")
Back to Journals » Patient Preference and Adherence » Volume 19
Risk Factors Affecting Quality of Life in Chronic Limb Threatening Ischemia Patients
Authors Wu R, Yu Y, Guo J, Gao X, Tong Z, Guo J, Cui S, Zhang C, Guo L
Received 3 April 2025
Accepted for publication 4 July 2025
Published 9 July 2025 Volume 2025:19 Pages 1965—1972
DOI https://doi.org/10.2147/PPA.S532224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Rui Wu,* Yuan Yu,* Julong Guo,* Xixiang Gao, Zhu Tong, Jianming Guo, Shijun Cui, Chengchao Zhang, Lianrui Guo
Department of Vascular Surgery, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lianrui Guo, Department of Vascular Surgery, Xuanwu Hospital, Capital Medical University, No. 45 Changchun Street, Xicheng District, Beijing, 100053, People’s Republic of China, Tel +86 15510170321, Email [email protected]
Purpose: To analyze the independent risk factors affecting quality of life (QoL) in chronic limb threatening ischemia (CLTI) patients, with a particular focus on the role of the Wound, Ischemia, and foot Infection (WIfI) classification. Understanding these relationships could provide insights into optimizing patient management and improving their overall QoL.
Patients and Methods: This study was conducted at our center from January 2021 to January 2024. Hospitalized patients diagnosed with CLTI (Rutherford categories 4– 6) were enrolled for QoL assessment using the Vascular Quality of Life Questionnaire (VascuQoL). We analyzed the differences in the scores of vascuQoL and its five dimensions among patients grouped by different WIfI stages. A linear regression model was used to identify independent risk factors of overall VascuQoL scores and its different dimensions.
Results: This study included 309 patients with an average age of 70.11 years; 30.1% were female. The mean baseline VascuQoL score was 2.02 ± 0.83. According to the WIfI classification, patients were distributed as follows: 15.53% stage 4, 39.16% stage 3, 27.83% stage 2, and 17.48% stage 1. WIfI classification emerged as a key independent predictor, significantly affecting overall VascuQoL scores (β=− 0.15, 95% CI − 0.24 to − 0.06, P=0.002) and four out of five QoL dimensions (activity, symptoms, emotional well-being, and social interactions). Female sex, smoking history, cerebral infarction history, and previous limb revascularization also affect the quality of life from different dimensions or as a whole.
Conclusion: CLTI markedly worsens patients’ QoL, with WIfI stage playing a crucial role in determining outcomes.
Keywords: chronic limb threatening ischemia, peripheral arterial disease, quality of life, WIfI classification system
Introduction
Chronic Limb Threatening Ischemia (CLTI), the advanced stage of peripheral arterial disease (PAD), is characterized by rest pain, ulcers, or gangrene, significantly impairing patients’ quality of life (QoL).1 Persistent ischemic pain severely limits mobility, while chronic wounds and infections necessitate frequent hospital visits, disrupt daily activities, and often lead to social isolation.2 Studies using generic QoL tools, such as the SF-36, have demonstrated that CLTI patients score significantly lower in physical functioning, mental health, and social roles compared to both healthy populations and those with earlier-stage PAD. Furthermore, emotional distress such as anxiety, depression, and stigmatization associated with limb-threatening conditions worsens QoL.3,4 Given the profound and multifaceted impact of CLTI on patients’ QoL, identifying the factors influencing QoL is crucial for developing effective treatment and care strategies tailored to this vulnerable population.
The Vascular Quality of Life Questionnaire (VascuQoL), a tool specifically used to assess quality of life in patients with PAD, is commonly used to evaluate multiple domains, including symptoms, activity limitations, pain, emotional well-being, and social interactions.2 VascuQoL addresses the limitations of generic Questionnaire tools by providing a disease-specific assessment that captures the unique challenges faced by patients with vascular conditions. Among the various factors influencing VascuQoL scores, the Wound, Ischemia, and foot Infection (WIfI) classification system stands out as a widely adopted tool for stratifying the risk of major amputation. While WIfI classification system has become a cornerstone for predicting amputation risk and guiding treatment decisions,5 its relationship with multidimensional QoL outcomes remains underexplored.
