")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Saudi Radiology Technologists’ Perception of Occupational Hazards from a Personal and Social Lens
Authors Alshamrani KM , Alzahrani DA, Alghamdi YS, Aljohani LM, Al Nufaiei ZF
Received 29 August 2024
Accepted for publication 24 October 2024
Published 30 October 2024 Volume 2024:17 Pages 2609—2622
DOI https://doi.org/10.2147/RMHP.S492974
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kubra Kaya
Khalid M Alshamrani,1– 3 Dana A Alzahrani,1 Yara S Alghamdi,1 Lama M Aljohani,1 Ziyad F Al Nufaiei1– 3
1College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 2King Abdullah International Medical Research Center, Jeddah, Saudi Arabia; 3Ministry of the National Guard - Health Affairs, Jeddah, Saudi Arabia
Correspondence: Khalid M Alshamrani, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, P. O. Box 9515, Internal Mail Code 6610, Jeddah, 21423, Saudi Arabia, Tel +966-12-2266666 Ext 46396, Email [email protected]
Background: Occupational hazards among healthcare workers (HCWs) present serious risks, from infectious diseases to physical and chemical dangers, along with psychological stress, all of which threaten their health and safety. This study aims to identify the unique challenges and hazards encountered by radiology technologists in in Saudi Arabia by assessing the key factors contributing to these risks.
Methods: A descriptive questionnaire study was conducted in January-February 2023, targeting 75 radiology technologists at King Abdulaziz Medical City (KAMC), Jeddah, with participants recruited via non-probability convenience sampling and invited to complete a widely recognized questionnaire previously used among radiographers. Descriptive statistics were calculated, and the Kruskal–Wallis H-test was conducted to examine the relationships between demographic factors and different aspects of occupational hazards.
Results: Of the 75 technologists contacted, 63 responded, resulting in an 84% participation rate. Workload, work shifts, and patient-related factors are major contributors to occupational hazards, surpassing technologist-specific and organizational elements. Additionally, 68.3% cited rigid leadership and unequal treatment as aggravating factors, while insufficient staffing, inadequate protective devices, and patient interaction were also significant concerns. Over 60% identified bending, lifting heavy patients, prolonged radiation exposure, and frequent walking as major hazard sources.
Conclusion: Key occupational hazards factors facing radiology technologists include high workloads, work shifts, and patient-related issues, with 68.3% citing rigid leadership and unequal treatment as exacerbating risks. Insufficient staffing and protective devices, along with demanding work conditions, further heighten these hazards. This study emphasizes the need for targeted interventions in staffing, resources, and culture to improve radiology technologists’ safety.
Keywords: healthcare workers, Kingdom of Saudi Arabia, occupational health, professional risk, radiologic technology, safety
Graphical Abstract:

Introduction
Occupational Safety and Health (OSH) is a multidisciplinary field focused on ensuring the safety and well-being of workers.1 Its primary aim is to create and maintain a safe and healthy work environment through comprehensive health and safety programs.2 Under common law, employers are legally obligated to prioritize the safety of their employees, with additional regulations often set by government bodies to enforce specific standards and tasks.3 OSH not only safeguards workers but also extends protection to coworkers, families, employers, and others who may be impacted by the working environment.4
A healthcare facility is dedicated to providing patient care through various services, including diagnosis, treatment, and preventive measures.5 Individuals employed within these facilities are recognized as healthcare workers (HCWs).6 Globally, healthcare facilities employ more than 59 million workers, according to the World Health Organization (WHO).7,8 In the Kingdom of Saudi Arabia (KSA), the healthcare sector employs around 424,000 workers, comprising both Saudi citizens and expatriates.9 In healthcare settings, particularly hospitals, infection control is a critical aspect of patient care.10 Hospitals, while dedicated to treating diseases, also serve as environments where individuals with compromised health are more susceptible to infections.11
For radiology workers, adhering to infection control policies is a fundamental professional responsibility, essential for ensuring the safety of patients, radiology technologists, and other healthcare team members.12 The ongoing emergence of new diseases, the re-emergence of old ones, and the rise of hospital-acquired infections resistant to multiple drugs underscore the importance of these policies in preventing the spread of infections.13 In the field of radiology, occupational hazards are diverse and include biological, psychological, and physical risks.14 Among these, ionizing radiation stands out as a critical diagnostic tool in medical imaging, widely utilized across various therapeutic and diagnostic applications. While ionizing radiation plays a pivotal role in modern medicine, it is essential to balance its benefits with the associated risks.15 The hazardous effects of ionizing radiation on biological systems are well-documented, including its potential to cause irreversible damage.16 Exposure to ionizing radiation has been linked to an increased risk of cancer and can adversely affect various systems in the body, such as the gastrointestinal and central nervous systems, as well as the gonads.17 These effects may manifest in the individual exposed (somatic effects) or in future generations (genetic effects).18
The working conditions of HCWs are closely tied to the quality of care provided to patients. Factors such as psychosocial dynamics, shift schedules, work hours, team management, and organizational culture all play crucial roles in determining the health and safety of HCWs.19–21 Contrary to the common perception that HCWs are resistant to illness, research reveals a different reality.6,22–26 Ensuring the well-being of HCWs not only safeguards public health but also strengthens a workforce that constitutes 10 to 18% of a nation’s total workforce.9,27 Despite efforts to reduce occupational risks, HCWs around the world still encounter various biological and non-biological hazards in their workplaces.28,29
