")
Back to Journals » Journal of Inflammation Research » Volume 18
Rheumatoid Arthritis Aggravates Disease Severity and the Risk of Postoperative Recurrence in Chronic Rhinosinusitis
Authors Zhou X, Wang D, Cao S, Tu Y, Chen R, Huang H, Lou W
Received 30 April 2025
Accepted for publication 11 July 2025
Published 16 July 2025 Volume 2025:18 Pages 9401—9411
DOI https://doi.org/10.2147/JIR.S533652
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ujjwol Risal
Xiaoying Zhou,1,* Dan Wang,2,* Shouming Cao,1 Yi Tu,1 Rui Chen,1 Haosu Huang,1 Wenrong Lou3
1Department of Otolaryngology-Head and Neck Surgery, The Second Affiliated Hospital of Kunming Medical University, Kunming, People’s Republic of China; 2Department of Algology, The Second Affiliated Hospital of Kunming Medical University, Kunming, People’s Republic of China; 3Department of Otolaryngology-Head and Neck Surgery, The Affiliated Yan’an Hospital of Kunming Medical University, Kunming, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenrong Lou, Department of Otolaryngology-Head and Neck Surgery, The Affiliated Yan’an Hospital of Kunming Medical University, Kunming, 650051, People’s Republic of China, Email [email protected]
Objective: Rheumatoid arthritis (RA) may share pathophysiological mechanisms with chronic rhinosinusitis (CRS), but its impact on CRS remains unclear. This study aimed to investigate the associations between RA and CRS disease severity, as well as postoperative recurrence risk.
Methods: A retrospective analysis was conducted on CRS patients who underwent functional endoscopic sinus surgery. Patients were divided into subgroups based on the presence of RA and gender. CRS patients were followed up for three years and categorized into non-recurrent and recurrent groups. Binary logistic regression analyses were performed to investigate the impact of RA on the risk of postoperative recurrence in CRS.
Results: Among 568 CRS patients, 169 experienced recurrence after three years. The RA group showed a significantly higher recurrence rate than the non-RA group in both genders (P < 0.05). In addition, RA patients had younger age, higher body mass index, higher prevalence of nasal polyps, and higher baseline VAS, Lund-Kennedy, and Lund-Mackay scores. At three-year follow-up, the RA group demonstrated greater improvements in VAS and Lund-Kennedy scores (P < 0.05). Logistic regression identified RA, allergic rhinitis, and asthma as independent risk factors for CRS recurrence (P < 0.05). Unadjusted and adjusted analysis highlighted RA as an independent predictor in males and females. Kaplan-Meier analysis further revealed that RA was associated with a significantly higher risk of postoperative CRS recurrence (P < 0.05).
Conclusion: RA might aggravate the disease severity and affect the prognosis of CRS. Additionally, RA may be a potential risk factor for postoperative recurrence of CRS, regardless of gender.
Keywords: chronic rhinosinusitis, functional endoscopic sinus surgery, recurrence, rheumatoid arthritis
Introduction
Chronic rhinosinusitis (CRS) is a common inflammatory disorder characterized by chronic inflammation in the nasal and paranasal sinus mucosa.1,2 CRS, being a multifactorial condition, entails intricate interplays among environmental, genetic, and immunological factors.3,4 It presents through a variety of clinical symptoms and includes different subtypes, including chronic rhinosinusitis with nasal polyps (CRSwNP) and chronic rhinosinusitis without nasal polyps (CRSsNP).5 To date, there have been significant advancements in the diagnosis and treatment of CRS, placing emphasis on comprehensive clinical evaluation, endoscopic examination, imaging studies, and targeted medical and surgical interventions.6,7 Notably, functional endoscopic sinus surgery (FESS) has become the primary treatment modality for CRS patients who do not experience adequate improvement with medical therapy.8 However, despite these treatment advancements, postoperative recurrence continues to pose a significant challenge in the management of CRS.9,10 Therefore, exploring the factors influencing postoperative recurrence and discovering the underlying recurrent mechanisms are crucial for improving personalized treatment for CRS patients.11,12 Several potential risk factors have been identified, including age, sex, duration of CRS, and surgical techniques.8,13 Furthermore, concurrent conditions like asthma, allergic rhinitis, and immunodeficiency are increasingly acknowledged as significant contributors to the recurrence of CRS.14,15 However, there are no reliable biomarkers used in clinical practice for predicting the risk of postoperative recurrence, and the underlying mechanisms of recurrence remain poorly elucidated.
