")
Back to Journals » Clinical Ophthalmology » Volume 18
Safety and Efficacy of STREAMLINE Canaloplasty with Phacoemulsification in Hispanic Adults with Open-Angle Glaucoma: 12-Month Outcomes
Authors Lazcano-Gomez G , Orlich C, Batlle JF , Ison EM, Reynolds HP, Harbin M , Kahook MY
Received 16 April 2024
Accepted for publication 14 November 2024
Published 27 December 2024 Volume 2024:18 Pages 3967—3976
DOI https://doi.org/10.2147/OPTH.S473981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gabriel Lazcano-Gomez,1 Claudio Orlich,2 Juan F Batlle,3 Elysia M Ison,4 Heather P Reynolds,4 Med Harbin,4 Malik Y Kahook5
1Department of Glaucoma, Clínica Laser y Ultrasonido Ocular, Puebla City, Mexico; 2Clinica 20/20, San José, Costa Rica; 3Laser Center, Santo Domingo, Dominican Republic; 4New World Medical, Inc., Rancho Cucamonga, CA, USA; 5Department of Ophthalmology, University of Colorado Anschutz Medical Campus, Aurora, CO, USA
Correspondence: Malik Y Kahook, Department of Ophthalmology, University of Colorado Anschutz Medical Campus, Aurora, CO, USA, Tel +1 720 848 2501, Email [email protected]
Purpose: To report the 12-month clinical outcomes in eyes with mild to moderate open-angle glaucoma (OAG) in Hispanic adults undergoing STREAMLINE Surgical System (STREAMLINE) canaloplasty combined with phacoemulsification.
Patients and Methods: This was a prospective, multi-center, interventional clinical trial involving 45 eyes of 45 Hispanic adult patients receiving topical medical therapy for mild to moderate OAG and undergoing phacoemulsification surgery for visually significant cataracts at three sites. All eyes underwent a Screening visit, followed by medication washout and a subsequent Baseline visit to determine eligibility for STREAMLINE canaloplasty. The primary outcome was the proportion of unmedicated eyes with intraocular pressure (IOP) reduction of ≥ 20% from Baseline at Month 12. Secondary outcomes included mean change in IOP from post-washout Baseline, mean change in IOP-lowering medications compared to pre-washout Screening, and adverse events (AEs).
Results: 43 eyes met the eligibility criteria for analysis and 40 eyes completed the 12-month visit. The mean (standard deviation) age was 68.7 (8.6 years), 76.7% were female, and 72.1% of the eyes were classified as having mild OAG. The mean number of IOP-lowering medications at Screening was 1.95 (0.82). After washout, the Baseline mean IOP was 23.0 (1.8) mmHg. At Month 12, 28/40 eyes (70.0%) remained medication-free, of which 27 (96.4%) had an IOP reduction of ≥ 20% from Baseline. The mean IOP at Month 12 was 15.3 (2.8) mmHg, a reduction of 7.8 (3.0) mmHg from Baseline (p< 0.001). The mean medication use at Month 12 was 0.63 (1.19) per eye, representing a mean reduction of 1.38 (1.03) medications from Screening (p< 0.001). Device- or procedure-related ocular AEs were mostly mild in severity and self-limited.
Conclusion: STREAMLINE canaloplasty in combination with phacoemulsification provides clinically and statistically significant reduction in IOP and IOP-lowering medications in eyes with mild to moderate OAG in Hispanic adults.
Keywords: STREAMLINE Surgical System, canaloplasty, intraocular pressure, minimally invasive glaucoma surgery, open-angle glaucoma
Introduction
Minimally invasive glaucoma surgery (MIGS) has transformed the surgical approach to lowering intraocular pressure (IOP) by providing safer surgical options that can be used early in the treatment paradigm. Collectively, the MIGS family of procedures—including canaloplasty, goniotomy, and implanted trabecular meshwork (TM) bypass stents—have provided a safe and effective surgical option for patients with mild to moderate glaucoma to reduce IOP and/or IOP-lowering medications.1–6 With the growing interest in MIGS procedures and expanding options in devices, especially when combined with phacoemulsification cataract surgery, clinical evidence showing safety and efficacy would better aid clinicians with their decision-making.
The STREAMLINE Surgical System (New World Medical, Rancho Cucamonga, CA) was developed to provide a novel and minimally invasive method of performing canaloplasty. This device has been available in the United States (US) since 2021 and can be used as a standalone procedure or combined with cataract surgery. The STREAMLINE Surgical System consists of a single-use, disposable handpiece featuring a stainless-steel outer cannula within a polymer sleeve and an internal stainless steel catheter.7 Upon depressing the actuator button on the handpiece, the sleeve is retracted, and the internal catheter tip pierces the TM and enters the canal of Schlemm (CS). Simultaneously, an ophthalmic viscoelastic device (OVD) is delivered through the catheter to viscodilate the canal, stretch the TM, and flush the distal collector channels. The OVD reservoir of the handpiece holds sufficient volume to perform up to 8 applications, each injecting ~7 µL of OVD.
The Hispanic population is the largest and fastest-growing ethnic minority in the US. The prevalence of OAG in the Hispanic community is high and is expected to increase over the next few decades.8–10 Despite this high prevalence, the clinical data on various MIGS devices and procedures among Hispanic adults remain relatively sparse. Of note, a previously published single-surgeon study evaluated the safety and efficacy of STREAMLINE canaloplasty among Hispanic adults at 6 and 12 months and described favorable surgical outcomes.5,6 The current study is a prospective, multi-center (Mexico, Dominican Republic and Costa Rica), multi-surgeon, 12-month trial conducted to further evaluate and validate the clinical outcomes of the STREAMLINE canaloplasty combined with cataract surgery in eyes with mild to moderate OAG in a Hispanic adult population. The presented data are unique to this study and not part of previously published STREAMLINE canaloplasty studies.