In Saudi Arabia, the Ministry of Health (MOH) established a standardized policy to ensure a safe and healthy environment across all public and private healthcare facilities. Each facility has developed its own vision, mission, and policies, aligned with the overarching guidelines set by the MOH.5 Regular evaluation of the occupational health risks encountered by healthcare workers is crucial for enhancing the nation’s public healthcare system.20,27 This improvement can be realized by identifying the current prevalence of health hazards and the risk factors that healthcare workers face in their workplaces.27,29 In 2018, Abdulmageed et al conducted research on 161 hCWs at a Hospital in Jeddah to identify the risk factors for biological hazards. Their findings revealed that 32.90% of the participants had experienced sharps injuries, with nurses being especially vulnerable due to factors like long work hours, rotating shifts, and heavy workloads.25 A recent study involving 379 physicians and nurses across six hospitals in Makkah found that 67.8% had experienced work-related injuries.30 A study conducted in select government hospitals in Saudi Arabia revealed that nurses, in particular, face an annual incidence of 3.2 needlestick injuries (NSIs) per 100 occupied beds.31 Similarly, recent research in a Medina region hospital reported that 32% of HCWs experience NSIs each year.32 Furthermore, in a study of 450 dental assistants from 40 private clinics in Jeddah, 63% reported experiencing NSIs but did not report them to authorities, with factors such as non-compliance with hepatitis B vaccination protocols, inadequate knowledge of infection control, and attending to 12 or fewer patients daily being significantly linked to a higher risk of NSIs.33
The existing literature reveals a notable gap in research on occupational hazards specific to radiology technologists, both globally and in Saudi Arabia. While studies have generally addressed HCWs, they have largely overlooked the unique risks faced by radiology technologists, who are exposed to a distinct set of hazards, including radiation. This study seeks to address this gap by focusing exclusively on the occupational hazards encountered by radiology technologists in the study area, with the aim of providing insights that can inform safety protocols both locally and internationally. Our study hypothesizes that radiology technologists in Saudi Arabia are subjected to distinct occupational hazards that are currently underreported or underestimated. This forms the basis for our investigation and sets the stage for a deeper exploration of the associated health implications. The primary objective of this research is to identify and evaluate the key factors contributing to these hazards, thereby offering critical insights that have not been explored in previous studies. This focus not only highlights the significance of the issue but also underscores the necessity of addressing the occupational safety of radiology technologists. In Saudi Arabia, a Radiology Technologist is defined as a professional with a bachelor’s degree, which includes four years of undergraduate education and a one-year internship.34–36
Materials and Methods
Participants and Procedure
A descriptive questionnaire study was carried out between January and February 2023, targeting radiology technologists employed in the medical imaging department at King Abdulaziz Medical City (KAMC) in Jeddah, a prominent tertiary hospital in Saudi Arabia. KAMC is a part of the Ministry of National Guard Health Affairs (MNG-HA), a government-funded health system established in 1983, renowned for its comprehensive healthcare services. The study invited all 75 radiology technologists working at KAMC to participate. Using the Raosoft® Sample Size Calculator,37,38 the recommended sample size was determined to be 63, considering a 5% margin of error and a 95% confidence level. The study focused exclusively on radiology technologists, excluding radiologists and nurses. Participants were recruited through non-probability convenience sampling via Email and WhatsApp invitations. The survey was administered online using Google Forms.
Study Measures
Radiology technologists were invited to complete a questionnaire that has been previously employed among radiographers. The questionnaire was initially developed based on a comprehensive review of relevant literature, with a particular focus on occupational hazards specific to radiology technologists. Notably, we referred to established research, such as Rajan et al’s study on radiographers’ perceptions of occupational hazards,39 to align the questionnaire’s content with existing evidence in this domain and therefore enhance its relevance and content validity. Following its preliminary development and to ensure the instrument’s face validity, the questionnaire underwent a rigorous review process by a panel of experts, including three senior radiology practitioners with substantial expertise in radiological technology, along with the director of infection prevention and control and a consultant microbiologist with extensive experience in environmental and occupational health and safety. This expert review process guaranteed that the questionnaire was precisely tailored to our study’s demographic, was clear and concise, and maintained a focused and purposeful approach for accurately assessing occupational hazards in radiology settings. The questionnaire consistent use in previous research highlights its reliability in capturing similar constructs effectively across studies.40,41
The questionnaire used to gather primary data was divided into two sections. Section “A” focused on the background information of the radiology technologists, while Section “B” addressed nine major causes of occupational hazards, each encompassing various subfactors. The second part of the questionnaire was structured using a five-point Likert scale, offering responses ranging from Strongly Agree to Strongly Disagree, with corresponding values of 5, 4, 3, 2, and 1. The perceptions of the radiology technologists were then quantified and categorized into three levels based on a 5-point Likert scale: 1–2 = Low, 3 = Moderate, and 4–5 = High.
Ethical Consideration
This research received approval from the local Institutional Review Board (IRB) under protocol number SP23J-137-08. Participation was entirely voluntary, with participants providing written informed consent prior to completing the questionnaire. The consent process was integrated into the Google Form questionnaire, where participants were asked to carefully read the consent form at the beginning and indicate their agreement by selecting an option before continuing. All responses were kept anonymous and confidential, adhering strictly to the principles outlined in the Declaration of Helsinki. The electronic survey application generated a password-protected Microsoft Excel file that excluded any identifying participant information.
Statistical Analyses
The statistical analyses were carried out in three distinct phases. Initially, a descriptive analysis was performed to outline demographic characteristics, including counts and percentages, and to compute the mean and standard deviation (SD) for the sample’s scores. Next, the Shapiro–Wilk test was utilized to evaluate the normality of the score distribution. Lastly, Mann–Whitney U and Kruskal–Wallis H nonparametric tests were employed to explore potential variations in weighted mean scores across occupational hazard dimensions based on demographic factors. All analyses were executed using SPSS version 24, with a significance level set at p < 0.05.
