")
Back to Journals » Clinical Ophthalmology » Volume 19
Screening for Occult Macular Pathology Prior to Cataract Surgery Using Optical Coherence Tomography
Authors Fouad YA , ElGwaily AM , Shaaban YM
Received 2 December 2024
Accepted for publication 28 January 2025
Published 31 January 2025 Volume 2025:19 Pages 317—324
DOI https://doi.org/10.2147/OPTH.S507995
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Yousef A Fouad, Amr Mohamed ElGwaily, Yasmine Maher Shaaban
Department of Ophthalmology, Ain Shams University Hospitals, Cairo, Egypt
Correspondence: Yousef A Fouad, Department of Ophthalmology, Ain Shams University Hospitals, Ramses st., Abbassiya, Cairo, 11517, Egypt, Tel +201063781237, Email [email protected]
Purpose: To study the prevalence of occult macular pathology using optical coherence tomography (OCT) during the preoperative evaluation for cataract surgery and associated risk factors.
Methods: A retrospective analysis of patients’ medical records and imaging. Adult patients who underwent cataract extraction who had normal preoperative fundoscopic examination and available preoperative OCT imaging were included.
Results: The analysis included 121 eyes belonging to 121 patients. The prevalence of occult macular pathology was 21.5%, with the most common being interface abnormalities (8.3% of the eyes), drusen (4.1%), and diabetic macular edema (4.1%). Visually significant pathologies were noted in 6.6% of the eyes. Occult macular pathology was rare in patients aged less than 50 years (4.5%) and common among patients 70 years of age or older (43.3%). The most significant predictors of occult macular pathology were advanced age (OR: 1.06, p = 0.033) and diabetes mellitus (OR: 6.79, p = 0.002).
Conclusion: Relying on fundoscopic evaluation alone would miss 1 in 5 eyes with occult macular pathology and 1 in 15 with pathologies that would alter the visual outcome. Preoperative OCT screening prior to cataract surgery should be considered, especially in patients with advanced age and diabetes mellitus.
Keywords: cataract, macular, optical coherence tomography, preoperative assessment, imaging
Background
Cataract extraction is one of the most widespread surgical interventions performed across the globe,1 with increasing rates over the past years.2 A discrepancy exists between patients’ expectations and actual visual outcomes following cataract surgery.3 The two most common causes of suboptimal visual outcomes are refractive error and pre-existing ocular comorbidities.4 While advances in biometric technology and formulas, intraocular lens design, and microsurgical techniques have improved refractive outcomes over the years,5 underlying ocular comorbidities remain a challenge especially for low- and middle-income countries.4 Of those, retinal disorders and maculopathy represent the leading causes of postoperative visual impairment.6,7
A debate has been ongoing on the value of preoperative optical coherence tomography (OCT) for picking up macular pathology in eyes with apparently normal fundus examination.8–10 Although preoperative OCT seems cost-effective when multifocal intraocular lenses are used,11 its value for routine cataract surgery is not fully recognized. In a contemporary global survey of cataract surgery practice patterns, only half of the respondents reported using routine preoperative OCT prior to surgery.12
Studies have shown varying rates of occult macular pathology on OCT in cataract surgery candidates, ranging from 4% to 42%.8,9,13–19 A recent review on the topic has concluded that 1 in 10 eyes undergoing cataract surgery would have an occult macular pathology diagnosed using OCT, the most common being macular degeneration and interface abnormalities.20 However, not all occult macular pathology picked up on OCT would affect the visual outcome or require referral to the retina service,15 and it is important to make the distinction when conducting such screening studies. Further, analyzing the characteristics of patients with occult macular pathology would help in selecting high-risk patients who would benefit more from macular OCT screening.
The aim of this work was to add to the literature on the prevalence of occult macular pathology detected using OCT before cataract surgery in a lower-middle income setting, with a focus on visually significant pathology. We also aimed to analyze patient factors that predict an abnormal OCT to suggest screening priority.
Methods
This was a retrospective observational study conducted at the department of ophthalmology, Ain Shams University Hospitals, Cairo, Egypt. The study adhered to the terms of the Declaration of Helsinki and formal ethical approval was obtained from the local research ethics committee (Research Ethics Committee of the Faculty of Medicine, Ain Shams University, approval identification number: FMASU R274 /2024). Informed consent was waived by the committee owing to the retrospective nature of the study, and no identifying information was included in the analysis.
