")
Back to Journals » Clinical Ophthalmology » Volume 18
Scheimpflug Tomography as a Predictor of Corneal Edema After Phacoemulsification in Fuchs Endothelial Corneal Dystrophy
Authors Eleiwa TK, Mohammed MAEA, Bayoumy ASM
Received 23 April 2024
Accepted for publication 8 August 2024
Published 19 August 2024 Volume 2024:18 Pages 2303—2311
DOI https://doi.org/10.2147/OPTH.S474788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Taher K Eleiwa,1,2 Mona Abd El-Azim Mohammed,3 Ahmed Sherin M Bayoumy1
1Department of Ophthalmology, Benha University, Benha, Egypt; 2Department of Ophthalmology, Magrabi Eye and Dental Hospital, Qassim, Kingdom of Saudi Arabia; 3Department of Ophthalmology, Mansoura Ophthalmic hospital, Mansoura, Egypt
Correspondence: Taher K Eleiwa, Email [email protected]
Purpose: To determine if Scheimpflug tomography pachymetry map and posterior elevation map patterns can predict the occurrence of corneal edema following uneventful phacoemulsification surgery in Fuchs endothelial corneal dystrophy (FECD).
Design: Observational prospective case–control study.
Participants: Fifty FECD eyes (50 patients) with visually significant cataract: 25 with subclinical corneal edema (SCE) versus 25 without SCE.
Methods: Preoperatively, FECD was clinically assessed, and only patients devoid of clinical corneal edema were enrolled. Utilizing the Mayo Clinic classification for subclinical corneal edema (SCE), eligible FECD eyes were stratified based on Scheimpflug imaging pachymetry map and posterior elevation map characteristics, including loss of regular isopachs, displacement of the cornea’s thinnest point, and the presence of posterior surface depression, into two groups: Group A representing FECD with SCE, and Group B: FECD without SCE. One week postoperatively, clinical and tomographic evaluation was performed. Regression analysis was conducted to evaluate predictors of corneal edema after uneventful phacoemulsification surgery in both groups.
Results: All patients were successfully imaged before and 1 week after surgery. Visual acuity was significantly improved in both groups (P < 0.001). No postoperative clinical edema was observed in Group B, while 23 (92%) had mild edema and 2 (8%) had moderate edema in Group A. Both groups showed a significant increase in postoperative central corneal thickness (CCT) and thinnest corneal thickness (TCT) (both P < 0.001). Compared to Group B, Group A showed a significant central flattening of the anterior corneal surface (P = 0.007 and P = 0.04 for K1 and K2 respectively), and a significant increase in the postoperative posterior surface depression. Multivariate analysis showed that 94% of postoperative corneal edema could be predicted by the presence of preoperative posterior surface depression (P = 0.04, ARR = 5.8 (1.89– 35.7)).
Conclusion: Scheimpflug tomography pachymetry map and posterior elevation map patterns can predict corneal edema after uneventful phacoemulsification surgery in FECD with subclinical corneal edema.