Results
Characteristics of the Participants
Table 1 summarizes the sociodemographic profile of the radiology technologists. Out of 75 contacted technologists, 63 responded, yielding a participation rate of 84%. The gender breakdown was 44.4% males (n = 28) and 55.6% females (n = 35). The majority of participants, 77.8% (n = 49), were between the ages of 20 and 30. Nearly half of the participants (46.1%, n = 29) had less than one year of experience, while 41.2% (n = 26) had three or more years of experience. A notable portion (41.3%, n = 26) specialized in radiography, mammography, and fluoroscopy, and 28.6% (n = 18) specialized in computed tomography (CT).
 |
Table 1 Characteristics of the Participants |
Factors Contributing to Occupational Hazards
Table 2 through 6 outline the primary causes and underlying factors contributing to occupational hazards. Figure 1 represents the overall mean of the key dimensions influencing occupational hazards. Workload, work shift, interruptions, and patient-related factors exhibited the highest mean scores (greater than 3.7), followed by radiology technologist-related factors (mean = 3.6) and organizational structure and policy (mean = 3.59). A rigid leadership style and unequal treatment of employees were identified as the leading organizational structure and policy-related factors linked to occupational hazards, with 68.3% (n = 43) of respondents agreeing or strongly agreeing (Table 2). Conversely, tasks such as bending and lifting heavy patients, along with frequent walking and climbing stairs to perform mobile X-rays, were recognized as the primary radiology technologist-related factors contributing to occupational hazards. These factors were agreed upon by 69.8% (n = 44) and 60.3% (n = 38) of respondents, respectively (Table 3).
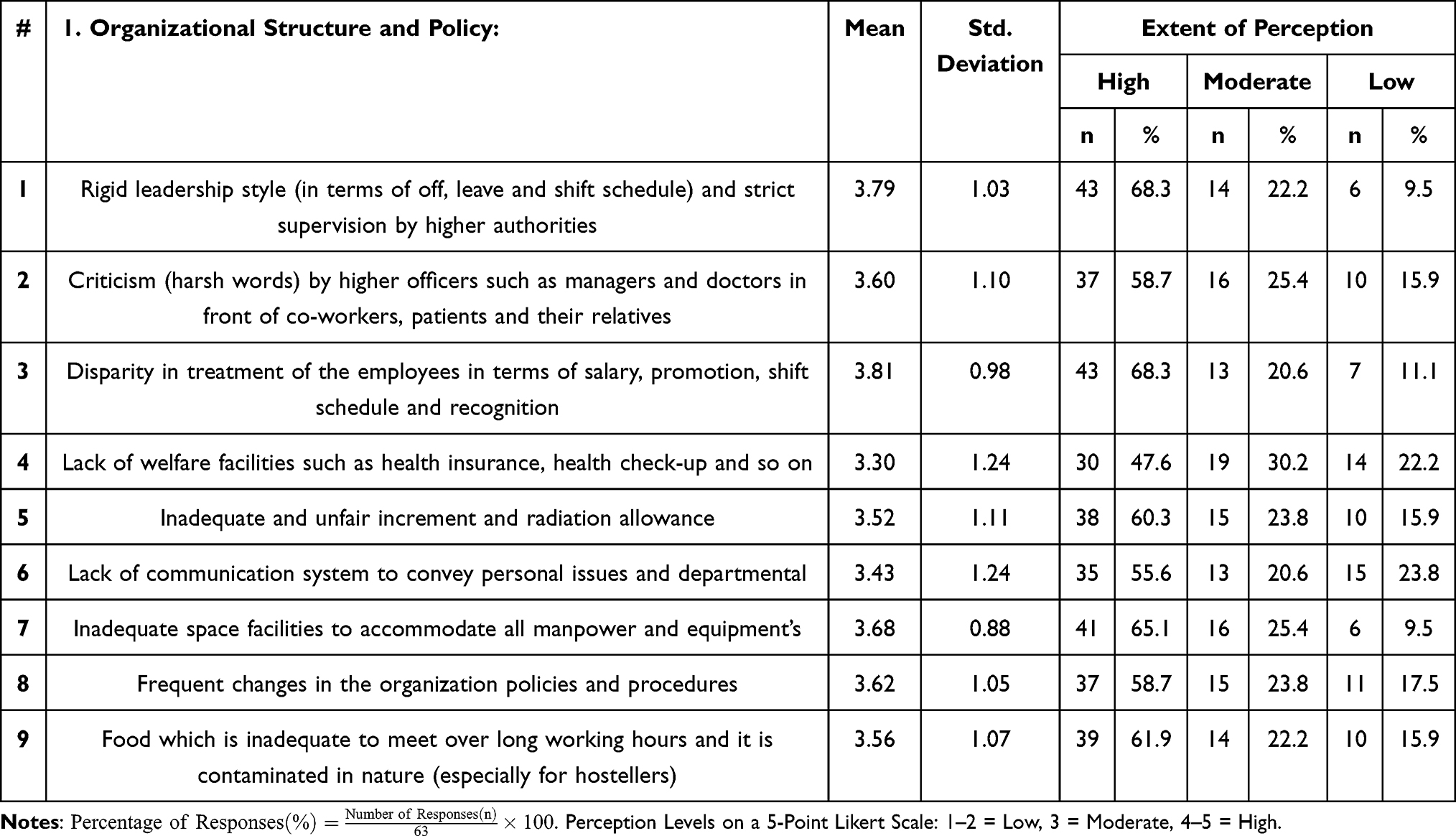 |
Table 2 Causes of Occupational Hazards: Organizational Structure and Policy Factors |
 |
Table 3 Causes of Occupational Hazards: Radiology Technologists’ Specific Factors |
 |
Figure 1 Aggregate Mean of Main Dimensions Contributing to Occupational Hazards. |
The fear of making errors during work processes and report preparation emerged as the top fear and safety-related factor associated with occupational hazards, with nearly half of the participants (49.2%, n = 31) expressing agreement or strong agreement. Furthermore, factors such as insufficient radiographers and support staff, poorly maintained equipment, and the unavailability of doctors were identified as the primary resource-related contributors to occupational hazards, with over 44% of participants agreeing or strongly agreeing (Table 4).
 |
Table 4 Causes of Occupational Hazards: Fear and Safety, Resources Factors |
Excessive workload, cited by 68.3% (n = 43) of participants, along with long working hours and the inability to leave duty on time (65.1%, n = 41), were the most prominent workload and shift-related factors contributing to occupational hazards. Additionally, cramped workspace and prolonged exposure to air conditioning, which increases susceptibility to infections, were identified as the key environment and hygiene-related factors, with more than half of the respondents agreeing or strongly agreeing (Table 5).