Materials and Methods
This was a prospective, open-label, non-randomized, multi-center, multi-surgeon, interventional clinical trial involving Hispanic adults to evaluate the safety and IOP-lowering efficacy of STREAMLINE canaloplasty in eyes diagnosed with mild to moderate OAG undergoing cataract surgery in Mexico, Costa Rica, and the Dominican Republic. The participating surgeons (GLG, CO, and JFB) were trained in the use of the STREAMLINE device and had prior experience performing anterior chamber angle-based glaucoma surgery. The protocol and consent form were reviewed and approved by all applicable ethics committees in Mexico (APEC Hospital de la Seguerra Vicente Garcia Torres), Dominican Republic (Hospital General de la Plaza de la Salud Comite De Etica de la Investigacion), and Costa Rica (Instituto Costarricense de Investigaciones Clinical Comite Etico Cientifico). Study participants were enrolled between February 2021 and March 2022 and written informed consent was obtained prior to participation in study-related examinations. The trial is registered on www.ClinicalTrials.gov (NCT05089474) and conducted in accordance with the tenets of the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Potential subjects enrolled in the study were at least 22 years of age, had at least one eye with a visually significant cataract, diagnosed with mild to moderate OAG, and were on 1 to 3 topical IOP-lowering medications at Screening. Subjects met the eligibility criteria for the study if their preoperative IOP after medication washout was between 21–36 mmHg inclusive. The following were excluded per the study protocol: women of childbearing potential, eyes with narrow or closed angles, advanced glaucoma (one or more of the following: visual field (VF) mean deviation worse than −12 dB; sensitivity <10 dB in 2 or more of the 4 central test points; cup-disc (C/D) ratio > 0.8; inability to safely undergo washout of IOP-lowering medications), history of intraocular surgery within 6 months or laser surgery within the past 3 months of Screening, history of incisional eye surgery or any prior history of laser iridotomy, best-corrected visual acuity (BCVA) worse than 20/80 in either eye, ocular inflammation or infection in the last 6 months, or any medication that would be contraindicated for a glaucoma surgical procedure.
Procedures
Potential subjects underwent a comprehensive Screening examination, which included BCVA, slit lamp exam, dilated fundus exam, automated perimetry, pachymetry, and endothelial cell count. Eligible subjects underwent appropriate washout of IOP-lowering medications, followed by an eligibility (Baseline) visit at which the unmedicated IOP was measured. If both eyes met the eligibility criteria, the eye with the higher unmedicated IOP was designated as the study eye (except in cases where the IOP in both eyes were equal, the right eye became the study eye). Following a successful phacoemulsification cataract surgery and intraocular lens implantation, STREAMLINE canaloplasty was performed according to the manufacturer’s instructions for use as follows:7 Preoperatively, OVD was loaded into the handpiece. The patient’s head was positioned 45° away from the surgeon and the microscope was angled 45° toward the surgeon. The cannula was introduced through the cataract surgery incision under direct gonioscopic visualization and advanced across the anterior chamber to the nasal angle. The outer sleeve was positioned against the TM to indent the tissue. The actuator button was then fully depressed, retracting the outer sleeve and allowing the inner catheter to enter into the CS. Continuous pressure on the actuator button for 2 seconds delivered OVD into the canal. The tip was then withdrawn from the TM and the actuator button was released. The procedure was repeated, spacing each application approximately 1 clock hour away from prior applications, for a total of 5 to 8 applications across 4 to 6 clock hours of the drainage angle.
Postoperative Management
Following surgery, steroids and antibiotics were administered according to the surgeon’s standard of care for phacoemulsification cataract surgery. Postoperative assessments conducted 1 day, 1 week, and 1, 3, 6, 9, and 12 months after surgery included medication use, BCVA, IOP, and anterior segment examination. Gonioscopy and dilated posterior segment examination were repeated at Months 3 and 12. IOP was measured by Goldmann tonometry, in which each value represents the mean of two measurements taken at each assessment (a third was included if the first two differed by more than 3 mmHg). In cases where the 3 IOP measurements were taken, the 2 measurements that were the closest in values were averaged.
Outcome Measures
The primary outcome measure of this study was the proportion of unmedicated eyes with an IOP reduction ≥20% from the post-washout (Baseline) visit at Month 12. The secondary outcomes included the mean unmedicated IOP change from eligibility (Baseline) visit to Month 12 and the mean change in the number of IOP-lowering medications from pre-washout (Screening) to Month 12. Safety outcomes included the nature and frequency of intra- and postoperative AEs.
Statistical Analysis
All analyses were considered exploratory, and no specific hypotheses were tested; therefore, no a priori power analysis was performed. The sample size of up to 60 subjects was selected to provide a sufficiently large dataset to estimate the primary outcome. The normality of the scale data was assessed using the Shapiro Wilk test. For the comparison of Baseline IOP and Screening medication count, paired t-test was used for parametric data, and a Wilcoxon signed-rank test was used for non-parametric data.
Post Hoc Analyses
A post hoc power calculation was performed to evaluate whether a sample size of 40 provides adequate power for the study. The results showed that a sample size of 40 provided statistical power of 99.9% for the comparison of IOP and the number of IOP-lowering medications at 12 months compared to pre- and postoperative values.