In recent years, with the increasing incidence of rheumatoid arthritis (RA) and the exploration of disease pathophysiology, researchers have found an association between RA and CRS.16–20 RA is associated with systemic inflammation and immune dysregulation, potentially impacting various organ systems beyond the joints.21,22 Previous studies have suggested a possible link between RA and CRS, with both conditions often coexisting in patients.16–18 Furthermore, growing evidence indicates that CRS and RA may share common pathophysiological mechanisms.19,20,23 A nationwide population-based cohort study found that CRS may be associated with an increased risk of subsequent RA events, regardless of the phenotype.24 Mendelian randomization analysis also suggested a genetically causal effect of CRS on the incidence of RA, with a significantly higher risk of RA in individuals with CRS.25 Unfortunately, the current understanding of the association between RA and pathophysiology and prognosis of CRS recurrence is limited. Given the overlapping inflammatory pathways, it is plausible that CRS patients with RA may exhibit more complex histopathological features, more severe clinical symptoms, and a higher risk of postoperative recurrence.
This study seeks to evaluate the impact of RA on CRS by examining the clinical characteristics and surgical outcomes of CRS patients with RA. Our objective is to provide valuable insights into the potential association between RA and disease severity, as well as the increased risk of CRS recurrence. Understanding the interplay between these conditions could guide the optimization of treatment strategies and improve postoperative management for this patient population.
Materials and Methods
Patients and Study Design
The present study was approved by the Human Ethical Committee of The Second Affiliated Hospital of Kunming Medical University (No.20230733). Given the retrospective design, use of de-identified data, and absence of any intervention or commercial intent, the requirement for informed consent was waived. This study complies with the Declaration of Helsinki. CRS patients who were treated with FESS at our center from January 2018 to December 2021 were included in this retrospective study. All patients were diagnosed with CRS based on established clinical guidelines, requiring ≥12 weeks of symptoms such as nasal obstruction or nasal discharge, supported by endoscopic signs or CT evidence of sinus inflammation.26 Functional endoscopic sinus surgery (FESS) was performed in cases where medical treatment had failed. Inclusion criteria were as follows: 1) age > 18 years and < 60 years; 2) complete clinical data; 3) no history of prior nasal surgery. Exclusion criteria were as follows: 1) concurrent malignancy or other severe systemic diseases; 2) major psychiatric disorders (eg, schizophrenia, bipolar disorder, or severe depression with cognitive impairment); 3) fungal sinusitis, allergic fungal sinusitis, postoperative ethmoid sinus polyposis, cystic fibrosis; 4) withdrawal or loss to follow-up during the follow-up period; 5) systemic use of glucocorticoids and antibiotics within 1 month prior to surgery; 6) severe concomitant diseases not meeting surgical requirements.
Clinical Data Collection and Group Settings
Baseline data were obtained from electronic medical records of all CRS patients, including gender, age, smoking status, alcohol consumption, body mass index (BMI), duration of CRS, presence of RA, hypertension, and diabetes, fasting blood glucose (FBG) levels, systolic blood pressure (SBP), diastolic blood pressure (DBP), allergic rhinitis, asthma, and CRS phenotype. Furthermore, preoperative symptoms were evaluated through interviews utilizing visual analogue scales (VAS), Lund-Kennedy scales, and Lund-Mackay scales as previously described.27,28 BMI was calculated as weight (in kilograms) divided by height (in meters) squared. Diagnoses of hypertension, diabetes, allergic rhinitis, and asthma were established based on prior specialty consultations, medication records, and adherence to the latest diagnostic criteria. RA was defined according to the 2010 ACR/EULAR classification criteria, with a total score of ≥6.22 Considering the impact of gender on RA, CRS patients were divided into non-RA and RA groups based on gender. Comparisons of variables between these groups were conducted separately for male and female patients.
Postoperative Management and Follow-up
All patients received FESS under the same medical team and were managed according to a standardized postoperative management schedule, including antibiotic use, intranasal corticosteroid spray, saline irrigation, and sinus cavity clearance as previously described.27,28 All patients included in the study were followed up for a minimum of 3 years, with scheduled outpatient visits at 2 weeks, 1 month, 3 months, and then every six months after the first year postoperatively. Nasal endoscopy and/or CT scans were performed as necessary to assess postoperative status. The follow-up endpoint was defined as either recurrence or completion of the 3-year period. Diagnosis of CRS recurrence was established based on patients’ clinical symptoms, physical examination findings, nasal endoscopy results, and sinus CT scan results. Postoperative recurrence was defined in accordance with previous literature as the reappearance of clinical symptoms along with endoscopic and CT evidence persisting for at least 2 months, despite treatment with previously described antibiotics and oral steroids.29,30 At the final follow-up, the VAS and Lund-Kennedy scores were collected again and compared with their baseline levels in CRS patients. The difference between the final follow-up scores and baseline scores was recorded as the improvement of VAS and Lund-Kennedy scores.