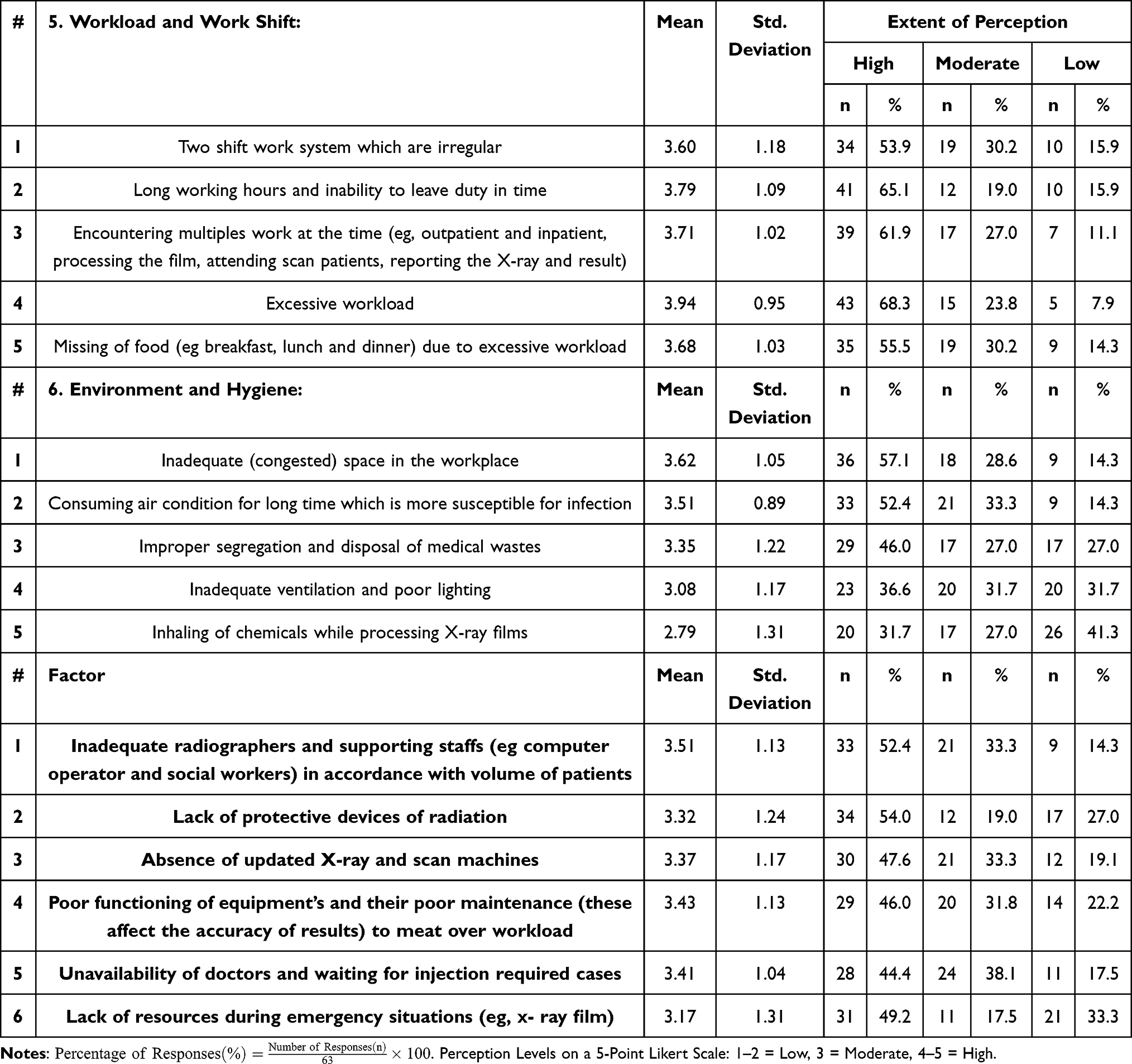 |
Table 5 Causes of Occupational Hazards: Workload & Work Shift, and Environment & Hygiene Factors |
High levels of pressure from various sources, including the heavy involvement of outpatient departments and personal assistants in report-related tasks, as well as receiving conflicting instructions from multiple authorities, were identified as significant contributors to occupational hazards, with over 58% of respondents expressing agreement or strong agreement. Additionally, insufficient information on job-related occupational hazards and the absence of clear guidelines were highlighted as key communication and training issues, with more than half of the participants concurring. Furthermore, dealing with infectious patients, such as those with Tuberculosis or HIV, was noted as a major occupational risk by 76.2% (n = 48) of respondents, while managing emotionally unstable patients and their relatives was identified by 60.3% (n = 38) as a prominent patient-related factor contributing to these hazards (Table 6).
 |
Table 6 Causes of Occupational Hazards: Interruption & Work Shift, Communication & Training, and Patient Factors |
Workload, shift patterns, patient interactions, and interruptions emerged as the primary factors contributing to occupational hazards among radiology technologists (Figure 1). Interestingly, no statistically significant differences were observed in the weighted mean scores across occupational hazard dimensions when analyzed by demographic factors (Table 7).
 |
Table 7 Inferential Analyses of Occupational Hazard Dimensions by Demographic Variables |
Discussion
This study explored potential factors contributing to occupational hazards among radiology technologists at a major tertiary hospital in Jeddah, Saudi Arabia. The research findings suggest several noteworthy trends: First, workload, work shifts, interruptions, and patient-related factors appeared to play a more prominent role in contributing to occupational hazards compared to technologist-specific factors or organizational structure. Additionally, 68.3% of participants reported that a rigid leadership style and disparities in employee treatment might exacerbate occupational hazards within the organization. Over half of the respondents also indicated that insufficient staffing and a lack of adequate radiation protective devices could contribute to these hazards. Moreover, high workloads, extended working hours, and physically demanding tasks were perceived as significant risks by radiology technologists. Finally, frequent interaction with infectious or emotionally unstable patients, along with the fear of making errors, were identified as potential hazards related to patient interaction and safety concerns.
