")
Back to Journals » Journal of Inflammation Research » Volume 17
Rheumatoid Factor Titer as an Indicator of the Risk of Rheumatoid Arthritis Activity: Dose–Effect Analysis with the Restricted Cubic Spline Model
Authors Peng XC, Yin R, Luo LP, Xu S, Shuai Z
Received 25 July 2024
Accepted for publication 3 December 2024
Published 10 December 2024 Volume 2024:17 Pages 10699—10709
DOI https://doi.org/10.2147/JIR.S488605
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Xin-Chen Peng, Ruoyanran Yin, Li-Ping Luo, Shengqian Xu, Zongwen Shuai
Department of Rheumatology and Immunology, The First Affiliated Hospital of Anhui Medical University, Hefei, 230022, People’s Republic of China
Correspondence: Shengqian Xu; Zongwen Shuai, Email [email protected]; [email protected]
Background: Rheumatoid factor (RF) titer is known to be correlated to rheumatoid arthritis (RA) activity, but the ideal cut-off titer of RF remains unclear. Here, the relationship between RF titer and RA activity was investigated in order to determine the ideal RF value indicative of the risk of RA activity.
Methods: Clinical data from 2044 eligible patients were collected from the First Affiliated Hospital of Anhui Medical University from February 2022 to October 2023. A restricted cubic spline (RCS) model was used to evaluate the relationship between RF titer and RA activity.
Results: Data from a total of 2044 patients with RA were collected and analyzed. Multivariate logistic regression analysis revealed that higher RF levels were significant predictors of the risk of RA activity calculated according to the disease activity score 28 (DAS28)-erythrocyte sedimentation rate (ESR) (OR = 2.020, 95% CI = 1.457– 2.801, P < 0.001) and DAS28-C reactive protein (CRP) (OR = 1.526, 95% CI = 1.092– 2.131, P = 0.013), after the results were adjusted for potential covariates. The relationship between log2RF and the risk of RA activity was non‑linear in the RCS model (P < 0.05). The cutoff value of RF titers for determining the risk of RA activity was 65.80 IU/mL. When RF exceeded the cutoff value, the risk of RA activity based on DAS28-ESR increased by 99.2% and the risk of RA activity based on DAS28-CRP increased by 62.8% (P < 0.001).
Conclusion: The risk of RA activity increased non-linearly with the continuous change in RF titer.
Keywords: rheumatoid factor, rheumatoid arthritis, restricted cubic spline, disease activity score 28, dose–effect analysis
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disease associated with systemic inflammation and erosive and symmetrical polyarthritis.1 RA is more common in women and is predominantly in middle-aged individuals.2 The number of new cases of RA reported is increasing by years, and the mortality associated with RA is also elevating.3,4 Highly active RA results in the destruction of joints; in addition, RA is associated with systemic inflammation that may involve other tissues and organs and result in extra-articular effects, such as secondary Sjogren’s syndrome,5 interstitial pneumonia,6 and rheumatoid nodules,7 that are associated with poor prognosis.8
Rheumatoid factors (RFs) are defined as autoantibodies that recognize the Fc fragments of other immunoglobulins.9 The most common RFs are IgM and IgA RFs that bind to the Fc fragment of IgG.9 RFs are clearly detectable and often present in the early stages of RA, years before the clinical symptoms appear in some patients.10 The RF titer is considered as a diagnostic and prognostic marker of RA. RF still has an irreplaceable value in the classification standard of RA. The combination of RF and anti-cyclic citrullinated protein/peptide antibodies (ACPA) can improve the diagnostic specificity of RA.11 In a Danish cohort study, healthy individuals with elevated RF levels had an increased risk of developing RA disease.12 Studies have reported that high levels of RF have a good response to B cell-depleting therapy.13 Moreover, RF is associated with the activity of RA.14–16 A decrease in RF titers was found to be consistent with a decrease in activity in RA patients after treatment.17 However, until now, no researchers have explored the specific relationship between RF titers and RA activity.
