")
Back to Journals » Journal of Inflammation Research » Volume 17
Safety Evaluation of a Potential Anti-Rheumatoid Arthritis Candidate, Levamisole
Authors Wang JX , Zhang JH, Guo M , Huang WR, Zheng HL, Liao YQ, Yan YX, Lin ZL, Qiu NF, Dai CT, Yu XB, Yu Y
Received 24 July 2024
Accepted for publication 24 October 2024
Published 29 October 2024 Volume 2024:17 Pages 7837—7849
DOI https://doi.org/10.2147/JIR.S477013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Jun-Xiang Wang,1,* Jia-Hui Zhang,1,* Mu Guo,1,* Wei-Rui Huang,1 Han-Lu Zheng,1 Yi-Qi Liao,1 Ying-Xue Yan,1 Zhao-Long Lin,1 Neng-Fu Qiu,1 Cui-Ting Dai,2 Xiang-Bin Yu,1 Yue Yu1
1School of Pharmacy & Fujian Center for New Drug Safety Evaluation, Fujian Medical University, Fuzhou, 350122, People’s Republic of China; 2Department of Pathology, The People’s Hospital Affiliated to Fujian University of Traditional Chinese Medicine, Fuzhou, 350004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yue Yu; Xiang-Bin Yu, Email [email protected]; [email protected]
Introduction: Given the limitations and adverse effects of current rheumatoid arthritis (RA) treatments, there is an urgent need for safer and more effective therapeutic options. Levamisole (LVM) is a non-specific immunomodulator with potential for treating skin diseases, tumors, and autoimmune disorders. Recognizing LVM’s potential despite its controversial reputation, this study aimed to investigate its safety profile and therapeutic efficacy towards RA.
Methods: To evaluate the potential toxicity of LVM, a 28-day oral administration was conducted in SD rats, assessing general toxicity and neurotoxicity using serum biochemical indicators, the Morris water maze test, transmission electron microscopy, and H&E staining. Subsequently, the therapeutic effects of LVM on RA were evaluated.
Results: The results showed that 30 mg/kg LVM has promising therapeutic effects in the treatment of RA with negligible toxicity from 45 mg/kg to 180 mg/kg.
Discussions: This study provides valuable preclinical data on the safety and efficacy of LVM, laying the groundwork for future clinical applications and potentially offering a safer and more effective treatment option for RA patients.
Keywords: levamisole, general toxicity, neurotoxicity, rheumatoid arthritis
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by persistent synovial inflammation, ultimately leading to erosive damage to cartilage and bone, resulting in joint stiffness and deformity.1 It is estimated that approximately 0.46% of the global population suffers from RA.2 Current treatment options for RA include non-steroidal anti-inflammatory drugs (NSAIDs), glucocorticoids, and methotrexate.3 However, NSAIDs can lead to serious adverse effects, such as gastrointestinal bleeding, renal failure, and heart failure.4 Glucocorticoids are suitable only for short-term use, as prolonged administration can induce muscle weakness, diabetes, and osteoporosis.5 While methotrexate is a first-line clinical treatment for RA, its use is also associated with severe adverse reactions.6 Therefore, it is crucial to develop an effective and safe pharmaceutical agent for the treatment of RA.
Levamisole (LVM), a synthetic thiazole derivative, was initially employed as an efficacious broad-spectrum antihelminthic agent.7,8 Further research has revealed that LVM possesses notable anti-inflammatory and immunomodulatory properties.9,10 It can induce a type I immune response and stimulate cellular immune responses. Based on its immunomodulatory properties, LVM has been employed in the treatment of a range of conditions, including autoimmune disorders, nephrotic syndrome, infectious diseases, and cancer.11,12 Additionally, clinical case reports have documented the effective treatment of arthritis with LVM.13 In a four-month double-blind trial, 40 patients with rheumatoid arthritis received LVM treatment. Of these patients, 50% demonstrated favorable or excellent clinical outcomes.14 To further elucidate the therapeutic potential of LVM in the management of RA, a comprehensive assessment of its effects in a relevant animal model is warranted. At the same time, it also provides a reference dose for exploring the mechanism of LVM therapy for RA in the future.
In the clinical setting, the incidence of adverse events associated with LVM at therapeutic doses is relatively low, with occasional mild side effects such as dizziness, nausea, vomiting, abdominal pain, anorexia, fever, somnolence, and fatigue. Some studies have reported that LVM can cause demyelinating brain lesions, but these usually resolve after discontinuation of the drug.15 Despite these clinical observations, the limited comprehensive safety data hinders an accurate assessment of the clinical safety of LVM. To ensure that LVM are safe for clinical use, it is necessary to reassess the safety of oral LVMs in relevant animal models. In this study, we first investigated the general toxicity of LVM and then evaluated its neurotoxicity. Finally, we chose a safe dose to evaluate the therapeutic potential of oral LVM for RA treatment.
Materials and Methods
Drugs and Chemicals
LVM (purity ≥ 98%, LV161106) was procured from the Nanjing Baijingyu Pharmaceutical Company (Nanjing, Jiangsu, China). MTX (purity ≥ 99%, CAS: 59-05-2) was provided by Macklin (Shanghai, China). M. Tuberculosis Des. H37 Ra (SKU: 231141) was provided by Becton, Dickinson and Company (New Jersey, USA). LVM, dissolved in saline, was administered to animals by intragastric administration. Complete Freund’s Adjuvant (CFA) was prepared by sonicating and vortexing mineral oil and M. Tuberculosis, which formed the suspension solution with a concentration of 15 mg/mL.