Keywords: phacoemulsification, cataract surgery, corneal edema, Scheimpflug tomography, pentacam, Fuchs endothelial corneal dystrophy
Introduction
Cataract surgery stands as the prevailing ocular procedure worldwide among adults aged 50 and above.1 Among the various complications that may occur following cataract surgery, corneal edema is frequently encountered. Post-phacoemulsification corneal edema can result from endothelial pump failure, which may be triggered by mechanical or chemical injury, subsequent infection or inflammation, or concurrent or pre-existing endothelial compromise.2
Fuchs endothelial corneal dystrophy (FECD) is described as a progressive bilateral asymmetric condition affecting the corneal endothelium. It is characterized by the loss of endothelial cells, disruption of the endothelial barrier, thickening of the Descemet’s membrane (DM), and the development of excrescences called guttae. These manifestations can lead to corneal edema and a decline in visual acuity.3 Currently, an estimated 300 million individuals aged 30 years and above are believed to have FECD worldwide, with projections indicating a rise to 415 million by 2050.4
Gradual corneal thickening progresses over time, often accompanied by a phase of subclinical edema, which refers to edema not readily apparent during slit-lamp biomicroscopy but may manifest symptoms such as glare and subjective visual haziness.5 While diagnosing FECD is typically straightforward through the detection of guttae via slit-lamp examination, identifying subclinical corneal edema poses more challenges. Awareness of this condition is crucial in general ophthalmology as patients may experience symptoms related to subclinical edema and require counseling regarding the potential progression of FECD, particularly in the context of cataract surgery.6
Prognostic indicators for FECD are currently lacking in clinical practice, often relying on subjective judgment. Decision-making for cataract surgery alone or combined with keratoplasty in FECD is challenging, with suggested methods like assessing central corneal thickness (CCT) and endothelial cell density being deemed misleading.5,7–9 Corneal backscatter cutoffs measured by confocal microscopy have been proposed but present challenges in clinical implementation.8
Patel et al introduced a Scheimpflug imaging classification for FECD, categorizing it into clinically obvious edema, subclinical corneal edema, or no edema independently of central corneal thickness (CCT). Their study identified specific tomographic patterns, including irregular isopachs, displacement of the cornea’s thinnest point, and focal posterior surface depression, associated with subclinical corneal edema in FECD. The classification recommends diagnosing FECD clinically with slit-lamp biomicroscopy, further refining it with Scheimpflug tomography when edema is not clinically evident.5
In this study, we utilized the Scheimpflug tomography to explore the potential of the aforementioned tomographic patterns in predicting corneal edema after uneventful phacoemulsification surgery in cataractous eyes with early FECD.
Methods
This was an observational prospective case–control study that was conducted on patients with early FECD who had visually significant cataract and underwent uneventful phacoemulsification surgery between November 2022 and November 2023. The study was approved by the Benha Faculty of Medicine Research Ethics Committee (MS 19-9-2021) and complied with the principles of declaration of Helsinki. Informed consent was taken from all patients prior to the study.
Study Participants
All patients were subjected to full ophthalmic evaluation. Visual acuity was recorded using logMAR unit. Each eye underwent slit-lamp examination conducted by a cornea specialist (T.K.E), and FECD eyes were graded clinically based on the following criteria: grade 1 represented non-confluent guttae; grade 2 indicated the presence of any area with confluent guttae but without evident clinical edema; grade 3 denoted confluent guttae accompanied by clinical edema; grade 4 signified edema coupled with whitening or haze.10 We only included grades 1 and 2 as early-stage FECD, while grades 3 and 4 were indicated for combined phacoemulsification and endothelial keratoplasty (EK), thus excluded from our study. Further, contact lens users, those with prior corneal surgeries (including keratorefractive procedures), corneal trauma, prior or current non-FECD corneal pathology, inflammatory ocular diseases, ocular surface diseases, glaucoma, systemic diseases with ocular involvement, or those using topical (except artificial tears) or systemic medications that could impact the cornea were excluded from our study.
Imaging
Before and one week after surgery, Scheimpflug tomography (Pentacam, software version 1.20r 112; Oculus, Wetzlar, Germany) was utilized to image patients, following procedures outlined elsewhere.11 Image acquisition occurred at any time within regular clinic hours (9:30 am to 12:30 pm). The “4 Maps Refractive” display, generated by the instrument’s software from enrolled eyes, was exported as a high-resolution image, following previously outlined methods;5 only images meeting the quality criteria of the instrument’s software were considered. De-identified images were randomly presented to a trained ophthalmology resident (M.A.M) and cornea specialist (T.K.E), blinded to patient outcomes, for independent evaluation of the tomography maps, assessing the loss of regular isopachs and the displacement of the thinnest point of the cornea, and focal posterior surface depression (Figure 1).