To address this gap, this single-center study aims to analyze the independent risk factors affecting QoL in CLTI patients, with a particular focus on the role of WIfI classification. Understanding these relationships could provide insights into optimizing patient management and improving their overall QoL.
Materials and Methods
Study Design and Population
This study was conducted at our center from January 2021 to January 2024. Hospitalized patients diagnosed with CLTI were enrolled for quality-of-life assessment using the Vascular Quality of Life Questionnaire (VascuQoL). We performed this analysis by screening patients according to criteria. The inclusion criteria were as follows: (1) Rutherford classification of 4–6; (2) no vascular intervention performed on the target limb within the past two weeks; and (3) willingness and ability to complete the VascuQoL assessment. All assessments were performed at the time of admission and administered by trained nursing staff with extensive experience. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Xuanwu Hospital Ethics Committee. Informed consent was obtained from all participants before enrollment.
Data Collection
The VascuQoL instrument consists of 25 questions covering five domains: activities, symptoms, pain, emotional well-being, and social interactions. Scores for each question range from 1 (worst) to 7 (best), with higher scores indicating better quality of life. Additional patient data were collected, including demographic information (age, sex, body mass index [BMI]), clinical characteristics (number of affected limbs, comorbidities, history of vascular reconstruction of the target limb), lesion location, below-knee and foot runoff scores, and WIfI stages.
Statistical Analysis
The methodology for this study followed approaches commonly used in similar research. Continuous variables were reported as means with standard deviations or medians with interquartile ranges, as appropriate. Categorical variables were presented as frequencies and percentages. Comparisons between different WIfI stage groups were performed using one-way ANOVA for normally distributed variables, whereas non-normally distributed variables were analyzed with Kruskal–Wallis test. Univariate linear regression analysis was performed to explore associations between potential independent variables and VascuQoL scores at admission, which served as the dependent variable. To avoid omitting potentially meaningful variables, variables with a p-value < 0.1 in univariate analysis were included in the multivariate linear regression model to identify independent predictors of overall VascuQoL scores and its different dimensions (activity, symptom, pain, emotional, and social). Independent variables considered in the analysis included age, sex, BMI, number of affected limbs, comorbidities, history of vascular reconstruction, lesion location, below-knee and foot runoff scores, and WIfI grades. The results of linear regression were presented as regression coefficients with 95% confidence intervals (CIs) and corresponding p-values. Statistical significance was defined as P< 0.05. Statistical analysis was performed using SPSS version 26.0 (IBM, Armonk, New York) and R version 4.2.2 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline Characteristics
A total of 309 patients with CLTI were included in this study. The mean age was 70.11 ± 11.64 years, with females comprising 30.1% (93/309) of the cohort. Most patients had unilateral CLTI (91.59%) and a high prevalence of comorbidities, including hypertension (66.02%) and diabetes (72.17%). The infrapopliteal artery was the most common lesion location (80.58%), followed by the femoropopliteal artery (61.17%). In terms of WIfI classification, 15.53% of patients were categorized as stage 4, 39.16% as 3, 27.83% as stage 2, and 17.48% as stage 1. The mean baseline VascuQoL score was 2.02 ± 0.83, indicating poor quality of life among participants. Meanwhile, QoL scores were low for all five dimensions (Table 1).
