")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Retrospective Multicentre Real-Life Study Evaluating the Efficacy of Atezolizumab Combined with Bevacizumab for the Treatment of Metastatic Hepatocellular Carcinoma: HIREAL Study
Authors Barbe-Richaud JB, Moinard-Butot F , Husson-Wetzel S, Bolliet M, Chiappa P, Belletier C, Ribeiro M, Poprawa E, Bigot C, Abergel A, Ben Abdelghani M
Received 6 February 2025
Accepted for publication 10 June 2025
Published 1 July 2025 Volume 2025:12 Pages 1279—1286
DOI https://doi.org/10.2147/JHC.S521130
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Ali Hosni
Jean-Baptiste Barbe-Richaud,1,* Fabien Moinard-Butot,1,* Stéphanie Husson-Wetzel,2 Marion Bolliet,3 Pascale Chiappa,1 Christine Belletier,1 Mathieu Ribeiro,4 Elodie Poprawa,1 Cécile Bigot,1 Armand Abergel,5 Meher Ben Abdelghani1
1Medical Oncology Department, Institut de Cancérologie de Strasbourg Europe (ICANS), Strasbourg, France; 2Hepato-Gastroenterology Department, Centre Hospitalier de Mulhouse, Mulhouse, France; 3Hepato-gastroenterology Department, Centre Hospitalier de Colmar, Colmar, 68000, France; 4Digestive and Hepato-Biliary Surgery Department, Hôpital Universitaire de Clermont-Ferrand, Clermont-Ferrand, France; 5Digestive and Hepatobiliary Medicine Department, Hôpital Universitaire de Clermont-Ferrand, Clermont-Ferrand, France
*These authors contributed equally to this work
Correspondence: Meher Ben Abdelghani, Email [email protected]
Background: Hepatocellular carcinoma (HCC) is the most common hepatic malignancy and is one of the most prevalent cancers worldwide. The prognosis of late-stage HCC remains poor. The ImBrave 150 trial successfully demonstrated that overall survival (OS) and progression-free survival (PFS) was improved among patients treated with atezolizumab combined with bevacizumab (AB) compared with patients treated with sorafenib. Real-world data are essential to assess the safety and efficacy of new therapies in HCC, given patients’ fragility and the heterogeneity of underlying liver diseases.
Objective: The primary objective of this study was to evaluate the OS and PFS of patients with locally advanced or metastatic HCC treated with atezolizumab combined with bevacizumab. The secondary objective was to conduct subgroup analyses to further examine how the effects of the combination treatment differ based on Child‒Pugh scores, prior local treatment, and alpha-fetoprotein (AFP) levels.
Methods: We conducted a multicentric retrospective study. All patients with confirmed locally advanced or metastatic HCC treated with atezolizumab combined with bevacizumab between January 2021 and December 2023 were included.
Results: Seventy patients were included. A total of 76% presented with cirrhosis, among which 85% had Child‒Pugh class A cirrhosis. The cirrhosis cases were mostly nonviral (85.7%). The median OS was 19 months (95% CI: 15–NA), and the median PFS was 6.7 months (95% CI: 4.7– 14.2 months). The secondary analysis revealed a statistically significant difference in OS between patients with Child‒Pugh class A cirrhosis and those with Child‒Pugh class B cirrhosis, with median OS durations of 18.9 months (95% CI: 16.9-NA) and 6.0 months (95% CI: 1.5-NA), respectively (p = 0.03). However, the retrospective design and the lack of a control group represent important limitations.
Conclusion: Our real-life study yielded OS and PFS durations similar to those reported in the ImBrave 150 trial.