 |
Figure 1 Scheimpflug tomography pachymetry (left column) and posterior elevation (right column) maps of a 54-year-old female patient with early FECD and nuclear grade 2 cataract, preoperative (top row) and one week postoperative (bottom row). Pachymetry maps were assessed for irregular isopachs (red arrows), while posterior elevation maps were evaluated for negative elevation (black ovals) and displacement of the thinnest point (asterisk) relative to the pupil center. Preoperative tomography revealed subtle loss of regular isopachs and focal posterior surface depression. Postoperatively, marked loss of regular isopachs with diffuse posterior surface depression and nasal displacement of the thinnest location. |
Loss of regular isopachs was characterized by the absence of a nearly circular or oval shape or the lack of parallelism to adjacent isopachs within the central 4 mm of the cornea for any single line of equal thickness. We defined displacement of the thinnest point of the cornea as its position outside the inferotemporal quadrant, with reference to the pupil center, or if it extended beyond 1 mm from the pupil center in any quadrant.12 Focal posterior depression, indicating the posterior corneal surface protruding towards the anterior chamber, was defined as any isolated area showing negative elevation compared to the best-fit sphere within the central 4 mm of the cornea. Each characteristic was evaluated as either present or absent.5 According to preoperative tomography findings (Mayo Clinic subclinical corneal edema classification), eligible eyes were grouped into Group A: FECD with subclinical corneal edema (SCE), and Group B: FECD without SCE.
The sample size was calculated using G* power software version 3.1.9.2, based on a study by Abdelbary et al which reported a change in corneal thickness with an effect size of 0.957.13 Using t-tests for dependent means, with an effect size of 0.957, α error of 0.05, and power of 0.8, the required sample size was determined to be 11 cases. To account for dropouts or missed data, the sample size was increased to 50 cases.
Surgical Procedure
All 2.8-mm phacoemulsification procedures were conducted, using Geuder Megatron S4 (Germany) machine, by two experienced surgeons (T.K.E and A.S.B). The surgeries took place with patients’ eyes under peribulbar anesthesia, employing a standard dispersive-cohesive viscoelastic soft-shell technique, as previously outlined.14 Following surgery, 0.3% tobramycin and 0.1% dexamethasone eye drops were administered four times daily throughout the initial week and gradually tapered over the subsequent three weeks. At the second postoperative visit (postoperative day 7), patients’ corneas were clinically graded by the cornea specialist (T.K.E) and trained resident (M.A.M), blinded to the tomographic outcomes, as absent, mild (striate keratopathy or Descemet’s folds but iris details can be clearly seen), moderate (iris details partially seen through corneal edema) or severe (iris details cannot be seen) corneal edema. If disagreement found, a third masked cornea specialist (A.S.B) would be brought to assess. The follow-up Pentacam imaging was done at the same visit and analyzed as previously mentioned. In cases of postoperative corneal edema observed through slit-lamp examination, 50% compounded glycerin ophthalmic drops were utilized and continued until the patient reported improvement.
Statistical Analysis
Data analysis utilized SPSS software version 25 (SPSS Inc., PASW Statistics for Windows version 25, Chicago: SPSS Inc). Qualitative data were presented using numbers and percentages. For quantitative data, mean ± standard deviation (SD) was used to describe parametric data, while the median (range) was used for non-parametric data after assessing normality with the Kolmogorov-Smirnov test. Significance was determined at the ≤0.05 level, and Bonferroni correction method was used to adjust P values when multiple significance tests were conducted. For comparisons, Chi-Square and Monte Carlo tests assessed qualitative data between groups, and the McNemar test compared pre- and post-treatment. Wilcoxon-signed-rank test was used to compare two paired readings for non-normally distributed data within the same group and Mann–Whitney U-test to compare two studied groups with non-normally distributed data. Paired t-tests compared two paired readings for normally distributed data, and Student’s t-tests compared two studied groups with normally distributed data. The Spearman’s rank-order correlation gauged the strength and direction of a linear relationship between two non-normally distributed continuous or ordinal variables. Binary logistic regression, employing the Stepwise/Forward Wald/Enter technique, evaluated the impact of combinations of more than two independent variables on dichotomous outcomes.