 |
Table 1 Baseline Characteristics of Patients |
VascuQoL Scores of Different WIfI Stages
In the overall vascuQoL score, stage 1 was significantly higher than other stages, with respective P-values of 0.029, 0.002, and <0.001. Specifically, the scores were 2.36 ± 0.85 for stage 1, 2.05 ± 0.79 for stage 2, 1.94 ± 0.82 for stage 3, and 1.78 ± 0.75 for stage 4. Regarding activity scores, stage 1 was significantly higher than all other, with respective P-values of 0.027, 0.001, and <0.001. Additionally, stages 2 and 3 were also significantly higher than stage 4 (P=0.005, 0.045). The symptom score for stage 1 was significantly higher than that for stage 3 (P=0.002) and stage 4 (P=0.002). Additionally, the symptom score for stage 2 was significantly higher than that for stage 4 (P=0.047). Pain scores showed a trend of decreasing scores from stage 1 to 4, although the significantly difference was only found between stage 1 and 4 (P=0.017). In the emotional and social scores, stage 1 was significantly higher than other stages (Figure 1).
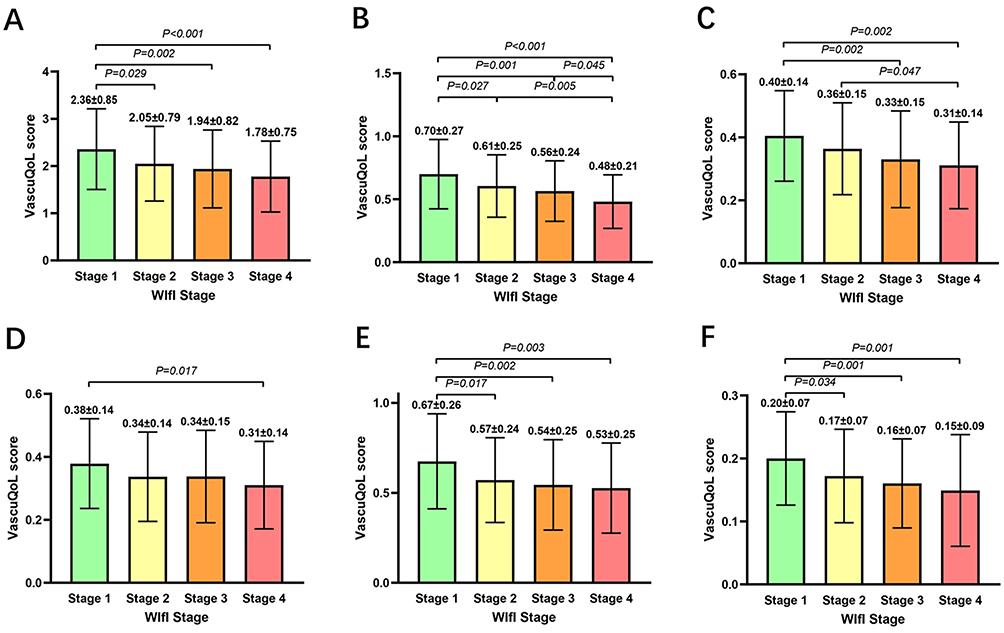 |
Figure 1 Comparison of vascuQoL and its different dimensional scores across different WIfI stage groups. (A) overall score; (B) activity dimension; (C) symptom dimension; (D) pain dimension; (E) emotional dimension; (F) social dimension. The results showing significant differences between groups were presented. Abbreviations: WIfI, Wound, Ischemia, and foot Infection. |
Regression Analysis of Overall VascuQoL
Univariate linear regression identified several factors significantly or nearly significantly associated with lower VascuQoL scores. These included female sex (β=−0.29, P=0.004), smoking history (β=−0.20, P=0.045), WIfI stage (β=−0.18, P< 0.001), and a history of previous limb revascularization (β=−0.19, P=0.066). Multivariable analysis confirmed WIfI stage as an independent predictor of VascuQoL scores (β=−0.15, 95% CI: −0.24 to −0.06, P=0.002), along with female sex (β=−0.37, 95% CI: −0.58 to −0.17, P< 0.001) and smoking history (β=−0.31, 95% CI: −0.51 to −0.10, P=0.003). While other clinical and demographic factors were not significantly associated with VascuQoL scores (Table 2).