Animals
The study utilized SD rats (SPF adult male, weighing 150 ± 20 g) obtained from the Shanghai Slac Laboratory Animal Company (License no. SCXK 2022–0004, Shanghai, China). This study has obtained approval from the Animal Ethics Committee of Fujian Medical University (APVL No: FJMU IACUC 2023–0156). We follow the welfare guidelines outlined in GB/T 42011–2022, General Principles of Animal Welfare, in our animal experiments. The animals were kept in the indexed vertex cages, with standard rat pellets and water under controlled temperature (26 ± 2°C), humidity (65–75%), and a 12-h light/12-h dark cycle. The rats were anesthetized using pentobarbital sodium and euthanized via carbon dioxide. Every effort was made to minimize animal suffering and reduce the number of animals used. The toxicological experiments were conducted in accordance with the Organization for Economic Cooperation and Development (OECD) guidelines for the testing of chemicals and the United States Environmental Protection Agency (USEPA) Testing Guidelines for Toxicology.
General Toxicological Study Regimen
According to the standard operating procedures of Fujian Medical University, 40 SD rats were randomly divided into four groups. The groups were designated as follows: Control group (n = 10), LVM low-dose group (n = 10, 45 mg/kg), LVM median-dose group (n = 10, 90 mg/kg), and LVM high-dose group (n = 10, 180 mg/kg). In this study, the control group received a daily oral dose of saline, while each dose group was administered a daily oral dose of LVM dissolved in saline for a duration of 28 days.
Body Weight and Macroscopic Changes Observations
A series of observations were conducted on the animals at regular intervals following the administration of the gavage. These observations were conducted on a range of anatomical sites, including the eyes, ears, nose, oral cavity, fur, abdomen, vulva, perianal area, limbs, claws, toes, gait, behavior, excretion, feeding, and drinking. Additionally, each rat underwent a weight assessment before the commencement of the study, on a weekly basis throughout the 28-day period, and on the day of necropsy.
Gross Necropsy and Organ Weights
The rats were euthanasia under profound isoflurane anesthesia one day after the repeated oral dosing was terminated. Following the collection of blood samples, the rats were euthanasia by exsanguination. The external surfaces, orifices, and all organs and their contents in the cranial, thoracic, and abdominal cavities were then inspected. Tissues were collected from all rats and preserved for microscopic examination. Furthermore, the absolute and relative (organ-to-body weight ratio) weights of the liver, kidneys, spleen, brain, lung, and heart were determined.
Hematology and Serum Biochemistry Analysis
Whole blood and serum were collected from rats after 28 days of continuous administration. Prior to blood collection, all rats were fasted for approximately 12 hours. Blood samples were taken from the aorta under sodium pentobarbital anesthesia. A total of 2 mL of blood was collected in a complete blood count bottle (EDTA 2 K; 3 mL, Vacutainer, BD, USA) and analysed using a XT2000i automatic blood cell analyser (SYSMEX, Hyogo, Japan). The indicators for hematological analysis include white blood cells (WBC), red blood cells (RBC), hemoglobin (HGB), hematocrit (HCT), blood platelets (PLT), mean platelet volume (MPV), median corpuscular hemoglobin concentration (MCHC), and red cell distribution width (RDW-SD). Furthermore, prothrombin time and activated partial thromboplastin time were determined in the remaining blood samples treated with sodium citrate (9NC Sodium Citrate; BD Vacutainer) using a coagulometer (ACL ELITE PRO; Instrumentation Laboratory, Bedford, MA, USA). A total of 2 mL of blood was collected during necropsy and placed in a 5-mL blood collection tube (Insepack; Sekisui, Tokyo, Japan) containing a clot activator. The blood was allowed to coagulate at room temperature for 15–20 minutes, after which it was centrifuged for 10 minutes. The following serum biochemistry variables were analyzed using the AU480 Automatic Biochemical Analyzer (Beckman, California, United States) and the Medica EasyLyte PLUS Electrolyte Analyzer (Medica, Massachusetts, United States). The indicators for serum biochemical analysis include albumin (ALB), total bilirubin (TBIL), aspartate aminotransferase (AST), alanine transaminase (ALT), total protein (TP), alkaline phosphatase (ALP),16 triglyceride (TG), creatinine (CREA), blood urea nitrogen (BUN), cholesterol (CHOL), glucose (GLU), and creatine kinase (CK).
Histopathological Analysis
All organs and tissues from the control and all dosage groups underwent histopathological assessment. The liver, kidneys, heart, lungs, and spleen were extracted from each rat and preserved in a 10% neutral-buffered formalin solution. The preserved tissues were then processed, embedded in paraffin, and stained with hematoxylin and eosin for subsequent microscopic examinations.
Neurotoxicity Study Regimen
The rats were randomly divided into four groups: a control group (n = 8), a low-dose group (n = 8, 45 mg/kg), a medium-dose group (n = 8, 90 mg/kg), and a high-dose group (n = 8, 180 mg/kg). A six-day Morris water maze experiment was conducted on the 23rd day after gavage to investigate whether LVM affects the learning and memory function of rats.
Morris Water Maze Test
To assess potential alterations in spatial learning, we conducted Morris water maze (MWM) experiments on animals. The MWM apparatus is a circular, dark-colored water tank filled with black-dyed water (70 cm deep, 25±1°C), divided into four imaginary quadrants, with fixed visual cues on the walls of the room. The animals underwent one day of acclimatization training on day 23 of administration, followed by four days of formal training, and were tested on day 28. During the training, a platform was placed in one of the four virtual quadrants, with its top hidden below the water surface. Each training session consisted of four trials with a 60-second interval. In each trial, the animal was placed in a different quadrant and given 60 seconds to find the hidden platform. The time taken to reach the hidden platform (escape latency) was used to evaluate the animal’s learning progress. On the day of the experiment, the platform was removed, and the animals were tracked for 60 seconds to assess spatial memory by measuring the time spent in each quadrant.