Keywords: hepatocellular carcinoma, atezolizumab, bevacizumab, real-life data, overall survival, progression-free survival
Introduction
Hepatocellular carcinoma (HCC) is the most prevalent primary liver malignancy and represents a significant global health burden, with over 700,000 new cases and approximately 400,000 deaths annually worldwide.1 In France, the incidence of HCC has been increasing, with an estimated 10,000 new cases diagnosed each year.2 Despite advances in diagnostic and therapeutic strategies, the prognosis of locally advanced or metastatic HCC remains poor, with a 5-year survival rate of less than 20%.3
The combination of atezolizumab, an anti-PD-L1 (programmed cell death-ligand 1) antibody, and bevacizumab, an anti-VEGF (vascular endothelial growth factor) antibody, showed promising results for the treatment of locally advanced or metastatic HCC in the IMbrave150 trial, which was published in 2020. Compared with standard-of-care therapy (ie, sorafenib, a VEGF tyrosine kinase inhibitor (TKI)), the combination therapy significantly improved overall survival (OS) (13.4 months vs 19.2 months, respectively; confidence interval [95% CI]: 0.42–0.79) and progression-free survival (PFS) (4.3 months vs 6.8 months; 95% CI: 0.47–0.76) among patients with unresectable HCC.4
Despite the robust data from the IMbrave150 trial, real-world evidence on the efficacy and safety of atezolizumab combined with bevacizumab (AB) in diverse patient populations is important to obtain. The main risk factor for HCC is cirrhosis. The aetiology of cirrhosis is dichotomized into viral and nonviral cirrhosis. Viral hepatitis caused by hepatitis B virus (HBV) and/or hepatitis C virus (HCV) is the leading cause of cirrhosis and HCC in Asia and Africa. In contrast, nonviral cirrhosis, which is mostly represented by alcohol liver disease (ALD) and non-alcoholic fatty liver disease (NAFLD), remains the major cause of HCC in America and Europe.1 Drastic geographical variation in the underlying cause of cirrhosis has led to a heterogeneous landscape of patients harbouring HCC.
Additionally, the identification of predictive biomarkers for response to immunotherapy, such as the neutrophil-to-lymphocyte ratio (NLR) or early AFP variation, is increasingly explored to guide therapeutic choices. New combination strategies are also under evaluation, such as anti-PD-1/anti-VEGF plus TKIs or chemotherapy, reflecting a rapidly evolving treatment landscape.
Real-world studies are fundamental for providing insights into the performance of this therapeutic combination outside the controlled settings of clinical trials, as such studies encompass a broader spectrum of patient characteristics and comorbidities.
The current HIREAL study aims to evaluate the real-world application of AB for the treatment of locally advanced or metastatic HCC in a French cohort.
Methods
Study Design and Population
This retrospective, observational study was conducted across 6 centres in France and aimed evaluate the real-world efficacy and safety of AB combination therapy in patients with locally advanced or metastatic HCC. The study included patients treated between January 2021 and December 2023 who met the inclusion criteria.
Inclusion and Exclusion Criteria
Patients were included if they were aged 18 years or older, caucasian, had a confirmed diagnosis of metastatic or locally advanced HCC according to the European Association for the Study of the Liver (EASL) criteria, and had received at least one dose of AB combination therapy. Patients were excluded if they refused to participate. Data regarding BCLC stage were not systematically available and could not be included in the analysis.
Data Collection
All the data were collected from electronic medical records and included demographic information, clinical characteristics, laboratory results, treatment details, and outcomes. The specific data points included age, sex, ECOG performance status, underlying liver disease aetiology, Child‒Pugh score, and prior treatments for HCC.
Treatment Protocol
Patients received atezolizumab at a dose of 1200 mg and bevacizumab at a dose of 15 mg/kg. These agents were administered intravenously every three weeks, as per the standard of care. Treatment continued until disease progression, unacceptable toxicity, or until the physician or patient opted for discontinuation. Response to treatment was evaluated using RECIST version 1.1 criteria, as mRECIST evaluations were not systematically available across centres.