Statistical Analysis
Categorical variables were presented as numbers and percentages and compared using the chi-square test. Normally distributed quantitative variables were expressed as mean ± standard deviation and compared between groups using Student’s t-test. Non-normally distributed data were presented as median and interquartile range (IQR) and compared using the Mann–Whitney U-test. Interaction was assessed using multifactorial analysis of variance, revealing a significant interaction among gender, RA, and CRS recurrence rate. Consequently, all analyses were stratified by gender. Patients were divided into non-RA and RA groups to explore differences in clinical characteristics between the two groups. Furthermore, patients were divided into non-recurrent CRS and recurrent CRS groups, and logistic regression analysis was conducted to explore factors influencing CRS postoperative recurrence. The relationship between RA and CRS recurrence risk was further investigated in different adjustment models. Kaplan-Meier curve analysis was performed to evaluate the association between the presence of RA and the risk of postoperative recurrence of CRS. Significance was accepted at a two-tailed P < 0.05. Statistical analyses were conducted using SPSS version 23.0 (IBM, Chicago, IL, USA).
Results
Clinical Data of CRS Patients with Different Characteristics
A total of 652 patients with CRS were initially enrolled in the study. During the three-year follow-up period, 84 patients were lost to follow-up, resulting in 568 eligible participants included in the final analysis. Among them, 366 were male and 202 were female. The baseline characteristics of the study population are displayed in Table 1. Among them, 169 patients were determined to suffer postoperative recurrence. Upon initial gender-based stratification, it was observed that male patients had notably higher rates of alcohol consumption and smoking compared to female patients. Conversely, female patients were found to have a higher prevalence of comorbid RA (P < 0.05). Subsequently, we further categorized individuals based on gender and the presence of RA to compare postoperative recurrence rates and clinical characteristics. As shown in Table 2, regardless of gender, the recurrence rate of CRS in the RA group was significantly higher in comparison with the non-RA group (P < 0.05). Moreover, in comparison to the non-RA group, the RA group demonstrated a significantly younger age, higher BMI, and a greater prevalence of CRSwNP in both genders (P < 0.05).
 |
Table 1 Baseline Characteristics of CRS Patients in Male and Female |
 |
Table 2 Baseline Demographics and Clinical Characteristics Between Non-RA and RA Groups in Both Genders |
RA Exacerbated the Disease Severity and Affected the Prognosis of CRS
To investigate the effects of RA on disease severity, we compared VAS, Lund-Kennedy, and Lund-Mackay scores in different groups based on the presence of RA and gender. As depicted in Figure 1, the baseline VAS, Lund-Kennedy, and Lund-Mackay scores were notably higher in the RA group compared to the non-RA group, regardless of gender (P < 0.05). Additionally, we collected VAS and Lund-Kennedy scores of CRS patients at their final follow-up and compared them with their baseline levels. As illustrated in Figure 2, the improvement of VAS and Lund-Kennedy scores in the RA group was significantly lower compared to the non-RA group in both genders (P < 0.05). All these findings collectively suggest that the presence of RA may exacerbate the severity of CRS in patients, impacting both the improvement of symptoms and disease control postoperatively.