Restricted cubic spline (RCS) is a data analysis model that can combine continuous variables with outcomes. It can reveal the influence of independent variables on outcome risk in the form of continuous curves, and it is an important method to analyze the dose-response relationship between continuous variables and outcomes.18 At present, it has been applied in many researches.19,20 This study sought to fill in this research gap by using the restricted cubic spline (RCS) function to perform a dose–effect analysis and quantify the association of RF titer with RA activity.
Materials and Methods
Study Participants
The cross-sectional study recruited 2044 patients with RA, which was diagnosed and classified according to the 2010 criteria of the American College of Rheumatology and the European League Against Rheumatism (ACR-EULAR).21 The patients were recruited between February 2022 and October 2023 from the First Affiliated Hospital of Anhui Medical University. Potential participants were first screened for their eligibility by two rheumatologists, who interviewed and assessed disease activity in the patients by calculating the disease activity score 28 (DAS28)-erythrocyte sedimentation rate (ESR) (DAS28-ESR) and DAS28-C reactive protein (CRP).22–24 Those with severe infections, severe trauma, and other inflammatory and autoimmune diseases were excluded. The Ethics Committee of the Anhui Medical University gave its approval for the study (Approval no.20121090) and all processes were in accordance with the 1964 Declaration of Helsinki.
Demographic and Clinical Data
Data on the following variables were obtained: sex, age, duration of RA, body mass index (BMI), presence of hypertension and diabetes, history of cigarette smoking and consumption of drugs within the past 3 months, including glucocorticoids (GCs), non-steroidal antiinflammatory drugs (NSAIDs), conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), biological DMARDs (bDMARDs), and targeted synthetic DMARDs (tsDMARDs).
Laboratory Assessment
Standard laboratory tests were performed to measure ESR (mm/h), CRP (mg/l), RF (IU/mL), white blood cell count (WBC, ×109/l), hemoglobin (HB, g/l), lymphocyte percentage (LY%), blood platelet count (BPC, ×109/l), albumin (ALB, g/l), alanine aminotransferase (ALT, U/l), aspartate aminotransferase (AST, U/l), blood urea nitrogen (BUN, mmol/l), uric acid (UA, µmol/l), and creatinine (CR, µmol/l). ESR was evaluated with the Wintrobe method, and the CRP level was determined with a turbidimetric assay (BioSystems). RF (isotype IgM) was assayed with an automated turbidimetric assay system (BioSystems), with the cut-off for RF detection set at 14 IU/mL.
Statistical Methods
SPSS 26.0 and R 4.4.0 were used to perform all the data analyses. Clinical variables were evaluated with descriptive statistics. The Mann–Whitney U-test was employed to analyze non-parametric data, and the chi-square test, to analyze frequencies. The RCS model was used to determine the non‑linear relationship of RF titer with RA activity. The factors that were significantly associated with the risk of RA activity were identified by univariate and unconditional multivariate logistic regression analyses, with odds ratios (ORs) and 95% confidence intervals (CIs) used to describe the risk ratio. A p-value <0.05 was assumed to indicate statistical significance.
Results
Characteristics of the Cohort
Of the 2044 participants with RA, 85.91% were female and 14.09% were male. The participants were divided into RF-positive (RF > 14 IU/mL, n = 1792) and RF-negative (RF ≤ 14 IU/mL, n = 252) groups. The groups showed significant differences in duration of RA, BMI, DAS28-ESR, DAS28-CRP, use of NSAIDs and csDMARDs, number of affected joints (indicated by tenderness and swelling), ESR, CRP, WBC, LY%, and ALB (P < 0.05 for all). The detailed clinical characteristics are presented in Table 1.