Routine preoperative evaluation for patients undergoing cataract surgery at the hospital includes initial assessment by residents, preoperative optical biometry, and clearance for surgery by two specialists after complete ophthalmological examination. Selective referral for OCT evaluation is only made when one or both specialists record or suspect a macular lesion on fundus biomicroscopy or if the cataract grade does not explain the reduction in visual acuity (VA). Selective referral for specular microscopy is made for patients above 70 years, cornea guttata on examination, or those with dense cataracts and expected high levels of delivered phacoemulsification energy.
Over the period of 22 months between January 2023 and September 2024, adult patients cleared for cataract surgery with a normal fundoscopic examination were offered a complimentary macular OCT evaluation. Patients who agreed underwent a raster scanning protocol with 21 B-scans centered over the fovea using a spectral-domain OCT machine (Optovue Avanti, Visionix, USA). The OCT B-scans were evaluated by two graders (YAF & YMS) for the presence of any pathology. Macular pathology was graded as altering or non-altering to the visual outcome. Examples of a non-altering pathology include small drusen or early epiretinal membrane (ERM), and examples of altering pathology include center-involved diabetic macular edema (DME) or exudative age-related macular degeneration (AMD). Patients with poor-quality scans that did not allow for analysis of the images were excluded from the study. If the patient underwent cataract surgery in both eyes, only the first eye was included in the analysis to avoid inter-eye correlation. The age of the patient and comorbidities were extracted from the medical records. Preoperative corrected Snellen VA was also extracted from the records and converted to the logarithm of the minimal angle of resolution (logMAR) format using standard conversion methods.21
Statistical analysis was conducted using the Statistical Package for the Social Sciences (SPSS version 25). Descriptive statistics were calculated as the mean, standard deviation and median for quantitative variables, and as percentages for categorical variables. Comparison between means was made using the Student’s t-test and comparison between rates was made using Chi-square test. A p-value less than 0.05 was considered significant. Logistic regression was used to calculate the odds ratio (OR) of significant variables for predicting macular pathology.
Results
The final analysis included 121 eyes belonging to 121 patients, more than half of them (71 patients, 58.7%) were females. The mean age of the patients was 60.7 years (standard deviation [SD]: 11.9 years) with an age range of 24 to 84 years. Less than half of the sample (55 patients, 45.5%) did not have a medical comorbidity. The most prevalent medical comorbidities were hypertension (52 patients, 43%) and diabetes mellitus (32 patients, 26.4%), followed by cardiovascular disease (8 patients, 6.6%), thyroid disease (3 patients, 2.5%) and chronic kidney disease (2 patients, 1.7%). The mean preoperative logMAR VA was 0.67 (SD: 0.26).
Twenty-six eyes had an occult macular pathology on OCT, resulting in a prevalence of 21.5%. The most common macular pathologies (Figure 1) were interface abnormalities (including ERM and vitreomacular traction syndrome) that were seen in 10 eyes (8.3%), drusen (5 eyes, 4.1%), and DME (5 eyes, 4.1%) which was non-center-involving in 3 eyes (2.5%) and center-involving in 2 eyes (1.7%). Photoreceptor disruption was noted in 2 eyes (1.7%), central serous chorioretinopathy was noted in 1 eye (0.8%, Figure 2), as was acquired vitelliform lesions, exudative AMD, and paracentral acute middle maculopathy (PAMM, Figure 2). Of note, the patient with PAMM was referred for urgent cardiovascular evaluation and was found to have a ruptured atherosclerotic plaque with showering emboli on the same side of the lesion. In 8 eyes (6.6%), the macular pathology altered the expected visual outcome.
