")
Back to Journals » International Journal of General Medicine » Volume 18
Role of Peripheral Blood Regulatory T Cells and IL-2 in the Collateral Circulation of Acute Ischemic Stroke
Authors Zhang S, Rao C, Wen M, Zhang X, Zha Z, Gu T, Zhu L , Yu C
Received 1 November 2024
Accepted for publication 20 February 2025
Published 25 February 2025 Volume 2025:18 Pages 1075—1088
DOI https://doi.org/10.2147/IJGM.S504218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Redoy Ranjan
Simin Zhang,1,2,* Chen Rao,1,2,* Meihai Wen,3 Xuke Zhang,3 Zhiwen Zha,1,2 Tong Gu,1,2 Lei Zhu,1,2 Chuanqing Yu1,2
1The Medical School of Anhui University of Science & Technology, Huainan, Anhui Province, 232000, People’s Republic of China; 2Department of Neurology, The First Hospital of Anhui University of Science & Technology (The First People’s Hospital of Huainan), Huainan, Anhui Province, 232000, People’s Republic of China; 3Bengbu Medical University, Bengbu, Anhui Province, 233000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chuanqing Yu; Lei Zhu, Email [email protected]; [email protected]
Background: Inflammation is recognized as a pivotal factor in the pathophysiology of acute ischemic stroke (AIS) and has the potential to influence the collateral circulation of patients. The objective of this investigation was to explore the link between peripheral regulatory T cells (Tregs), interleukin-2 (IL-2), and the status of collateral circulation.
Methods: Between September 2023 and May 2024, the study incorporated 117 AIS patients from the neurology department, with 60 identified as having good collateral status (GCS) and 57 with poor collateral status (PCS). Additionally, a control group of 46 healthy individuals was included. Collateral circulation in AIS patients was assessed via computed tomography angiography. The levels of peripheral blood Tregs were quantified through flow cytometry, while IL-2 was measured by ELISA.
Results: In this investigation, patients diagnosed with PCS demonstrated reduced Tregs (5.77 ± 1.55%) and IL-2 levels (7.37 ± 2.61 pg/mL) compared to individuals with GCS (7.09 ± 1.32%, 9.95 ± 3.58 pg/mL) and healthy controls (7.17 ± 1.40%,10.33 ± 4.01 pg/mL). Logistic regression analysis identified significant associations between Tregs and IL-2 levels and collateral circulation status (p< 0.05), with diminished levels of both being independent predictors of PCS when compared to GCS. A nomogram was developed to forecast risk factors for collateral circulation, further highlighting the potential of plasma Tregs and IL-2 levels as biomarkers in predicting collateral circulation among AIS patients. The diagnostic performance of Tregs and IL-2 was assessed utilizing receiver operating characteristic (ROC) analysis. The area under the ROC curve (AUC) for Tregs in differentiating GCS from PCS patients was ascertained to be 0.741 (95% confidence interval [CI]: 0.652– 0.830), while for IL-2, it was 0.710 (95% CI: 0.618– 0.803). Moreover, the combined measurement of Tregs and IL-2 resulted in an AUC of 0.779 (95% CI: 0.695– 0.863).
Conclusion: Plasma levels of peripheral blood Tregs and IL-2 may function as promising biomarkers for the prediction of collateral circulation status, suggesting potential new therapeutic approaches aimed at enhancing cerebral collateral circulation, and providing new therapeutic targets for acute ischemic stroke.
Keywords: acute ischemic stroke, collateral circulation, interleukin-2, neuroinflammation, regulatory T cells
Graphical Abstract:

Introduction
Acute ischemic stroke (AIS) ranks among the primary contributors to mortality and long-term disability worldwide, exerting considerable economic strain on both society and families.1 Cerebral collateral circulation serves a pivotal function in safeguarding the brain from ischemic and reperfusion injury.2 In the event of stenosis or occlusion of cerebral blood vessels, collateral circulation permits the delivery of blood to the infarct-adjacent region, commonly referred to as the penumbra, thus offering protection to the ischemic brain tissue in that area.3 Good collateral status (GCS) has been linked to improved clinical outcomes in AIS patients undergoing intravenous thrombolysis or endovascular therapy.4
Clinically, the assessment of collateral circulation is predominantly performed using imaging techniques, with digital subtraction angiography (DSA) widely acknowledged as the premier approach for detecting collateral circulation status.5 Despite its accuracy, the invasive nature of DSA limits its widespread use. Computed tomography angiography (CTA), valued for its non-invasive approach, has emerged as a preferable method for evaluating collateral circulation in AIS patients.6 However, various neuroimaging techniques are often confined to major stroke centers and are inaccessible in numerous other regions, hindering the ability to monitor dynamic changes in collateral circulation during long-term follow-up of ischemic stroke.7 At present, effective and sensitive biomarkers for predicting collateral circulation remain unavailable. Thus, identifying reliable biomarkers is of great significance for predicting collateral circulation and determining the clinical prognosis.