 |
Table 1 Characteristics of the Study Cohort (N = 2044) |
Logistic Regression Analysis of Factors Associated with the Risk of RA Activity
DAS28 greater than 3.2 was considered to indicate active RA, and DAS28 less than 3.2 was considered to indicate low RA activity.25 According to the results of univariate logistic regression analysis, the following factors were identified as significant predictors of the risk of RA activity according to DAS28-ESR: sex; age; duration of RA; diabetes; use of GCs, NSAIDs, csDMARDs, bDMARDs, and tsDMARDs; WBC; HB; LY%; BPC; ALB; ALT; AST; and RF. Further, the following variables emerged as significant predictors of the risk of RA activity assessed by DAS28-CRP: age; duration of RA; use of GCs, NSAIDs, csDMARDs, bDMARDs, and tsDMARDs; WBC count; HB, LY%, BPC, ALB, AST, Cr, UA, and RF (Table 2).
 |
Table 2 Univariate Logistic Regression Analysis of Significant Factors Associated with the Risk of RA Activity |
The variables identified in the univariate analysis were entered into the multivariate logistic regression model to determine which ones were independently related with the risk of RA activity. As shown in Table 3, the use of csDMARDs, bDMARDs and tsDMARDs; WBC count, LY%; HB; BPC; ALB; and RF titers were identified as being independently associated with the risk of RA activity according to DAS28. In addition, age was an independent predictor of the risk of RA activity according to DAS28-ESR, and duration of RA was an independent predictor of the risk of RA activity according to DAS28-CRP.
 |
Table 3 Multivariate Logistic Regression Analysis of Independent Factors Associated with the Risk of RA Activity |
Sensitivity Analysis
The RF titer was transformed from a continuity variable to a quartile categorical variable. As can be seen from Table 4, the risk of RA activity determined by DAS28-ESR for the lowest category of RF was 1.117 in the crude model, and it increased to 2.457 and 3.619 for the median and highest category, respectively. In the adjusted model, its value was 1.088 for the lowest category and increased to 1.904 and 2.020 in the median and highest category, respectively. The risk of RA activity assessed by DAS28-CRP for the lowest category of RF was 0.978 in the crude model and increased to 2.199 and 3.096 for the median and highest category, respectively. In the adjusted model, it was 0.880 for the lowest category of RF and increased to 1.519 and 1.526 for the median and highest category, respectively.