Additional post hoc analyses were performed to further confirm the validity of our key endpoints. One such analysis included the proportion of eyes that were on the same or fewer medications at Month 12 compared to their pre-washout medications, using the data-as-observed approach to mimic real-world outcomes.
Results
Study Population and Baseline Characteristics
Of the initial 45 eyes enrolled in the study, 2 were later found to have been on no medications at Screening and were thus disqualified from the analysis. The demographic data and glaucoma status of the 43 subjects who qualified for this analysis are listed in Table 1. The mean age was 68.7 (range, 37–89 years); most (76.7%) were female, and all were Hispanic. Glaucoma severity was graded as mild in 72.1% and moderate in 27.9% of eyes. The proportions of eyes using one (34.9%), two (34.9%), and three (30.2%) medications at Screening were almost evenly distributed. Of the 43 eyes at Baseline, 1 patient died of a myocardial infarction unrelated to the study interventions after the Month 9 visit; 2 other eyes were lost to follow-up, with 1 following through the Month 6 visit and 1 following through the Month 9 visit. In addition, 2 eyes had a visual acuity (VA) worse than 20/80 in the study eye, 1 eye was included without a Screening VF, and 2 eyes were included that had a C/D ratio of greater than 0.8. However, the investigators determined that all of these eyes had mild or moderate OAG, and they have been included in all analyses.
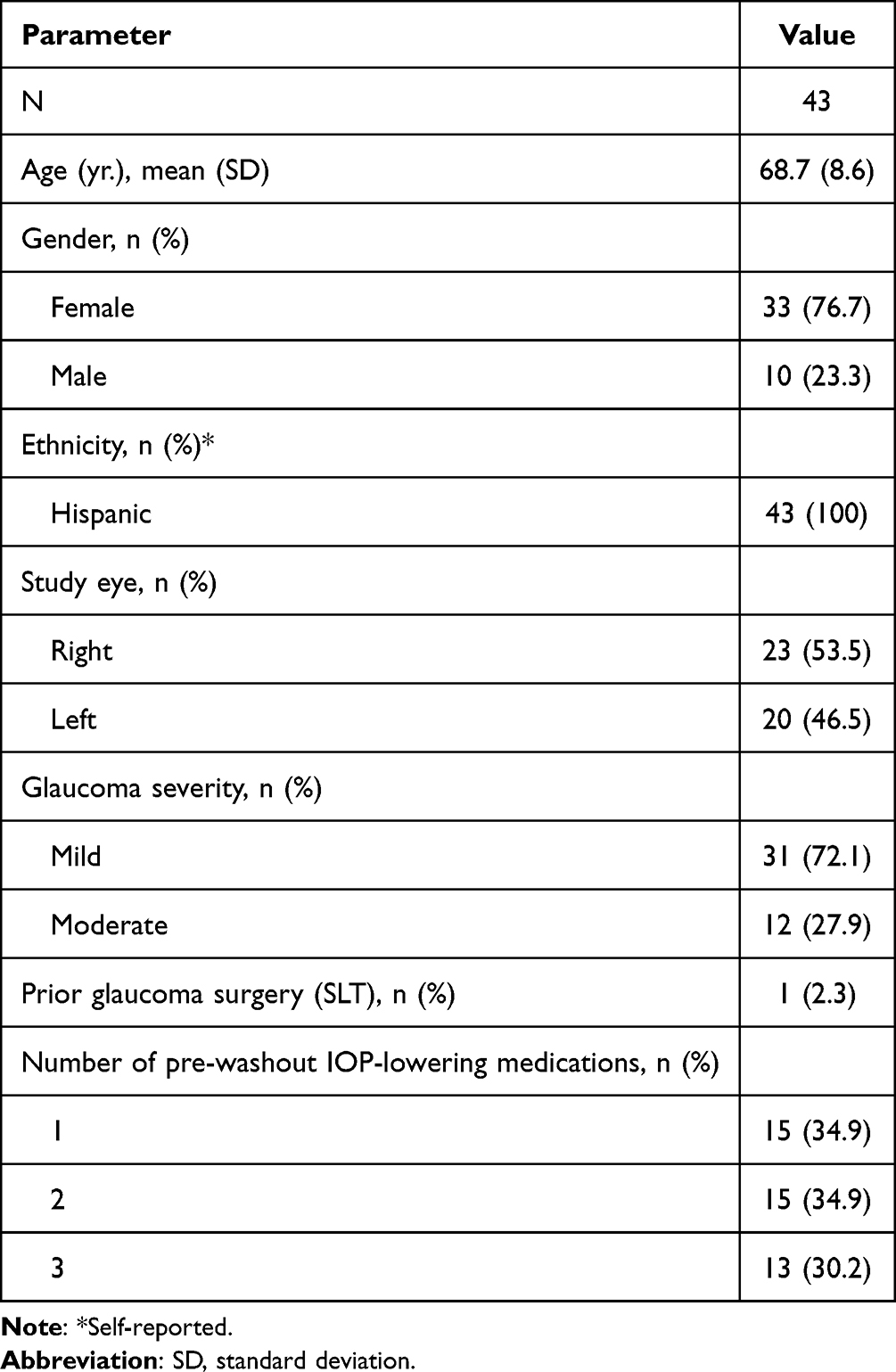 |
Table 1 Demographic Data and Glaucoma Status of the Analysis Population |
Postoperative Outcomes
IOP and Medication Use
Overall, 40 eyes completed the Month 12 follow-up. The mean IOP data at each postoperative visit are shown in Figure 1. Mean (standard deviation) medicated IOP at Screening was 18.3 (3.5) mmHg and unmedicated Baseline IOP (post-washout) was 23.0 (1.8) mmHg. Mean IOP decreased as early as the first postoperative day, with a statistically significant (p<0.001) reduction from Baseline at each visit, ranging from 14.1–15.5 mmHg through Month 12. This represents a 32.3–38.1% reduction from Baseline (Table 2). Of the 40 eyes that completed the Month 12 follow-up visit, 90.0% (36/40) of the eyes achieved a mean IOP reduction of ≥20% from Baseline. At Month 12, 70.0% (28/40) of the eyes were medication-free. The proportion of unmedicated eyes with ≥20% reduction in IOP at Month 12 compared to Baseline was 96.4% (27/28). This represents 67.5% (27/40) of all eyes that completed the Month 12 visit. Furthermore, 92.5% (37/40) of eyes achieved IOP ≤18 mmHg and 45.0% (18/40) achieved IOP ≤15 mmHg at Month 12 (Table 3).