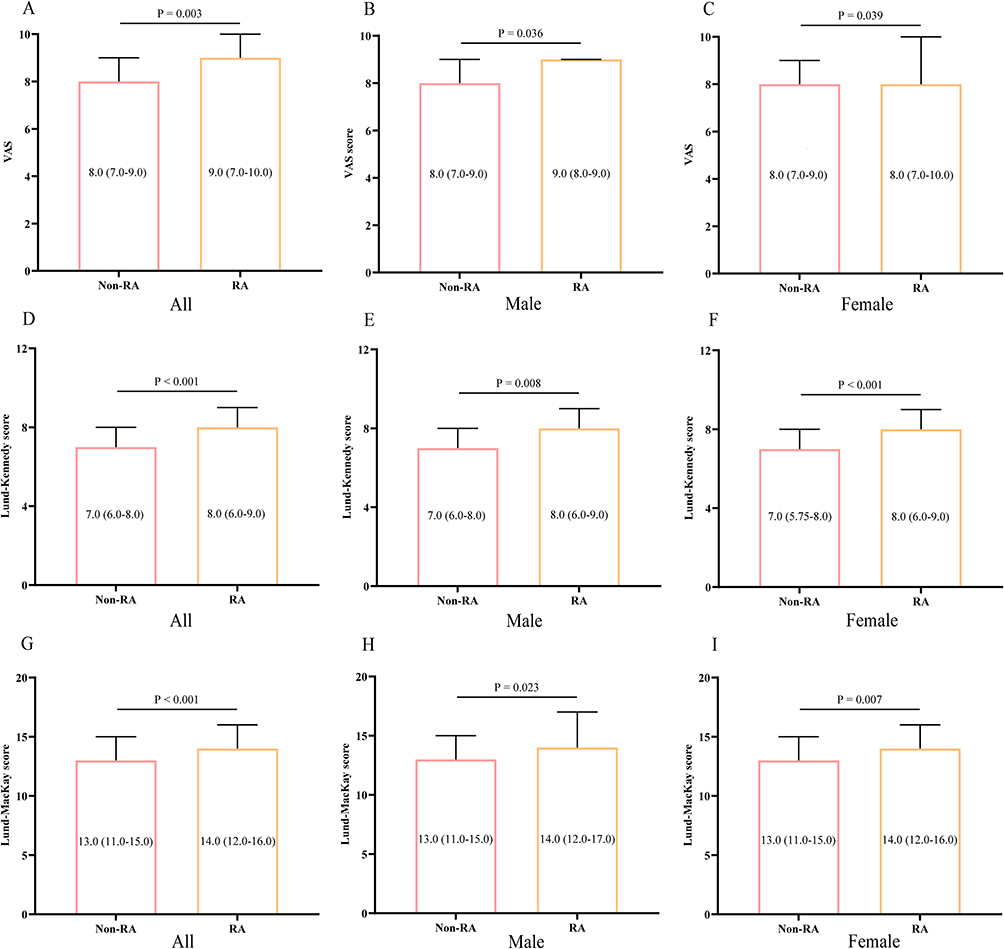 |
Figure 1 Comparison of baseline scores of different symptom scales between non-RA group and RA group in both male and female CRS patients. (A–C) VAS score; (D–F) Lund-Kennedy score; (G–I) Lund-Mackay score. Data are presented as median (IQR). Abbreviations: VAS, visual analogue scale; RA, rheumatoid arthritis; CRS, chronic rhinosinusitis. |
 |
Figure 2 The improvements of VAS and Lund-Kennedy scores in male and female CRS patients after 3 years of follow-up. (A–C) VAS score; (D–F) Lund-Kennedy score. Data are presented as median (IQR). T0: baseline; T3: 3 years after surgery. Abbreviations: VAS, visual analogue scale; RA, rheumatoid arthritis; CRS, chronic rhinosinusitis. |
RA Increased the Risk of Postoperative Recurrence of CRS
To explore potential factors influencing the postoperative recurrence of CRS, we stratified patients into recurrent CRS and non-recurrent CRS groups by gender. As depicted in Table 3, logistic regression analysis revealed that in both male and female CRS patients, RA, allergic rhinitis, and asthma were associated with an elevated risk of postoperative recurrence (P < 0.05). To delve deeper into the relationship between RA and postoperative recurrence risk in CRS, we conducted unadjusted and adjusted logistic regression model analyses, as shown in Table 4. The results indicated a significant association between RA and an increased risk of postoperative recurrence in both male and female CRS patients, with this risk remaining independent after adjusting for potential confounders (P < 0.05). Furthermore, Kaplan-Meier curve analysis illustrated that the presence of RA was correlated with a heightened risk of postoperative recurrence in CRS patients of both genders (P < 0.05, Figure 3).
 |
Table 3 Logistic Regression Analysis of Potential Risk Factor of Postoperative Recurrence of CRS in Both Genders |
 |
Table 4 Unadjusted and Adjusted Binary Logistic Regression Analysis for CRS Recurrence According to RA |
 |
Figure 3 Kaplan-Meier curve analyzing the association between RA and the risk of postoperative recurrence of CRS. (A) all patients; (B) male; (C) female. Abbreviations: RA, rheumatoid arthritis; CRS, chronic rhinosinusitis. |
Discussion
In recent years, with improved understanding of the pathology of CRS and advancements in assessment methods, increasing evidence confirms CRS as a highly heterogeneous disease with significant variations in disease severity.31,32 Despite advancements in treatment modalities and the standardization of postoperative management and follow-up, a considerable proportion of patients still experience postoperative recurrence during follow-up, imposing heavy economic burdens and psychological distress on patients.8,29 The intricate nature of tissue heterogeneity and the uncertainty regarding the etiology of postoperative recurrence highlight the need for a macroscopic differentiation of CRS patients based on diverse clinical characteristics and accompanying diseases.33,34 This differentiation is crucial for enabling precise treatment approaches. Previous studies have revealed significant differences in disease severity, tissue pathology, and postoperative recurrence risk among CRS patients with different accompanying diseases.30,35,36 For example, CRS patients with obesity or hyperuricemia exhibit profoundly aggravated tissue inflammation and a significantly increased risk of postoperative recurrence.30,35 These findings underscore the importance of summarizing and synthesizing the disease characteristics of CRS patients with different demographics and accompanying diseases, thereby enabling personalized treatment approaches.