 |
Table 2 Univariate and Multivariable Linear Regression Analysis of Overall Vascular Quality of Life (VascuQoL) |
Regression Analysis of Different VascuQoL Dimensions
Multivariable analysis revealed that female sex (β=−0.08, 95% CI: −0.14 to −0.02, P=0.007) and WIfI stage (β=−0.06, 95% CI: −0.09 to −0.03, P< 0.001) were significant predictors of lower activity scores. Lower symptom scores were significantly associated with WIfI stage (β=−0.03, 95% CI: −0.04 to −0.01, P=0.003), female sex (β=−0.06, 95% CI: −0.10 to −0.03, P=0.001), and smoking history (β=−0.06, 95% CI: −0.10 to −0.03, P< 0.001). Significant predictors of lower pain scores included female sex (β=−0.07, 95% CI: −0.10 to −0.03, P< 0.001), and smoking history (β=−0.06, 95% CI: −0.10 to −0.03, P=0.001). While WIfI stage did not show significant association with pain scores in the multivariable model. Lower scores in the emotional well-being dimension were significantly associated with WIfI stage (β=−0.04, 95% CI: −0.07 to −0.01, P=0.015), female sex (β=−0.11, 95% CI: −0.17 to −0.04, P=0.002), and smoking history (β=−0.11, 95% CI: −0.17 to −0.04, P=0.002). Finally, WIfI stage (β=−0.02, 95% CI: −0.03 to −0.01, P< 0.001), cerebral infarction history (β=−0.03, 95% CI: −0.06 to −0.01, P=0.031), and previous limb revascularization (β=−0.02, 95% CI: −0.04 to −0.01, P=0.032) were significant predictors of lower social interaction scores. All these results were presented in the Supplemental Tables 1–5.
Discussion
This study highlights the substantial impact of CLTI on patients’ quality of life, which was assessed by VascuQoL. Our results indicate that the mean overall VascuQoL score in this cohort was 2.02 ± 0.83, reflecting severe impairment of QoL. Moreover, when examining individual dimension scores, this impairment was consistently evident across all five dimensions.1,6–8 Importantly, our study demonstrates that the WIfI stage was significantly associated with the overall VascuQoL score and four of its five dimensions—activity, symptoms, emotional, and social. Notably, no significant association was observed between WIfI classification and the pain dimension, a finding that warrants further exploration.
It was found that with the development of PAD, the patient’s quality of life in many aspects, such as activity, pain, and psychology, decreased significantly.3,4,8 The association between higher WIfI stages and poorer QoL likely reflects the increased ischemic burden, wound severity, and infection risk as the disease progresses. Advanced WIfI stages are characterized by severe tissue ischemia and large, infected, non-healing wounds, both of which worsen physical disability and reduced emotional and social functioning.9 Individuals frequently suffer from emotional distress, which includes sensations of disgrace, embarrassment, a decline in self-assurance, anxiety, remorse, depressive symptoms, and a sense of being cut off from others, as a result of their wound-related issues.10,11 This explains the significant associations of WIfI classification with activity, symptoms, emotional well-being, and social dimensions. The absence of a linear relationship between WIfI classification and the pain dimension may be attributed to peripheral neuropathy, which affects up to 60% of CLTI patients and can mask the sensation of ischemic pain, creating a disconnect between objective disease severity and subjective pain reporting.12,13 Additionally, psychological factors such as depression and anxiety, prevalent in this population, may further distort pain perception.4 These findings highlight the need for comprehensive pain assessment tools that account for both neuropathic and psychosocial components in CLTI patients.