Inflammation is recognized as a key factor in the pathophysiology of ischemic stroke, encompassing a complex interplay of various cell types and effector molecules, impacting tissues beyond the central nervous system.8 Uncontrolled and excessive inflammatory responses exacerbate ischemic brain damage and impede post-stroke cerebral recovery. Regulatory T cells (Tregs), a vital subgroup of anti-inflammatory T cells, serve a function in mediating immune tolerance and ensuring tissue homeostasis.9,10 Tregs are involved in post-ischemic stroke inflammatory and immune responses via multiple mechanisms, significantly contributing to the limitation of brain damage and the promotion of recovery after stroke. In addition to stroke, research indicates that Tregs play a critical role in cardiovascular diseases, diabetes, and other conditions. In cardiovascular diseases, Tregs can limit the inflammatory response in atherosclerotic plaques, thereby reducing plaque rupture and subsequent cardiovascular events.11 Similarly, in diabetes, Tregs are involved in maintaining immune tolerance, and their dysfunction is closely associated with the onset and progression of type 2 diabetes.12
Interleukin-2 (IL-2), commonly called T cell growth factor, is produced by T lymphocytes in response to antigenic stimulation and is crucial for regulatory T cells expansion. Previous studies have demonstrated that defects in the IL-2 receptor and its downstream signaling pathways are closely linked to the pathogenesis of type 1 diabetes, and enhancing IL-2 signaling can prevent and reverse the disease by restoring Tregs cell function.13 Additionally, research has shown that a single intravenous injection of recombinant human interleukin-2 (rhIL-2) improves cardiac function after myocardial infarction by promoting angiogenesis and activating natural killer (NK) cells.14 Following ischemic stroke, IL-2 exerts neuroprotective effects by promoting Tregs expansion and inhibiting inflammation.
Nevertheless, it remains unclear whether Tregs and IL-2 have additional roles following ischemic stroke, particularly concerning their potential impact on cerebral collateral circulation post-ischemia. This study aims to investigate the association between two systemic immune-inflammatory markers, Tregs and IL-2, and the collateral circulation status in AIS patients through flow cytometry and enzyme-linked immunosorbent assay (ELISA), highlighting their potential as biomarkers for predicting and improving treatment outcomes.
Materials and Methods
Study Design and Subjects
The study design flowchart is presented in Figure 1. This investigation is a retrospective, single-center, observational case-control study. Between September 2023 and May 2024, AIS patients who received treatment at the Department of Neurology, The First Hospital of Anhui University of Science & Technology, were prospectively enrolled.
 |
Figure 1 Flow chart of the study design. |
The inclusion criteria were as follows: (1) A clinical diagnosis of AIS verified through cranial magnetic resonance imaging and diffusion-weighted imaging; (2) Symptom onset within 3 days; (3) Patients aged 18 years or older; (4) The presence of intracranial atherosclerotic stenosis (≥50%) or occlusion in the anterior circulation, confirmed by CTA within 7 days after symptom onset.
The exclusion criteria included the following: (1) Intracranial hemorrhage identified through neuroimaging; (2) A confirmed life expectancy of less than 6 months, attributable to cancer or severe systemic diseases; (3) Presence of chronic inflammatory conditions, pregnancy, or being a kidney transplant recipient; (4) A history of trauma, surgical procedures, or administration of steroids, immunosuppressants, immunomodulators, or antibiotics within 30 days prior to hospitalization; (5) Evidence of active infection (body temperature >37.5 °C, increased white blood cell [WBC] count), symptoms such as productive cough, urinary dysfunction, or diarrhea; (6) Thrombolysis or thrombectomy following stroke onset, as well as a baseline modified Rankin Scale (mRS) score of ≥2.
Collateral circulation status was not utilized as an inclusion criterion in this study. It was assessed by independent, blinded observers through the previously established TAN scoring system.15 AIS patients were categorized into two groups: individuals with GCS (TAN 2–3) and those with poor collateral circulation (PCS, TAN 0–1). Healthy volunteers, free of any stroke history, were selected as the control group and matched with AIS patients based on age and gender, minimizing the confounding effects of other risk factors.
Clinical Examination
Demographic information, including age, epidemiological details, and comorbidities, was extracted from the participant’s medical records. Laboratory findings such as WBC count, renal function, lipid profile, cystatin C, fasting blood glucose, lipoprotein (a), and homocysteine levels were recorded. Upon admission, professionally trained neurologists evaluated the severity of neurological deficits in all AIS patients utilizing the National Institutes of Health Stroke Scale (NIHSS). At 90 days following the onset of stroke, the mRS was employed to score the patients.
Measurement of Peripheral Blood Tregs and IL-2
Peripheral blood samples (2 mL) were drawn from AIS patients on the second-day post-admission, with control group samples obtained during routine physical examinations, all under fasting conditions. Flow cytometry was employed to examine the expression of specific surface antigens on circulating Tregs. Specifically, 100 μL of peripheral blood underwent incubation with the following monoclonal antibodies for labeling: 20 μL anti-CD3, 20 μL anti-CD4, 20 μL anti-CD25, and 20 μL anti-CD127 (BD, Franklin Lakes, NJ, USA). The cells were evaluated utilizing a FACSCanto II flow cytometer (BD, Franklin Lakes, NJ, USA) and processed via Kaluza analysis software (Beckman Coulter, Brea, CA, USA). Tregs were defined as CD4+/CD25+/CD127 low-stained cells within the lymphocyte gate. For all analyses, Tregs% was represented as the proportion of Tregs relative to the total CD4+ lymphocyte population.
Additionally, 4 mL of peripheral blood was collected under fasting conditions on the second day (for controls, this occurred during the physical examination). Plasma IL-2 levels were quantified using an ELISA kit (IL-2 ELISA kit, double antibody sandwich method, catalog number 11321001; Hunan Xieguang Biotechnology Co., Ltd., Hunan, China) per the supplier’s protocols.