Evans Blue Staining
After 28 days of oral gavage, the rats were subjected to Evans blue (EB) staining. The procedure begins with the injection of EB dye into the rats’ tails, which is done slowly to ensure the dye is absorbed into the rats’ bodies. After two hours, the rats’ brains are collected and ground using a grinder. The resulting powder is then placed in a centrifuge at 4000 r/min for 15 minutes. The supernatant is then extracted and its absorbance value is measured. Finally, the Evans blue content is calculated using a standard curve to represent blood-brain barrier permeability.
Hippocampus and Myelin Sheath Sections
After 28 days of drug administration, the experimental rats were euthanasia and their brain tissues were collected for histological analysis. Hematoxylin and eosin (H&E) staining and myelin staining using the Luxol Fast Blue (LFB) method were performed. To obtain the pathological specimens, pentobarbital sodium was injected into the abdominal cavity, followed by saline perfusion through the heart. The brain was meticulously isolated and fixed in 4% paraformaldehyde, followed by 10% formalin fixation for 24 hours. After embedding the samples in paraffin, 4μm thick sections were cut using a microtome and placed on glass slides for dewaxing. The sections were stained with H&E and LFB to assess inflammation and demyelination. The infiltration of cells and the extent of demyelination were observed under a light microscope.
Transmission Electron Microscopy
The brain tissue obtained by perfusion was fixed in 2% paraformaldehyde solution at 4°C for 2 hours. Then, the tissue was washed with 0.1 mol/L potassium sodium tartrate buffer every 2 hours, for a total of 3 times. The next day, the tissue was soaked in 1% osmic acid solution at 4°C for 2 hours, and then washed with 0.1 mol/L potassium sodium tartrate buffer twice, for 15 minutes each time. After dehydration with gradient ethanol and permeation with epoxy propane for 15 minutes twice, the tissue was permeated with 1:1 permeation solution (incomplete embedding liquid:epoxy propane = 1:1) for 1 hour, followed by permeation with 2:1 permeation solution (incomplete embedding liquid:epoxy propane = 2:1) for 1 hour. The tissue was then immersed in incomplete embedding liquid overnight. After being completely immersed in embedding liquid at 35°C for 6 hours, the tissue was transferred to an embedding plate and incubated at 42°C overnight, followed by drying at 60°C for 48 hours. After the tissue was embedded, it was sectioned and positioned. Random fields were selected in the adjacent area of the corpus callosum of each rat group for photographing and observing the ultrastructure of myelin sheath.
Anti-Rheumatoid Arthritis Study Regimen
The Adjuvant-Induced Arthritis (AIA) rat model was established via a subcutaneous injection of 100 μL of CFA (15 mg/mL) at the base of the tail, while the control group was given 100 μL saline at the same part. A total of 20 rats were randomly divided into four groups, as follows: Control group (n = 5): received no intervention. AIA model group (n = 5): received a subcutaneous injection of CFA on day 1, followed by daily oral gavage of an equivalent volume of saline for 25 consecutive days. MTX group (n = 5): received a subcutaneous injection of CFA on day 1, followed by oral administration of MTX suspension solution (1 mg/kg/day) for 25 days. LVM group (n = 5): received a subcutaneous injection of CFA on day 1, followed by oral administration of LVM solution (30 mg/kg/day) for 25 days. The control group and the AIA model group were administered the same volume of saline by gavage.
Therapeutical Effect Towards AIA
The body weight, foot thickness of rats, and arthritis index were measured at the outset of the study (day 0) and at five-day intervals thereafter.17 The foot swelling thickness was recorded at days 5, 10, 15, 20, and 25 post-modeling. The arthritis index is used to evaluate the degree of swelling and erythema of the rats’ per limbs, with a maximum score of 16 per rat. The scoring criteria are as follows: The scoring criteria for the arthritis index are as follows: 0 points, normal; 1 point, erythema and mild swelling confined to the ankle and toes; 2 points, erythema and mild swelling extending from ankle to midfoot; 3 points, erythema and severe swelling extending from the ankle joint to the metatarsal joint; 4 points, ankylosing deformity with joint swelling.11
The spleen, an important immune organ in RA disease, was removed and weighed to determine the spleen index after sacrifice. The spleen index was calculated as the ratio of the mean organ weight to the mean body weight. Meanwhile, as it is well known that the synovial membrane is prone to inflammation during RA pathology, the synovial membrane was stained for analysis. The staining method previously described was employed to stain the joint synovium and spleen of the rat with hematoxylin and eosin. The stained tissue was then observed under a microscope to assess the severity of RA.
Following euthanasia, the hind limb of each rat was fixed in 4% formaldehyde. The ankle joint and paw were then analyzed by 3D microcomputed tomography (micro-CT, Bruker SkyScan 1272, America). The parameters employed were as follows: a voltage of 60 kV, an electric current of 166 μA, and an exposure time of 1399 ms.
Statistical Analysis
The statistical analysis was conducted using SPSS 26.0 (IBM) software. The data were plotted using GraphPad Prism Software (version 8.0.1). The data are presented as the Mean ± SEM, with statistical significance set at p < 0.05.