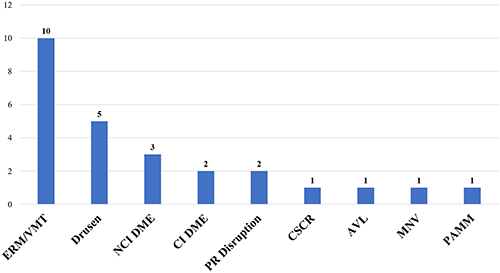 |
Figure 1 Distribution of occult macular pathology (x-axis) in the sample, y-axis represents number of eyes. Abbreviations: AVL, acquired vitelliform lesion; CI, center-involving; ERM, epiretinal membrane; MNV, macular neovascularization; NCI, non-center-involving; PR, photoreceptors; PAMM, paracentral acute middle maculopathy; VMT, vitreomacular traction. |
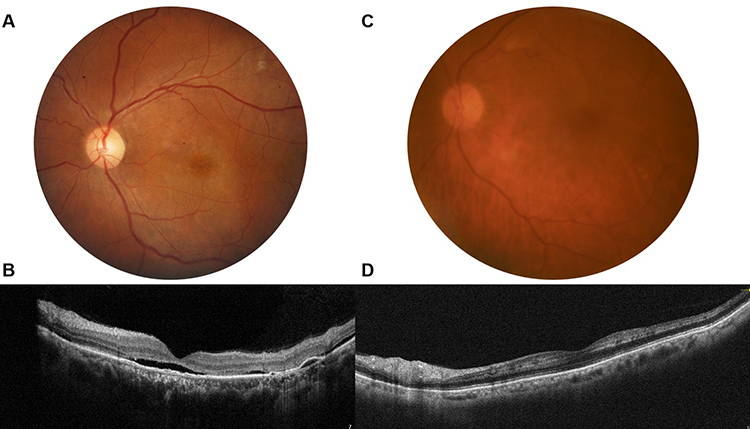 |
Figure 2 Examples of visually significant occult macular pathology. Left panel (A and B) depicts imaging of the left eye of a 59-year-old male patient with long-standing drop of vision (Snellen acuity: 6/24), nuclear and cortical cataract, and an unremarkable fundus photograph (A). Optical coherence tomography of the same eye (B) showed subfoveal fluid, photoreceptor attenuation, a pachychoroid, and a serous pigment epithelial detachment, consistent with a diagnosis of chronic central serous chorioretinopathy (the other eye had a similar appearance). Patient was referred for micropulse laser therapy. Right panel (C and D) depicts the left eye of a 62-year-old male patient with recent drop in vision (Snellen acuity: 6/60) in the left eye, grade II nuclear cataract and an unremarkable fundus photograph except for minor tessellations (C). Optical coherence tomography of the same eye (D) showed hyperreflective bands along the inner nuclear layer with a skip pattern, consistent with paracentral acute middle maculopathy. The patient was urgently referred for cardiovascular workup which revealed a showering atheroma in the left common carotid artery. |
Table 1 compares the characteristics of patients with occult macular pathology and those without. Patients with occult macular pathology were on average 10 years older than those without (mean ± SD = 68.2 ± 9 vs 58.7 ± 11.8 years, p < 0.001) and had a significantly worse logMAR VA (0.86 ± 0.22 vs 0.62 ± 0.24, p < 0.001). Only 1 of 22 patients (4.5%) who were younger than 50 years and 3 of 48 patients (6.2%) who were younger than 60 years had an occult macular pathology, while 13 of 30 patients (43.3%) who were older than 70 years had an occult macular pathology (p < 0.001). A significantly higher proportion of patients with occult macular pathology had a systemic comorbidity (p = 0.032) and diabetes mellitus (p < 0.001).
 |
Table 1 Comparison Between the Characteristics of Patients with and without Occult Macular Pathology (n = 121) |
A logistic regression equation was fitted with the following variables: age, sex, hypertension, diabetes, and logMAR VA. The results showed that the strongest predictor of occult macular pathology was diabetes mellitus, where patients with diabetes mellitus had on average 7 times the odds of occult macular pathology than those without (OR: 6.79 [95% CI: 1.96–23.5], p = 0.002). LogMAR VA was a significant predictor of occult macular pathology where each 0.1 increase in LogMAR VA was associated with 1.61 higher odds of having occult macular pathology (95% CI: 1.19–2.17, p = 0.002). Advanced age was also a significant predictor of occult macular pathology but at lower odds (OR: 1.06 [95% CI: 1.01–1.13], p = 0.033). Male sex and hypertension were not significant predictors of occult macular pathology (Table 2).
 |
Table 2 Multivariate Regression Analysis of the Predictive Patient Factors for Occult Macular Pathology |
Discussion
In this study, we found that relying on fundus examination alone during preoperative evaluation for cataract surgery would miss 1 in 5 eyes with occult macular pathology that are only visible on spectral-domain OCT. In approximately 1 in 15 eyes, the pathology would affect the visual outcome, requiring modification in the treatment plan or in patient counseling. Advanced age, poor preoperative visual acuity, and diabetes mellitus were the strongest predictors of occult macular pathology.