Results
Our study included 25 FECD eyes with SCE (25 patients), versus age and gender-matched 25 FECD eyes without SCE (25 patients) who underwent uneventful phacoemulsification surgery and were successfully imaged perioperatively. A trend with higher age in the SCE-group was found, but age was adjusted for in the regression models. Differences in cumulative dissipated energy and ultrasound time during phacoemulsification between groups were not statistically significant. Table 1 summarizes demographics and baseline clinical characteristics of both groups. No disagreement was found between both observers regarding the perioperative tomographic evaluation in the studied eyes.
 |
Table 1 Demographic, Clinical and Tomographic Characteristics of the Studied Cases |
The visual acuity had significantly improved for FECD-SCE group and FECD without SCE group (P < 0.001, effect size = 4.25 and P < 0.001 with effect size = 3.64, respectively) (Table 2). Clinically, no postoperative corneal edema was observed in FECD without SCE group, while 23 (92%) had mild edema, and 2 (8%) had moderate edema in FECD-SCE group (P = 0.001). No disagreement was found in clinical evaluation of postoperative corneal edema. All cases with corneal edema had resolved with topical glycerin 50% every 8 hours by the third postoperative visit (14 ± 2.1 days).
 |
Table 2 Comparison Between Both Groups Regarding Pre- and Post-Operative Visual Acuity, Central and Thinnest Corneal Locations |
Compared to preoperative, there was a significant increase in CCT and TCT in both groups (both P < 0.001; Table 2), associated with significant central flattening of the anterior corneal surface only in FECD-SCE group (P = 0.07), compared to Group B (P = 0.55).
Table 3 illustrates the frequency of tomographic patterns in both groups pre- and post-operatively. No significant increase in the frequency of irregular isopachs and posterior surface depression was observed in both groups compared to the preoperative one (Figure 1). However, there was a statistically significant increase in the frequency of displacement of the thinnest point in FECD-SCE group compared to preoperatively (P = 0.008).