Results
28-Day General Toxicological Study of LVM in SD Rat
The experimental procedure is depicted in Figure 1A. Observations of macroscopic changes indicate that during the 28-day repeated oral administration of LVM, no significant abnormal changes were observed in any of the dosage groups compared to the blank control group, except for a decrease in spontaneous activity in the high-dose group after 7 days of repeated administration. There was no significant difference in body weight between the control and LVM-treatment groups over the 28-day repeated oral administration, as shown in Figure 1B. This indicated that oral LVM administration did not affect the rats’ appetite or weight. The liver coefficients of rats in the orally administered LVM groups at various doses were significantly increased compared to the control group (p <0.01). However, there were no significant differences in the coefficients of the heart, spleen, lungs, kidneys, and brain between the orally administered LVM group and the control group (p > 0.05), as illustrated in Figure 1C. H&E staining and microscopic pathological observations were conducted on vital organs such as the heart, liver, spleen, lungs, and kidneys of rats in each group. No significant damage was observed in any of the organs compared to the control group (Figure 1D). The findings of this study indicate that oral administration of LVM for 28 days did not cause organic damage to the organs of rats, and all organs in each group were healthy and normal.
 |
Figure 1 28-day general toxicological study (A) Experimental workflow for the general toxicity assessment of gavage LVM administration in SD Rats. (B) Changes in the body weight of rats following continuous gavage administration of LVM for 28 days. (C) Organ weight/body weight (O/B) coefficient of rats following continuous gavage administration of LVM for 28 days. (D) Images of H&E staining of organs at 200 x magnification (Scale bar=100 μm). All data are shown as mean ± SEM. ** p < 0.01 compared with the control group. n = 10 in each group. |
As demonstrated in Table 1, there were no significant alterations in the hepatobiliary function indices of ALB, TBIL, AST, ALT, TP, ALP, and the blood lipid index of TG in the serum of rats across all LVM-treatment groups administered orally. These findings indicate that the oral administration of LVM yielded no discernible impact on hepatic function. In terms of renal indicators, creatinine (CREA) was significantly reduced in the low-dose group compared with the control group (p < 0.05), while blood urea nitrogen (BUN) was significantly increased in the high-dose group (p < 0.05). Furthermore, the cholesterol (CHOL) and creatine kinase (CK) indices were significantly increased in the high-dose group (p < 0.05) in comparison to the control group. Changes in renal function markers may be a normal physiological response or influenced by environmental factors. Furthermore, the fluctuation trend of these markers is inconsistent with the fluctuating changes of markers for kidney injury.
 |
Table 1 Parameters of Blood Biochemical Examination (n=10, Mean ± SD) |
The above data indicate that oral administration of LVM does not significantly affect the physiological function of the liver and kidneys.
In addition, a hematological examination was conducted to evaluate the potential impact of LVM on the body’s blood system and coagulation function (Table 2). The results demonstrated a non-significant decrease in WBC, RBC, HGB, HCT, PLT, and MPV between the control and each dose group after four weeks. In comparison to the control group, the median-dose group exhibited a significantly decreased median corpuscular hemoglobin concentration (MCHC), a significantly increased red cell distribution width (RDW-SD), and a significantly increased RDW-CV in the high-dose group (p < 0.05). While certain indicators demonstrated significant deviations, their slight deviation beyond the normal range fell within 10% of clinically acceptable limits. It can be assumed that oral administration of LVM had no significant effect on the hematological system and coagulation function of rats.
 |
Table 2 Parameters of Hematological Examination (n=10, Mean ± SD) |
The experimental results demonstrated that long-term administration of LVM exhibited no evident toxicity towards the hematologic system.
28-Day Neurotoxicity Study of LVM in SD Rat
The experimental design of the MWM test is depicted in Figure 2A. The time taken by rats to locate the hidden platform reflected their learning and memory function, with shorter latencies indicating stronger abilities. During the training phase from day 24 to day 27, there were no significant differences in the ability to find the target platform between the control group and the LVM groups (Figure 2B). Furthermore, there were no significant differences in the average swimming speed (Figure 2C) and total path length (Figure 2D) between the LVM groups and the control group. In the probe trial on day 28, the number of times the LVM groups crossed the missing platform within 60 seconds did not differ significantly from that of the control group (Figure 2E and F). Although the LVM groups exhibited a tendency to spend less time in the quadrant where the target platform was located, this difference was not statistically significant (Figure 2G).
 |
Figure 2 Evaluation of cognitive function using the Morris Water Maze Test following gavage Administration of LVM in Rats. (A) The experimental design of the MWM test is displayed (B) Time for rats to find the hidden platform. (C) Average swimming speed of rats. (D) Total distance covered by rats to find the target platform. (E) Number of times rats crossed the platform. (F) Representative swimming routes of rats from the first quadrant to the target platform on the fifth and sixth days. (G) Time spent by rats in the target quadrant. n = 10 in each group. |
These results indicate that oral administration of LVM did not significantly impair the spatial learning and memory abilities of rats in the MWM test when compared to the control group.
Following the histological examination of the hippocampus and corpus callosum in the four groups, the hippocampal slices of the control group and the LVM-treated group exhibited normal morphological structures (Figure 3A). There was no evidence of infiltration of inflammatory cells or neuronal loss. Similarly, the corpus callosum slices of the control group and the LVM group also demonstrated normal morphological structures (Figure 3B). Compared to the control group, the corpus callosum exhibited greater density and no overall structural loss. Transmission electron microscopy observations of the ultrastructure of the myelin sheath revealed that in the three dosage groups, the myelin sheath lamellar structure was relatively dense and intact, with no apparent pathological changes such as focal dissolution and edema. There was no significant difference compared to the control group, as shown in Figure 3C and D. The brain tissue of rats was dissected to observe the depth of dye color on the brain surface. The findings revealed no significant difference between the control group and the various dosage groups (Figure 3E).
