")
Back to Journals » Clinical Ophthalmology » Volume 18
Risk Factors for Postoperative Refractive Error in New-Generation Intraocular Lens Calculation Formulas
Authors Nishida S, Inomata Y, Hirata A
Received 29 March 2024
Accepted for publication 6 August 2024
Published 12 August 2024 Volume 2024:18 Pages 2253—2259
DOI https://doi.org/10.2147/OPTH.S471393
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Shohei Nishida,1 Yasuya Inomata,1 Akira Hirata2
1Inomata Eye Clinic, Kumamoto City, Kumamoto, Japan; 2Hayashi Eye Hospital, Fukuoka City, Fukuoka, Japan
Correspondence: Shohei Nishida; Yasuya Inomata, Email [email protected]; [email protected]
Purpose: We examined differences in the accuracy of three intraocular lens (IOL) calculation formulas: the traditional Sanders-Retzlaff-Kraff/Theoretical (SRK/T) formula; the Barrett Universal II (BU II) formula, which is a new-generation IOL calculation formula; and the postoperative spherical equivalent prediction using artificial intelligence and linear algorithms developed by Debellemanière, Gatinel, and Saad formula (PEARL-DGS [PEARL]) formula, and evaluated factors that cause postoperative refractive error (PE).
Patients and Methods: The study included 205 patients (205 eyes) with a mean age of 75.2 ± 8.7 years who underwent cataract surgery at our institution from December 2018 to October 2023. The PE of the three IOL calculation formulas was calculated and compared. Multivariate logistic regression analysis was performed with a PE higher than ± 0.50 D as the dependent variable, and age, sex, axial length (AL), mean keratometry (mean K), anterior chamber depth (ACD), lens thickness (LT), and white-to-white (WTW) as independent variables.
Results: The mean PE (ME) ± standard deviation of the SRK/T, BU II, and PEARL formulas was 0.11 ± 0.52, 0.11 ± 0.50, and 0.21 ± 0.50 D, respectively. MEs of the three IOL calculation formulas were significantly different from 0 (p < 0.01). The median absolute error (MedAE) was not significantly different among the three IOL calculation formulas (p = 0.83). The percentage of PE within ± 0.50 D was not significantly different among the three IOL calculation formulas (p = 0.13). Multivariate logistic regression analysis showed that the significantly associated factors with PE higher than ± 0.50 D were AL, ACD, and LT for the SRK/T formula, sex and LT for the BU II formula, and LT for the PEARL formula (all p < 0.05).
Conclusion: In the BU II and PEARL formulas, AL was excluded as a factor affecting PE, indicating that LT was a risk factor.
Keywords: cataract, lens thickness, logistic models, refractive surgical procedures
Introduction
In recent years, cataract surgery has become more significant as a refractive surgery, rather than a conventional surgery, to improve visual function, with the development of new-generation intraocular lens (IOL) calculation formulas and improvements in biometric technology enabling highly accurate surgeries.1,2 The Sanders-Retzlaff-Kraff/Theoretical (SRK/T) formula has been used for many years as a vergence-based IOL calculation formula utilizes axial length (AL) and mean keratometry (mean K), the factors causing postoperative refractive error (PE) in the SRK/T formula are AL,3,4 keratometry,5 and age at surgery.6 Among the new-generation IOL calculation formulas, the Barrett Universal II (BU II) formula is a theoretical IOL calculation formula published in 2010 that uses measurements of anterior chamber depth (ACD), lens thickness (LT) and white-to-white (WTW) in addition to AL and mean K in its calculation. The BU II formula is more accurate than the traditional SRK/T formula, with smaller PE at AL >25 mm and <22 mm.7,8 In addition, the postoperative spherical equivalent prediction using artificial intelligence and linear algorithms developed by Debellemanière, Gatinel, and Saad (PEARL-DGS [PEARL]) formula using machine learning models of artificial intelligence in 2017 is as accurate as or more accurate than the BU II formula in long and short eyes, and the new-generation IOL calculation formula is less sensitive to ocular morphology.9,10 However, Shammas et al reported that the percentage of PE within ±0.50 D was 75%, 80.5%, and 81.7% in the SRK/T, BU II, and PEARL formulas, respectively.9 Thus, even with the new-generation IOL calculation formula, PE may occur in some cases. Therefore, we examined the factors related to PE in the new-generation IOL calculation formulas. The PE of the traditional (SRK/T) and new-generation IOL calculation formulas (BU II and PEARL) were compared. In addition, the PE of each formula was considered the dependent variable, and parameters such as age, sex, AL, mean K, ACD, LT, and WTW were considered the independent variables, and the factors related to refractive error were examined using multivariate logistic regression analysis.