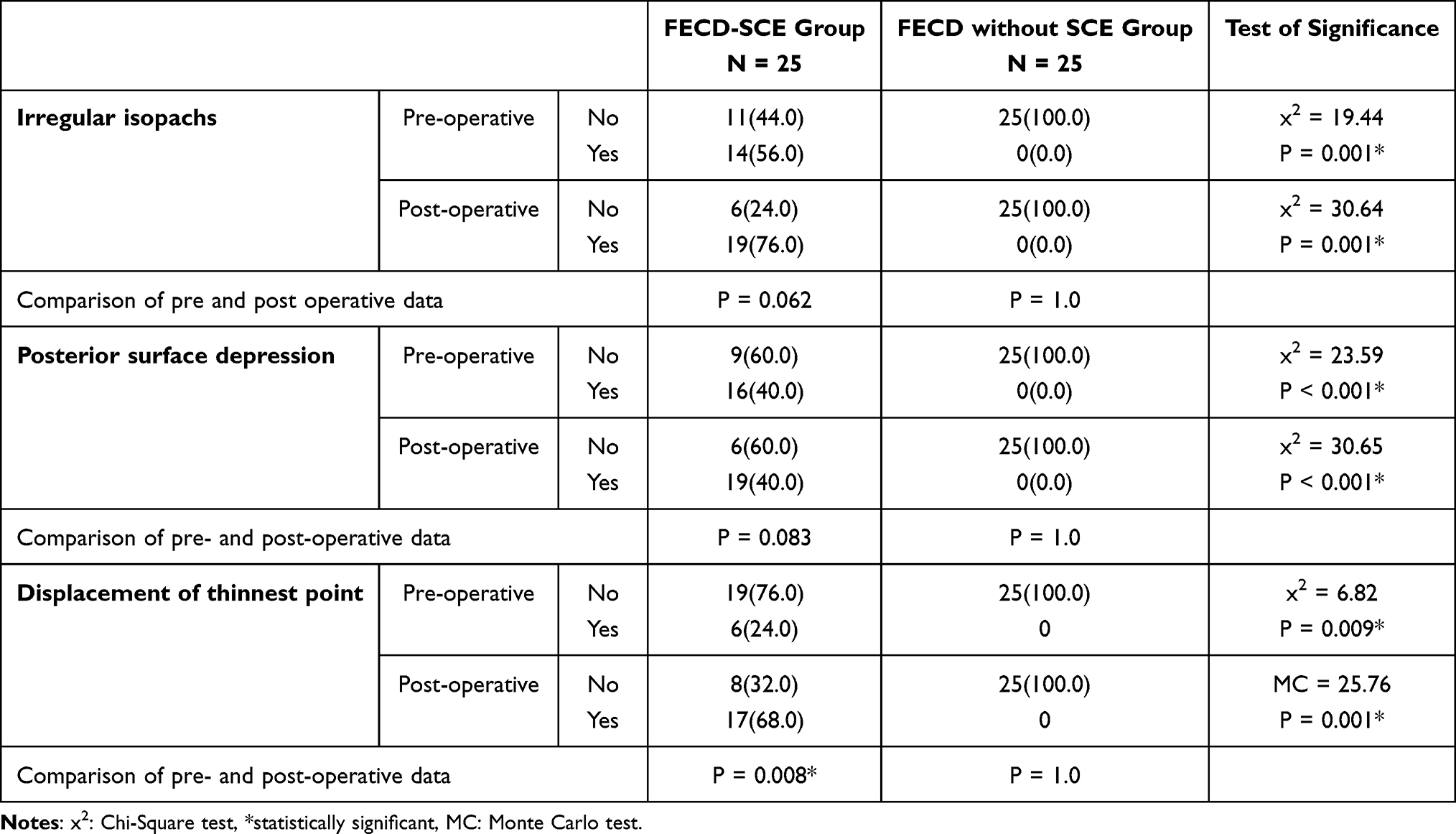 |
Table 3 Tomographic Patterns of the Studied Groups Pre- & Post-Operative |
Univariate analysis revealed that the loss of regular isopachs (P = 0.003, CRR: 16.0 (2.16–40.6)) and posterior surface depression (P = 0.036, CRR: 6.0 (1.96–37.4)) were significant predictors of postoperative corneal edema. However, multivariate analysis showed that 94% of postoperative corneal edema could be predicted by the presence of posterior surface depression alone (P = 0.04, ARR = 5.8 (1.89 −35.7)) (Table 4).
 |
Table 4 Univariate & Multivariate Regression Analysis for Predictors of Corneal Edema Among Studied Cases |
Discussion
Our study is the first to report using Scheimpflug tomography patterns to predict corneal edema after phacoemulsification surgery in early FECD. We revealed that while uneventful phacoemulsification surgery in both Fuchs endothelial corneal dystrophy (FECD) groups, with and without subclinical corneal edema (SCE), showed no significant differences in surgical parameters, distinct outcomes emerged postoperatively (Figure 1). Visual acuity significantly improved in both groups, in agreement with Viberg et al, who reported improved visual function in patients with cornea guttata after cataract surgery.15 However, corneal edema was notably absent in the FECD without SCE group. Conversely, the FECD-SCE group exhibited a high incidence of mild-to-moderate edema. Tomographic analysis demonstrated increased frequency of displacement of the thinnest point in the FECD-SCE group. Notably, posterior surface depression emerged as a significant predictor of postoperative corneal edema, contributing to 94% predictability. These findings underscore the importance of identifying specific tomographic patterns, particularly posterior surface depression, as potential predictors for postoperative outcomes in FECD patients, shedding light on crucial considerations for surgical decision-making and patient management strategies.