Starting in the last decade, multiple studies have reported on the utility of preoperative OCT in detecting occult macular pathology before cataract surgery (Table 3). Most such studies were conducted in high income8,14,17,22–24 or upper-middle income18,19,25,26 countries according to the latest World Bank classification.27 Only two studies9,13 were conducted in lower-middle income countries, the current study being the third. A recent systematic review and meta-analysis of cataract surgery outcomes by region found poorer visual outcomes in lower-middle income countries compared to high income countries, with ocular comorbidities being a major cause.4 While this highlights the greater need for OCT evaluation in the developing world, the extra requirement may also pose a burden on limited-resource healthcare systems. Cost-effectiveness analyses of the value of routine OCT screening prior to cataract surgery are needed in low- and middle-income settings.
 |
Table 3 Prior Studies in the Literature on Detecting Occult Macular Pathology Using Optical Coherence Tomography |
The prevalence of occult macular pathology varied across reports from as low as 4–5%8,16,26 to as high as 40–42%.14,15 This may be explained by several reasons. First, the definition of what constituted a macular pathology was not consistent across reports. For example, the study by Kowallick et al14 with the highest prevalence of occult macular pathology (42%) counted eyes with physiological vitreous alterations (eg, incomplete posterior vitreous detachment or vitreous opacities) as having an abnormal OCT, resulting in an overestimated prevalence. Second, the different spectral-domain OCT devices used across studies have different resolutions which may translate into variable sensitivity in detecting macular pathology.28 Third, a regional difference in the prevalence of ocular and systemic comorbidities that may underlie some of the macular pathologies (eg, DME29) may be contributory.
Only five studies8,14–17 highlighted the percentage of visually significant macular pathology which still varied from 0.8% to 26%. Again, the definition of what constitutes a visually significant pathology was not clear across reports. For example, small drusen (ageing changes) may require referral to the retina service for evaluation but would not affect the visual outcome of cataract surgery. In the Beaver Dam Eye Study, the prevalence of ERM in healthy subjects aged 60 or more years using spectral-domain OCT was 34%.30 Cost-effectiveness analysis would require the identification of pathologies that would alter the surgical decision, patient counseling and consent, or in which referral would have an impact on the patient’s systemic or ocular health.
The most commonly identified risk factor for occult macular pathology across reports was advanced age.16,18,24,26 This is consistent with our study in which the mean age of the patients with occult macular pathology was 10 years greater than those without and almost half of the patients aged 70 years or more had an occult macular pathology. On multivariate analysis, age was a significant predictor of occult macular pathology. Other risk factors reported in the literature included male gender,22 systemic hypertension,16,25 diabetes mellitus,25 smoking,22 cardiovascular disease,22 and myopia.25 However, most of the studies did not include a multivariate analysis to account for confounders. In our study, the prevalence of occult macular pathology did not significantly vary by gender, and only diabetes mellitus rather than hypertension was a significant predictor of occult macular pathology on multivariate analysis (nearly 7 times higher odds).
Limitations of the current study include the relatively small sample size. However, this is the first study from Egypt and one of the few from a lower-middle income setting to explore the subject. Another limitation is the unavailability of data on cataract grade as well as some risk factors such as smoking status and axial length which may introduce confounders to our analysis. Further studies with larger sample sizes exploring more variables are required to corroborate our findings.
In conclusion, our study highlights the importance of preoperative OCT screening for detecting occult macular pathology before cataract surgery. Relying on fundoscopic examination alone would miss 1 in 5 patients with occult pathology and 1 in 15 patients with visually significant pathology. If selective screening is to be considered, high risk groups seem to include those aged 70 years or older and those with systemic comorbidities, especially diabetes mellitus.