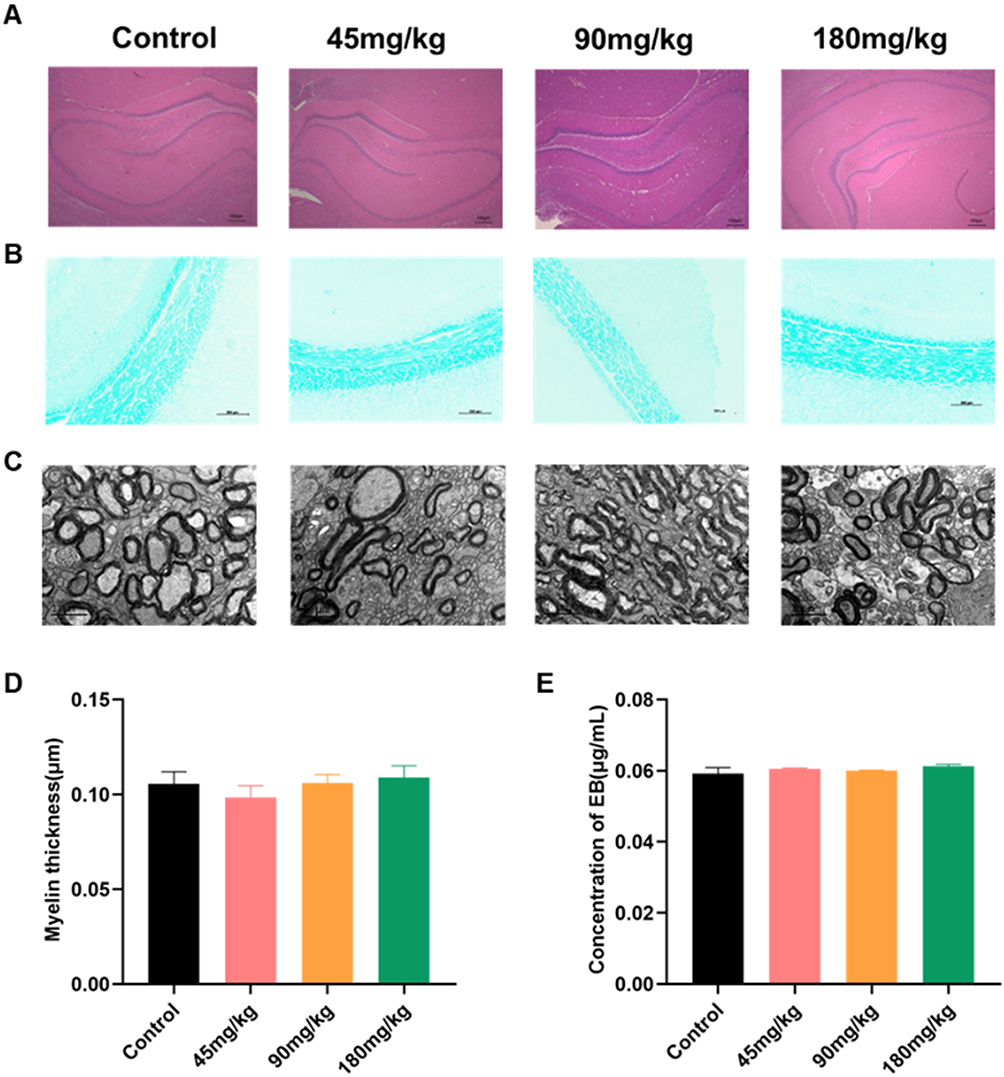 |
Figure 3 (A) H&E pathological sections of rat hippocampus (Scale bar=100μm). (B) LFB staining of rat corpus callosum (Scale bar=200 μm). (C) Transmission electron microscopy of the corpus callosum (Scale bar=100 μm). (D) Analysis of differences in myelin sheath thickness. (E) Concentration of Evans Blue dye in the rat’s brain. |
These results indicate that oral administration of LVM did not significantly affect learning and memory in rats. There were no significant pathological changes in the hippocampus and corpus callosum, and the structure of the nerve myelin sheath and the blood-brain barrier remained intact without damage.
Therapeutical Effect Towards AIA
The experimental procedure is depicted in Figure 4A. The body weight of all rats gradually increased throughout the experimental period, as illustrated in Figure 4B. Following LVM treatment, several clinical phenotypes exhibited improvements, including the arthritis index, paw swelling, and paw thickness (Figure 4C–E). The reduction in paw swelling and redness after administration of LVM is more clearly depicted in Figure 4F. Micro-CT imaging analysis revealed that the ankle joints of rats in the control group exhibited a clear and smooth structure, whereas the model group demonstrated bone destruction with high open porosity. Notably, the bone structure was distinctly improved after the treatment of LVM (Figure 4G). The histological examination of synovial tissues revealed a number of pathological changes in AIA rats, including the infiltration of inflammatory and lymphocytes cells, connective tissue fibrosis, destruction of the cavity structure, and vascular hyperplasia. These pathological changes were effectively alleviated in the LVM group and positive control groups (Figure 4H). From the results of H&E staining of the spleen, healthy rats exhibited a structure comprising the white and red pulp, with the principal artery traversing the white pulp and encircled by a marginal zone. In contrast, the white pulp in the AIA model group exhibited structural deformation and proliferation, while these changes could be alleviated after LVM treatment (Figure 4I).
 |
Figure 4 Therapeutic Efficacy of LVM in the AIA Rat Model. (A) The process of research on therapeutical effect in the AIA rat model. Rats were divided into four groups, including the Control, AIA, MTX, and LVM groups. (B) Body weight changes of rats in each group after drug administration. (C) Arthritis scores of rats. (D) Changes in paw volume of rats within 25 days of gavage administration. (E) Changes in paw thickness of rats within 25 days of gavage administration (F) The macroscopic observations and (G) micro 3D analysis images of inflammation and swelling in the foot of rats. (H) The results of H&E staining of synovial membrane and (I) spleen from rats in each group (Scale bar=100 μm) were shown. All data are presented as mean ± SEM. #p < 0.05, ##p < 0.01 compared with the control group; *p < 0.05, **p < 0.01 compared with the model group. |
All results in this part demonstrated a positive therapeutic effect on AIA in rats.
