")
Back to Journals » Vascular Health and Risk Management » Volume 21
Self-Care Behavior Based on Knowledge of Patients with Hypertension: A Cross-Sectional Study
Authors Sari EA , Mirwanti R , Herliani YK , Pratiwi SH
Received 1 August 2024
Accepted for publication 22 November 2024
Published 15 January 2025 Volume 2025:21 Pages 17—24
DOI https://doi.org/10.2147/VHRM.S489688
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Harry Struijker-Boudier
Eka Afrima Sari,1 Ristina Mirwanti,2 Yusshy Kurnia Herliani,1 Sri Hartati Pratiwi1
1Medical and Surgical Nursing Department, Faculty of Nursing, Universitas Padjadjaran, Bandung, 45363, Indonesia; 2Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, 45363, Indonesia
Correspondence: Eka Afrima Sari, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +6281321440453, Email [email protected]
Background: Adequate self-care behavior is an important factor in controlling hypertension to reduce the number of complications. A patient’s knowledge about hypertension can influence their self-care behavior in practice.
Purpose: The aim of this study was to identify self-care behaviors among hypertension patients based on their knowledge.
Patients and Methods: This descriptive correlational study was conducted on patients with hypertension in primary care. The sample was selected using purposive sampling, with a one-month data collection period yielding 115 samples. The Hypertension Self-Care Profile instrument was used to assess self-care behavior while the Knowledge on Hypertension instrument was utilized to evaluate knowledge. The characteristics variable was analyzed using descriptive statistics, while the correlation between self-care behavior and knowledge was evaluated using spearman rank correlation.
Results: Most participants had favorable attitudes towards self-care (53%), and they had adequate knowledge about hypertension (53.9%). Patients with favorable behavior and adequate knowledge were 52.5%, while patients with unfavorable behavior and inadequate knowledge were 63.0%. This study found no significant association between self-care behavior and knowledge (p = 0.099, r = 0.155).
Conclusion: Despite most participants demonstrated favorable attitudes and adequate knowledge regarding hypertension self-care, a significant association between these variables was not identified. This suggests that knowledge alone may not be a sufficient predictor of self-care behavior in this population and further research is required to understand the complex factors influencing self-care adherence and develop effective interventions to improve patient outcomes.
Keywords: behavior, hypertension, knowledge, primary care, self-care
A Letter to the Editor has been published for this article.
Introduction
Hypertension is the leading cause of cardiovascular disease and premature death worldwide.1,2 Uncontrolled hypertension can lead to increased morbidity and mortality, as well as life-threatening complications.3 Hypertension cannot be cured, but it can be controlled. Self-care is one way to control hypertension. It can lead to better clinical outcomes, better blood pressure control, and fewer doctor visits, which can improve quality of life, prevent disability, reduce healthcare costs and reduce complication.4–6
Self-care refers to an individual’s ability to engage in activities that achieve, promote, and maintain optimal health.7 Self-care in patients with hypertension correlates with blood pressure control and the prevention of complications.8 Self-care for patients with hypertension includes adherence to treatment and lifestyle modifications,9 such as not smoking, weight management, a low-sodium and low-fat diet, physical activity, reducing alcohol consumption, monitoring blood pressure, visiting the doctor regularly, and reducing stress.10 The patients’ capacity to self-manage is associated with improved clinical outcomes, enhanced blood pressure regulation, decreased frequency of medical consultations, and lower prescription usage.11 Furthermore, improper self-care can lead to hospitalization. As many as 50% of people with hypertension who do not practice self-care will be hospitalized, whereas those who do practice self-care can avoid it.12 Self-care also reduces primary care visits.13
Self-care is an important factor for managing hypertension. A study among patients with hypertension found that self-care practices were unfavorable in rural areas in India.13 Another study in primary health care in southern Tunisia showed that patients with hypertension had a high total self-care practice score.4 Additionally, several studies indicate an average level of self-care behavior among patients with hypertension in healthcare centers in Khamir (Iran) and Malang (Indonesia).14,15 Studies in Malang and Padang (Indonesia) have shown significant differences in self-care behavior based on factors such as gender, level of education, ethnicity, marital status, and body mass index.15,16 These show that patients with hypertension had varying levels of self-care behavior and characteristics.
Self-care behaviors are essential for preventing and controlling hypertension.5,17 A patient’s understanding of hypertension can influence their self-care behavior.4 The patient’s comprehension of hypertension influences their motivation and behavior during self-care. The study found that patient with hypertension have various levels of self-care and knowledge.18 There is a significant relationship between knowledge and self-care.5,14,19 Elders with inadequate knowledge were less adherent to self-care behavior. Otherwise, another study showed that there is no significant relationship between knowledge and self-care behavior.18,20 Many studies on self-care behaviors and knowledge related to hypertension have been conducted in different countries and regions with varying results, but differences in socio-demographic, cultural, access, and health care infrastructure characteristics require further research in different places. Therefore, the aim of this study was to identify self-care behaviors and knowledge on hypertension among patients with the condition and examine the correlation between these two factors.