Endothelial imaging’s utility in assessing FECD severity is restricted, largely due to the interference caused by guttae,16 therefore considered not optimal for clinical-decision making.5 In the presence of guttae, not all endothelial cells are discernible for analysis. Confluent guttae obscure cell visibility entirely, necessitating specialized analysis methods that make assumptions based on the guttae-occupied image area to quantify cell density.16 Moreover, significant regional discrepancies in guttae distribution can lead to wide variations in cell density measurements within the same cornea, contingent upon the measurement method and location. Consequently, endothelial cell density may not consistently correlate with endothelial function.9 On the other hand, several studies had recently reported that corneal tomography may serve as an effective tool for objectively grading disease severity in FECD and aiding in surgical decision-making.5,6,9,17–19
In 2019, Sun et al studied 93 eyes with varying degrees of Fuchs endothelial corneal dystrophy (FECD) and 74 normal corneas. They aimed to evaluate Scheimpflug tomography’s ability to detect subclinical corneal edema in FECD and propose a new FECD classification. Three tomographic features—loss of regular isopachs, displacement of the thinnest corneal point, and posterior surface depression—were found in all FECD corneas with definite edema, over 81% of suspected subclinical edema cases, and less than 42% of non-edematous cases. Less than 5% of normal corneas showed these features. Corneas with suspected subclinical edema that underwent endothelial keratoplasty (EK) showed improvements post-EK, confirming preoperative subclinical edema.5
In 2020, Patel et al recommended evaluating pachymetry and posterior elevation maps in FECD when patients present with visual symptoms or are considering cataract surgery. This method is more clinically significant than measuring CCT alone, especially if prior FECD evaluation has not been done and corneal edema is not evident.6 They identified loss of regular isopachs, displacement of the thinnest point, and focal posterior surface depression as risk factors for FECD progression, whereas CCT was not.6 They also developed a predictive model for corneal improvement after Descemet membrane endothelial keratoplasty (DMEK) that outperformed preoperative CCT predictions, offering potential clinical and research applications.17
In a retrospective study of 115 eyes undergoing DMEK for FECD, Santana et al used Scheimpflug-derived parameters preoperatively and 6 months postoperatively to assess DMEK’s impact based on FECD severity and subclinical edema. Eyes without preoperative edema showed more parameters reversing to “normal” than those with subclinical edema.18 In a prospective study, Arnalich-Montiel et al established a risk prediction model for EK post-cataract surgery using Scheimpflug imaging. The risk for EK within two years significantly increased with more tomographic features.19 These studies support using Scheimpflug measurements to grade FECD and predict edema, aiding preoperative decisions.
One limitation of the study pertained to the utilization of the Pentacam system, which may not necessarily offer interchangeable predictions for corneal edema compared to other commonly employed systems. Consequently, further investigation into these variations is warranted. Additionally, the absence of a definitive standard for determining the necessity of topical hygroscopic agents posed another limitation. Nevertheless, our evaluation encompassed factors such as phacoemulsification time, intraoperative manipulations, and assessment of visual acuity. While our study was of short duration and small sample size, precluding definitive conclusions regarding the long-term effects of cataract surgery based on tomographic map features, most events within our cohort occurred within the initial 7 days. Although tomographic maps did not measure the influence of guttae on corneal edema prediction, the risk for corneal edema remained consistent across patients having tomographic features, including those with guttae but with subclinical edema, indicating a need for further investigation into this possibility.
In essence, our findings endorse the use of tomographic patterns for early identification of FECD eyes susceptible to corneal edema following uncomplicated cataract surgery, thereby optimizing visual outcomes. The widespread accessibility and straightforward interpretation of the Pentacam system make tomographic maps a valuable resource for clinicians in patient counseling, consent acquisition, and surgical planning, particularly in cases where corneal edema is not readily apparent. This predictive capability can be readily integrated into routine clinical practice, facilitating proactive measures to ensure postoperative corneal clarity or prompt referral to specialists in EK if necessary. External validation of our findings with longer-term follow-up is imperative for further validation.
Data Sharing Statement
All data generated or analyzed during this study are available upon request from the corresponding author.
Acknowledgment
We thank Dr. Hend Magdy, assistant professor of public health and biostatistics at Mansoura University, for conducting the statistical analysis.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Prokofyeva E, Wegener A, Zrenner E. Cataract prevalence and prevention in Europe: a literature review. Acta Ophthalmol. 2013;91(5):395–405. doi:10.1111/j.1755-3768.2012.02444.x
2. Sharma N, Singhal D, Nair S, et al. Corneal edema after phacoemulsification. Ind J Ophthalmol. 2017;65(12):1381. doi:10.4103/ijo.IJO_871_17
3. Rodrigues MM, Krachmer JH, Hackett J, et al. Fuchs’ corneal dystrophy: a clinicopathologic study of the variation in corneal edema. Ophthalmology. 1986;93(6):789–796. doi:10.1016/S0161-6420(86)33674-1
4. Aiello F, Gallo Afflitto G, Ceccarelli F, Cesareo M, Nucci C. Global prevalence of fuchs endothelial corneal dystrophy (FECD) in adult population: a systematic review and meta-analysis. J Ophthalmol. 2022;2022(1):3091695.