Statistical Analysis
All statistical analyses were conducted utilizing SPSS 27.0 software (IBM, Chicago, IL, USA). Quantitative data with normal distribution were denoted as mean ± standard deviation and compared between groups through t-tests. Data with non-normal distribution were denoted as median (interquartile range) [M(IQR)] and examined utilizing Mann–Whitney U-tests. Categorical variables were displayed as frequency (percentage) [n(%)] and examined utilizing χ2 tests. Bivariate correlations were assessed with Pearson coefficients for normally distributed variables and Spearman coefficients for non-normally distributed variables. Logistic regression analysis was applied to explore the association between Tregs and IL-2 with varying collateral circulation states. A receiver operating characteristic (ROC) curve evaluation was executed to assess Tregs’ and IL-2’s predictive ability to regulate different collateral circulation statuses. A P-value < 0.05 was deemed statistically significant.
Results
Participant Characteristics
This investigation encompassed 46 healthy controls, 60 patients with AIS and GCS, and 57 patients with AIS and PCS (Table 1). In comparison to the healthy control group, AIS patients demonstrated lower levels of lymphocytes, Tregs and IL-2 (Figure 2A and B), along with elevated systolic and diastolic blood pressure, a greater incidence of hypertension and diabetes, and increased levels of WBCs, neutrophil percentage (NEUT%), neutrophils, fasting blood glucose, homocysteine (HCY), creatinine (Cr), Cystatin-C, and low-density lipoprotein (LDL). No notable disparities in age, gender, other medical histories, or laboratory data were identified between the groups (Table 1).
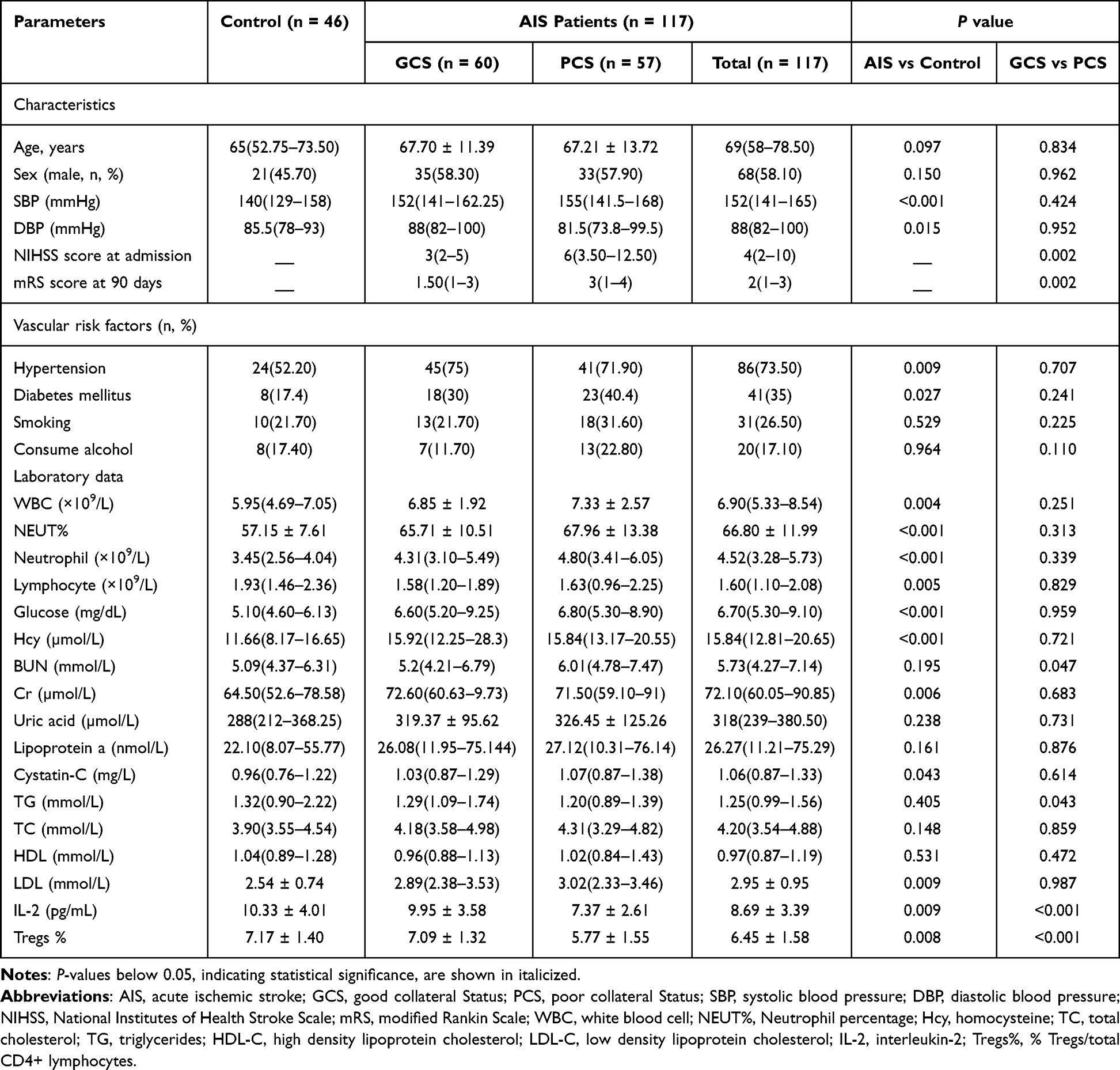 |
Table 1 Baseline Characteristics of Control and Patients with AIS |
 |
Figure 2 (A) Plasma IL-2 levels were lower in the AIS group compared to the control group. (B) Plasma Treg levels were lower in the AIS group compared to the control group. (C) Plasma IL-2 levels were lower in the PCS group compared to the GCS group. (D) Plasma Treg levels were lower in the PSC group compared to the GCS group. Indicators (**): express p<0.01, Indicators (***): express p<0.001. |
In addition, when compared to the PCS group, patients in the GCS group showed higher Treg and IL-2 levels (Figure 2C and D), lower NIHSS scores upon admission, lower mRS scores 90 days post-stroke, lower blood urea nitrogen (BUN) levels, and higher triglyceride (TG) levels. No notable disparities in age, gender, blood pressure, or vascular risk factors were noted between the GCS and PCS groups. Furthermore, no notable differences in other laboratory data were found between these two groups (Table 1).