Public hospital staff often face significant challenges due to overwhelming workloads and insufficient staffing, especially in developing countries where health infrastructure is underdeveloped and resources are scarce.42 This environment leaves HCWs particularly vulnerable to various occupational hazards, with stress being a prevalent issue.43 The demands of hospital jobs, characterized by high expectations and heavy workloads, frequently lead to job strain, physical exertion, and increased exposure to hazards, all of which contribute to the stress experienced by healthcare professionals.44 In fact, the present study found that 68.3% of radiology technologists identified excessive workload and 52.4% identified inadequate staffing as significant contributors to these occupational hazards.
In this study, rigid leadership styles and unequal treatment of employees were identified as key organizational factors contributing to occupational hazards, with 68.3% of respondents agreeing or strongly agreeing with this observation. Hierarchical and inflexible leadership can cultivate a work environment marked by heightened stress, diminished autonomy, and poor communication—factors consistently linked to increased occupational risks.45 Such leadership not only stifles employees’ ability to voice concerns but also creates a climate where strict adherence to protocols may overshadow personalized support for staff well-being.46,47 In these settings, radiology technologists may feel powerless to advocate for safer working conditions or challenge policies that heighten their exposure to hazards, such as extended work hours or inadequate radiation safety measures. Moreover, the disparities in employee treatment identified in this study—particularly in salary, promotions, shift schedules, and recognition—reflect an organizational culture where inequality is prevalent. These disparities exacerbate stress and job dissatisfaction, both of which are well-established precursors to mental and physical health issues in healthcare environments.48–51 Employees who perceive themselves as undervalued or unfairly treated are also more prone to burnout, a condition closely linked to compromised safety practices and an elevated risk of errors.48,52
In the present study, 54% of radiology technologists identified the shortage of adequate radiation protective devices and lack of guidelines as a key resource and communication-related factors contributing to occupational hazards. This observation is consistent with previous research conducted among 60 radiographers in a multi-specialty hospital in Tirunelveli City, India, which also highlighted the insufficient availability of protective devices as a significant contributor to occupational risks in the field.39 While the scarcity in the Tirunelveli study was attributed to financial constraints limiting access to essential safety equipment, the situation in the present study may reflect different underlying causes, such as administrative inefficiencies or gaps in policy implementation. Although financial barriers may not be as severe in Saudi hospitals, the shortage of protective devices continues to increase the risk of occupational exposure, underscoring the need for a more systematic approach to resource allocation and enforcement of safety protocols.
The results of the present study reveal that 76.2% of radiology technologists identified dealing with infectious patients, such as those with tuberculosis or HIV, as a primary cause of occupational hazards. These findings are consistent with other studies that highlight the risks associated with exposure to infectious patients.39,53,54 The likelihood of infection following an incident involving contaminated blood depends on several factors, including the type of exposure, the amount of infectious material, the inoculum size, the host’s immune response, and the specific infectious agent involved.54 Moreover, this aligns with research indicating that paramedics, due to their direct patient interactions, face increased vulnerability to occupational health hazards, particularly the risk of contracting hepatitis B in hospital departments where frequent contact with blood is common.53
Occupational hazards in healthcare settings are often rooted in inadequate equipment, poor work environments, and improper posture.39,55 Issues such as insufficient or outdated equipment, poorly designed work areas, and direct physical injuries, along with poor posture, contribute to these risks.56,57 Physical hazards like inadequate lighting, excessive noise, and trauma, as well as biological risks from radiation and microorganisms, further exacerbate the situation. Additionally, prolonged sitting with a flexed or twisted back can lead to neck, lower back, and other musculoskeletal problems among HCWs.56,58,59 The present study highlights that nearly half of radiology technologists identified inadequate workspace, outdated X-ray and scan machines, and malfunctioning equipment as significant contributors to occupational hazards. Furthermore, over 60% of respondents pointed to factors such as bending and lifting heavy patients, prolonged radiation exposure, and frequent walking and climbing stairs to perform mobile X-rays as major sources of these hazards.
Insufficient training and poorly designed environmental programs significantly contribute to occupational hazards.60,61 Previous studies revealed a strong connection between organizational factors—such as the absence of safety training, a weak safety culture, and unsafe practices—and the incidence of work-related injuries among HCWs.62,63 Notably, nearly half of the radiology technologists surveyed identified a lack of information about job-related hazards and insufficient training in critical areas like equipment handling, chemical use, report preparation, and patient interaction as major contributors to these risks.
Limitations
A key limitation of this study is the reliance on non-probability sampling, which may introduce selection bias and limit the generalizability of the findings. Additionally, the small population size reduces the statistical power of the study, potentially affecting the reliability of the results. Furthermore, the data were collected from a single hospital, which limits the ability to compare and generalize the findings across different healthcare settings, reducing the study’s external validity. Another important limitation of this study is the lack of a comparison group, such as other healthcare workers. Without this comparison, it is difficult to ascertain whether the identified occupational hazards are unique to radiology technologists or prevalent across other healthcare professions.