To the best of our knowledge, this study represents the first exploration of the association between RA and clinical characteristics, as well as postoperative recurrence of CRS, in a large-scale cohort. Our findings indicate that both male and female CRS patients with accompanying RA exhibit greater disease severity and poorer prognosis. Importantly, the postoperative recurrence rate of CRS patients with RA was significantly higher than that of those without RA over the 3-year follow-up period, irrespective of gender. This association remained significant even after adjusting for other potential risk factors. These results suggest that RA may influence the tissue pathology of CRS and contribute to its postoperative recurrence mechanisms.
As the exploration of the immunopathological mechanisms of CRS continues to deepen, researchers have progressively discovered the involvement of autoimmunity in the nasal inflammation.37 In recent years, there has been increasing attention to the relationship between autoimmune diseases and CRS, including RA, systemic lupus erythematosus and Sjogren’s syndrome.24,38 Emerging evidence suggest a potential overlap in the pathophysiological mechanisms between CRS and autoimmune diseases, with both often coexisting in patients.17,20,21,25 A recently published study has revealed a genetic link between CRS and the onset of RA.25 However, the impact of RA on CRS, particularly in terms of disease severity and postoperative recurrence, remains largely unexplored. This study aims to fill this gap by analyzing a large sample size of CRS cases, thereby confirming RA as a significant risk factor for CRS recurrence. Additionally, our findings suggest that CRS patients with RA tend to experience more severe symptoms and poorer prognoses, highlighting the contribution of RA to the complexity and diversity of CRS immunopathological mechanisms.
It’s widely recognized that recurrent CRS is primarily driven by the severe infiltration of inflammatory cells and the excessive accumulation of pro-inflammatory cytokines within the nasal mucosa.39,40 Immune and inflammatory processes play pivotal roles in the link between RA and CRS.24 RA, being a systemic autoimmune condition, frequently leads to an overactive immune system in affected individuals.41 This heightened immune activity often involves dysregulation of T cells and B cells, which are integral to orchestrating inflammatory mediator release, immune responses, as well as the generation of autoantibodies and the deposition of immune complexes.42,43 Prior research has indicated that the aberrant activation and infiltration of T cells and B cells, along with their cytokines, play significant roles in perpetuating inflammation and recurrence in CRS patients.39,43 Emerging evidence suggests that RA-related autoantibodies, including anti-citrullinated protein antibodies (ACPA), can damage nasal epithelial cells and promote the release of pro-inflammatory mediators such as IL-6, IL-1β, and IL-8, thereby activating downstream immune responses.44,45 Furthermore, the production of autoantibodies and the systemic dissemination of local ACPA could exacerbate persistent mucosal inflammation and bacterial dysbiosis.24,38 This chronic state of mucosal inflammation and microbiota dysbiosis are crucial in the progression and recurrence of CRS.46 Chronic inflammatory conditions observed in RA patients reportedly contribute to epithelial barrier dysfunction, triggering tissue epithelial-mesenchymal transition (EMT) and pathological fibrosis.47 However, it’s crucial to note that tissue EMT and fibrosis play significant roles in the pathophysiology of CRS and are crucial factors influencing its prognosis and recurrence.48 Moreover, immunomodulatory treatments commonly used in the management of RA, including immunosuppressants and biologics, directly affect the immune system and inflammatory responses.42 Although these treatments may alleviate abnormal immune activity and reduce the release of inflammatory mediators, long-term use may suppress immune responses, impairing the body’s normal immune reactions and reducing the nasal mucosa’s innate immune capability.17,39 This increases the risk of bacterial and viral infections, detrimentally impacting the prognosis of CRS and increasing the risk of postoperative recurrence. In summary, the influence of RA on CRS encompasses several dimensions, such as immune dysregulation, epithelial inflammation, remodeling, and treatment approaches. A deeper comprehension of these contributing factors is imperative for a more comprehensive assessment and treatment of CRS patients with RA, ultimately enhancing treatment efficacy and prognosis.
Regarding sex differences observed in RA, it predominantly affects females, with a male-to-female ratio of approximately 1:3.22,49 By summarizing and analyzing the clinical characteristics and prognosis of CRS patients with and without RA in different gender groups, we observed significant differences between the RA and non-RA groups, as well as among different gender groups. After stratifying by gender, we found that the impact of RA on the severity, prognosis, and recurrence of CRS showed no significant correlation with gender, aiming to establish more reliable conclusions. Therefore, preoperative RA treatment and individualized management for CRS patients with concomitant RA can contribute to improving prognosis and achieving precision treatment for this patient population.
This study has several limitations. Firstly, the patients included in this retrospective study were from a single medical center, which may lead to selection bias and limit the generalizability of the results to a broader population. Secondly, baseline information regarding RA disease activity and specific medication use was not available. Since different treatment modalities for RA, such as corticosteroids, conventional DMARDs, or biologics, may modulate systemic and local immune responses, their absence from the analysis may introduce potential confounding and limit interpretation of the observed associations. Thirdly, part of the study period overlapped with the COVID-19 pandemic, during which access to healthcare services and follow-up protocols may have been affected. Finally, there may be other unknown or unmeasured factors that could contribute to the risk of postoperative recurrence, which were not considered in this study.