Correlation Between Peripheral Blood Tregs and IL-2 Levels and Clinical Indicators
Correlation analyses, utilizing Pearson for normally distributed variables and Spearman for non-normally distributed variables, were performed to assess the relationships between Tregs, IL-2, and clinical indicators in AIS patients (Figure 3A–E). A significant positive association was detected between Tregs and IL-2 levels (r = 0.3849; p < 0.0001). Negative correlations were noted between Tregs levels and NIHSS scores (r = −0.2701; p = 0.0032), 90-day mRS scores (r = −0.4763; p < 0.0001), and SBP (r = −0.2472; p = 0.0072) (Supplementary Figure 1A). Similarly, IL-2 levels displayed negative associations with NIHSS scores (r = −0.1958; p = 0.0319), 90-day mRS scores (r = −0.2742; p = 0.0028), and systolic blood pressure (r = −0.2765; p = 0.0025) (Supplementary Figure 1B), while exhibiting a positive link to glucose (GLU) levels (r = 0.1886; p = 0.0417) (Supplementary Figure 1C).
 |
Figure 3 Correlation between peripheral blood Tregs and IL-2 levels with clinical indicators. (A) Treg levels show a significant positive correlation with IL-2 levels. (B) Treg levels are negatively correlated with NIHSS scores. (C) IL-2 levels are negatively correlated with NIHSS scores. (D) Treg levels are negatively correlated with 90-day mRS scores. (E) IL-2 levels are negatively correlated with 90-day mRS scores. |
Predictive Potential of Tregs and IL-2
To assess the predictive potential of Tregs and IL-2, logistic regression analysis, a nomogram, and ROC curve analysis were employed. Logistic regression analysis demonstrated that Tregs and IL-2 levels were linked to collateral circulation in both unadjusted and adjusted models. After adjusting for age, gender, blood pressure, vascular risk factors, and variables with p < 0.05 in the univariate analysis (laboratory data, NIHSS score at admission), low levels of Tregs and IL-2 remained independent predictors of PCS (compared to the GCS group) (Table 2). Moreover, a nomogram model was constructed to predict collateral circulation risk factors (Figures 4, 5, Supplementary Figure 2). These findings support the potential of plasma Tregs and IL-2 levels as biomarkers for predicting collateral circulation in AIS patients. Subsequently, ROC curve analysis was executed to assess the diagnostic efficiency of Tregs and IL-2. The area under the ROC curve (AUC) for Tregs in distinguishing GCS patients from PCS patients was 0.741 (0.652–0.830), while the AUC for IL-2 was 0.710 (0.618–0.803) (Figure 6A, Table 2). Furthermore, the AUC for the combination of Tregs and IL-2 reached 0.779 (Figure 6B).
 |
Table 2 Correlation Analysis of Biomarkers with Different Collaterals |
 |
Figure 4 Nomogram for collateral circulation risk factors. |
 |
Figure 5 Decision curve analysis for the collateral circulation risk nomogram. |
 |
Figure 6 Diagnostic efficiency of Tregs and IL-2. (A) ROC curves of plasma Tregs and IL-2 distinguish between GCS and PCS groups. (B) ROC curve for the combination of Tregs and IL-2. |
Subgroup Analysis
To further investigate the relationship between Tregs, IL-2, and collateral circulation status, we performed a series of subgroup analyses. As illustrated in Figure 7, none of the subgroups, including age, sex, the presence of hypertension or diabetes, as well as smoking and alcohol consumption, significantly modified the association between Tregs, IL-2, and collateral circulation status (all P values for interaction > 0.05).
 |
Figure 7 Subgroup analyses of the association between the Tregs, IL-2, and collateral circulation status. |
Discussion
In this study, plasma Tregs and IL-2 levels were compared between AIS patients and control groups, as well as between GCS and PCS patients. The key findings are as follows: (1) Plasma Tregs and IL-2 levels effectively distinguished GCS from PCS patients, with PCS patients displaying significantly lower levels of both markers in comparison to GCS patients and healthy controls. (2) A notable negative association was observed between Tregs and IL-2 levels and NIHSS scores at admission, as well as 90-day mRS scores. (3) Plasma Tregs and IL-2 levels were strongly linked to collateral circulation status in individuals with AIS, with lower levels of these markers identified as independent predictors of PCS. In conclusion, these results underscore the predictive value of plasma Tregs and IL-2 for assessing collateral circulation status in AIS patients, suggesting their potential as biomarkers and therapeutic targets for this patient population.