Discussion
There is a lack of toxicity evaluation data for LVM. Recent research has shown that subchronic intraperitoneal injection of LVM can lead to behavioral, cognitive, biochemical, and hematological changes.18 However, orally administered LVM did not cause significant changes in rats in this experiment. This suggests that oral administration may be safer than intraperitoneal injection and provides insights for the clinical use of LVM.
Since most adverse reactions reported for LVM are related to long-term administration, evaluating the general toxicity of orally administered LVM has clinical significance. The clinical dose of LVM is 2.5 mg/kg, equivalent to 15 mg/kg in rats. In a preliminary 2-week repeated oral dose toxicity study in rats, the lowest dose that did not result in any treatment-related adverse reactions was 180 mg/kg, which is approximately 12 times the clinical dosage. Therefore, we selected doses of 45 mg/kg, 90 mg/kg, and 180 mg/kg in rats, corresponding to 3, 6, and 12 times the clinical dose.
From the serum biochemistry results, compared with the control group, the renal function indicator BUN was significantly increased in the high-dose group (p<0.05). CREA indicators were significantly reduced in the low-dose group compared with the blank group (p<0.05). However, if the kidney is damaged, CREA will be relatively increased, and clinically BUN and CREA are often used to evaluate the indicators of the patient’s renal function status.19 The reduced CREA in the low-dose group may be caused by individual differences. Considering the pathological results, as well as the AST, ALT, CREA, and BUN indicators, it can be seen that high-dose exposure to LVM did not cause drug accumulation in the kidneys and liver. Compared with the control group, the CK and CHOL index were significantly increased in the high-dose group (p<0.05). The normal range of CK in rat serum is 55–650 U/L. However, in the medium and high dose groups, CK levels were found to be significantly higher than normal values. Elevated serum CK levels may be associated with heart disease, but no damage to cardiac muscle cells was observed in the pathological results.20 It could also be caused by exposure to certain drugs or toxins, so it cannot provide a specific diagnosis but rather indicate the need for further evaluation. Although CHOL is outside the normal range, it does not exceed 10% of its own value, so it has no toxicological significance.21
The hematological results indicated that high-dose exposure to LVM did not result in any significant changes. The mean corpuscular hemoglobin concentration (MCHC), red cell distribution width (RDW-SD), and RDW-CV parameters exhibited some differences when compared to the control group. However, the magnitude of these differences was within 10% of the mean value of the control group and within the normal range of this laboratory. Consequently, these differences have no toxicological significance. It has been reported that a single intraperitoneal injection of LVM can cause a significant increase in lymphocyte count and neutrophil count after inducing pleurisy.22 It has also been reported that oral administration of LVM at a dose of 25 mg/kg for three consecutive days caused toxicity in beagles, characterized by a significant decrease in total red blood cell (RBC) count and an increase in alanine aminotransferase (ALT) activity.23 However, no changes in these indicators were observed in this experiment.
LVM has been associated with neurological demyelinating diseases as an adverse reaction, which has been widely reported in clinical settings.24 However, many reports of adverse reactions are related to drug combinations.25 Furthermore, there have been few experiments that specifically examine the reaction after LVM administration alone. To investigate the most prevalent form of nerve myelin damage associated with LVM, we employed the Morris water maze test, a validated tool for evaluating spatial learning and memory in rats.26,27 Our findings revealed that there were no discernible differences in the data analysis compared to the control group at doses exceeding 3, 6, and 12 times the clinical dose. Additionally, we employed LFB staining and H&E staining to examine the microscopic pathology of the corpus callosum and hippocampus in rats.28 The blood-brain barrier (BBB) plays a pivotal role in preventing the entry of harmful substances into brain tissue and maintaining internal stability. Its destruction may result in inflammation and neurodegenerative diseases.29–31 To assess the impact of drug administration on BBB permeability, we employed Evans blue staining. Transmission electron microscopy was employed to facilitate further observation of myelin damage. The integrated analysis of these experiments demonstrated that LVM exhibited no discernible toxic effect on brain myelin sheath at the selected dose. LVM has been reported to induce adverse reactions such as vasculitis, granulocytopenia, and immunosuppression.32,33 The immunosuppression and symptoms of vasculitis associated with LVM are generally mild and may resolve spontaneously.34 Furthermore, the majority of vasculitis cases are linked to the use of cocaine adulterated with LVM, and existing data do not rule out the possibility that cocaine may contribute to the occurrence of these adverse reactions.33 The overall incidence of granulocytopenia is relatively low; in our study, there were no significant changes in white blood cell counts, indicating that neither granulocytopenia nor immunosuppression occurred in SD rats. However, further experimental studies are necessary to systematically evaluate the patterns and mechanisms underlying these adverse reactions.
As previously stated, the 15 mg/kg dose of LVM in rats is equivalent to the clinical dosage. Given the interspecies differences between humans and rats and the aforementioned toxicological research findings, our group scaled up the treatment dose to twice the amount of the clinical dosage. Therefore, we chose a dose of 30 mg/kg to investigate the therapeutic effects of LVM on RA through oral administration. The study demonstrated that LVM effectively reduced joint redness, swelling, arthritis index scores, paw pad thickness, and swelling. As joint erosion and damage are the primary causes of disability in RA, the study examined whether LVM could protect bone joints using micro-CT.35,36 The results demonstrated a distinct reduction in joint erosion by LVM. Synovitis is a defining feature of RA,37 and the results of H&E staining of synovial tissue demonstrated that LVM could significantly alleviate the pathological state of the synovium. Additionally, the spleen serves as a peripheral immune organ, containing a rich population of lymphocytes and functioning as the site of adaptive immunity to antigens.38,39 The weight of the spleen is directly correlated with the quantity of immune cells it contains, and this index reflects the extent of lymphocyte proliferation. However, excessive inflammation may result in impairment of these organs’ function.40 In comparison to the model group, LVM treatment demonstrated positive effects on spleen tissue, including the mitigation of abnormal spleen tissue proliferation and the alleviation of pathological symptoms. The results of the aforementioned studies indicate that LVM can be safely and effectively used to treat RA in animal models. This provides a reference for the clinical application of LVM in treating RA. Currently, the most commonly used medications in clinical practice are methotrexate and TNF-α inhibitors, with numerous reports documenting the adverse effects associated with methotrexate.6 Although TNF-α inhibitors can significantly improve signs and symptoms, their long-term and frequent use is linked to an increased risk of infections, notably higher than that observed in the non-biologic treatment group. Furthermore, this treatment approach is costly, and prolonged use can impose a significant financial burden on patients and their families.41 In contrast, the widespread clinical application of LVM for the treatment of RA could significantly alleviate the economic burden of disease management for patients. Nevertheless, the experimental design has inherent limitations, and future experiments will explore additional dosage levels to assess the therapeutic effects.