 |
Table 2 Intraocular Pressure (IOP) and Medication Use |
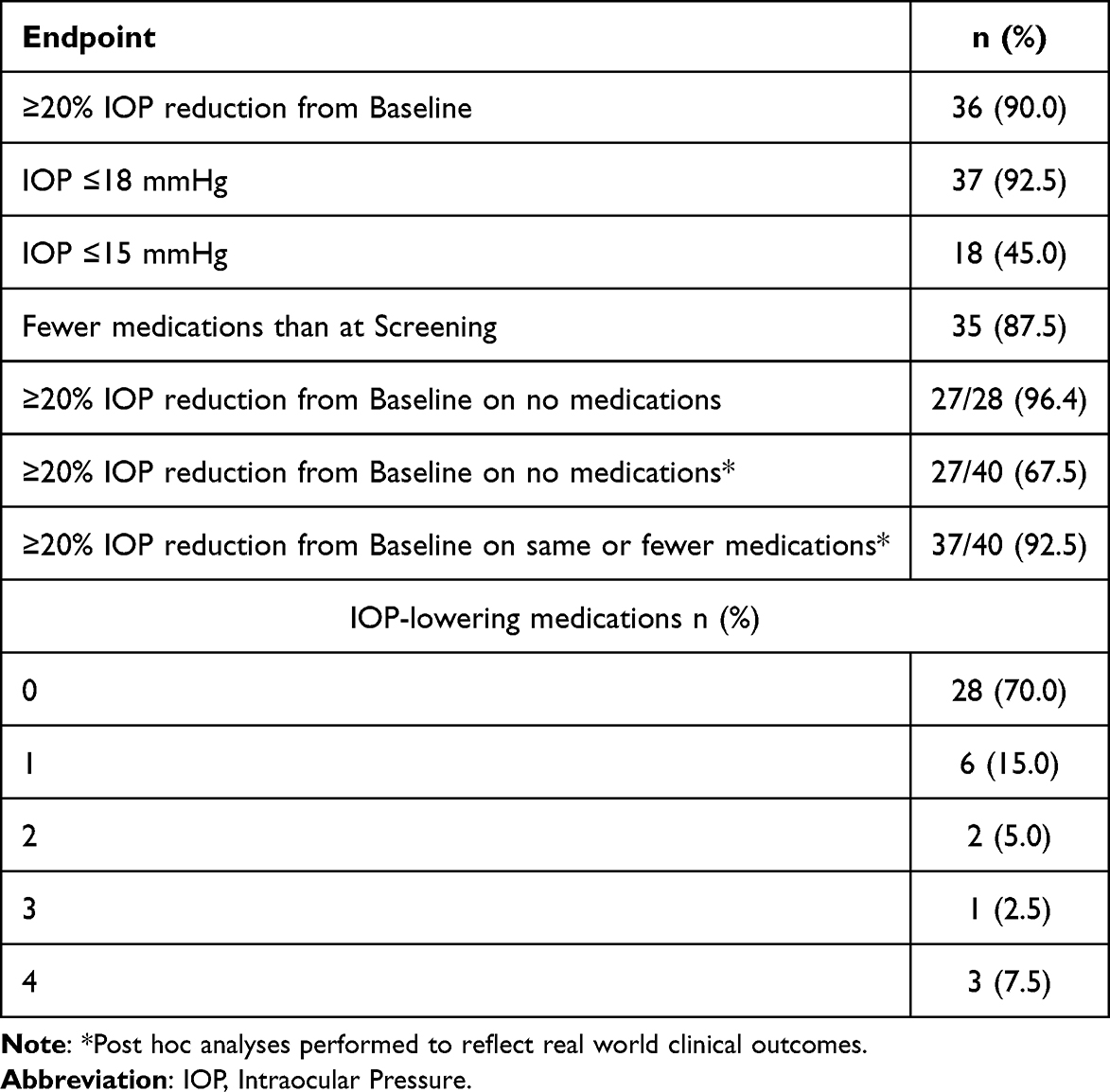 |
Table 3 Key Outcomes at Month 12 (N=40) |
 |
Figure 1 Change in Mean IOP Over Time from Baseline. There were statistically significant (P< 0.001) reduction in the mean IOP at each postoperative visit. Mean Error bars represent standard deviation. |
The mean IOP-lowering medication count at each visit are shown in Figure 2. Subjects used a mean of 1.95 (0.82) medications at Screening, and this was significantly reduced (p<0.001) at every postoperative visit. From Month 6 and beyond, the mean number of medications ranged from 0.51–0.63, representing a mean reduction of 76.3–79.8% from Screening (Table 2). At Month 12, 92.5% (37/40) of the eyes were on the same or fewer medications than at Screening (Table 3).