An increasing body of research indicates that collateral circulation is a key factor in determining clinical outcomes in AIS patients, regardless of whether they undergo acute reperfusion therapy.16,17 In individuals with adequate cerebral collateral blood supply, brain tissue within the affected vascular region may remain viable for an extended duration before evolving into an ischemic core.15 In this investigation, GCS patients were observed to exhibit milder neurological impairments. Moreover, 90-day functional outcomes, as measured by mRS scores, revealed that GCS patients had better daily living abilities. These observations are consistent with the findings of earlier research.
The development of collateral circulation in patients with AIS is influenced by several factors, including genetics, aging, sex, neurological pathways, and vascular risk conditions such as diabetes and hypertension.18 It has been suggested that heightened inflammatory responses following ischemic stroke can negatively influence collateral circulation formation.19 Inflammation negatively impacts collateral vessel formation through various mechanisms, one of which may involve a reduction in the number of endothelial progenitor cells, thereby hindering the development of collateral vessels.20 Early brain edema is partially mediated by inflammatory pathways, which may increase the resistance in collateral arterioles, ultimately leading to collateral circulation failure.21,22 Tregs play a crucial role in this process. Prior studies have highlighted the critical role of Tregs in maintaining immune tolerance and mitigating inflammatory collateral damage by regulating self-reactive immune responses.23,24 One investigation revealed that Tregs are capable of inhibiting the expression of neutrophil-derived matrix metalloproteinase-9 (MMP-9) and safeguarding the blood-brain barrier to mitigate cerebral damage after AIS. This mechanism requires cell-to-cell interaction and is mediated through PD-1/PD-L1 signaling.25 Furthermore, Tregs modulate the function of effector T cells by secreting inhibitory cytokines such as TGF-β, IL-10, and IL-35, thereby suppressing excessive inflammatory responses and reducing the potential damage to collateral vessels. Through this immune regulatory function, Tregs help alleviate inflammatory damage in collateral circulation and promote vascular stability and functional recovery. Moreover, another study observed a correlation between low MMP-9 levels and high monocyte chemoattractant protein-1 levels with GCS status prior to treatment.26 These studies suggest that Tregs, by regulating immune responses and particularly through the secretion of inhibitory cytokines to control inflammation, may play a significant role in the formation of collateral circulation following ischemic stroke. This study found that early peripheral blood Tregs in ischemic stroke patients were reduced when compared with a healthy control group, aligning with findings from Ruhnau et al.27 Furthermore, a negative correlation was identified between Tregs and 90-day mRS scores (r = −0.2742; p = 0.0028), indicating that elevated levels of Tregs are predictive of improved clinical outcomes. It was also demonstrated that GCS patients exhibited higher plasma Tregs levels than PCS patients, suggesting that elevated Tregs levels may enhance the development of collateral circulation.
Beyond their immunoregulatory role, emerging evidence underscores the significant involvement of Tregs in angiogenesis.28 The involvement of Tregs in angiogenesis has been investigated across a range of disease conditions, particularly in the field of oncology, due to their considerable therapeutic potential. The relationship between angiogenesis and Tregs can be classified into two mechanisms: one involves the VEGF signaling pathway, while the other is mediated through the regulation of other immune cells and the secretion of pro-angiogenic cytokines and growth factors. Studies providing direct evidence of Tregs regulating VEGF signaling are relatively scarce. Li et al29 demonstrated that Helios+ Tregs facilitate angiogenesis in the bone marrow of acute lymphoblastic leukemia mice via the VEGF-A/VEGFR-2 pathway. Similarly, Facciabene et al30 discovered that tumor hypoxia triggers an upregulation of chemokine CC-chemokine ligand 28, facilitating increased Tregs levels in tumors, which in turn promote angiogenesis by elevating VEGFA levels in the tumor microenvironment. In addition to their VEGF-mediated effects, Tregs can also indirectly influence angiogenesis by regulating the function of other immune cells. D’Alessio et al31 found that Tregs promote pulmonary angiogenesis by regulating macrophages and their cytokines, and their depletion leads to reduced angiogenesis and a decrease in macrophage numbers. Another study showed that hyperforin enhances Tregs infiltration in the ischemic hemisphere, increasing Treg-derived cytokines such as IL-10 and TGF-β in an astrocyte IL-6-dependent manner, thereby promoting neurovascular regeneration post-stroke.32 In conclusion, these findings support the hypothesis that Tregs may offer a protective effect on collateral circulation. However, the precise mechanisms require further elucidation.
IL-2, recognized as a growth factor essential for the proliferation of human T cells, plays a pivotal role in facilitating the differentiation and conversion of naive CD4+ T cells.33 Numerous studies have demonstrated a close association between IL-2 and Tregs. Post-stroke treatment with IL-2:IL-2 antibody complexes has been shown to elevate Tregs populations.34 Moreover, additional research indicates that IL-2, beyond its function in the generation of splenic and peripherally induced Tregs and maintaining the balance of peripherally induced Tregs, is crucial through its activation of signal transducer and activator of transcription 5 to enhance the suppressive function of Tregs.35 Although IL-2 plays a critical role in immune regulation by promoting the proliferation and functional enhancement of Tregs, its effects following ischemic stroke extend beyond immune tolerance. In fact, IL-2 may indirectly enhance the formation of collateral circulation and angiogenesis by increasing the number and suppressive activity of Tregs, thereby contributing positively to tissue repair and recovery.