5. Sun SY, Wacker K, Baratz KH, et al. Determining subclinical edema in Fuchs endothelial corneal dystrophy: revised classification using Scheimpflug tomography for preoperative assessment. Ophthalmology. 2019;126(2):195–204. doi:10.1016/j.ophtha.2018.07.005
6. Patel SV, Hodge DO, Treichel EJ, et al. Predicting the prognosis of Fuchs endothelial corneal dystrophy by using Scheimpflug tomography. Ophthalmology. 2020;127(3):315–323. doi:10.1016/j.ophtha.2019.09.033
7. Seitzman GD, Gottsch JD, Stark WJ. Cataract surgery in patients with Fuchs’ corneal dystrophy: expanding recommendations for cataract surgery without simultaneous keratoplasty. Ophthalmology. 2005;112(3):441–446. doi:10.1016/j.ophtha.2004.10.044
8. van Cleynenbreugel H, Remeijer L, Hillenaar T. Cataract surgery in patients with Fuchs’ endothelial corneal dystrophy: when to consider a triple procedure. Ophthalmology. 2014;121(2):445–453. doi:10.1016/j.ophtha.2013.09.047
9. Patel SV. Towards clinical trials in Fuchs endothelial corneal dystrophy: classification and outcome measures—the Bowman Club Lecture 2019. BMJ Open Ophthalmol. 2019;4(1):e000321.
10. Adamis AP, Filatov V, Tripathi BJ, et al. Fuchs’ endothelial dystrophy of the cornea. Surv Ophthalmol. 1993;38(2):149–168. doi:10.1016/0039-6257(93)90099-S
11. Wacker K, McLaren JW, Amin SR, et al. Corneal high-order aberrations and backscatter in Fuchs’ endothelial corneal dystrophy. Ophthalmology. 2015;122(8):1645–1652. doi:10.1016/j.ophtha.2015.05.005
12. Liu Z, Huang AJ, Pflugfelder SC. Evaluation of corneal thickness and topography in normal eyes using the Orbscan corneal topography system. Br J Ophthalmol. 1999;83(7):774–778. doi:10.1136/bjo.83.7.774
13. Abdelbary R, Kamel R, Elkhouly S, El-Awady HE. Quantitative evaluation of corneal edema after phacoemulsification surgery using corneal densitometry. Egypt J Ophthalmol. 2022;2(2):99–110.
14. Arshinoff SA. Dispersive-cohesive viscoelastic soft shell technique. J Cataract Refract Surg. 1999;25(2):167–173. doi:10.1016/S0886-3350(99)80121-7
15. Viberg A, Liv P, Behndig A, et al. The impact of corneal guttata on the results of cataract surgery. J Cataract Refract Surg. 2019;45(6):803–809. doi:10.1016/j.jcrs.2018.12.023
16. McLaren JW, Bachman LA, Kane KM, et al. Objective assessment of the corneal endothelium in Fuchs’ endothelial dystrophy. Invest Ophthalmol Visual Sci. 2014;55(2):1184–1190. doi:10.1167/iovs.13-13041
17. Patel SV, Camp JJ, Hodge DO, et al. Predicting corneal improvement after Descemet membrane endothelial keratoplasty for Fuchs endothelial corneal dystrophy. Ophthalmol Sci. 2022;2(2):100128. doi:10.1016/j.xops.2022.100128
18. Santana SV, Vasiliauskaitė I, van Dijk K, et al. Impact of Fuchs Endothelial Corneal Dystrophy Severity on Scheimpflug-Derived Parameters After Descemet Membrane Endothelial Keratoplasty. Cornea. 2023;42(8):970–979. doi:10.1097/ICO.0000000000003115
19. Arnalich-Montiel F, de-Arriba-Palomero P, Muriel A, et al. A risk prediction model for endothelial keratoplasty after uncomplicated cataract surgery in Fuchs endothelial corneal dystrophy. Am J Ophthalmol. 2021;231:70–78. doi:10.1016/j.ajo.2021.04.016
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.