Implication of the Study
The findings of this study offer critical insights into the occupational hazards faced by radiology technologists and underscore the need for targeted interventions to enhance workplace safety. Given the identification of workload, inadequate staffing, and lack of proper safety equipment as primary contributors to these hazards, healthcare administrators should prioritize optimizing staffing levels, improving resource allocation, and ensuring the availability of necessary protective devices. Additionally, the significant role of rigid leadership and inequities in employee treatment suggests that fostering a more supportive and inclusive organizational culture could mitigate many of the risks associated with occupational hazards. Furthermore, the study’s emphasis on the need for better training and environmental safety programs highlights the importance of comprehensive safety education tailored to the specific challenges faced by radiology technologists. Addressing these issues through policy changes and targeted training initiatives could not only reduce the incidence of work-related injuries but also improve overall job satisfaction and performance among HCWs.
Additionally, the implications of this research extend beyond the immediate context of the study, calling for a broader examination of occupational hazards in healthcare settings in Saudi Arabia. Future research should consider a more extensive and diverse sample across multiple institutions to validate these findings and develop more generalized strategies for mitigating occupational risks in the healthcare industry. Finally, future research is encouraged to employ multivariate analysis techniques, such as multiple regression or factor analysis, to gain a deeper understanding of the interactions among demographic and occupational factors contributing to occupational hazards. Such methods could offer a more comprehensive perspective on the collective influence of multiple variables on hazard dimensions, enhancing the analytical depth of occupational health studies.
Conclusion
This study provides a comprehensive examination of the occupational hazards confronting radiology technologists at a leading tertiary hospital in Jeddah, Saudi Arabia. The findings reveal that the most significant contributors to these hazards are high workloads, work shifts, frequent interruptions, and patient-related factors, which collectively overshadow other elements like technologist-specific issues and organizational structure. A concerning 68.3% of participants identified rigid leadership styles and disparities in employee treatment as exacerbating factors, highlighting the critical impact of organizational dynamics on workplace safety. Additionally, the study uncovered that more than half of the respondents pointed to insufficient staffing and a lack of adequate radiation protective devices as key resource-related issues that heighten occupational risks. The demanding nature of the work, characterized by extended hours and physically taxing tasks, poses substantial challenges specific to radiology technologists. Moreover, the frequent interaction with infectious or emotionally unstable patients, alongside the constant pressure to avoid errors, further complicates the safety landscape for these professionals. In sum, this study highlights the urgent need for targeted interventions in staffing, resource allocation, and organizational culture to mitigate the occupational hazards faced by radiology technologists. The insights gained here serve as a foundation for developing strategies that prioritize the well-being and safety of HCWs in similar high-risk environments.
Data Sharing Statement
Data are available on reasonable request. To access data, researchers are welcome to contact the corresponding author.
Ethics Approval and Consent to Participate
The Ethics Committee of King Abdullah International Medical Research Center approved this study (IRB Approval Number: IRB/2292/23; Ethics Study Number: SP23J-137-08). This study was conducted without the support of any specific grants from funding agencies in the public, commercial, or not-for-profit sectors. The authors declare no conflict of interest associated with this study. Furthermore, we confirm that written informed consent was obtained from all participants in the study, adhering to the ethical principles outlined in the Declaration of Helsinki.
Acknowledgments
The authors are indebted to all radiology technologists who kindly agreed to participate in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of Interest in this work.
References
1. Gupta P. Environmental Health and Occupational Safety. CRC Press; 2024; doi:10.1201/9781003464785
2. Sorensen G, Sparer E, Williams JAR, et al. Measuring best practices for workplace safety, health, and well-being. J Occup Environ Med. 2018;60(5):430–439. doi:10.1097/jom.0000000000001286
3. Albander H. Biomedical signal and image processing. Biomed Sig Imag Process. 2021. doi:10.5772/intechopen.95061
4. Schulte PA, Delclos G, Felknor SA, Chosewood LC. Toward an expanded focus for occupational safety and health: a commentary. Int J Environ Res Public Heal. 2019;16(24):4946. doi:10.3390/ijerph16244946
5. Thirunavukkarasu A, Alrawaili KAH, Al-Hazmi AH, et al. Prevalence and risk factors of occupational health hazards among health care workers of Northern Saudi Arabia: a multicenter study. Int J Environ Res Public Heal. 2021;18(21):11489. doi:10.3390/ijerph182111489
6. Joseph B, Joseph M. The health of the healthcare workers. Indian J Occup Environ Med. 2016;20(2):71–72. doi:10.4103/0019-5278.197518
7. Rafique R, Sehar S, Afzal M. Health hazards at work place: application of WHO modal with literature review. Saudi J Nurs Heal Care. 2019;02(12):438–442. doi:10.36348/sjnhc.2019.v02i12.010
8. Mengistu DA, Tolera ST, Demmu YM. Worldwide prevalence of occupational exposure to needle stick injury among healthcare workers: a systematic review and meta-analysis. Can J Infect Dis Méd Microbiol. 2021;2021:9019534. doi:10.1155/2021/9019534
9. Albejaidi F, Nair KS. Building the health workforce: Saudi Arabia’s challenges in achieving Vision 2030. Int J Heal Plan Manag. 2019;34(4):e1405–e1416. doi:10.1002/hpm.2861
10. Forder AA. A brief history of infection control - past and present. S Afr Méd J Suid-Afr Tydskr vir Geneeskd. 2007;97(11):1161–1164.