 |
Table 4 Logistic Regression Analyses of the Correlation Between RF and the Risk of RA Activity |
Non‑Linear Relationship Between RF Titers and RA Activity
Considering the skewed distribution of RF titers (Figure 1A), the values was log2-transformed for RCS analysis (Figure 1B). When the RCS function was used with 3 knots, a non-linear association between RF titers and RA activity was observed in the crude and adjusted models (Figures 2 and 3) (P < 0.05). In addition, a threshold effect was noted at a log2RF value of 6.04 (RF = 65.80 IU/mL). That is, when RF was less than 65.80 IU/mL, the risk of RA activity was almost unaffected or even reduced, but when RF was greater than 65.80 IU/mL, there was a rapid rise in the risk of RA activity.
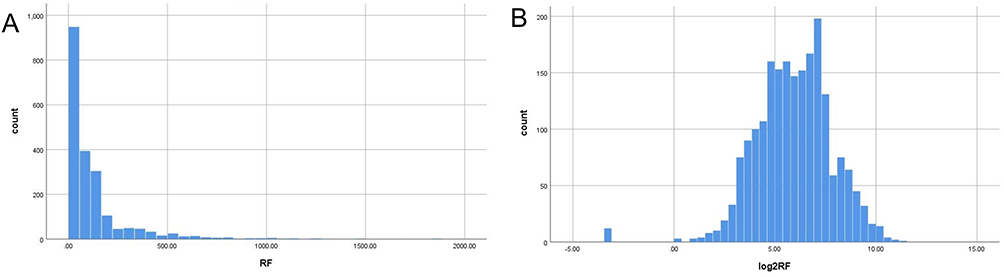 |
Figure 1 Distribution of RF titers. The figures show the distribution of (A) crude and (B) log2‑transformed RF titers. Abbreviation: RF, rheumatoid factor. |
 |
Figure 2 Association of RF titers with RA activity in the crude model. (A) Association of RF titers with RA activity according to DAS28-ESR. (B) Association of RF titers with RA activity according to DAS28-CRP. Abbreviations: RA, rheumatoid arthritis; RF, rheumatoid factor; DAS28, disease activity score 28; ESR, erythrocyte sedimentation rate; CRP, C reactive protein; OR, odds ratio; CI, confidence interval. |
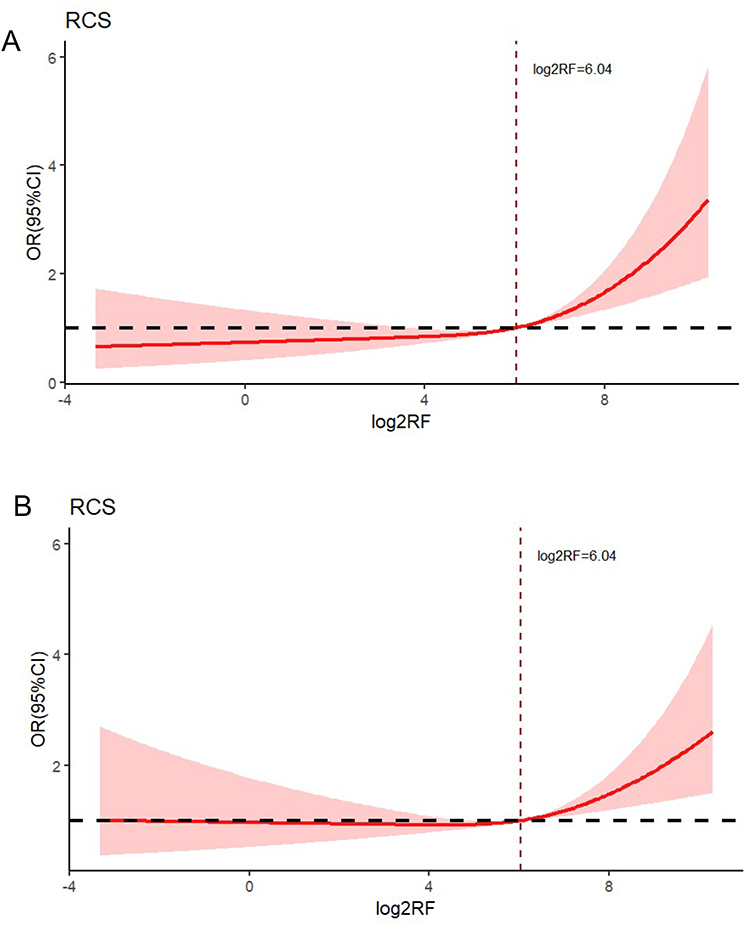 |
Figure 3 Association of RF titers with RA activity in the adjusted model. (A) Association of RF titers with RA activity according to DAS28-ESR. (B) Association of RF titers with RA activity according to DAS28-CRP. Abbreviations: RA, rheumatoid arthritis; RF, rheumatoid factor; DAS28, disease activity score 28; ESR, erythrocyte sedimentation rate; CRP, C reactive protein; OR, odds ratio; CI, confidence interval. |
RF titers were classified according to the cutoff value of 65.80 IU/mL. In the adjusted model, when RF exceeded the cutoff value, the risk of RA activity assessed by DAS28-ESR increased by 99.2% and the risk of RA activity assessed DAS28-CRP increased by 62.8% (Table 5 and Figure 4).