 |
Figure 2 Change in Mean IOP-lowering Medication Count Over Time from Screening. There were statistically significant (P< 0.001) reduction in the mean IOP-lowering medication count at each postoperative visit. Mean Error bars represent standard deviation. |
Postoperative Adverse Events
All ocular adverse events (AEs) were graded as mild or moderate in severity (Table 4), The device- or procedure-related AEs included transient IOP elevation in 3 eyes (7.0%), likely related to short-term postoperative steroid use or retained OVD during intraocular surgery, corneal striae in 3 eyes (7.0%), hyphema in 2 eyes (4.7%), pain and inflammation in 1 eye (2.3%) and corectopia in 1 eye (2.3%). Other AEs unrelated to the device or procedure were dry eye in 2 eyes (4.7%), dermatitis in 1 eye (2.3%), allergic reaction in 1 eye (2.3%), small leukoma in 1 eye (2.3%), and corneal ulceration due to ingrowth of an eyelash in 1 eye (2.3%). One device unrelated serious adverse event (SAE), death due to myocardial infarction, occurred during the study.
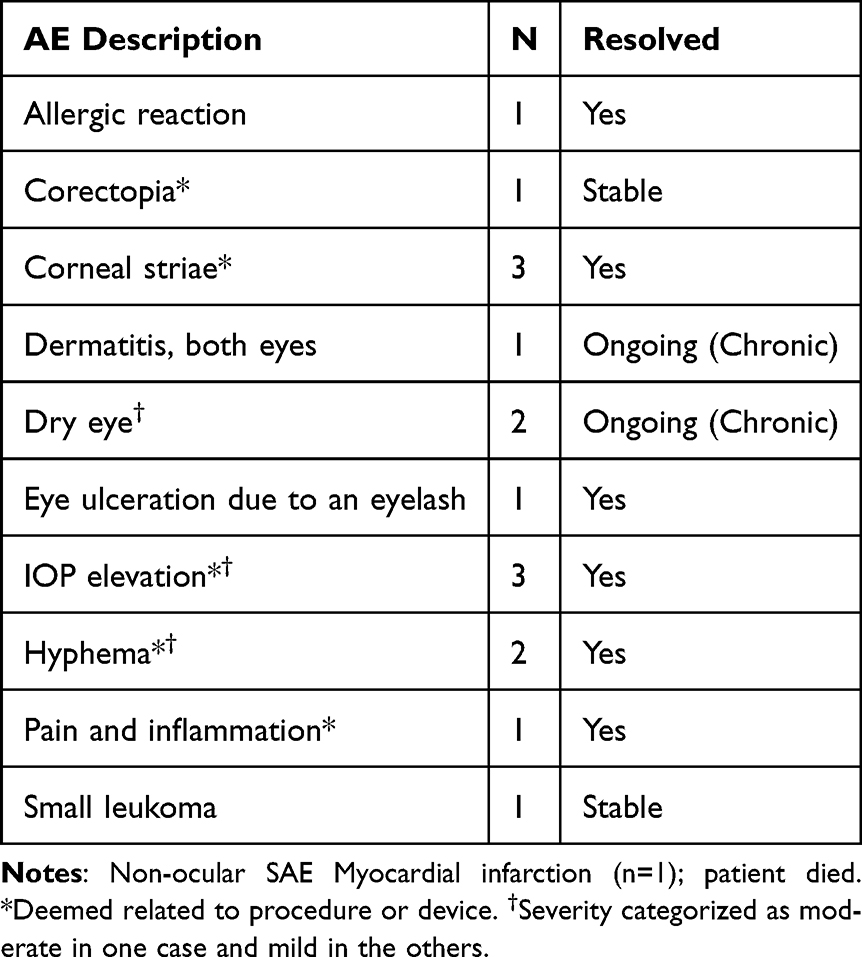 |
Table 4 Ocular Adverse Events (N=43) |
Discussion
This prospective, multi-center study contributes to the body of evidence on the STREAMLINE Surgical System. The results of this study demonstrate that STREAMLINE canaloplasty in combination with phacoemulsification cataract surgery provides substantial reduction in both IOP and the need for IOP-lowering medications through at least the first postoperative year in eyes of Hispanic adults with mild to moderate OAG.
The primary outcome in this study was the proportion of unmedicated eyes with a ≥20% reduction in IOP at Month 12 from eligibility (Baseline) and 96.4% (27/28) of eyes achieved this endpoint. The majority of eyes (70.0%, 28/40) were medication-free at Month 12, 90.0% (36/40) manifested IOP reductions of ≥20% from Baseline. The mean medication use also decreased (76.3%) from the Screening visit to Month 12. These results indicated a meaningful reduction in both IOP and medication use. Given the pre-washout mean IOP of 18.3 (3.5) mmHg, many eyes likely underwent combined surgery, at least in part, to reduce reliance on topical IOP-lowering medications. The majority of eyes (92.5%, 37/40) either maintained or successfully reduced their dependence on medications without compromising IOP with an average of 7.8 (3.0) mmHg decrease in pressure at Month 12 compared to Baseline.