Certainly, existing studies also suggest that IL-2 can promote angiogenesis by activating other immune cells. Previous research has demonstrated that IL-2-activated NK cells interact with TNF-α-stimulated endothelial cells to stimulate their proliferation and promote angiogenesis through mechanisms involving α4β7 integrin and killer cell lectin-like receptor 1.36 Additionally, IL-2 promotes angiogenesis by activating ROS and Akt signaling pathways, which enhance the expression of angiogenic factors such as VEGF and PDGF, stimulate tube formation in human umbilical vein endothelial cells, and its angiogenic effects have been confirmed in animal models.37 In this investigation, a notable positive association between Tregs and IL-2 levels (r = 0.3849; p < 0.0001) was observed, corroborating the previously established link between IL-2 and Tregs. Additionally, IL-2 levels were inversely linked to NIHSS scores (r = −0.1958; p = 0.0319) and 90-day mRS scores (r = −0.2742; p = 0.0028), implying that IL-2 could potentially serve as a biomarker for predicting functional outcomes and disease severity. Furthermore, IL-2 levels in the peripheral blood of AIS patients were noted to be diminished in the early stages relative to those in the healthy control group, with PCS patients exhibiting lower IL-2 levels than GCS patients. Supporting these findings, Nayak et al38 also reported that IL-2 may act as a biomarker for forecasting collateral circulation. However, it remains to be determined whether IL-2 influences collateral circulation through Tregs regulation or other pathways, warranting further investigation in future research.
Although Tregs represent only a small fraction of peripheral blood T cells and are present at low levels in ischemic brain tissue, effective strategies for stroke treatment have been developed through the ex vivo expansion of naturally derived thymus-originated autologous Tregs or by using biological and pharmacological agents to induce or expand Tregs in vivo. In recent years, novel Tregs genetic engineering techniques39 have been developed to enhance the functionality, specificity, and delivery efficiency of Tregs. These techniques have shown initial progress in clinical trials related to transplantation and are expected to provide further support for the treatment of stroke and other neurological diseases. Moreover, several studies have demonstrated that IL-2 primarily exerts its therapeutic effects by increasing the number of Tregs in stroke models. Systemic injection of IL-2/IL-2Ab complexes has been shown to effectively increase Tregs numbers in blood and lymphoid tissues, reduce infarct volume, alleviate neuroinflammation, and improve sensory and motor function.40 Additionally, IL-2 gene delivery targeting astrocytes has been shown to specifically increase brain Tregs, thereby providing effective protection against inflammatory damage in the brain.41 This discovery offers a potential delivery platform for clinical applications. Overall, these therapeutic strategies offer diverse treatment options for ischemic stroke and demonstrate significant potential. However, the efficacy and safety of these approaches require further validation through additional clinical trials, particularly for their application in stroke treatment. As research progresses and clinical validation continues, Tregs cell therapies and IL-2 are expected to become key treatment modalities for stroke and other neurological diseases.
Certain limitations of this investigation must be recognized. First, the single-phase CTA employed here may not be the most suitable method for the evaluation of collateral circulation. More comprehensive approaches, such as multi-phase CTA or DSA, could provide more precise assessments. Furthermore, the study was restricted to analyzing peripheral blood samples due to the difficulty of obtaining Tregs and IL-2 data from the brains of AIS patients. Additionally, since the collection of blood samples occurred outside the acute reperfusion therapy window for cerebral infarction, it remains uncertain whether Tregs and IL-2 levels can accurately reflect the status of collateral circulation during this critical therapeutic period, necessitating further investigation in future research. Lastly, the sample size was limited, further research with larger sample sizes is needed to explore the relationship between Tregs, IL-2, and collateral circulation. Additionally, more clinical trials or multi-center studies are required to validate the generalizability of these results.
Conclusion
The results of this investigation demonstrated that reduced levels of Tregs and IL-2 were linked to PCS status before treatment, indicating a potential relationship between the status of collateral circulation and immune inflammation. Peripheral blood Tregs and IL-2 concentrations might function as useful prognostic indicators for evaluating collateral circulation status. In the future, the regulation of Tregs and IL-2 levels could offer promising therapeutic approaches for enhancing cerebral collateral circulation, and providing new therapeutic targets for acute ischemic stroke.
Data Sharing Statement
The data underlying this study are accessible through the corresponding author upon justified request.
Ethics Statement
This clinical study received approval from the Ethics Committee of the First Affiliated Hospital of Anhui University of Science and Technology (approval number: 2023-KY-B104-001). The research complied with the ethical guidelines outlined in the Declaration of Helsinki, and informed consent was secured from all participants.
Acknowledgments
The authors would like to thank all the investigators who contributed to this study and thank Bullet Edits Limited for the linguistic editing and proofreading of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Anhui Provincial Health and Wellness Research Program (Grant No. AHWJ2023A20160), Stroke prevention and treatment technology research project (Grant No. WKZX2023CZ0115), and Medical Special Project of Anhui University of Science and Technology (Grant No. YZ2023H1C001).
Disclosure
There are no competing interests declared by the authors.