Abbreviations
AMD, age-related macular degeneration; AVL, acquired vitelliform lesion; CI, confidence interval; DME, diabetic macular edema; ERM, epiretinal membrane; LogMAR, logarithm of the minimum angle of resolution; MNV, macular neovascularization; OCT, optical coherence tomography; PAMM, paracentral acute middle maculopathy; SD, standard deviation; OR, odds ratio; PR, photoreceptors; VA, visual acuity, VMT, vitreomacular traction.
Acknowledgment
The authors would like to thank the residents at the department of ophthalmology, Ain Shams university hospitals, Cairo, Egypt, for their assistance with data acquisition.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McGhee CNJ, Zhang J, Patel DV. A perspective of contemporary cataract surgery: the most common surgical procedure in the world. J R Soc New Zeal. 2020;50(2):245–262. doi:10.1080/03036758.2020.1714673
2. Klein BEK, Howard KP, Lee KE, Klein R. Changing incidence of lens extraction over 20 years. Ophthalmology. 2014;121(1):5–9. doi:10.1016/j.ophtha.2013.06.006
3. Pager CK. Expectations and outcomes in cataract surgery. Arch Ophthalmol. 2004;122(12):1788. doi:10.1001/archopht.122.12.1788
4. Han X, Zhang J, Liu Z, et al. Real-world visual outcomes of cataract surgery based on population-based studies: a systematic review. Br J Ophthalmol. 2023;107(8):1056–1065. doi:10.1136/bjophthalmol-2021-320997
5. Khoramnia R, Auffarth G, Łabuz G, Pettit G, Suryakumar R. Refractive outcomes after cataract surgery. Diagnostics. 2022;12(2):243. doi:10.3390/diagnostics12020243
6. Salomão SR, Soares FS, Berezovsky A, et al. Prevalence and outcomes of cataract surgery in Brazil: the São Paulo Eye Study. Am J Ophthalmol. 2009;148(2):199–206.e2. doi:10.1016/j.ajo.2009.02.019
7. Shen W, Cun Q, Zhong H, Pan CW, Li J, Chen Q. Ethnic variation in prevalence, self-reported barriers and outcome of cataract surgery in a rural population in southwestern China: the Yunnan minority eye study. BMC Public Health. 2020;20(1):893. doi:10.1186/s12889-020-09009-5
8. Creese K, Ong D, Zamir E. Should macular optical coherence tomography be part of routine preoperative cataract assessment? Clin Experiment Ophthalmol. 2012;40(1):e118–e119. doi:10.1111/j.1442-9071.2011.02623.x
9. Sudhalkar A, Vasavada V, Bhojwani D, et al. Incorporating optical coherence tomography in the cataract preoperative armamentarium: additional need or additional burden? Am J Ophthalmol. 2019;198:209–214. doi:10.1016/j.ajo.2018.10.025
10. Goldhardt R, Rosen BS. Optical coherence tomography: critical tool to manage expectations after cataract extraction. Curr Ophthalmol Rep. 2020;8(3):129–135. doi:10.1007/s40135-020-00243-z
11. Leung EH, Gibbons A, Koch DD. Cost-effectiveness of preoperative OCT in cataract evaluation for multifocal intraocular lens. Ophthalmology. 2020;127(7):859–865. doi:10.1016/j.ophtha.2020.01.049
12. Rossi T, Romano MR, Iannetta D, et al. Cataract surgery practice patterns worldwide: a survey. BMJ Open Ophthalmol. 2021;6(1):e000464. doi:10.1136/bmjophth-2020-000464
13. Zafar S, Siddiqui MAR, Shahzad R, Shahzad MH. Swept-source optical coherence tomography to screen for macular pathology in eyes having routine cataract surgery. J Cataract Refract Surg. 2017;43(3):324–327. doi:10.1016/j.jcrs.2016.12.022
14. Kowallick A, Fischer CV, Hoerauf H. Optical coherence tomography findings in patients prior to cataract surgery regarded as unremarkable with ophthalmoscopy. PLoS One. 2018;13(12):e0208980. doi:10.1371/journal.pone.0208980
15. Weill Y, Hanhart J, Zadok D, Smadja D, Gelman E, Abulafia A. Patient management modifications in cataract surgery candidates following incorporation of routine preoperative macular optical coherence tomography. J Cataract Refract Surg. 2021;47(1):78–82. doi:10.1097/j.jcrs.0000000000000389