Conclusion
This study has demonstrated that LVM has the potential to be a promising therapeutic agent for the treatment of RA, with minimal general toxicity and neurotoxicity from 45 mg/kg to 180 mg/kg. From the perspectives of drug safety, efficacy, and economics, LVM offers unique advantages compared to commonly used clinical medications. This article provides information on the safe clinical use of LVM within the toxicological range and its therapeutic effects on RA. However, further research is necessary to assess the overall toxicity mechanism of LVM in RA of LVM and its potential for causing neurological demyelinating adverse reactions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was kindly supported by grants from the Scientific Research Initiation Fund of Fujian Medical University (No. 60000166), the Fujian Provincial Department of Science and Technology Joint Innovation Project Fund (No. 2021Y4011), and the Key Laboratory of Pharmaceutical Analysis and Laboratory Medicine (Putian University), Fujian Province University (No. PALM 202208).
Disclosure
This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-3958399/v1. The authors report no conflicts of interest in this work.
References
1. Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016;388(10055):2023–2038. doi:10.1016/s0140-6736(16)30173-8
2. Venetsanopoulou AI, Alamanos Y, Voulgari PV, Drosos AA. Epidemiology of rheumatoid arthritis: genetic and environmental influences. Expert Rev Clin Immunol. 2022;18(9):923–931. doi:10.1080/1744666x.2022.2106970
3. Radu AF, Bungau SG. Management of Rheumatoid Arthritis: an Overview. Cells. 2021;10(11):2857. doi:10.3390/cells10112857
4. Calle AM, Aguirre N, Ardila JC, Cardona Villa R. DRESS syndrome: a literature review and treatment algorithm. World Allergy Organ J. 2023;16(3):100673. doi:10.1016/j.waojou.2022.100673
5. Hua C, Buttgereit F, Combe B. Glucocorticoids in rheumatoid arthritis: current status and future studies. RMD Open. 2020;6(1):e000536. doi:10.1136/rmdopen-2017-000536
6. Wang W, Zhou H, Liu L. Side effects of methotrexate therapy for rheumatoid arthritis: a systematic review. Eur J Med Chem. 2018;158:502–516. doi:10.1016/j.ejmech.2018.09.027
7. Amery WK, Bruynseels JP. Levamisole, the story and the lessons. Int J Immunopharmacol. 1992;14(3):481–486. doi:10.1016/0192-0561(92)90179-o
8. Miller MJ. Use of levamisole in parasitic infections. Drugs. 1980;20(2):122–130. doi:10.2165/00003495-198020020-00005
9. Mühlig AK, Lee JY, Kemper MJ, et al. Levamisole in Children with Idiopathic Nephrotic Syndrome: clinical Efficacy and Pathophysiological Aspects. J Clin Med. 2019;8(6):860. doi:10.3390/jcm8060860
10. Meng Y, Li B, Jin D, Zhan M, Lu J, Huo G. Immunomodulatory activity of Lactobacillus plantarum KLDS1.0318 in cyclophosphamide-treated mice. Food Nutr Res. 2018;62:1296. doi:10.29219/fnr.v62.1296
11. Couderc A, Bérard E, Guigonis V, et al. Treatments of steroid-dependent nephrotic syndrome in children. Arch Pediatr. 2017;24(12):1312–1320. doi:10.1016/j.arcped.2017.09.002
12. Qiao X, Wang C, Wang W, et al. Levamisole enhances DR4-independent apoptosis induced by TRAIL through inhibiting the activation of JNK in lung cancer. Life Sci. 2020;257:118034. doi:10.1016/j.lfs.2020.118034