Our study also identified female sex and smoking history as significant predictors of poorer QoL, both overall and across multiple VascuQoL dimensions. Women with CLTI often report worse VascuQoL outcomes than men, as previously noted in the BEST-CLI trial.7 Similarly, some studies have found that female PAD patients have worse outcomes after endovascular intervention.14 The premenopausal hormonal environment can prevent nitric oxide-dependent endothelial dysfunction to a certain extent, resulting in a slow development of PAD in women before the age of 60 or even 70. However, this phenomenon disappeared in the subsequent period.14–18 Similarly, smoking is a well-established risk factor for poor vascular outcomes and QoL in PAD and CLTI populations.7,19,20 Smoking accelerates atherosclerotic disease progression, impairs wound healing, and increases the risk of reintervention, all of which diminish physical and emotional well-being.21 These findings underscore the importance of targeted smoking cessation programs to improve both clinical outcomes and quality of life. Patients with cerebral infarction and those who have undergone lower limb arterial surgery may experience diminished social interaction abilities due to neurological impairment or restricted physical function. Additionally, chronic pain, depressive symptoms, and insufficient social support during the postoperative recovery period may further undermine their willingness and capacity for social engagement. Our findings suggest that addressing modifiable risk factors, such as smoking cessation, and providing tailored interventions (eg, psychological support for high-WIfI patients or gender-specific care plans) could significantly enhance QoL outcomes in CLTI patients. Recent studies have demonstrated the efficacy of multidisciplinary approaches, including behavioral therapy and patient education, in improving both physical and emotional well-being in this population.9,11
This study has several limitations that must be acknowledged. First, as a single-center study, the generalizability of our findings to broader CLTI populations may be limited. Second, our use of the VascuQoL as the sole instrument for assessing QoL may not capture all aspects of patient well-being. While VascuQoL is a validated tool specific to vascular disease, its scope is limited compared to generic QoL measures such as the EQ-5D or SF-36, which assess broader domains of health.
Conclusion
CLTI significantly deteriorates the overall QoL of patients, affecting all domains. The factors influencing different dimensions of QoL in CLTI patients vary. Notably, WIfI classification plays a significant role in determining QoL outcomes, as it is strongly associated with the overall VascuQoL score and all dimensions, except for pain. Addressing these factors through comprehensive patient assessment, individualized care plans, and modifiable risk factor management could enhance QoL outcomes in this population.
Ethics Approval and Informed Consent
The study was approved by Xuanwu Hospital Ethics Committee (granted number: [2020]154).
Acknowledgments
Thanks to all the staff and patients who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Key Research and Development Projects (2022YFC3602400, 2022YFC3602404).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Conte MS, Bradbury AW, Kolh P, et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. Eur J Vasc Endovasc Surg. 2019;58:S1–S109.e33. doi:10.1016/j.ejvs.2019.05.006
2. Morgan MB, Crayford T, Murrin B, et al. Developing the vascular quality of life questionnaire: a new disease-specific quality of life measure for use in lower limb ischemia. J Vasc Surg. 2001;33:679–687. doi:10.1067/mva.2001.112326
3. Sprengers RW, Teraa M, Moll FL, et al. Quality of life in patients with no-option critical limb ischemia underlines the need for new effective treatment. J Vasc Surg. 2010;52:843–849. doi:10.1016/j.jvs.2010.04.057
4. Thomas M, Patel KK, Gosch K, et al. Mental health concerns in patients with symptomatic peripheral artery disease: insights from the PORTRAIT registry. J Psychosom Res. 2020;131:109963. doi:10.1016/j.jpsychores.2020.109963
5. van Reijen NS, Ponchant K, Ubbink DT, et al. Editor’s choice - the prognostic value of the WIfI classification in patients with chronic limb threatening ischaemia: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2019:58362–58371.