Outcomes
The primary endpoints were OS and PFS, defined as the time from the initiation of AB therapy to death from any cause and the time to the first documented disease progression or death, respectively. The secondary endpoints included the objective response rate (ORR), defined as the percentage of patients who achieved an objective radiological response (evaluated according to the RECIST 1.1 criteria); the disease control rate (DCR), defined as the percentage of patients who achieved an objective radiological response or stable disease; and the incidence of treatment-related adverse events (AEs). Secondary objectives included subgroup analyses based on Child‒Pugh score, prior locoregional treatment, and alpha-fetoprotein (AFP) levels.
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics and treatment outcomes. The Kaplan‒Meier method was used to estimate OS and PFS, and differences between subgroups were assessed via the Log rank test. Safety data were summarized via frequency counts and percentages. Subgroup analyses were performed to evaluate outcomes in patients with different baseline characteristics, including the Child‒Pugh score and Eastern Cooperative Oncology Group (ECOG) performance status score. All the statistical analyses were performed with R software (version 4.3.2).
Analyses were conducted on available data. Missing data were not imputed and were excluded from relevant subgroup analyses.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and approved by the institutional (Institut de Cancérologie Strasbourg Europe) review boards of the participating centres. Informed consent was obtained from all patients or their legal representatives for the use of their medical data for research purposes. Data confidentiality and patient anonymity were maintained throughout the study (IRB 2022–003).
Results
Patient Characteristics
A total of 70 patients with locally advanced or metastatic HCC were included in the study. The median age was 70 years (range: 26–86 years), with a male predominance (94%). Most patients had an ECOG performance status score of 0 or 1 (81%). A total of 76% presented with cirrhosis, among which 85% had Child‒Pugh class A cirrhosis, whereas 15% had Child‒Pugh class B cirrhosis. Regarding the aetiology of cirrhosis, the vast majority of cases were nonviral cirrhosis (85.7%). The liver disease underlying HCC was ALD in 37.1% of the patients, NAFLD in 20%, HBV or HCV in 14.3%, and no cirrhosis in 24.2%. Gastroscopy was performed on all 53 patients with cirrhosis. Prior locoregional therapies were reported in 55.7% of patients and mainly included surgery, transarterial chemoembolization (TACE) and radiofrequency ablation (RFA). Prior systemic treatments, primarily sorafenib, were reported by 75.7% of patients. Patient characteristics are summarized in Table 1.
 |
Table 1 Patient’s Characteristics at Baseline |
Efficacy Outcomes
The median follow-up duration was 14.9 months. The median OS for the entire cohort was 19 months (95% CI: 15–NA) (Figure 1). The median PFS was 6.7 months (95% CI: 4.7–14.2 months) (Figure 2). The ORR was 20%, with 2.9% achieving complete response (CR) and 17.1% achieving partial response (PR). Stable disease (SD) was observed in 34.3% of patients, leading to a DCR of 54.3%. Thirty percent of patients presented with progressive disease as the best response. Data regarding radiological response were missing or could not be obtained for 15.7% of patients, mainly because of premature death.