Conclusion
This study contributes to a better understanding of the relationship RA and chronic CRS. Our findings suggest that RA might aggravate CRS severity and may influence its prognosis. Furthermore, RA could be a potential risk factor for postoperative recurrence of CRS, regardless of gender. These insights may have clinical relevance in the preoperative management of CRS patients with RA, supporting the need for more personalized treatment approaches. Further research is warranted to elucidate the intricate interplay between RA and CRS and its implications for clinical management.
Abbreviations
RA, Rheumatoid Arthritis; CRS, Chronic Rhinosinusitis; CRSwNP, Chronic Rhinosinusitis with Nasal Polyps; CRSsNP, Chronic Rhinosinusitis without Nasal Polyps; FESS, Functional Endoscopic Sinus Surgery; BMI, Body Mass Index; FBG, Fasting Blood Glucose; SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure; VAS, Visual Analogue Scale; EMT, Epithelial-Mesenchymal Transition; ACPA, Anti-Citrullinated Protein Antibody; CT, Computed Tomography; IQR, Interquartile Range; SPSS, Statistical Package for the Social Sciences; ACR/EULAR, American College of Rheumatology/European League Against Rheumatism.
Funding
This work was supported by the Kunming Health Science and Technology Personnel Training Project, medical science and technology discipline reserve personnel training plan [2023-sw (reserve)-03].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sedaghat AR, Campbell RG, Douglas RG, et al. Outcome measures for chronic rhinosinusitis with nasal polyps. Rhinology. 2024;62(34):1–37. doi:10.4193/Rhin24.090
2. Fokkens WJ, Sedaghat AR, Soyka MB, Reitsma S. Recent advances in chronic rhinosinusitis: pathophysiology, treatments, and outcome measures. Rhinology. 2024;62(6):652–658. doi:10.4193/Rhin24.801
3. Porras-Gonzalez C, Palacios-Garcia JM, Sanchez-Gomez S, et al. Transcriptional analysis of nasal polyps fibroblasts reveals a new source of pro-inflammatory signaling in CRSwNP. Rhinology. 2023;61(2):180–189. doi:10.4193/Rhin22.309
4. Fokkens WJ, Viskens AS, Backer V, et al. EPOS/EUFOREA update on indication and evaluation of biologics in chronic rhinosinusitis with nasal polyps 2023. Rhinology. 2023;61(3):194–202. doi:10.4193/Rhin22.489
5. Chapurin N, Wu J, Labby AB, Chandra RK, Chowdhury NI, Turner JH. Current insight into treatment of chronic rhinosinusitis: phenotypes, endotypes, and implications for targeted therapeutics. J Allergy Clin Immunol. 2022;150(1):22–32. doi:10.1016/j.jaci.2022.04.013
6. Hernaiz-Leonardo JC, Alim BM, Pascual A, et al. Development and validation of the Sinonasal Endoscopic Score (SiNES) for chronic rhinosinusitis. Rhinology. 2024;62(4):480–487. doi:10.4193/Rhin23.434
7. Backaert W, Steelant B, Wils T, et al. Nasal hyperreactivity in allergic rhinitis and chronic rhinosinusitis with polyps: a role for neuronal pathways. Rhinology. 2024;62(3):299–309. doi:10.4193/Rhin23.287
8. Bai J, Huang JH, Price CPE, et al. Prognostic factors for polyp recurrence in chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol. 2022;150(2):352–361.e357. doi:10.1016/j.jaci.2022.02.029
9. Wautlet A, Bachert C, Desrosiers M, Hellings PW, Peters AT. The management of chronic rhinosinusitis with nasal polyps (CRSwNP) with biologics. J Allergy Clin Immunol Pract. 2023;11(9):2642–2651. doi:10.1016/j.jaip.2023.04.054
10. Wu PW, Chiu CH, Huang YL, et al. Tissue eosinophilia and computed tomography features in paediatric chronic rhinosinusitis with nasal polyps requiring revision surgery. Rhinology. 2023;61(3):348–357. doi:10.4193/Rhin22.435
11. Shah SA, Kobayashi M. Pathogenesis of chronic rhinosinusitis with nasal polyp and a prominent T2 endotype. Heliyon. 2023;9(9):e19249. doi:10.1016/j.heliyon.2023.e19249
12. Zhu KZ, He C, Li Z, et al. Development and multicenter validation of a novel radiomics-based model for identifying eosinophilic chronic rhinosinusitis with nasal polyps. Rhinology. 2023;61(2):132–143. doi:10.4193/Rhin22.361