Material and Methods
Ethics Approval and Informed Consent
This study conformed to the ethical provisions of the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of the Department of Inomata Eye Hospital. Informed consent was waived because we only used anonymized data.
Inclusion Criteria
Table 1 shows the patient background. A series of phacoemulsification cataract surgery between December 2018 and October 2023 was performed at the clinic. Preoperative measurements of AL, mean K, ACD (from the corneal epithelium to the lens), LT, and WTW were obtained using the OA-2000™ (TOMEY Corp. Nagoya-City, Aichi, Japan), and a one-piece hydrophobic acrylic IOL, the HOYA iSert Micro (HOYA Surgical Optics, Inc)., was used for in-the-bag implantation were included in the study. Exclusion criteria were keratopathy, lens subluxation, or other conditions that could affect PE, corrected distance visual acuity of 20/25 at 4 weeks postoperatively, and patients who were lost to follow up for >4 weeks postoperatively. Only one eye was selected randomly if both eyes underwent surgery.
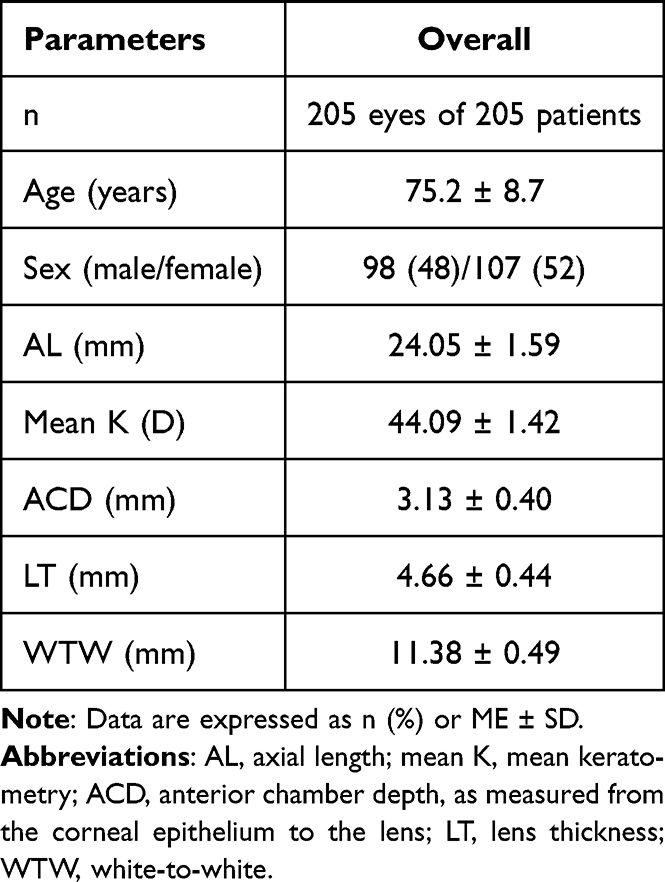 |
Table 1 Patient Background |
IOL Calculation Formula
We used the SRK/T formula11 based on the third-generation thin lens equations, the BU II formula12 based on the new-generation thick lens equations using paraxial space, and the PEARL-DGS formula13 based on the thick lens equations using a machine learning model to predict the distance between the posterior corneal radius and the theoretical IOL position, and the results were compared. The BU II formula was used for the actual inserted IOL calculation. A constant of 118.5 was based on the User Group for Laser-Interference Biometry.