11. Haque M, Sartelli M, McKimm J, Bakar MB. Health care-associated infections – an overview. Infect Drug Resist. 2018;11:2321–2333. doi:10.2147/idr.s177247
12. Ilyas F, Burbridge B, Babyn P. Health care–associated infections and the radiology department. J Méd Imaging Radiat Sci. 2019;50(4):596–606.e1. doi:10.1016/j.jmir.2019.07.011
13. Kubde D, Badge AK, Ugemuge S, Shahu S. Importance of hospital infection control. Cureus. 2023;15(12):e50931. doi:10.7759/cureus.50931
14. Ogenyi P, England A, Aliyu Y, et al. Occupational hazards among medical radiation workers. West Afr J Radiol. 2018;25(1):28. doi:10.4103/wajr.wajr_1_17
15. ICRP. The 2007 recommendations of the international commission on radiological protection. Ann ICRP. 2007;37(2):1.
16. Xiao C, He N, Liu Y, Wang Y, Liu Q. Research progress on biodosimeters of ionizing radiation damage. Radiat Med Prot. 2020;1(3):127–132. doi:10.1016/j.radmp.2020.06.002
17. Registry A for TS and D. ATSDR-Toxicological Profile for Ionizing Radiation. University of California, Irvine; 2002.
18. Amrenova A, Baudin C, Ostroumova E, Stephens J, Anderson R, Laurier D. Intergenerational effects of ionizing radiation: review of recent studies from human data (2018–2021). Int J Radiat Biol. 2024;1–11. doi:10.1080/09553002.2024.2309917
19. Henker H, Fox-Lewis S, Tep N, Vanna D, Pol S, Turner C. Healthcare workers’ perceptions of an organizational quality assurance program implemented in a resource-limited setting: a qualitative study. Heal Promot Perspect. 2018;8(3):179–186. doi:10.15171/hpp.2018.24
20. Weerdt CVD, Baratta R. Changes in working conditions for home healthcare workers and impacts on their work activity and on their emotions. Production. 2014;25(2):344–353. doi:10.1590/0103-6513.108412
21. McLinton SS, Loh MY, Dollard MF, Tuckey MMR, Idris MA, Morton S. Benchmarking working conditions for health and safety in the frontline healthcare industry: perspectives from Australia and Malaysia. J Adv Nurs. 2018;74(8):1851–1862. doi:10.1111/jan.13580
22. Khabour OF, Ali KHA, Mahallawi WH. Occupational infection and needle stick injury among clinical laboratory workers in Al-Madinah city, Saudi Arabia. J Occup Med Toxicol. 2018;13(1):15. doi:10.1186/s12995-018-0198-5
23. Hashmi A. Prevalence of needle-stick and sharps injuries among healthcare Workers, Najran, Saudi Arabia. Epidemiol Open Access. 2012;02(02). doi:10.4172/2161-1165.1000117
24. Ndejjo R, Musinguzi G, Yu X, et al. Occupational Health hazards among healthcare workers in Kampala, Uganda. J Environ Public Heal. 2015;2015:913741. doi:10.1155/2015/913741
25. Abdulmageed SS, Alabbassi F, Alradi M, Alghanaim N, Banjar S, Alnakhli M. Assessment of occupational exposure to sharp injuries among health care workers in King Abdulaziz University Hospital. Int J Community Med Public Heal. 2018;5(5):1756–1761. doi:10.18203/2394-6040.ijcmph20181434
26. Moore RM, Kaczmarek RG. Occupational hazards to health care workers: diverse, ill-defined, and not fully appreciated. Am J Infect Control. 1990;18(5):316–327. doi:10.1016/0196-6553(90)90231-g
27. Al-Hanawi MK, Khan SA, Al-Borie HM. Healthcare human resource development in Saudi Arabia: emerging challenges and opportunities—a critical review. Public Health Rev. 2019;40(1):1. doi:10.1186/s40985-019-0112-4
28. Senthil A, Anandh B, Jayachandran P, et al. Perception and prevalence of work-related health hazards among health care workers in public health facilities in southern India. Int J Occup Environ Heal. 2014;21(1):74–81. doi:10.1179/2049396714y.0000000096
29. Wilburn SQ, Eijkemans G. Preventing needlestick injuries among healthcare workers: a WHO-ICN collaboration. Int J Occup Environ Heal. 2013;10(4):451–456. doi:10.1179/oeh.2004.10.4.451
30. Alqithami MA, ALsadi A, Tashkandi M, Gaafar R. Identifying work-related injuries among healthcare workers in Makkah hospitals, Saudi Arabia: a cross-sectional study in 2024. Cureus. 2024;16(8):e67323. doi:10.7759/cureus.67323
31. Alfulayw KH, Al-Otaibi ST, Alqahtani HA. Factors associated with needlestick injuries among healthcare workers: implications for prevention. BMC Health Serv Res. 2021;21(1):1074. doi:10.1186/s12913-021-07110-y
32. Albeladi OA, Almudaraa S, Alqusibri AA, Alqerafi NM, Alsenani YS, Abd-Ellatif EE. Needle stick injuries among health care workers in AL-Madinah AL-munawara governmental hospitals in Saudi Arabia. Glob J Heal Sci. 2021;13(11):76. doi:10.5539/gjhs.v13n11p76
33. AlDakhil L, Yenugadhati N, Al-Seraihi O, Al-Zoughool M. Prevalence and associated factors for needlestick and sharp injuries (NSIs) among dental assistants in Jeddah, Saudi Arabia. Environ Heal Prev Med. 2019;24(1):60. doi:10.1186/s12199-019-0815-7
34. Alshamrani KM, Alkenawi AA, Kaifi RE, et al. The barriers, motives, perceptions, and attitudes toward research among radiology practitioners and interns in Saudi Arabia: a cross-sectional study. Front Med. 2023;10:1266285. doi:10.3389/fmed.2023.1266285
35. Alaamer AS. Radiography education and training in Saudi Arabia. Open J Radiol. 2012;2012(04):134–140. doi:10.4236/ojrad.2012.24025
36. Specialties SC for H. Saudi board of radiology technology and medical imaging; 2020. https://scfhs.org.sa/sites/default/files/2022-02/Radiology%20Technology%20%26%20MEDICAL%20IMAGING-%20editage%20final%201.pdf.