13. Cai S, Lou H, Zhang L. Prognostic factors for post-operative outcomes in chronic rhinosinusitis with nasal polyps: a systematic review. Expert Rev Clin Immunol. 2023;19(8):867–881. doi:10.1080/1744666X.2023.2218089
14. Bajpai S, Marino MJ, Rank MA, Donaldson AM, O’Brien EK, Lal D. Benefits of biologic therapy administered for asthma on co-existent chronic rhinosinusitis: a real-world study. Int Forum Allergy Rhinol. 2021;11(8):1152–1161. doi:10.1002/alr.22774
15. Geng B, Dilley M, Anterasian C. Biologic therapies for allergic rhinitis and nasal polyposis. Curr Allergy Asthma Rep. 2021;21(6):36. doi:10.1007/s11882-021-01013-y
16. Chandra RK, Lin D, Tan B, et al. Chronic rhinosinusitis in the setting of other chronic inflammatory diseases. Am J Otolaryngol. 2011;32(5):388–391. doi:10.1016/j.amjoto.2010.07.013
17. Kronzer VL, Huang W, Zaccardelli A, et al. Association of sinusitis and upper respiratory tract diseases with incident rheumatoid arthritis: a case-control study. J Rheumatol. 2022;49(4):358–364. doi:10.3899/jrheum.210580
18. Reckner Olsson A, Skogh T, Wingren G. Comorbidity and lifestyle, reproductive factors, and environmental exposures associated with rheumatoid arthritis. Ann Rheum Dis. 2001;60(10):934–939. doi:10.1136/ard.60.10.934
19. Shih LC, Hsieh HH, Tsay GJ, et al. Chronic rhinosinusitis and premorbid autoimmune diseases: a population-based case-control study. Sci Rep. 2020;10(1):18635. doi:10.1038/s41598-020-75815-x
20. Kronzer VL, Davis JM, Hanson AC, et al. Association between sinusitis and incident rheumatic diseases: a population-based study. RMD Open. 2024;10(1):e003622. doi:10.1136/rmdopen-2023-003622
21. Hajiesmaeili Y, Tamhankar P, Stranges S, Barra L. Factors associated with incident cardiovascular disease in patients with rheumatoid arthritis: a scoping review. Autoimmun Rev. 2024;23(5):103539. doi:10.1016/j.autrev.2024.103539
22. Kay J, Upchurch KS. ACR/EULAR 2010 rheumatoid arthritis classification criteria. Rheumatology. 2012;51(suppl 6):vi5–9. doi:10.1093/rheumatology/kes279
23. Chen S, Tan L, Qin D, et al. The causal relationship between multiple autoimmune diseases and nasal polyps. Front Immunol. 2023;14:1228226. doi:10.3389/fimmu.2023.1228226
24. Lee IH, Yang HG, Ha SS, Son GM, DW K, DK K. Effect of chronic rhinosinusitis on the risk of development of rheumatoid arthritis. Allergy Asthma Immunol Res. 2023;15(5):647–658. doi:10.4168/aair.2023.15.5.647
25. Dong Y, Ding W, Song K, Li F. Higher risk of rheumatoid arthritis in patients with chronic rhinosinusitis: prospective association in the U.K. biobank and genetic evidence by Mendelian randomization analysis. Am J Rhinol Allergy. 2024;38(2):82–91. doi:10.1177/19458924231225488
26. Fokkens WJ, Lund VJ, Mullol J, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50(1):1–12. doi:10.4193/Rhino12.000
27. de Loos DAE D, Cornet ME, Hopkins C, Fokkens WJ, Reitsma S. Measuring control of disease in chronic rhinosinusitis; assessing the correlation between sinonasal outcome Test-22 and visual analogue scale item scores. Rhinology. 2023;61(1):39–46. doi:10.4193/Rhin21.275
28. Sedaghat AR, Fokkens WJ, Lund VJ, et al. Consensus criteria for chronic rhinosinusitis disease control: an international delphi study. Rhinology. 2023;61(6):519–530. doi:10.4193/Rhin23.335
29. Brescia G, Contro G, Giacomelli L, Barion U, Frigo AC, Marioni G. Blood eosinophilic and basophilic trends in recurring and non-recurring eosinophilic rhinosinusitis with nasal polyps. Am J Rhinol Allergy. 2021;35(3):296–301. doi:10.1177/1945892420953960
30. Xie S, Zhang C, Xie Z, Zhang J, Zhang H, Jiang W. Serum metabolomics identifies uric acid as a possible novel biomarker for predicting recurrence of chronic rhinosinusitis with nasal polyps. Rhinology. 2023;61(6):541–551. doi:10.4193/Rhin23.236