 |
Table 5 Relationship Between RF Levels and the Risk of RA Activity Stratified Based on a Cutoff Value of 65.80 IU/Ml |
 |
Figure 4 Risk of RA activity based on an RF cutoff value of 65.80 IU/mL in the adjusted model. (A) Risk of RA activity assessed by DAS28-ESR. (B) Risk of RA activity assessed by DAS28-CRP. Abbreviations: RA, rheumatoid arthritis; RF, rheumatoid factor; DAS28, disease activity score 28; ESR, erythrocyte sedimentation rate; CRP, C reactive protein; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; bDMARDs, biological DMARDs; tsDMARDs, targeted synthetic DMARDs; WBC, white blood cell; HB, hemoglobin; LY%, lymphocyte percentage; BPC, blood platelet count; ALB, albumin; CI, confidence interval. |
Discussion
The present study demonstrates a significant, non-linear relationship between RF titer and RA activity in patients with RA after adjusting for all covariates. In addition, based on the data, we found that an RF cutoff of 65.80 IU/mL could be used to determine the risk of RA activity. In the adjusted model, when the RF value was greater than 65.80 IU/mL, there was a 99.2% increase in the risk of RA activity based on DAS28-ESR and a 62.8% increase in the risk of RA activity based on DAS28-CRP. In line with this observation, it has previously been reported that assessing RA activity with DAS28-CRP leads to significant underestimation of disease activity in comparison with assessing RA activity based on DAS28-ESR.26,27
As early as the 1980s, studies have found that RF positivity, especially high RF titers, is associated with a higher degree of inflammation in patients with RA.28,29 Further, fluctuations in RF levels are considered biomarkers of disease activity and treatment responsiveness in patients with RA.30–32 However, there is limited analysis of the continuous changes in RF titers with RA activity. Most studies analyze RF as a categorical variable and classify patients based on RF positivity or quartiles.31,33–35 For example, high RF levels (≥156.4 IU/mL) were found to be predictive of the development of refractory RA.36 Further, a systematic review found that RF was correlated to bone erosion in RA as determined by ultrasound observation.37 However, these approaches to classifying RF could mask important clinical features or prognostic outcomes.
This study seeks to overcome the limitation of previous studies by exploring the dose-effect relationship between RF titers and RA activity. To this end, we used the RCS function, which is a useful tool for analyzing dose-effect associations between successive exposures and outcomes.38–40 We also conducted logistic regression analyses and adjusted for other covariables to improve the accuracy and reliability of the results. Moreover, the non-linear relationship was explored by RCS and smooth curve fitting, and the critical point was at which RF value was indicative of RA activity risk was also calculated. Our threshold RF value of 65.80IU/mL may be low compared to other literature,36 possibly due to the different materials used to measure RF in different laboratories, furthermore, the range of RF normal value in our lab is no more than 14 IU/mL, and it is necessary to establish a uniform standard.11
Another important finding of the study was the identification of factors that influence RA activity. The results show that the use of csDMARDs, bDMARDs and tsDMARDs; WBC; LY%; HB; BPC; and ALB were associated with RA activity assessed with DAS28. This is consistent with previous research reports.39,41–47 In addition, age was associated with DAS28-ESR, and duration of RA was associated with DAS28-CRP. This difference might be attributable to differences in the reference indicators. That is, ESR is an indicator of disease activity in recent weeks and is affected by sex, age, anemia, and other factors,48 while CRP is indicative of a shorter inflammatory response time.44
A major limitation of the present study is its cross-sectional design, as a result of which it is difficult to establish a causal link between RF and RA activity. Moreover, while the regression model was adjusted for some variables, we could not account for covariables for which data were not collected or were unavailable. This is another limitation to be considered when interpreting the study findings. Finally, some research variables from the questionnaires and self-reports may be biased. Given these limits, more research needs to be conducted to verify the present observations. Nonetheless, we believe that this study serves as a critical reference point for future research on the subject.
Conclusion
This is the first study to elucidate the non-linear significant relationship between the risk of RA activity and RF titers. The results show that the risk of RA activity increased non-linearly along with the continuous change in RF titers. Thus, RF may be useful as a clinical marker of inflammation and risk of RA activity in patients with RA. Given its low cost and simplicity of measurement, we believe that RF as a predictor of RA disease activity might have immense clinical potential and impact in terms of providing meaningful data for timely intervention and treatment of RA.
Data Sharing Statement
Data are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
The study was reviewed by the Ethics Committee of The Anhui Medical University and received its approval (Reference Number: 20121090). Written informed consent for participation in the study was obtained from the participants before study commencement.
Acknowledgments
We would like to thank all the patients with RA who participated in this study.
Funding
This work was supported by the National Key Research and Development Plan (2022YFC2504603).
Disclosure
The authors declare that they have no competing interests.
