Sierra JMJ, Aceves OT. BRAO associated with prepapillary vascular loop. Retina Today. 2023;18(3);51–53.
25. Ruan C, Karagiannis D, Moore A, Wong J. Prepapillaryvascular loops-an unusual case of retinal artery occlusion in a young patient and a population-based survey. Clin Exp Ophthalmol. 2012;40:113–114.
26. Rubinstein A, Chen SD, Fletcher EC, Hundal K, Downes SM. Branch retinal artery obstruction in a patient with a prepapillary loop and carotid artery stenosis. Eye. 2006;20(2):257–258. doi:10.1038/sj.eye.6701835
27. Sánchez-Ramos JA, Hernández-Vázquez ÁY, Pérez-Montaño CR, Rojas-Juárez S, Ramírez-Estudillo A, Benito Celis-Suazo B. Paracentral acute middle maculopathy associated with pre-papillary vascular loops. A case report (Spanish). Rev Mex Oftalmol. 2022;96(6):256–259.
28. Singh R, Fujinami K, Moore AT. Branch retinal artery occlusion secondary to prepapillary arterial loop. Retin Cases Brief Rep. 2014;8(2):124–126. doi:10.1097/ICB.0000000000000020
29. Susanna BN, Barbosa GCS, de Almeida L, Neto JZ. Prepapillary arterial loop associated with central retinal artery occlusion: a case report. J Curr Ophthalmol. 2021;33(2):212–214. doi:10.4103/joco.joco_179_20
30. Vedantham V, Ramasamy K, Namperumalsamy P, Cunningham ET. Double prepapillary arterial loops associated with superior branch macular artery occlusion. Indian J Ophthalmol. 2005;53(2):126–128. doi:10.4103/0301-4738.16178
31. Walker CH. Thrombosis of the inferior temporal branch of the arteria centralis retinae in an eye with a persistent hyaloid artery and vein; caused by exposure to direct sunlight. Trans Ophthalmol Soc UK. 1903;23:279.
32. Walland MJ. Branch retinal arterial occlusion with trauma. Aust. N Z J Ophthalmol. 1993;21(4):280–281. doi:10.1111/j.1442-9071.1993.tb00973.x
33. Zekraoui Y, Nafizy I, Hajji Z, Benchekroun N, Boulanouar A, Berraho A. Boucle vasculaire prépapillaire bilatérale compliquée d’une occlusion artérielle (French). J Fr Ophtalmol. 2010;33(10):715–717. doi:10.1016/j.jfo.2010.10.007
34. Zermeno-Arce AJ, Ledesma-Gil G, Moreno-Mendoza R, Graue-Wiechers F. Arterial occlusion associated with a prepapillary vascular loop. Anatomical changes on the long term follow up (Spanish). Arch Soc Esp Oftalmol. 2019;94(8):405–408. doi:10.1016/j.oftal.2019.03.019
35. Maiz AM, Murali S, Miller JM. Retinal artery occlusion in young patients without typical cardiovascular risk factors: etiologies, prognosis, and suggested work-up. Graefes Arch Clin Exp Ophthalmol. 2024(262):3577–3587. doi:10.1007/s00417-024-06527-5
36. Shakin EP, Shields JA, Augsburger JJ, Brown GC. Clinicopathologic correlation of a prepapillary vascular loop. Retina. 1988;8(1):55–58. doi:10.1097/00006982-198808010-00010
37. Han HC. Twisted blood vessels: symptoms, etiology and biomechanical mechanisms. J Vasc Res. 2012;49(3):185–197. doi:10.1159/000335123
38. Lee KE, Jeong EH, Yu HJ, et al. Cerebral infarction caused by a tortuous subclavian artery: a case report. Neurointervention. 2014;9(1):53–55. doi:10.5469/neuroint.2014.9.1.53
39. Youssoufou Souley AS, Alsubari A, Chammout FZ, El Khoyaali A, Reda K, Oubaaz A. Prepapillary vascular loop with vitreous traction (French). J Fr Ophtalmol. 2018;41(10):1002. doi:10.1016/j.jfo.2018.02.022
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.