References
1. Feigin VL, Brainin M, Norrving B, et al. World stroke organization (WSO): global stroke fact sheet 2022. Inter J Stroke Official J Inter Stroke Soc. 2022;17(1):18–29. doi:10.1177/17474930211065917
2. Maguida G, Shuaib A. Collateral circulation in ischemic stroke: an updated review. J Stroke. 2023;25(2):179–198. doi:10.5853/jos.2022.02936
3. Soares BP, Tong E, Hom J, et al. Reperfusion is a more accurate predictor of follow-up infarct volume than recanalization: a proof of concept using CT in acute ischemic stroke patients. Stroke. 2010;41(1):e34–40. doi:10.1161/strokeaha.109.568766
4. Leng X, Leung TW. Collateral flow in intracranial atherosclerotic disease. Transl Stroke Res. 2023;14(1):38–52. doi:10.1007/s12975-022-01042-3
5. Liebeskind DS. Imaging the future of stroke: i. Ischemia. Ann Neurol. 2009;66(5):574–590. doi:10.1002/ana.21787
6. Sadeh-Gonik U, Budylev A, Krivitzky D, et al. Circle of Willis integrity in acute middle cerebral artery occlusion: does the posterior communicating artery matter? J Neurointerv Surg. 2024;16(8):801–808. doi:10.1136/jnis-2023-020326
7. Tian DS, Qin C, Zhou LQ, et al. FSAP aggravated endothelial dysfunction and neurological deficits in acute ischemic stroke due to large vessel occlusion. Signal Transduct Target Ther. 2022;7(1):6. doi:10.1038/s41392-021-00802-1
8. DeLong JH, Ohashi SN, O’Connor KC, Sansing LH. Inflammatory responses after ischemic stroke. Semin Immunopathol. 2022;44(5):625–648. doi:10.1007/s00281-022-00943-7
9. Feng P, Yang Q, Luo L, et al. Vps34 sustains Treg cell survival and function via regulating intracellular redox homeostasis. Cell Death Differ. 2024;31(11):1519–1533. doi:10.1038/s41418-024-01353-y
10. Sakaguchi S, Sakaguchi N, Asano M, Itoh M, Toda M. Immunologic self-tolerance maintained by activated T cells expressing IL-2 receptor alpha-chains (CD25). Breakdown of a single mechanism of self-tolerance causes various autoimmune diseases. J Immunol. 1995;155(3):1151–1164. doi:10.4049/jimmunol.155.3.1151
11. Wang X, Zhou H, Liu Q, et al. Targeting regulatory T cells for cardiovascular diseases. Front Immunol. 2023;14:1126761. doi:10.3389/fimmu.2023.1126761
12. Zi C, He L, Yao H, Ren Y, He T, Gao Y. Changes of Th17 cells, regulatory T cells, Treg/Th17, IL-17 and IL-10 in patients with type 2 diabetes mellitus: a systematic review and meta-analysis. Endocrine. 2022;76(2):263–272. doi:10.1007/s12020-022-03043-6
13. Hulme MA, Wasserfall CH, Atkinson MA, Brusko TM. Central role for interleukin-2 in type 1 diabetes. Diabetes. 2012;61(1):14–22. doi:10.2337/db11-1213
14. Bouchentouf M, Williams P, Forner KA, et al. Interleukin-2 enhances angiogenesis and preserves cardiac function following myocardial infarction. Cytokine. 2011;56(3):732–738. doi:10.1016/j.cyto.2011.09.023
15. Olthuis SGH, Pirson FAV, Pinckaers FME, et al. Endovascular treatment versus no endovascular treatment after 6-24 h in patients with ischaemic stroke and collateral flow on CT angiography (MR CLEAN-LATE) in the Netherlands: a multicentre, open-label, blinded-endpoint, randomised, controlled, Phase 3 trial. Lancet. 2023;401(10385):1371–1380. doi:10.1016/s0140-6736(23)00575-5
16. Binder NF, El Amki M, Glück C, et al. Leptomeningeal collaterals regulate reperfusion in ischemic stroke and rescue the brain from futile recanalization. Neuron. 2024;112(9):1456–1472.e6. doi:10.1016/j.neuron.2024.01.031
17. Uniken Venema SM, Dankbaar JW, Wolff L, et al. Collateral status and recanalization after endovascular treatment for acute ischemic stroke. J Neurointerv Surg. 2023;15(6):531–538. doi:10.1136/neurintsurg-2021-018545
18. Mangiardi M, Bonura A, Iaccarino G, et al. The pathophysiology of collateral circulation in acute ischemic stroke. Diagnostics. 2023;13(14). doi:10.3390/diagnostics13142425
19. Lu M, Liu Y, Xian Z, et al. VEGF to CITED2 ratio predicts the collateral circulation of acute ischemic stroke. Front Neurol. 2022;13:1000992. doi:10.3389/fneur.2022.1000992
20. Edwards N, Langford-Smith AWW, Wilkinson FL, Alexander MY. Endothelial progenitor cells: new targets for therapeutics for inflammatory conditions with high cardiovascular risk. Front Med Lausanne. 2018;5:200. doi:10.3389/fmed.2018.00200
21. Rocha M, Jovin TG. Fast versus slow progressors of infarct growth in large vessel occlusion stroke: clinical and research implications. Stroke. 2017;48(9):2621–2627. doi:10.1161/strokeaha.117.017673