References
1. Smolen JS, Aletaha D, Barton A, et al. Rheumatoid arthritis. Nat Rev Dis Primers. 2018;4:18001. doi:10.1038/nrdp.2018.1
2. Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis: a review. JAMA. 2018;320(13):1360–1372. doi:10.1001/jama.2018.13103
3. Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet. 2010;376(9746):1094–1108. doi:10.1016/S0140-6736(10)60826-4
4. Global. regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;385(9963):117–171. doi:10.1016/S0140-6736(14)61682-2
5. Laroche M, Degboe Y, Constantin A. Sjögren’s syndrome associated with erosive rheumatoid arthritis alters its prognosis and long-term therapeutic response: a case-control study. Rheumatol Int. 2023;43(2):363–366. doi:10.1007/s00296-021-05074-0
6. Koduri G, Solomon JJ. Identification, monitoring, and management of rheumatoid arthritis-associated interstitial lung disease. Arthritis Rheumatol. 2023;75(12):2067–2077. doi:10.1002/art.42640
7. Ziff M. The rheumatoid nodule. Arthritis Rheum. 1990;33(6):761–767. doi:10.1002/art.1780330601
8. Conforti A, Di Cola I, Pavlych V, et al. Beyond the joints, the extra-articular manifestations in rheumatoid arthritis. Autoimmun Rev. 2021;20(2):102735. doi:10.1016/j.autrev.2020.102735
9. Maibom-Thomsen SL, Trier NH, Holm BE, et al. Immunoglobulin G structure and rheumatoid factor epitopes. PLoS One. 2019;14(6):e0217624. doi:10.1371/journal.pone.0217624
10. Scherer HU, Häupl T, Burmester GR. The etiology of rheumatoid arthritis. J Autoimmun. 2020;110:102400. doi:10.1016/j.jaut.2019.102400
11. Steiner G, Van Hoovels L, Csige D, Gatto M, Iagnocco A, Szekanecz Z. Should ACR/EULAR criteria be revised changing the RF and ACPA scores? Autoimmun Rev. 2024;23(1):103421. doi:10.1016/j.autrev.2023.103421
12. Nielsen SF, Bojesen SE, Schnohr P, Nordestgaard BG. Elevated rheumatoid factor and long term risk of rheumatoid arthritis: a prospective cohort study. BMJ. 2012;345:e5244. doi:10.1136/bmj.e5244
13. Isaacs JD, Cohen SB, Emery P, et al. Effect of baseline rheumatoid factor and anticitrullinated peptide antibody serotype on rituximab clinical response: a meta-analysis. Ann Rheum Dis. 2013;72(3):329–336. doi:10.1136/annrheumdis-2011-201117
14. Aletaha D, Alasti F, Smolen JS. Rheumatoid factor determines structural progression of rheumatoid arthritis dependent and independent of disease activity. Ann Rheum Dis. 2013;72(6):875–880. doi:10.1136/annrheumdis-2012-201517
15. Steiner G, Toes REM. Autoantibodies in rheumatoid arthritis - rheumatoid factor, anticitrullinated protein antibodies and beyond. Curr Opin Rheumatol. 2024;36(3):217–224. doi:10.1097/BOR.0000000000001006
16. Reyes-Pérez IV, Sánchez-Hernández PE, Muñoz-Valle JF, et al. Cytokines (IL-15, IL-21, and IFN-γ) in rheumatoid arthritis: association with positivity to autoantibodies (RF, anti-CCP, anti-MCV, and anti-PADI4) and clinical activity. Clin Rheumatol. 2019;38(11):3061–3071. doi:10.1007/s10067-019-04681-4
17. Ingegnoli F, Castelli R, Gualtierotti R. Rheumatoid factors: clinical applications. Dis Markers. 2013;35(6):727–734. doi:10.1155/2013/726598
18. van Dijk SC, Sohl E, Oudshoorn C, et al. Non-linear associations between serum 25-OH vitamin D and indices of arterial stiffness and arteriosclerosis in an older population. Age Ageing. 2015;44(1):136–142. doi:10.1093/ageing/afu095
19. Tan Y, Fu Y, Yao H, et al. Relationship between phthalates exposures and hyperuricemia in U.S. general population, a multi-cycle study of NHANES 2007-2016. Sci Total Environ. 2023;859(Pt 1):160208. doi:10.1016/j.scitotenv.2022.160208
20. Li L, Zhao M, Zhang Z, et al. Prognostic significance of the stress hyperglycemia ratio in critically ill patients. Cardiovasc Diabetol. 2023;22(1):275. doi:10.1186/s12933-023-02005-0