13. Sany J. Immunological treatment of rheumatoid arthritis. Clin Exp Rheumatol. 1990;8(5):81–88.
14. Feldmann JL, Mery C, Amor B, Kahan A, de Gery A, Delbarre F. Effectiveness of levamisole in rheumatoid arthritis: immune changes and long-term results. Scand J Rheumatol. 1981;10(1):1–8. doi:10.1080/03009748109095263
15. Ahammadunny R, Rathish B, Abraham M, Wilson A, Warrier A. A Case of Levamisole Induced Multifocal Inflammatory Leukoencephalopathy and Secondary Nocardia Veterana Brain Abscess. Ann Indian Acad Neurol. 2021;24(5):814–816. doi:10.4103/aian.AIAN_575_20
16. Jain S, Tripathi S, Tripathi PK. Antioxidant and antiarthritic potential of berberine: in vitro and in vivo studies. Chin Herb Med. 2023;15(4):549–555. doi:10.1016/j.chmed.2023.02.007
17. Bao J, Song Y, Hang M, et al. Huangqi Guizhi Wuwu Decoction suppresses inflammation and bone destruction in collagen-induced arthritis mice. Chin Herb Med. 2024;16(2):274–281. doi:10.1016/j.chmed.2023.10.003
18. Laurentino AOM, Solómon J, Tonietto BD, et al. Levamisole, a cocaine cutting agent, induces acute and subchronic systemic alterations in Wistar rats. Toxicol Appl Pharmacol. 2021;426:115649. doi:10.1016/j.taap.2021.115649
19. Li H, Dong S, Liu Y, et al. Efficacy and Safety of ”Bushen Huoxue Therapy”-Based Combined Chinese and Western Medicine Treatment for Diabetic Kidney Disease: an Updated Meta-Analysis of 2105 Patients. Evid Based Complement Alternat Med. 2022;2022:3710074. doi:10.1155/2022/3710074
20. Roberts R, Sobel BE. Creatine kinase isoenzymes in the assessment of heart disease. Am Heart J. 1978;95(4):521–528. doi:10.1016/0002-8703(78)90245-4
21. Liu Z, Xu P, Gong F, et al. Altered lipidomic profiles in lung and serum of rat after sub-chronic exposure to ozone. Sci Total Environ. 2022;806(Pt 2):150630. doi:10.1016/j.scitotenv.2021.150630
22. Kuropka P, Leśków A, Małolepsza-Jarmołowska K, et al. Effect of a Single and Triple Dose of Levamisole on Hematological Parameters in Controlled Inflammation Model. Animals (Basel). 2022;12(16):2110. doi:10.3390/ani12162110
23. Gokce HI, Gunes V, Erdogan HM, Citil M, Akca A, Yuksek N. The effects of levamisole poisoning on the haematological and biochemical parameters in dogs. Dtsch Tierarztl Wochenschr. 2004;111(2):81–85.
24. Campillo JT, Eiden C, Boussinesq M, Pion SDS, Faillie JL, Chesnais CB. Adverse reactions with levamisole vary according to its indications and misuse: a systematic pharmacovigilance study. Br J Clin Pharmacol. 2022;88(3):1094–1106. doi:10.1111/bcp.15037
25. Michels L, Moisa M, Stämpfli P, et al. The impact of levamisole and alcohol on white matter microstructure in adult chronic cocaine users. Addict Biol. 2022;27(3):e13149. doi:10.1111/adb.13149
26. Othman MZ, Hassan Z, Che Has AT. Morris water maze: a versatile and pertinent tool for assessing spatial learning and memory. Exp Anim. 2022;71(3):264–280. doi:10.1538/expanim.21-0120
27. Jin H, Yang C, Jiang C, et al. Evaluation of Neurotoxicity in BALB/c Mice following Chronic Exposure to Polystyrene Microplastics. Environ Health Perspect. 2022;130(10):107002. doi:10.1289/ehp10255
28. Yardım A, Kandemir FM, Çomaklı S, et al. Protective Effects of Curcumin Against Paclitaxel-Induced Spinal Cord and Sciatic Nerve Injuries in Rats. Neurochem Res. 2021;46(2):379–395. doi:10.1007/s11064-020-03174-0
29. Chow BW, Gu C. The molecular constituents of the blood-brain barrier. Trends Neurosci. 2015;38(10):598–608. doi:10.1016/j.tins.2015.08.003
30. Obermeier B, Daneman R, Ransohoff RM. Development, maintenance and disruption of the blood-brain barrier. Nat Med. 2013;19(12):1584–1596. doi:10.1038/nm.3407
31. AlFadly ED, Elzahhar PA, Tramarin A, et al. Tackling neuroinflammation and cholinergic deficit in Alzheimer’s disease: multi-target inhibitors of cholinesterases, cyclooxygenase-2 and 15-lipoxygenase. Eur J Med Chem. 2019;167:161–186. doi:10.1016/j.ejmech.2019.02.012
32. Pinals RS. The non-hematological side effects of levamisole in the treatment of rheumatoid arthritis--A review. J Rheumatol Suppl. 1978;4:71–75.
33. Abdul-Karim R, Ryan C, Rangel C, Emmett M. Levamisole-induced vasculitis. Proc (Bayl Univ Med Cent). 2013;26(2):163–165. doi:10.1080/08998280.2013.11928946
34. Chang A, Osterloh J, Thomas J. Levamisole: a dangerous new cocaine adulterant. Clin Pharmacol Ther. 2010;88(3):408–411. doi:10.1038/clpt.2010.156
35. Díaz-González F, Hernández-Hernández MV. Rheumatoid arthritis. Med Clin. 2023;161(12):533–542. doi:10.1016/j.medcli.2023.07.014
36. Lei Q, Yang J, Li L, et al. Lipid metabolism and rheumatoid arthritis. Front Immunol. 2023;14:1190607. doi:10.3389/fimmu.2023.1190607
37. Firestein GS, McInnes IB. Immunopathogenesis of Rheumatoid Arthritis. Immunity. 2017;46(2):183–196. doi:10.1016/j.immuni.2017.02.006
38. Lewis SM, Williams A, Eisenbarth SC. Structure and function of the immune system in the spleen. Sci Immunol. 2019;4(33). doi:10.1126/sciimmunol.aau6085
39. Mebius RE, Kraal G. Structure and function of the spleen. Nat Rev Immunol. 2005;5(8):606–616. doi:10.1038/nri1669
40. Guo H, Wang Y, Cui H, et al. Copper Induces Spleen Damage Through Modulation of Oxidative Stress, Apoptosis, DNA Damage, and Inflammation. Biol Trace Elem Res. 2022;200(2):669–677. doi:10.1007/s12011-021-02672-8
41. Sampaio-Barros PD, van der Horst-Bruinsma IE. Adverse effects of TNF inhibitors in SpA: are they different from RA? Best Pract Res Clin Rheumatol. 2014;28(5):747–763. doi:10.1016/j.berh.2014.10.001
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.