This study is similar to the one reported by Lazcano et al,6 which was a single-site, prospective 12-month analysis of 37 eyes of 37 Hispanic adults with mild or moderate OAG that underwent combined phacoemulsification with STREAMLINE canaloplasty. At one year, the mean IOP decreased by 30% and medication use decreased by 61%; 80% of eyes achieved a ≥20% reduction in IOP from the unmedicated Baseline, and 51.4% were medication-free. The outcomes of our current study also show similar results when compared to the 12- or 24-month outcomes for other phaco-MIGS devices: the first- and second-generation iStent (Glaukos),11–13 the Hydrus microstent (Alcon),14–16 VISCO360 or OMNI (Sight Sciences),17,18 and the iTrack (Nova Eye Medical).19,20
The American Academy of Ophthalmology (AAO) defines canaloplasty as “cannulation of Schlemm’s canal with a catheter or stent with either an internal or external approach for at least three clock hours with an injection of viscoelastic while removing the stent to dilate the canal. Alternatively, viscoelastic injections made via three or more punctures of the trabecular meshwork spanning at least three clock hours (90 degrees) to dilate Schlemm’s canal should also qualify as canaloplasty”.21 STREAMLINE is designed to inject a significant volume (~7 µL) of OVD with each application using a total of 5–8 applications approximately 1 clock hour away from each other (total injected OVD volume of 35 to 56 µL). This volume of OVD is similar to or greater than that used by other commercial canaloplasty devices.22,23 The end result of STREAMLINE canaloplasty is the reduction of IOP and the need for IOP-lowering medications by targeting the primary site of aqueous humor outflow obstruction at the level of the TM, CS, and distal collector channels.
An additional advantage of canaloplasty with the STREAMLINE procedure is that it does not require the permanent implantation of a device such as a TM bypass stent. This is relevant because implanted glaucoma devices—whether glaucoma drainage devices, certain MIGS devices, or sustained-release drug delivery platforms—have been associated with corneal endothelial cell loss (ECL).24–26 A previous study demonstrated that the ECL following STREAMLINE combined with phacoemulsification (16.8% at 12 months6) is consistent with reports of ECL following phacoemulsification alone in eyes with glaucoma (~10-17% in various studies24).
This study exclusively enrolled Hispanic patients from centers in 3 different countries in Latin America. Hispanic ethnicity is a known risk factor for the development of OAG.8–10,27,28 Relatively little is known regarding the efficacy of glaucoma therapies in Hispanic patients. The Registry in Glaucoma Outcomes Research (RiGOR) study found no differences in response to medical, laser, or surgical therapy by ethnicity,29 and a study of Hispanic patients undergoing phacoemulsification, trabeculectomy, or phacotrabeculectomy demonstrated IOP and medication reductions comparable to those in white patients.30 Conversely, other studies have found Hispanic ethnicity to be a risk factor for surgical failure of trabeculectomy and tube-shunt surgery.31–33 With regard to phaco-MIGS procedures, effective clinical outcomes have been reported in Hispanic patients undergoing excisional goniotomy with the Kahook Dual Blade (KDB) (New World Medical),34,35 trabecular ablation with the Trabectome (MicroSurgical Technology),36 trabecular micro bypass with the iStent,37 and canaloplasty with trabeculotomy with the OMNI System.38
Along with the strengths of our study, there were some limitations that must be acknowledged. The study population exclusively comprised Hispanic patients, which may limit generalizability to the entire OAG patient population but provides insight into outcomes in a high-risk and understudied subset of glaucoma patients. There was no planned terminal washout for our study since the primary endpoint was the proportion of unmedicated eyes with IOP reduction ≥ 20% from Baseline (post-washout) at Month 12. Although a formal medication washout was not required at Month 12, 70% (28/40) of the subjects were medication-free and 92.5% (37/40) were on the same or fewer medications. Another limitation is not having a control group and having a primary endpoint that considers only responders (medication-free subjects). The IOP-lowering effect of phacoemulsification alone has been well described. A meta-analysis conducted by Malvankar-Mehta et al39 reported the weighted mean reduction for IOP and glaucoma medications at 12 months compared to baseline on pre-selected iStent-Phaco vs standalone Phacoemulsification studies in OAG patients. Their results showed a 4% IOP reduction with phacoemulsification alone, while iStent in combination with phacoemulsification showed a 9–27% IOP reduction from baseline. Furthermore, their study showed a reduction in mean number of medications by 1.01 with phacoemulsification alone, and 1.1 to 1.33 in iStent combined with phacoemulsification, when compared to baseline. Both are consistent with our post hoc analysis findings of 13.7% (−2.9) mmHg IOP reduction and 1.38 medication count reduction at Month 12 compared to (pre-washout) Screening.
Because the STREAMLINE Surgical System has been available for use only since 2021, published clinical data in peer-reviewed literature are currently limited. Additional and longer-term data are needed to determine the durability of treatment effect in Hispanic population and OAG patients, in general.
Conclusion
This prospective study adds further evidence to support effective outcomes of STREAMLINE canaloplasty in Hispanic adults. In summary, STREAMLINE canaloplasty in combination with phacoemulsification provides clinically meaningful reduction in both IOP and the number of IOP-lowering medications in eyes with mild to moderate OAG. This procedure should be considered a valuable addition to MIGS options for OAG patients undergoing cataract surgery.
Data Sharing Statement
Study data are available from the corresponding author upon reasonable request.
Acknowledgments
Anthony Realini, MD for preparing the initial draft of manuscript; Raman Bedi, MD for statistical (data) analysis; Theresa Landry, PhD for protocol development.