PE Evaluation
The expected refraction of each formula was subtracted from the spherical equivalent of the objective refraction using the auto refractometer (model ARK-1a from Nidek Co., Ltd. Nagoya-City, Aichi, Japan) at 4 weeks postoperatively14 and evaluated as the refractive error with positive mean PE (ME) and negative ME representing refractive error for hyperopia and myopia, respectively. We calculated the ME, standard deviation (SD), median absolute error (MedAE), and percentage of eyes with PE within ±0.50 D.
Statistical Analysis
Statistical analyses using EZR15 (version 2.6–1, Sun Apr) were performed based on the published protocol.14 Kolmogorov–Smirnov test was used to examine data normality. One-sample t-test was used to examine whether the ME of each IOL calculation formula was significantly different from 0. Friedman test was used to compare MedAE, and Bonferroni adjustment was used for multiple comparisons. The χ2 test was performed to compare the percentages of cases within ±0.50 D of PE. Risk factors were determined using multivariate logistic regression analysis in cases with PE higher than ±0.50 D as dependent variables and each parameter (age, sex, AL, mean K, ACD, LT, and WTW) as independent variables. Significant difference was determined at p < 0.05.
Results
Table 1 shows the patient background. We included 205 eyes of 205 patients. The mean age of the patients was 75.2 ± 8.7 years, and 98 and 107 were male and female patients, respectively. Table 2 shows the PE results for each IOL calculation formula. The MEs of the three IOL calculation formulas were significantly different from 0 (one-sample t-test: all p < 0.01). The MedAE were not statistically significantly different among the three IOL calculation formulas (Friedman test: p = 0.83). The percentage of cases within ±0.50 D of PE was not statistically significantly different among the three IOL calculation formulas (χ²-test: p = 0.13). Tables 3–5 show the multivariate logistic regression analysis results for factors with PE higher than ±0.50 D in the SRK/T, BU II, and PEARL formulas, respectively. Significantly associated factors were AL (p = 0.02), ACD (p = 0.01), and LT (p = 0.01) for the SRK/T formula. Moreover, the significantly associated factors in the BU II formula were sex (female: p = 0.04) and LT (p = 0.04), and the significantly associated factor in the PEARL formula was LT (p = 0.04).
 |
Table 2 PE Results for Three IOL Calculation Formulas |
 |
Table 3 Multivariate Logistic Regression Analysis Results for Factors with PE Higher Than ±0.50 D in the SRK/T Formula |
 |
Table 4 Multivariate Logistic Regression Analysis Results for Factors with PE >±0.50 D in the BU II Formula |
 |
Table 5 Multivariate Logistic Regression Analysis Results for Factors with PE Higher Than ±0.50 D in the PEARL Formula |
Discussion
The only factors significantly associated with PE higher than ±0.50 D were AL, ACD, and LT for the SRK/T formula; sex and LT for the BU II formula; and LT for the PEARL formula, indicating that LT was a risk factor for PE in new-generation IOL calculation formulas. The accuracy of each IOL calculation formula was similar to that reported by Fernandes et al and Cheng et al16,17 In recent years, the accuracy of the new-generation IOL calculation formulas and factors affecting PE have been high.7–10 Regarding the risk factors for PE higher than ±0.50 D in the SRK/T formula, which was different from the results of Koga et al who reported that PE higher than ±0.50 D was significantly associated with age.18 This may be because of the inclusion of 66 patients >90 years, whereas our study only included 2 patients >90 years. Regarding the risk factors for PE higher than ±0.50 D in the BU II formula, Sella et al reported