37. I R. Sample Size Calculator by Raosoft Inc. http://www.raosoft.com/samplesize.html.
38. McCrum-Gardner E. Sample size and power calculations made simple. Int J Ther Rehabilitation. 2010;17(1):10–14. doi:10.12968/ijtr.2010.17.1.45988
39. Rajan D. Personal and social perception of occupational hazards by health care workers: a study among radiographers. Bus Ethics Leadersh. 2018;2(4):46–63. doi:10.21272/bel.2(4).46-63.2018
40. Ikart EM. Survey questionnaire survey pretesting method: an evaluation of survey questionnaire via expert reviews technique. Asian J Soc Sci Stud. 2019;4(2):1. doi:10.20849/ajsss.v4i2.565
41. Morgado FFR, Meireles JFF, Neves CM, Amaral ACS, Ferreira MEC. Scale development: ten main limitations and recommendations to improve future research practices. Psicol Reflexão e Crítica. 2017;30(1):3. doi:10.1186/s41155-016-0057-1
42. Landsbergis PA. Occupational stress among health care workers: a test of the job demands‐control model. J Organ Behav. 1988;9(3):217–239. doi:10.1002/job.4030090303
43. AlDhaen E. Awareness of occupational health hazards and occupational stress among dental care professionals: evidence from the GCC region. Front Public Health. 2022;10:922748. doi:10.3389/fpubh.2022.922748
44. Hashemian SM, Triantis K. Production pressure and its relationship to safety: a systematic review and future directions. Saf Sci. 2023;159:106045. doi:10.1016/j.ssci.2022.106045
45. Fernandopulle N. To what extent does hierarchical leadership affect health care outcomes? Méd J Islam Repub Iran. 2021;35:117. doi:10.47176/mjiri.35.117
46. Sfantou DF, Laliotis A, Patelarou AE, Pistolla DS, Matalliotakis M, Patelarou E. Importance of leadership style towards quality of care measures in healthcare settings: a systematic review. Healthcare. 2017;5(4):73. doi:10.3390/healthcare5040073
47. Mehraein V, Visintin F, Pittino D. The dark side of leadership: a systematic review of creativity and innovation. Int J Manag Rev. 2023;25(4):740–767. doi:10.1111/ijmr.12334
48. Marenus MW, Marzec M, Chen W. Association of workplace culture of health and employee emotional wellbeing. Int J Environ Res Public Heal. 2022;19(19):12318. doi:10.3390/ijerph191912318
49. Sainz M, Moreno‐Bella E, Torres‐Vega LC. Perceived unequal and unfair workplaces trigger lower job satisfaction and lower workers’ dignity via organizational dehumanization and workers’ self‐objectification. Eur J Soc Psychol. 2023;53(5):921–938. doi:10.1002/ejsp.2944
50. Stamarski CS, Hing LSS. Gender inequalities in the workplace: the effects of organizational structures, processes, practices, and decision makers’ sexism. Front Psychol. 2015;6:1400. doi:10.3389/fpsyg.2015.01400
51. Hing LSS, Sakr N, Sorenson JB, Stamarski CS, Caniera K, Colaco C. Gender inequities in the workplace: a holistic review of organizational processes and practices. Hum Resour Manag Rev. 2023;33(3):100968. doi:10.1016/j.hrmr.2023.100968
52. Hoxha G, Simeli I, Theocharis D, Vasileiou A, Tsekouropoulos G. Sustainable healthcare quality and job satisfaction through organizational culture: approaches and outcomes. Sustainability. 2024;16(9):3603. doi:10.3390/su16093603
53. Gestal JJ. Occupational hazards in hospitals: accidents, radiation, exposure to noxious chemicals, drug addiction and psychic problems, and assault. Br J Ind Med. 1987;44(8):510. doi:10.1136/oem.44.8.510
54. Haiduven DJ, Simpkins SM, Phillips ES, Stevens DA. A survey of percutaneous/mucocutaneous injury reporting in a public teaching hospital. J Hosp Infect. 1999;41(2):151–154. doi:10.1016/s0195-6701(99)90053-1
55. Hoe VC, Urquhart DM, Kelsall HL, Zamri EN, Sim MR. Ergonomic interventions for preventing work‐related musculoskeletal disorders of the upper limb and neck among office workers. Cochrane Database Syst Rev. 2018;2018(10):CD008570. doi:10.1002/14651858.cd008570.pub3
56. Rucker LM, Sunell S. Ergonomic risk factors associated with clinical dentistry. J Calif Dent Assoc. 2002;30(2):139–148.
57. Manyisa ZM, Aswegen EJ. Factors affecting working conditions in public hospitals: a literature review. Int J Afr Nurs Sci. 2017;6:28–38. doi:10.1016/j.ijans.2017.02.002
58. Boal WL, Leiss JK, Sousa S, Lyden JT, Li J, Jagger J. The National study to prevent blood exposure in paramedics: exposure reporting. Am J Ind Med. 2008;51(3):213–222. doi:10.1002/ajim.20558
59. Lehto TU, Helenius HYM, Alaranta HT. Musculoskeletal symptoms of dentists assessed by a multidisciplinary approach. Comm Dent Oral Epidemiol. 1991;19(1):38–44. doi:10.1111/j.1600-0528.1991.tb00103.x
60. Berhane K, Kumie A, Samet J. Health effects of environmental exposures, occupational hazards and climate change in Ethiopia: synthesis of situational analysis, needs assessment and the way forward. Ethiop J Heal Dev Ya’Ityopya tena lemat mashet. 2016;30(1):50–56.
61. Ayenew E, Akafu W, Daka DW. Prevalence of work-related health hazard and associated factors among health workers in public health institutions of gambella town, Western Ethiopia: cross-sectional survey. J Environ Public Heal. 2022;2022(1):6224280. doi:10.1155/2022/6224280
62. Gimeno D, Felknor S, Burau KD, Delclos GL. Organisational and occupational risk factors associated with work related injuries among public hospital employees in Costa Rica. Occup Environ Med. 2005;62(5):337. doi:10.1136/oem.2004.014936
63. Rai R, El-Zaemey S, Dorji N, Rai BD, Fritschi L. Exposure to occupational hazards among health care workers in low- and middle-income countries: a scoping review. Int J Environ Res Public Heal. 2021;18(5):2603. doi:10.3390/ijerph18052603
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.