21. Aletaha D, Neogi T, Silman AJ, et al. Rheumatoid arthritis classification criteria: an American college of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi:10.1002/art.27584
22. Wells G, Becker JC, Teng J, et al. Validation of the 28-joint disease activity score (DAS28) and European league against rheumatism response criteria based on C-reactive protein against disease progression in patients with rheumatoid arthritis, and comparison with the DAS28 based on erythrocyte sedimentation rate. Ann Rheum Dis. 2009;68(6):954–960. doi:10.1136/ard.2007.084459
23. van der Heijde DM, van ‘t Hof MA, van Riel PL, et al. Judging disease activity in clinical practice in rheumatoid arthritis: first step in the development of a disease activity score. Ann Rheum Dis. 1990;49(11):916–920. doi:10.1136/ard.49.11.916
24. Felson DT, Anderson JJ, Boers M, et al. American college of rheumatology. Preliminary definition of improvement in rheumatoid arthritis. Arthritis Rheum. 1995;38(6):727–735. doi:10.1002/art.1780380602
25. Fransen J, van Riel PL. The disease activity score and the EULAR response criteria. Clin Exp Rheumatol. 2005;23(5 Suppl 39):S93–9.
26. Matsui T, Kuga Y, Kaneko A, et al. Disease activity score 28 (DAS28) using C-reactive protein underestimates disease activity and overestimates EULAR response criteria compared with DAS28 using erythrocyte sedimentation rate in a large observational cohort of rheumatoid arthritis patients in Japan. Ann Rheum Dis. 2007;66(9):1221–1226. doi:10.1136/ard.2006.063834
27. Son KM, Kim SY, Lee SH, Yang CM, Seo YI, Kim HA. Comparison of the disease activity score using the erythrocyte sedimentation rate and C-reactive protein levels in Koreans with rheumatoid arthritis. Int J Rheum Dis. 2016;19(12):1278–1283. doi:10.1111/1756-185X.12698
28. Robbins DL, Feigal DW Jr, Leek JC. Relationship of serum IgG rheumatoid factor to IgM rheumatoid factor and disease activity in rheumatoid arthritis. J Rheumatol. 1986;13(2):259–262.
29. Withrington RH, Teitsson I, Valdimarsson H, Seifert MH. Prospective study of early rheumatoid arthritis. II. Association of rheumatoid factor isotypes with fluctuations in disease activity. Ann Rheum Dis. 1984;43(5):679–685. doi:10.1136/ard.43.5.679
30. Mikuls TR, O’Dell JR, Stoner JA, et al. Association of rheumatoid arthritis treatment response and disease duration with declines in serum levels of IgM rheumatoid factor and anti-cyclic citrullinated peptide antibody. Arthritis Rheum. 2004;50(12):3776–3782. doi:10.1002/art.20659
31. Raheel S, Matteson EL, Crowson CS, Myasoedova E. Improved flare and remission pattern in rheumatoid arthritis over recent decades: a population-based study. Rheumatology. 2017;56(12):2154–2161. doi:10.1093/rheumatology/kex352
32. Paulshus Sundlisæter N, Olsen IC, Aga AB, et al. Predictors of sustained remission in patients with early rheumatoid arthritis treated according to an aggressive treat-to-target protocol. Rheumatology. 2018;57(11):2022–2031. doi:10.1093/rheumatology/key202
33. Weman L, Salo H, Kuusalo L, et al. Initial presentation of early rheumatoid arthritis. PLoS One. 2023;18(7):e0287707. doi:10.1371/journal.pone.0287707
34. Nakayama Y, Watanabe R, Murakami K, et al. Differential efficacy of TNF inhibitors with or without the immunoglobulin fragment crystallizable (Fc) portion in rheumatoid arthritis: the ANSWER cohort study. Rheumatol Int. 2022;42(7):1227–1234. doi:10.1007/s00296-021-05086-w
35. Pongratz G, Frieser R, Brinks R, et al. Association between autoantibody level and disease activity in rheumatoid arthritis is dependent on baseline inflammation. Clin Exp Rheumatol. 2020;38(4):691–698.