Disclosure
GLG, CO, and JFB were investigators for the clinical study. MYK is a consultant to New World Medical and his university receives fees on his behalf for this consultancy. In addition, MYK has a patent (No. 10,729,584) related to the STREAMLINE Surgical System technology and a patent US 2021/0322218 A1 owned by New World Medical. Funding for this study was provided by New World Medical. EMI, HR, and MH are employees of New World Medical. Inc. EMI reports Consultant Fee from Heru, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Yuan PH, Dorling M, Shah M, Panarelli JF, Durr GM. Combined Micro-Invasive Glaucoma Surgery (MIGS) with phacoemulsification in open angle glaucoma: a systematic review and meta-analysis. Am J Ophthalmol. 2024; 2024:S0002.
2. Lavia C, Dallorto L, Maule M, Ceccarelli M, Fea AM. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12(8):e0183142. doi:10.1371/journal.pone.0183142
3. Pillunat LE, Erb C, Junemann AG, Kimmich F. Micro-invasive glaucoma surgery (MIGS): a review of surgical procedures using stents. Clin Ophthalmol. 2017;11:1583–1600. doi:10.2147/OPTH.S135316
4. Richter GM, Coleman AL. Minimally invasive glaucoma surgery: current status and future prospects. Clin Ophthalmol. 2016;10:189–206. doi:10.2147/OPTH.S80490
5. Lazcano-Gomez G, Garg SJ, Yeu E, Kahook MY. Interim analysis of STREAMLINE® surgical system clinical outcomes in eyes with glaucoma. Clin Ophthalmol. 2022;16:1313–1320. doi:10.2147/OPTH.S358871
6. Lazcano-Gomez G, Antzoulatos GL, Kahook MY. Combined phacoemulsification and STREAMLINE surgical system canal of schlemm transluminal dilation in eyes of Hispanic patients with mild to moderate glaucoma. Clin Ophthalmol. 2023;17:1911–1918. doi:10.2147/OPTH.S409164
7. New World Medical. STREAMLINE SURGICAL SYSTEM Instructions for Use. Rancho Cucamonga, CA: New World Medical; 2021.
8. Quigley HA, West SK, Rodriguez J, et al. The prevalence of glaucoma in a population-based study of Hispanic subjects: proyecto VER. Arch Ophthalmol. 2001;119(12):1819e1826. doi:10.1001/archopht.119.12.1819
9. Varma R, Ying-Lai M, Francis BA, et al. Prevalence of open-angle glaucoma and ocular hypertension in Latinos: the Los Angeles Latino Eye Study. Ophthalmology. 2004;111(8):1439–1448. doi:10.1016/j.ophtha.2004.01.025
10. Vajaranant TS, Wu S, Torres M, Varma R. The changing face of primary open-angle glaucoma in the United States: demographic and geographic changes from 2011 to 2050. Am J Ophthalmol. 2012;154(2):303–314.e3. PMID: 22541661; PMCID: PMC3401269. doi:10.1016/j.ajo.2012.02.024
11. Samuelson TW, Katz LJ, Wells JM, Duh YJ, Giamporcaro JE. Randomized evaluation of the trabecular micro-bypass stent with phacoemulsification in patients with glaucoma and cataract. Ophthalmology. 2011;118:459–467. doi:10.1016/j.ophtha.2010.07.007
12. Samuelson TW, Sarkisian SR, Lubeck DM, et al. Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results. Ophthalmology. 2019;126:811–821. doi:10.1016/j.ophtha.2019.03.006
13. Seibold LK, Gamett KM, Kennedy JB, et al. Outcomes after combined phacoemulsification and trabecular microbypass stent implantation in controlled open-angle glaucoma. J Cataract Refract Surg. 2016;42(9):1332–1338. PMID: 27697252. doi:10.1016/j.jcrs.2016.07.023
14. Samuelson TW, Chang DF, Marquis R, et al. A schlemm canal microstent for intraocular pressure reduction in primary open-angle glaucoma and cataract: the HORIZON Study. Ophthalmology. 2019;126:29–37. doi:10.1016/j.ophtha.2018.05.012
15. Jones J, Koch DD, Vold S, et al; HORIZON U.S. investigators. Results from the United States cohort of the HORIZON trial of a Schlemm canal microstent to reduce intraocular pressure in primary open-angle glaucoma. J Cataract Refract Surg. 2019;45(9):1305–1315. PMID: 31326225. doi:10.1016/j.jcrs.2019.03.024
16. Pfeiffer N, Garcia-Feijoo J, Martinez-de-la-Casa JM, et al. A randomized trial of a schlemm’s canal microstent with phacoemulsification for reducing intraocular pressure in open-angle glaucoma. Ophthalmology. 2015;122(7):1283–1293. PMID: 25972254. doi:10.1016/j.ophtha.2015.03.031
17. Gallardo MJ, Pyfer MF, Vold SD, et al; GEMINI study group. Canaloplasty and trabeculotomy combined with phacoemulsification for glaucoma: 12-month results of the GEMINI Study. Clin Ophthalmol. 2022;16:1225–1234. PMID: 35493971; PMCID: PMC9039153. doi:10.2147/OPTH.S362932
18. Vold SD, Williamson BK, Hirsch L, et al. Canaloplasty and trabeculotomy with the OMNI system in pseudophakic patients with open-angle glaucoma: the ROMEO Study. Ophthalmol Glaucoma. 2021;4(2):173–181. PMID: 33045423. doi:10.1016/j.ogla.2020.10.001
19. Gallardo MJ, Supnet RA, Ahmed IIK. Viscodilation of schlemm’s canal for the reduction of IOP via an ab-interno approach. Clin Ophthalmol. 2018;12:2149–2155. doi:10.2147/OPTH.S177597
20. Gallardo MJ. 24-month efficacy of viscodilation of schlemm’s canal and the distal outflow system with iTrack Ab-interno canaloplasty for the treatment of primary open-angle glaucoma. Clin Ophthalmol. 2021;15:1591–1599. doi:10.2147/OPTH.S272506
21. American Academy of Ophthalmology. Canaloplasty. 2022. Available from: https://www.aao.org/practice-management/news-detail/canaloplasty.