no significant factors associated with PE in the BU II formula.19 This may be because of LT not being used in the analysis, and the dependent variable was PE higher than ±1.00 D, thereby this study inferred that the results differed from those in a previous report.19 However, Li et al reported that PE higher than ±0.50 D was significantly associated with female sex in a multivariate logistic regression analysis of refractive error after cataract surgery in patients with primary angle closure glaucoma, and the BU II formula indicated that female sex influences PE.20 Some studies showed that LT and PE showed a positive correlation,21 whereas others reported that patients with an LT ≥4.74 mm postoperatively shifted to myopia; hence, the association between the BU II formula and LT is still unclear.22 This study showed that the odds ratio for LT was 2.68, and that the risk of PE higher than ±0.50 D increased with higher LT. The only risk factor in the PEARL formula was LT. The PEARL formula is less influenced by ACD and LT.10 However, the detailed characteristics of the formula remain unclear. In the results of this study, LT was significantly associated with PE, and the risk of PE higher than ±0.50 D increased with higher LT. The reason why LT Influences PE is suggested that the postoperative IOL position is determined by the postoperative ACD, and the postoperative ACD depends on both the LT and the preoperative ACD. Therefore, we speculate that higher LT that deviate from theoretical values used in each IOL calculation formula will have a more pronounced Influence on the postoperative ACD, leading to shift in the postoperative IOL position. The odd ratios for LT were 4.00, 2.68, and 2.69 for the SRK/T, BU II, and PEARL formulas, respectively. The results indicate that although LT influences the new-generation IOL calculation formula, its influence is smaller than that of the SRK/T formula. A limitation of this study was the small number of patients, in future studies, additional cases should be included to establish cutoff values for LT and clarify the impact of other risk factors.
Conclusion
In the new-generation IOL calculation formulas, the BU II and PEARL, indicating that LT is a risk factor. However, the effect of LT varies depending on the IOL calculation formula, and the importance of the factor varies.
Abbreviations
ACD, anterior chamber depth; AL, axial length; BU II, Barrett Universal II; IOL, intraocular lens; LT, lens thickness; ME, mean postoperative refractive error; MedAE, median absolute error; PE, postoperative refractive error; PEARL-DGS (PEARL), postoperative spherical equivalent prediction using artificial intelligence and linear algorithms developed by Debellemanière, Gatinel, and Saad; SD, standard deviation; SRK/T, Sanders-Retzlaff-Kraff/Theoretical; WTW, white-to-white.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank Enago (www.enago.com) for the English language.
Ethics Approval and Informed Consent
This study conforms to the ethical provisions outlined in the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest to declare for this work.
References
1. Sorkin N, Achiron A, Abumanhal M, et al. Comparison of two new integrated SS-OCT tomography and biometry devices. J Cataract Refract Surg. 2022;48(11):1277–1284. doi:10.1097/j.jcrs.0000000000000974
2. Stopyra W, Langenbucher A, Grzybowski A. Intraocular lens power calculation formulas-a systematic review. Ophthalmol Ther. 2023;12(6):2881–2902. doi:10.1007/s40123-023-00799-6
3. Lin L, Xu M, Mo E, et al. Accuracy of newer generation IOL power calculation formulas in eyes with high axial myopia. J Refract Surg. 2021;37(11):754–758. doi:10.3928/1081597X-20210712-08