36. Watanabe R, Hashimoto M, Murata K, et al. Prevalence and predictive factors of difficult-to-treat rheumatoid arthritis: the KURAMA cohort. Immunol Med. 2022;45(1):35–44. doi:10.1080/25785826.2021.1928383
37. Abdelhafiz D, Baker T, Glascow DA, Abdelhafiz A. Biomarkers for the diagnosis and treatment of rheumatoid arthritis - a systematic review. Postgrad Med. 2023;135(3):214–223. doi:10.1080/00325481.2022.2052626
38. Desquilbet L, Mariotti F. Dose-response analyses using restricted cubic spline functions in public health research. Stat Med. 2010;29(9):1037–1057. doi:10.1002/sim.3841
39. Zhou E, Wu J, Zhou X, Yin Y. The neutrophil-lymphocyte ratio predicts all-cause and cardiovascular mortality among U.S. adults with rheumatoid arthritis: results from NHANES 1999-2020. Front Immunol. 2023;14:1309835. doi:10.3389/fimmu.2023.1309835
40. Deng X, Tan Y. A national cross-sectional analysis of selenium intake and risk of osteoarthritis: NHANES 2003-2016. Front Public Health. 2022;10:1047605. doi:10.3389/fpubh.2022.1047605
41. Xue L, Tao L, Sun H, et al. Association between blood PLT and RBC related indices and disease activity in patients with rheumatoid arthritis. Int J Gen Med. 2022;15:573–581. doi:10.2147/IJGM.S351505
42. Koehm M, McIntosh MJ, Hofmann MW, et al. Individual therapeutic DAS28-d(crit) responses differentiate between effectiveness of rheumatoid arthritis therapies and reflect patient-reported outcomes: retrospective analysis of DAS28 responses in comparative tocilizumab studies. Rheumatol Int. 2020;40(5):747–755. doi:10.1007/s00296-020-04514-7
43. Frazzei G, Musters A, de Vries N, Tas SW, van Vollenhoven RF. Prevention of rheumatoid arthritis: a systematic literature review of preventive strategies in at-risk individuals. Autoimmun Rev. 2023;22(1):103217. doi:10.1016/j.autrev.2022.103217
44. Pope JE, Choy EH. C-reactive protein and implications in rheumatoid arthritis and associated comorbidities. Semin Arthritis Rheum. 2021;51(1):219–229. doi:10.1016/j.semarthrit.2020.11.005
45. Padjen I, Öhler L, Studenic P, Woodworth T, Smolen J, Aletaha D. Clinical meaning and implications of serum hemoglobin levels in patients with rheumatoid arthritis. Semin Arthritis Rheum. 2017;47(2):193–198. doi:10.1016/j.semarthrit.2017.03.001
46. Olumuyiwa-Akeredolu OO, Page MJ, Soma P, Pretorius E. Platelets: emerging facilitators of cellular crosstalk in rheumatoid arthritis. Nat Rev Rheumatol. 2019;15(4):237–248. doi:10.1038/s41584-019-0187-9
47. Hayashi H, Satoi K, Sato-Mito N, et al. Nutritional status in relation to adipokines and oxidative stress is associated with disease activity in patients with rheumatoid arthritis. Nutrition. 2012;28(11–12):1109–1114. doi:10.1016/j.nut.2012.02.009
48. Prevoo ML, van ‘t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995;38(1):44–48. doi:10.1002/art.1780380107
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.