22. Sight Sciences. OMNI® Surgical System. Instructions for Use. Available from: https://omnisurgical.com/wp-content/uploads/2023/08/PN-05854-Rev-K-IFU-OMNI-System-2.0-US.pdf.
23. US Food & Drug Administration. iTrackTM Advance Canaloplasty Microcatheter with Advanced Delivery System. US FDA Approval Letter and Indications for Use. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf22/K221872.pdf.
24. Realini T, Gupta PK, Radcliffe NM, et al. The effects of glaucoma and glaucoma therapies on corneal endothelial cell density. J Glaucoma. 2021;30(3):209–218. doi:10.1097/IJG.0000000000001722
25. Medeiros FA, Walters TR, Kolko M, et al. Phase 3, randomized, 20-month study of bimatoprost implant in open-angle glaucoma and ocular hypertension (ARTEMIS 1). Ophthalmology. 2020;127(12):1627–1641. doi:10.1016/j.ophtha.2020.06.018
26. Obuchowska I, Konopińska J. Corneal endothelial cell loss in patients after minimally invasive glaucoma surgery: current perspectives. Clin Ophthalmol. 2022;16:1589–1600. PMID: 35642179; PMCID: PMC9148582. doi:10.2147/OPTH.S359305
27. Wurster P, Harris A, Gonzalez AC, et al. Risk factors for open-angle glaucoma in persons of Latin American descent. J Glaucoma. 2020;29(3):217–225. doi:10.1097/IJG.0000000000001429
28. American Academy of Ophthalmology. Primary Open-Angle Glaucoma: Preferred Practice Pattern. San Francisco: American Academy of Ophthalmology; 2020.
29. Coleman AL, Lum FC, Velentgas P, Su Z, Gliklich RE. Impact of treatment strategies for open angle glaucoma on intraocular pressure: the RiGOR study. J Comp Eff Res. 2016;5(1):87–98. doi:10.2217/cer.15.58
30. Jung JL, Isida-Llerandi CG, Lazcano-Gomez G, SooHoo JR, Kahook MY. Intraocular pressure control after trabeculectomy, phacotrabeculectomy and phacoemulsification in a hispanic population. J Curr Glaucoma Pract. 2014;8:67–74. doi:10.5005/jp-journals-10008-1164
31. Van Buskirk EM. Five-year follow-up of the fluorouracil filtering surgery study. Am J Ophthalmol. 1996;122(5):751–752. doi:10.1016/S0002-9394(14)70507-0
32. Garris WJ, Le C, Zurakowski D, Ayyala RS. Comparison of surgical outcomes between canaloplasty and trabeculectomy with mitomycin C at 2-year follow-up: a longitudinal cohort study. Indian J Ophthalmol. 2018;66:66–70. doi:10.4103/ijo.IJO_543_17
33. Ou Y, Yu F, Law SK, Coleman AL, Caprioli J. Outcomes of Ahmed glaucoma valve implantation in children with primary congenital glaucoma. Arch Ophthalmol. 2009;127:1436–1441.
34. Porter M, Garza A, Gallardo M. Excisional goniotomy in latino patients with open-angle glaucoma: outcomes through 24 months. Clin Ophthalmol. 2020;14:3619–3625. doi:10.2147/OPTH.S271923
35. Espinoza G, Justiniano MJ, Rodriguez-Una I, Godin F, Arango A, Villamizar S. Twelve-month outcomes of Kahook dual blade goniotomy combined with cataract surgery in Latino patients. Int Ophthalmol. 2024;44(1):44. PMID: 38337081. doi:10.1007/s10792-024-03024-w
36. Okeke CO, Miller-Ellis E, Rojas M; Trabectome Study G. Trabectome success factors. Medicine. 2017;96:e7061. doi:10.1097/MD.0000000000007061
37. Gallardo MJ, Supnet RA. Three-year outcomes of combined trabecular micro-bypass and phacoemulsification in a predominantly Hispanic population with primary open-angle glaucoma. Clin Ophthalmol. 2019;13:869–879. PMID: 31239633; PMCID: PMC6554518. doi:10.2147/OPTH.S189071
38. Gallardo MJ, Dhamdhere K, Dickerson JE. Canaloplasty and trabeculotomy ab interno combined with cataract surgery: 12-month outcomes in hispanic patients with open-angle glaucoma. Clin Ophthalmol. 2022;16:905–908. PMID: 35356700; PMCID: PMC8959719. doi:10.2147/OPTH.S358878
39. Malvankar-Mehta MS, Iordanous Y, Chen YN, et al. iStent with phacoemulsification versus phacoemulsification alone for patients with glaucoma and cataract: a meta-analysis. PLoS One. 2015;10(7):e0131770. PMID: 26147908; PMCID: PMC4492499. doi:10.1371/journal.pone.0131770
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.