22. Broocks G, Kemmling A, Meyer L, et al. Computed tomography angiography collateral profile is directly linked to early edema progression rate in acute ischemic stroke. Stroke. 2019;50(12):3424–3430. doi:10.1161/strokeaha.119.027062
23. Sakaguchi S. Regulatory T cells: key controllers of immunologic self-tolerance. Cell. 2000;101(5):455–458. doi:10.1016/s0092-8674(00)80856-9
24. Wang HY, Ye JR, Cui LY, Chu SF, Chen NH. Regulatory T cells in ischemic stroke. Acta Pharmacol Sin. 2022;43(1):1–9. doi:10.1038/s41401-021-00641-4
25. Li P, Mao L, Liu X, et al. Essential role of program death 1-ligand 1 in regulatory T-cell-afforded protection against blood-brain barrier damage after stroke. Stroke. 2014;45(3):857–864. doi:10.1161/strokeaha.113.004100
26. Mechtouff L, Bochaton T, Paccalet A, et al. Matrix metalloproteinase-9 and monocyte chemoattractant protein-1 are associated with collateral status in acute ischemic stroke with large vessel occlusion. Stroke. 2020;51(7):2232–2235. doi:10.1161/STROKEAHA.120.029395
27. Ruhnau J, Schulze J, von Sarnowski B, et al. Reduced numbers and impaired function of regulatory T cells in peripheral blood of ischemic stroke patients. Mediators Inflamm. 2016;2016:2974605. doi:10.1155/2016/2974605
28. Astarita JL, Dominguez CX, Tan C, et al. Treg specialization and functions beyond immune suppression. Clin Exp Immunol. 2023;211(2):176–183. doi:10.1093/cei/uxac123
29. Li X, Li D, Shi Q, Huang X, Ju X. Umbilical cord blood‑derived Helios‑positive regulatory T cells promote angiogenesis in acute lymphoblastic leukemia in mice via CCL22 and the VEGFA‑VEGFR2 pathway. Mol Med Rep. 2019;19(5):4195–4204. doi:10.3892/mmr.2019.10074
30. Facciabene A, Peng X, Hagemann IS, et al. Tumour hypoxia promotes tolerance and angiogenesis via CCL28 and T(reg) cells. Nature. 2011;475(7355)::226–30. doi:10.1038/nature10169
31. D’Alessio FR, Zhong Q, Jenkins J, Moldobaeva A, Wagner EM. Lung angiogenesis requires CD4(+) forkhead homeobox protein-3(+) regulatory T cells. Am J Respir Cell mol Biol. 2015;52(5):603–610. doi:10.1165/rcmb.2014-0278OC
32. Yao H, Zhang Y, Shu H, et al. Hyperforin promotes post-stroke neuroangiogenesis via astrocytic IL-6-mediated negative immune regulation in the ischemic brain. Front Cell Neurosci. 2019;13:201. doi:10.3389/fncel.2019.00201
33. Spolski R, Li P, Leonard WJ. Biology and regulation of IL-2: from molecular mechanisms to human therapy. Nat Rev Immunol. 2018;18(10):648–659. doi:10.1038/s41577-018-0046-y
34. Shi L, Sun Z, Su W, et al. Treg cell-derived osteopontin promotes microglia-mediated white matter repair after ischemic stroke. Immunity. 2021;54(7):1527–1542.e8. doi:10.1016/j.immuni.2021.04.022
35. Chinen T, Kannan AK, Levine AG, et al. An essential role for the IL-2 receptor in T(reg) cell function. Nat Immunol. 2016;17(11):1322–1333. doi:10.1038/ni.3540
36. Bouchentouf M, Forner KA, Cuerquis J, et al. Induction of cardiac angiogenesis requires killer cell lectin-like receptor 1 and α4β7 integrin expression by NK cells. J Immunol. 2010;185(11):7014–7025. doi:10.4049/jimmunol.1001888
37. Bae J, Park D, Lee YS, Jeoung D. Interleukin-2 promotes angiogenesis by activation of Akt and increase of ROS. J Microbiol Biotechnol. 2008;18(2):377–382.
38. Nayak AR, Kashyap RS, Purohit HJ, Kabra D, Taori GM, Daginawala HF. Evaluation of the inflammatory response in sera from acute ischemic stroke patients by measurement of IL-2 and IL-10. Inflamm Res. 2009;58(10):687–691. doi:10.1007/s00011-009-0036-4
39. Ellis GI, Sheppard NC, Riley JL. Genetic engineering of T cells for immunotherapy. Nat Rev Genet. 2021;22(7):427–447. doi:10.1038/s41576-021-00329-9
40. Zhang H, Xia Y, Ye Q, et al. In vivo expansion of regulatory T cells with IL-2/IL-2 antibody complex protects against transient ischemic stroke. J Neurosci. 2018;38(47):10168–10179. doi:10.1523/jneurosci.3411-17.2018
41. Yshii L, Pasciuto E, Bielefeld P, et al. Astrocyte-targeted gene delivery of interleukin 2 specifically increases brain-resident regulatory T cell numbers and protects against pathological neuroinflammation. Nat Immunol. 2022;23(6):878–891. doi:10.1038/s41590-022-01208-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Neutrophil to High-Density Lipoprotein Ratio is Associated with Hemorrhagic Transformation in Patients with Acute Ischemic Stroke
Zhang R, Jin F, Zheng L, Liao T, Guan G, Wang J, Zhao S, Fei S, Chu Z, Xu Y
Journal of Inflammation Research 2022, 15:6073-6085
Published Date: 4 November 2022