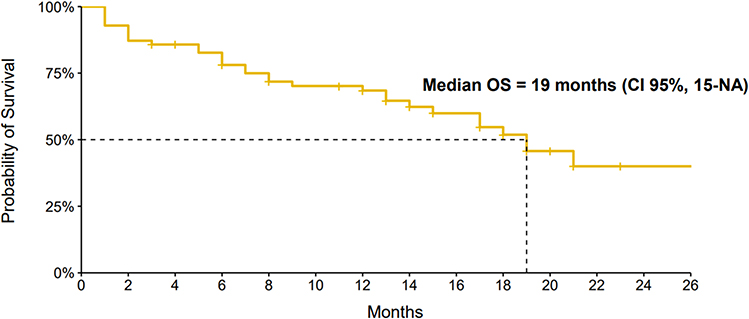 |
Figure 1 Kaplan-Meier Curve of Overall Survival (OS). |
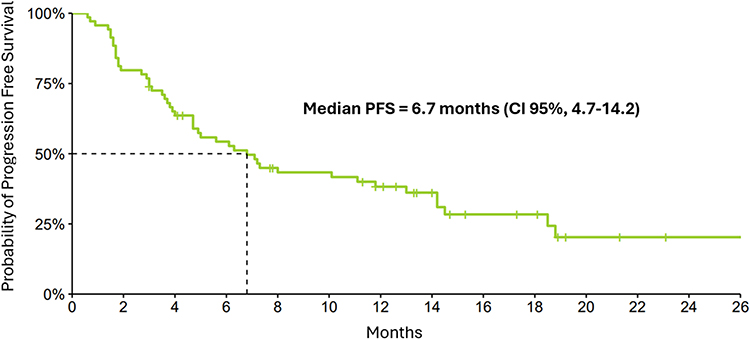 |
Figure 2 Kaplan-Meier Curve of Progression Free Survival (PFS). |
Subgroup Analyses
Subgroup analysis (N = 53) revealed a statistically significant difference between patients with Child‒Pugh class A cirrhosis and those with Child‒Pugh class B cirrhosis, with median OS durations of 18.9 months (95% CI: 16.9-NA) and 6.0 months (95% CI: 1.5-NA), respectively (p = 0.03) (Figure 3). PFS was also significantly different between patients with Child‒Pugh class A cirrhosis and those with Child‒Pugh class B cirrhosis, with median durations of 7.2 months (95% CI: 4.9–14.5) and 3.9 months (95% CI: 1.5-NA), respectively (p=0.04). There was no difference in OS durations based on alpha-fetoprotein (AFP) levels (N = 66) (> 400 ng/mL or < 400 ng/mL; p= 0.98), history of prior local treatment (p=0.75) or the aetiology of cirrhosis (viral or nonviral; p=0.9).
 |
Figure 3 Kaplan-Meier Curves of Overall Survival (OS) of Child-Pugh A patient compared to Child-Pugh B. |
Safety Outcomes
Treatment-related adverse events were reported in 50% of patients. The most common AEs included fatigue (24.2%), hypertension (18.6%), dysthyroidism (17.1%), and gastrointestinal symptoms such as diarrhoea (14.3%) (Table 2). Severe adverse events (SAEs) occurred in 17.1% of patients, with 7.1% discontinuing treatment due to AEs. There were no bleeding events during the follow-up period of the study.
 |
Table 2 Adverse Events |
Postprogression Treatments
Upon disease progression, 37.1% of patients received subsequent lines of therapy. The most common second-line treatment included sorafenib (88.6%). The median OS after disease progression was 15.1 months (95% CI: 6.9-NA).
Discussion
This real-world study provided valuable insights regarding the efficacy and safety of AB combination therapy for locally advanced or metastatic HCC within a French cohort. Our findings corroborate the results of the IMbrave150 trial, underscoring the benefits of this combination therapy in a real-world setting.4
The IMbrave150 trial was a landmark study that demonstrated the beneficial effects of AB combination therapy compared with sorafenib (the previous standard of care) in terms of significantly improving OS and PFS. Our study aligns with these results, showing comparable OS and PFS outcomes. Specifically, our cohort presented a median OS similar to the 19.2 months reported in the IMbrave150 study. The hazard ratios for OS (HR = 0.58) and PFS (HR = 0.59) also support the robust efficacy of this combination therapy.4
Furthermore, our findings are consistent with those of a large real-world study conducted in the United States, which confirmed the effectiveness and safety of atezolizumab combined with bevacizumab in a broader patient population with advanced HCC.5 This strengthens the external validity of our results and supports the integration of this combination therapy into routine clinical practice. Moreover, our study underscores the safety profile of combination therapy, which is consistent with the findings of the IMbrave150 trial. The incidence of AEs in our cohort was manageable and did not present new safety signs. Common adverse events such as hypertension and gastrointestinal symptoms were in line with those reported in the IMbrave150 trial, suggesting that the safety profile remains stable across different populations.6,7 The absence of gastrointestinal bleeding in our cohort may reflect the systematic pre-treatment assessment with gastroscopy and management of portal hypertension, including prophylactic measures such as variceal ligation or beta-blockers, in accordance with guidelines for AB therapy.