16. Alizadeh Y, Akbari M, Moghadam RS, Medghalchi A, Dourandeesh M, Bromandpoor F. Macular optical coherence tomography before cataract surgery. J Curr Ophthalmol. 2021;33(3):317–322. doi:10.4103/joco.joco_240_20
17. Herranz-Cabarcos A, Vega-López Z, Salas-Fandos O, et al. Macular optical coherence tomography for screening of pathology prior to cataract surgery: an approach based on tele-evaluation. Eur J Ophthalmol. 2022;32(6):3433–3437. doi:10.1177/11206721221080818
18. Dos Santos BB, Ribeiro Junior MDLB, Garcia NP, Colombo Barboza GN, Colombo Barboza MN. OCT to identify macular changes not clinically detectable in elderly patients with cataract. J Cataract Refract Surg. 2023;49(7):711–715. doi:10.1097/j.jcrs.0000000000001179
19. Icoz M, Gurturk Icoz SG. Importance of optical coherence tomography before cataract surgery. BMC Ophthalmol. 2024;24(1):339. doi:10.1186/s12886-024-03622-3
20. Ahmed TM, Siddiqui MAR, Hussain B. Optical coherence tomography as a diagnostic intervention before cataract surgery—a review. Eye. 2023;37(11):2176–2182. doi:10.1038/s41433-022-02320-y
21. Moussa G, Bassilious K, Mathews N. A novel excel sheet conversion tool from Snellen fraction to LogMAR including “counting fingers”, “hand movement”, “light perception” and “no light perception” and focused review of literature of low visual acuity reference values. Acta Ophthalmol. 2021;99(6):e963–e965. doi:10.1111/aos.14659
22. Klein BR, Brown EN, Casden RS. Preoperative macular spectral-domain optical coherence tomography in patients considering advanced-technology intraocular lenses for cataract surgery. J Cataract Refract Surg. 2016;42(4):537–541. doi:10.1016/j.jcrs.2016.01.036
23. Rein AP, Abulafia A, Zadok D, Hanhart J, Gelman E, Weill Y. The additive value of Foveal OCT-based biometry to fundus biomicroscopy for detecting macular pathology prior to cataract surgery. Am J Ophthalmol. 2021;228:8–15. doi:10.1016/j.ajo.2021.03.028
24. Murphy G, Owasil R, Kanavati S, Ashena Z, Nanavaty MA. Preoperative fundoscopy versus optical coherence tomography to detect occult maculopathy during cataract surgery preassessment. Eye. 2023;37(4):665–669. doi:10.1038/s41433-022-02027-0
25. Huang X, Zhang Z, Wang J, Meng X, Chen T, Wu Z. Macular assessment of preoperative optical coherence tomography in ageing Chinese undergoing routine cataract surgery. Sci Rep. 2018;8(1):5103. doi:10.1038/s41598-018-22807-7
26. Pinto WP, Rabello LP, Ventura MC, Rocha CS, Ventura BV. Prevalence of macular abnormalities identified only by optical coherence tomography in Brazilian patients with cataract. J Cataract Refract Surg. 2019;45(7):915–918. doi:10.1016/j.jcrs.2019.01.022
27. World Bank country classifications by income level for 2024-2025. World Bank Blogs. Published 2024. Available from: https://blogs.worldbank.org/en/opendata/world-bank-country-classifications-by-income-level-for-2024-2025.
28. Bahrami B, Ewe SYP, Hong T, et al. Influence of retinal pathology on the reliability of macular thickness measurement: a comparison between optical coherence tomography devices. Ophthalmic Surg Lasers Imaging Retina. 2017;48(4):319–325. doi:10.3928/23258160-20170329-06
29. Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis. 2015;2:17. doi:10.1186/s40662-015-0026-2
30. Meuer SM, Myers CE, Klein BEK, et al. The epidemiology of vitreoretinal interface abnormalities as detected by spectral-domain optical coherence tomography. Ophthalmology. 2015;122(4):787–795. doi:10.1016/j.ophtha.2014.10.014
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.