6. Perlander A, Broeren M, Österberg K, et al. Disease specific health related quality of life in patients with chronic limb threatening ischaemia undergoing revascularisation of femoropopliteal lesions. Eur J Vasc Endovasc Surg. 2023;66:245–251. doi:10.1016/j.ejvs.2023.05.014
7. Siracuse JJ, Rowe VL, Menard MT, et al. Relationship between WIfI stage and quality of life at revascularization in the BEST-CLI trial. J Vasc Surg. 2023;77:1099–1106e4. doi:10.1016/j.jvs.2022.11.050
8. Roijers JP, van den Houten MM, Hopmans NJ, et al. A comparison of quality of life in elderly patients with intermittent claudication and chronic limb-threatening ischemia. Ann Vasc Surg. 2020;69:285–291. doi:10.1016/j.avsg.2020.05.048
9. Klevsgård R, Hallberg IR, Risberg B, et al. The effects of successful intervention on quality of life in patients with varying degrees of lower-limb ischaemia. Eur J Vasc Endovasc Surg. 2000;19:238–245. doi:10.1053/ejvs.1999.0995
10. Liu X, Xie J-Q, Liao Z-Y, et al. Changes in wound symptoms and quality of life of patients with newly diagnosed malignant fungating wounds. J Wound Care. 2024;33:262–270. doi:10.12968/jowc.2024.33.4.262
11. Nowak M, Piechota D, Baranska-Rybak W. Gdansk Wound-QoL questionnaire: pilot study on health-related quality of life of patients with chronic ulcers with emphasis on professional physician-patient relations. Dermatol Pract Concept. 2024;14:e2024138. doi:10.5826/dpc.1403a138
12. Trocha A, Gontscharuk V, Icks A, et al. The value of loss of protective pain sensation in predicting a first ulceration of the foot in people with diabetes. Diabet Med. 2024;41:e15241. doi:10.1111/dme.15241
13. Gröne E, Üçeyler N, Abahji T, et al. Reduced intraepidermal nerve fiber density in patients with chronic ischemic pain in peripheral arterial disease. Pain. 2014;155:1784–1792. doi:10.1016/j.pain.2014.06.003
14. Manvar-Singh P, Folk A, Genovese EA. A scoping review of female sex-related outcomes after endovascular intervention for lifestyle-limiting claudication and chronic limb-threatening ischemia. Semin Vasc Surg. 2023;36:541–549. doi:10.1053/j.semvascsurg.2023.10.001
15. Moreau KL, Stauffer BL, Kohrt WM, et al. Essential role of estrogen for improvements in vascular endothelial function with endurance exercise in postmenopausal women. J Clin Endocrinol Metab. 2013;98:4507–4515. doi:10.1210/jc.2013-2183
16. Hsu S-P, Lee W-S. Effects of female sex hormones on the development of atherosclerosis. Chin J Physiol. 2020;63:256–262. doi:10.4103/CJP.CJP_69_20
17. Madonna R, Balistreri CR, De Rosa S, et al. Impact of sex differences and diabetes on coronary atherosclerosis and ischemic heart disease. Chin J Physiol. 2019;8:98.
18. Martelli E, Zamboni M, Sotgiu G, et al. Sex-related differences and factors associated with peri-procedural and 1 year mortality in chronic limb-threatening ischemia patients from the CLIMATE Italian registry. J Pers Med. 2023;13:316. doi:10.3390/jpm13020316
19. Liu M, Zhang W, Yan Z, et al. Smoking increases the risk of diabetic foot amputation: a meta-analysis. Exp Ther Med. 2018;15:1680–1685. doi:10.3892/etm.2017.5538
20. Acar E, Kacıra BK. Predictors of lower extremity amputation and reamputation associated with the diabetic foot. J Foot Ankle Surg. 2017;56:1218–1222. doi:10.1053/j.jfas.2017.06.004
21. Patel RJ, Zarrintan S, Jagadeesh V, et al. Long-term outcomes after lower extremity bypass in the actively smoking claudicant. J Vasc Surg. 2023;78:1003–1011. doi:10.1016/j.jvs.2023.05.047
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.