One of the significant strengths of this study is its real-world context, which includes a broader spectrum of patient characteristics and comorbidities than the controlled environment of a clinical trial. This diversity allows for a more comprehensive understanding of the treatment’s applicability and effectiveness across various patient subgroups. For example, our cohort included patients with more advanced disease stages and varying degrees of liver function, providing a deeper understanding of the real-world efficacy of this therapy.
However, the management of HCC patients with severe liver failure has always been critical.8 The risk of decompensation has led to the frequent exclusion of those patients in clinical trials. Our study also highlights a critical limitation in the efficacy of AB in patients with Child‒Pugh class B liver function. This subgroup analysis revealed that the therapeutic benefits observed in the general population did not extend to patients with more advanced liver cirrhosis. These patients did not experience significant improvements in OS or PFS, which aligns with findings from other studies suggesting that patients with Child‒Pugh class B liver function may not derive the same benefit from this combination therapy.9–11 This highlights the importance of careful patient selection and the need for alternative therapeutic strategies for this subgroup. A recent retrospective analysis of 217 patients with Child‒Pugh class B cirrhosis suggested that lenvatinib, a VEGF TKI, meaningfully improved OS and PFS as first-line therapy compared with AB;12 however, another retrospective study suggested no substantial difference.13 Furthermore, emerging evidence suggests that the ALBI score, a more objective measure of liver dysfunction, could offer superior prognostic value over the Child‒Pugh score, particularly in patients with Child‒Pugh class B cirrhosis, by better stratifying the risk of adverse outcomes.13 As a predictive model, some studies have explored the ability of the neutrophil‒lymphocyte ratio (NLR) to predict OS and PFS in patients treated with AB. The available data seem to demonstrate an independent link between a high NLR and poor outcomes.14–16 The major limitation is the nonconsensual cut-off used. Another study explored the variation in the serum AFP level, the early variation of which seems to be correlated with long-term outcomes.17,18 Our findings confirm that patients with Child‒Pugh class B cirrhosis derive limited benefit from AB therapy, with a median OS of only 3.9 months. In this population, prognosis is predominantly driven by hepatic insufficiency rather than tumor burden, and disease management should prioritize stabilization of liver function. For some patients, exclusive palliative care may be the most appropriate approach.
Several limitations of this study should be acknowledged. The retrospective nature of the analysis may introduce selection bias, and the lack of a randomized control group limits the ability to draw definitive conclusions about the comparative efficacy of the treatment. As a retrospective study, our analysis may be subject to selection and information bias. Some clinical data were missing, and no imputation was performed, which may limit the interpretation of certain subgroup findings. Furthermore, we were unable to collect data on the Barcelona Clinic Liver Cancer (BCLC) stage, which may limit the accuracy of stratifying patient prognosis and therapeutic response. Additionally, the follow-up period, while substantial, may not comprehensively capture long-term outcomes and rare adverse events. In contrast, our study did not find a difference in outcome between patients with viral cirrhosis and those with nonviral cirrhosis, mainly because of a lack of patients. A less favourable outcome to immunotherapy for nonviral cirrhosis has been well described in the literature.18,19 Recent work from Rimini et al suggested that lenvatinib is associated with better OS and PFS for nonviral HCC patients than ABs in a large retrospective analysis.19 Furthermore, we were unable to collect data on the Barcelona Clinic Liver Cancer (BCLC) stage, which may limit the accuracy of stratifying patient prognosis and therapeutic response. Furthermore, although some patients received only one or two cycles of treatment, we chose to include all eligible patients to reflect the heterogeneity of real-world practice. This may limit the comparability with clinical trials, but improves the external validity of our findings.