31. Yilmaz G, Eyigor H, Gur OE, et al. The role of TAS2R38 genotype in surgical outcomes and culturable bacteria in chronic rhinosinusitis with or without nasal polyps. Rhinology. 2023;61(1):54–60. doi:10.4193/Rhin22.118
32. Hellings PW, Fokkens WJ, Orlandi R, et al. The EUFOREA pocket guide for chronic rhinosinusitis. Rhinology. 2023;61(1):85–89. doi:10.4193/Rhin22.344
33. Jo S, Lee SH, Jo HR, et al. Eosinophil-derived TGFβ1 controls the new bone formation in chronic rhinosinusitis with nasal polyps. Rhinology. 2023;61(4):338–347. doi:10.4193/Rhin22.439
34. Xu X, Seet JE, Yap QV, et al. Latent class analysis of structured histopathology in prognosticating surgical outcomes of chronic rhinosinusitis with nasal polyps in Singapore. Rhinology. 2023;61(4):358–367. doi:10.4193/Rhin22.455
35. Xie S, Jiang S, Fan R, et al. Elevated body mass index increased the risk of recurrence in Chinese patients with chronic rhinosinusitis. Am J Otolaryngol. 2023;44(4):103841. doi:10.1016/j.amjoto.2023.103841
36. Nakayama T, Haruna SI. A review of current biomarkers in chronic rhinosinusitis with or without nasal polyps. Expert Rev Clin Immunol. 2023;19(8):883–892. doi:10.1080/1744666X.2023.2200164
37. Fiorelli D, Francavilla B, Velletrani G, et al. Autoantibody profiles assessment in individuals with persistent olfactory impairment following SARS-CoV-2 infection. Int Immunopharmacol. 2024;129:111599. doi:10.1016/j.intimp.2024.111599
38. Lee IH, Kim DK. Relationship of chronic rhinosinusitis with Sjogren’s syndrome, systemic lupus erythematosus, and ankylosing spondylitis. Rhinology. 2023;61(2):124–131. doi:10.4193/Rhin22.300
39. Czerwaty K, Piszczatowska K, Brzost J, Ludwig N, Szczepański MJ, Dżaman K. Immunological aspects of chronic rhinosinusitis. Diagnostics. 2022;12(10).
40. Cakir Cetin A, Tuncok Y, Keskinoglu P, Arici MA, Onen F, Ecevit MC. Methotrexate for recurrent chronic rhinosinusitis with nasal polyps: a randomized controlled Phase II clinical trial. Int Forum Allergy Rhinol. 2022.
41. van Steenbergen HW, Cope AP, van der Helm-van Mil AHM. Rheumatoid arthritis prevention in arthralgia: fantasy or reality? Nat Rev Rheumatol. 2023;19(12):767–777. doi:10.1038/s41584-023-01035-y
42. Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016;388(10055):2023–2038. doi:10.1016/S0140-6736(16)30173-8
43. Yang M, Zhu L. Osteoimmunology: the crosstalk between T cells, B cells, and osteoclasts in rheumatoid arthritis. Int J Mol Sci. 2024;25(5).
44. Holers VM, Demoruelle MK, Kuhn KA, et al. Rheumatoid arthritis and the mucosal origins hypothesis: protection turns to destruction. Nat Rev Rheumatol. 2018;14(9):542–557. doi:10.1038/s41584-018-0070-0
45. Cergan R, Berghi O, Dumitru M, et al. Interleukin 8 molecular interplay in allergic rhinitis and chronic rhinosinusitis with nasal polyps: a scoping review. Life. 2025;15(3).
46. Zhao Y, Chen J, Hao Y, et al. Predicting the recurrence of chronic rhinosinusitis with nasal polyps using nasal microbiota. Allergy. 2022;77(2):540–549. doi:10.1111/all.15168
47. Sarrand J, Soyfoo MS. Involvement of epithelial-mesenchymal transition (EMT) in autoimmune diseases. Int J Mol Sci. 2023;24(19):14481. doi:10.3390/ijms241914481
48. Wu Y, Sun K, Tu Y, et al. miR-200a-3p regulates epithelial-mesenchymal transition and inflammation in chronic rhinosinusitis with nasal polyps by targeting ZEB1 via ERK/p38 pathway. Int Forum Allergy Rhinol. 2024;14(1):41–56. doi:10.1002/alr.23215
49. Hafkenscheid L, de Moel E, Smolik I, et al. N-linked glycans in the variable domain of IgG anti-citrullinated protein antibodies predict the development of rheumatoid arthritis. Arthritis Rheumatol. 2019;71(10):1626–1633. doi:10.1002/art.40920
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hyperuricemia Increases the Risk of Postoperative Recurrence in Chinese Patients with Chronic Rhinosinusitis
Jiang S, Xie S, Xie Z, Jiang W, Zhang H
Journal of Inflammation Research 2024, 17:2669-2679
Published Date: 1 May 2024