4. Wendelstein J, Hoffmann P, Hirnschall N, et al. Project hyperopic power prediction: accuracy of 13 different concepts for intraocular lens calculation in short eyes. Br J Ophthalmol. 2022;106(6):795–801. doi:10.1136/bjophthalmol-2020-318272
5. Reitblat O, Levy A, Kleinmann G, Lerman TT, Assia EI. Intraocular lens power calculation for eyes with high and low average keratometry readings: comparison between various formulas. J Cataract Refract Surg. 2017;43(9):1149–1156. doi:10.1016/j.jcrs.2017.06.036
6. Hayashi K, Ogawa S, Yoshida M, Yoshimura K. Influence of patient age on intraocular lens power prediction error. Am J Ophthalmol. 2016;170:232–237. doi:10.1016/j.ajo.2016.08.016
7. Stopyra W. Comparison of the accuracy of six intraocular lens power calculation formulas for eyes of axial length exceeding 25.0mm. J Fr Ophtalmol. 2021;44(9):1332–1339. doi:10.1016/j.jfo.2021.04.009
8. Solomon R, Tamilarasi S, Sachdev G, Dandapani R. Accuracy of Barrett versus third-generation intraocular lens formula across all axial lengths. Oman J Ophthalmol. 2022;15(3):290–294. doi:10.4103/ojo.ojo_188_21
9. Shammas HJ, Taroni L, Pellegrini M, Shammas MC, Jivrajka RV. Accuracy of newer intraocular lens power formulas in short and long eyes using sum-of-segments biometry. J Cataract Refract Surg. 2022;48(10):1113–1120. doi:10.1097/j.jcrs.0000000000000958
10. Hipólito-Fernandes D, Luís ME, Serras-Pereira R, et al. Anterior chamber depth, lens thickness and intraocular lens calculation formula accuracy: nine formulas comparison. Br J Ophthalmol. 2022;106(3):349–355. doi:10.1136/bjophthalmol-2020-317822
11. Retzlaff JA, Sanders DR, Kraff MC. Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg. 1990;16(3):333–340. doi:10.1016/S0886-3350(13)80705-5
12. Barrett Universal. Formula version1.05. Available from: http://calc.apacrs.org/barrett_universal2105/.
13. IOLsolver. Pearl DGS formula. Available from: https://iolsolver.com/.
14. Hoffer KJ, Savini G. Update on intraocular lens power calculation study protocols: the better way to design and report clinical trials. Ophthalmology. 2021;128(11):e115–e120. doi:10.1016/j.ophtha.2020.07.005
15. Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. doi:10.1038/bmt.2012.244
16. Hipólito-Fernandes D, Elisa Luís M, Gil P, et al. VRF-G, a new intraocular lens power calculation formula: a 13-formulas comparison study. Clin Ophthalmol. 2020;14:4395–4402. doi:10.2147/OPTH.S290125
17. Cheng H, Kane JX, Liu L, Li J, Cheng B, Wu M. Refractive predictability using the IOLMaster 700 and artificial intelligence-based IOL power formulas compared to standard formulas. J Refract Surg. 2020;36(7):466–472. doi:10.3928/1081597X-20200514-02
18. Koga Y, Kojima K, Yoshii K, et al. Prediction error of intraocular lens power calculation in very elderly patients over 90 years old. Curr Eye Res. 2021;46(8):1148–1153. doi:10.1080/02713683.2020.1858486
19. Sella R, Chou L, Schuster AK, Gali HE, Weinreb RN, Afshari NA. Accuracy of IOL power calculations in the very elderly. Eye. 2020;34(10):1848–1855. doi:10.1038/s41433-019-0752-0
20. Li Y, Guo C, Huang C, et al. Development and evaluation of the prognostic nomogram to predict refractive error in patients with primary angle-closure glaucoma who underwent cataract surgery combined with goniosynechialysis. Front Med Lausanne. 2021;8:749903. doi:10.3389/fmed.2021.749903
21. Lee Y, Kim MK, Oh JY, Choi HJ, Yoon CH, Bayoumi NHL. Intraocular lens power calculation in eyes with a shallow anterior chamber depth and normal axial length. PLoS One. 2023;18(7):e0288554. doi:10.1371/journal.pone.0288554
22. Yesilkaya EC, Garip R. Accuracy of different lens power calculation formulas in patients with mature cataracts. Cureus. 2023;15(10):e47053. doi:10.7759/cureus.47053
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.