Future research should focus on prospective, randomized real-world studies to further validate these findings and explore the long-term efficacy and safety of AB. Moreover, investigations into clinically useful biomarkers for response prediction and mechanisms of resistance will be crucial in optimizing patient selection and therapeutic strategies. Special attention should be given to developing and testing alternative treatments for patients with Child‒Pugh class B liver function.
Conclusion
The HIREAL study reinforced the positive effects of atezolizumab combined with bevacizumab on survival outcomes for patients with locally advanced or metastatic HCC, as demonstrated in the IMbrave150 trial. However, the limited benefit observed in patients with Child‒Pugh class B liver function and nonviral HCC highlights the need for more personalized therapeutic approaches. Future prospective studies are needed to define optimal treatment strategies for these subgroups and to investigate predictive biomarkers for treatment response.
Acknowledgment
Jean-Baptiste Barbe-Richaud and Fabien Moinard-Butot are co-first authors for this study. This paper has been uploaded to ESMO Annals of Oncology as a preprint: https://www.annalsofoncology.org/article/S0923-7534(24)00348-X/fulltext.
Funding
No funding was received for this work.
Disclosure
Dr Pascale Chiappa reports grants from MSD, Pierre Fabre, AMGEN, Merck, during the conduct of the study; grants from Merck, outside the submitted work. Professor Armand Abergel reports personal fees from ROCHE, during the conduct of the study; board member of ABBVIE, outside the submitted work. Dr Meher Ben Abdelghani reports grants from ROCHE, Pierre Fabre, servier, Novartis, and Merck, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Toh MR, Wong EYT, Wong SH, et al. Global epidemiology and genetics of hepatocellular carcinoma. Gastroenterology. 2023;164(5):
2. SPF. Estimations nationales de l’incidence et de la mortalité par cancer en France métropolitaine entre 1990 et 2018 - Tumeurs solides: Étude à partir des registres des cancers du réseau Francim [Internet]. [cité juill 14, 2024]. Disponible sur: https://www.santepubliquefrance.fr/import/estimations-nationales-de-l-incidence-et-de-la-mortalite-par-cancer-en-france-metropolitaine-entre-1990-et-2018-tumeurs-solides-etude-a-partir.
3. Brar G, Greten TF, Graubard BI, et al. Hepatocellular carcinoma survival by etiology: a SEER‐medicare database analysis. Hepatol Commun. 2020;4(10):
4. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):
5. Storandt MH, Zemla TJ, Patell K, et al. Atezolizumab plus bevacizumab as first-line systemic therapy for hepatocellular carcinoma: a multi-institutional cohort study. Oncologist. 2024;29(11):
6. D’Alessio A, Fulgenzi CAM, Nishida N, et al. Preliminary evidence of safety and tolerability of atezolizumab plus bevacizumab in patients with hepatocellular carcinoma and child-Pugh A and B cirrhosis: a real-world study. Hepatology. 2022;76(4):
7. Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):
8. Tandon P, Garcia-Tsao G. Prognostic indicators in hepatocellular carcinoma: a systematic review of 72 studies. Liver Int. 2009;29(4):
9. Cheon J, Kim H, Kim HS, et al. Atezolizumab plus bevacizumab in patients with child-Pugh B advanced hepatocellular carcinoma. Ther Adv Med Oncol. 2023;15:17588359221148541. doi:10.1177/17588359221148541
10. Tanaka T, Hiraoka A, Tada T, et al. Therapeutic efficacy of atezolizumab plus bevacizumab treatment for unresectable hepatocellular carcinoma in patients with child-Pugh class A or B liver function in real-world clinical practice. Hepatol Res. 2022;52(9):
11. Pasta A, Calabrese F, Jaffe A, et al. Safety and Efficacy of Atezolizumab/Bevacizumab in patients with hepatocellular carcinoma and impaired liver function: a systematic review and meta-analysis. Liver Cancer. 2024;13(3):
12. Rimini M, Persano M, Tada T, et al. Survival outcomes from atezolizumab plus bevacizumab versus Lenvatinib in Child Pugh B unresectable hepatocellular carcinoma patients. J Cancer Res Clin Oncol. 2023;149(10):7565–7577. doi:10.1007/s00432-023-04678-2
13. Ohama H, Hiraoka A, Tada T, et al. Comparison between atezolizumab plus bevacizumab and Lenvatinib for hepatocellular carcinoma in patients with Child-Pugh Class B in real-world clinical settings. Oncology. 2023;101(9):
14. Ochi H, Kurosaki M, Joko K, et al. Usefulness of neutrophil-to-lymphocyte ratio in predicting progression and survival outcomes after atezolizumab-bevacizumab treatment for hepatocellular carcinoma. Hepatol Res. 2023;53(1):
15. Eso Y, Takeda H, Taura K, Takai A, Takahashi K, Seno H. Pretreatment neutrophil-to-lymphocyte ratio as a predictive marker of response to atezolizumab plus bevacizumab for hepatocellular carcinoma. Curr Oncol. 2021;28(5):
16. Tada T, Kumada T, Hiraoka A, et al. Neutrophil-lymphocyte ratio predicts early outcomes in patients with unresectable hepatocellular carcinoma treated with atezolizumab plus bevacizumab: a multicenter analysis. Eur J Gastroenterol Hepatol. 2022;34(6):
17. Kelley RK, Rimassa L, Cheng AL, et al. Cabozantinib plus atezolizumab versus sorafenib for advanced hepatocellular carcinoma (COSMIC-312): a multicentre, open-label, randomised, Phase 3 trial. Lancet Oncol. 2022;23(8):
18. Mattos ÂZ, Debes JD, Vogel A, et al. Non-alcoholic fatty liver disease-related hepatocellular carcinoma: is there a role for immunotherapy? World J Gastroenterol. 2022;28(28):
19. Rimini M, Rimassa L, Ueshima K, et al. Atezolizumab plus bevacizumab versus lenvatinib or sorafenib in non-viral unresectable hepatocellular carcinoma: an international propensity score matching analysis. ESMO Open. 2022;7(6):100591. doi:10.1016/j.esmoop.2022.100591
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Retrospective Study of the Efficacy and Safety of Chemoembolization with Drug-Eluting Microspheres Combined with Intra-Arterial Infusion of Bevacizumab for Unresectable Hepatocellular Carcinoma
Ueda S, Hori S, Hori A, Makitani K, Wan K, Sonomura T
Journal of Hepatocellular Carcinoma 2022, 9:973-985
Published Date: 12 September 2022
Immune-Based Combination Therapies for Advanced Hepatocellular Carcinoma
Carloni R, Sabbioni S, Rizzo A, Ricci AD, Palloni A, Petrarota C, Cusmai A, Tavolari S, Gadaleta-Caldarola G, Brandi G
Journal of Hepatocellular Carcinoma 2023, 10:1445-1463
Published Date: 6 September 2023
Safety and Efficacy of Atezolizumab and Bevacizumab Combination as a First Line Treatment of Advanced Hepatocellular Carcinoma
Zanuso V, Pirozzi A, Balsano R, Pressiani T, Rimassa L
Journal of Hepatocellular Carcinoma 2023, 10:1689-1708
Published Date: 2 October 2023
Cost-Effectiveness and Budget Impact Analyses of Selective Internal Radiation Therapy versus Atezolizumab Plus Bevacizumab from a German Statutory Health Insurance Perspective
Schwander B, Klesper K, Rossol S, Herrmann K, Zoellner YF
ClinicoEconomics and Outcomes Research 2024, 16:483-492
Published Date: 6 June 2024
Transarterial Chemoembolization Combined with Atezolizumab Plus Bevacizumab versus Transarterial Chemoembolization Alone in Intermediate‐stage Hepatocellular Carcinoma: A Multicenter Retrospective Study
Zheng Y, Xiang Y, Shi H, Lin Z, Cheng S, Zhu J
Journal of Hepatocellular Carcinoma 2024, 11:1079-1093
Published Date: 12 June 2024