Materials and Methods
Study Design and Participants
A descriptive-correlational strategy was employed. Using purposive sampling, 115 patients with hypertension were selected from primary care settings. This sample size was obtained by collecting data for one month, as patients had primary care appointments every month. Inclusion criteria were: individuals aged 18 and older with a diagnosis of hypertension, who were currently on antihypertensive medication, and who were able to complete the questionnaire. Exclusion criteria included patients with acute or terminal conditions, psychiatric diagnoses, or any other condition that prevented participation in the study. Additionally, subjects experiencing unstable conditions, characterized by fluctuations in blood pressure, pulse, or respiration, were excluded.
Measurement
Data were collected using a questionnaire, which comprised three sections. The first section covered socio-demographic information developed by researchers, including gender, family history, level of education, length of time since diagnosis, age, and blood pressure. The second section assessed patients’ knowledge of hypertension using the Knowledge on Hypertension instrument developed by Eugene et al, using the Guttman scale.21 The final section employed the Hypertension Self-Care Profile instrument, developed by Han et al,10 to evaluate self-care techniques for controlling and monitoring hypertension using a Likert scale. The questionnaire was translated into Indonesian using the forward and backward translation method, adapted to Indonesian culture, and tested for relevance and reliability. The adaptation process involves adapting several questions to the Indonesian culture. To examine the tools’ content validity, the questionnaire was distributed to three experts in health education, chronic disease, and self-care, and their feedback was used to adjust the questionnaire based on Indonesian culture. Cronbach’s alpha was 0.919 in this study.
In this study, self-care behaviors encompass the use of medication and various lifestyle factors, including refraining from smoking, managing weight, adhering to a low-sodium and low-fat diet, engaging in physical activity, consuming alcohol in moderation, self-monitoring blood pressure, attending regular doctor’s appointments, and reducing stress. Knowledge on hypertension encompasses complications, regular check-ups, blood pressure monitoring, blood pressure level, and behaviors that influence blood pressure, such as smoking, alcohol consumption, physical exercise, and diet.
Data Collection
The researcher coordinated the data collection with authorized persons in primary care. Researchers engage in collaboration with on-duty nurses to identify participants according to established criteria. Participants received information regarding the purpose and procedure of data collection. The participants were informed of their rights and assured of data confidentiality. After signing a written informed consent, participants were given a questionnaire to complete. The completion time for the questionnaire was approximately 10 to 15 minutes. The completed questionnaires were returned to the researcher.
Statistical Analysis
The data was analyzed using descriptive and correlational statistics. Descriptive statistics were used to describe behavior and knowledge of the sample by using frequency, percentage, and median. Preliminary testing was done to meet the assumption of non-parametric testing before running the non-parametric tests. Spearman rank correlation parametric (ρ) was calculated to examine the relationship between self-care behaviors and knowledge of hypertension among patients with hypertension.
Ethical Considerations
This study was conducted according to the Declaration of Helsinki and has received ethical approval from the Padjadjaran University Research Ethics Committee with number 671/UN6.KEP/EC/2018. Patients were informed about the study and provided consent by signing an informed consent form. Participation in the study is voluntary, and participants can exit the process without any consequences. All information obtained was kept confidential and only used for academic purposes.
Results
Characteristic of Participant
In this study, the total number of participants was 115; the majority were women (79.1%). The mean age was 59.74 (SD ± 10.276) years; it ranged from 39 to 83 years, and most participants were within the age group of over 55 years (68.7%). Of the total, 50.4% had a family history of hypertension, and 49.6% had achieved high school or college education. Participants had hypertension for 2–5 years (43.5%); the mean was 6.65 (SD ±7.946) years. This study found that mean systolic and diastolic blood pressure of participants were 153.03 (SD ± 18.127) mmHg and 92.10 (SD ± 11.754) mmHg, respectively, and 83.5% of participants had stage 2 hypertension (Table 1).22
 |
Table 1 Sociodemographic Characteristic of Patients with Hypertension (n=115)22 |
Self-Care Behavior
Most participants exhibit favorable self-care behaviors (53%), with a median score of 49 (range: 34–62) (Table 2). Most of the participants demonstrating favorable behavior were women (54.95%), aged 65 years or older (61.54%), and had stage 2 hypertension (53.13%). Moreover, more than half of them had no family history of hypertension (56.14%), had hypertension for 6–10 years (57.14%), and had achieved secondary school education (59.26%) (Table 3).
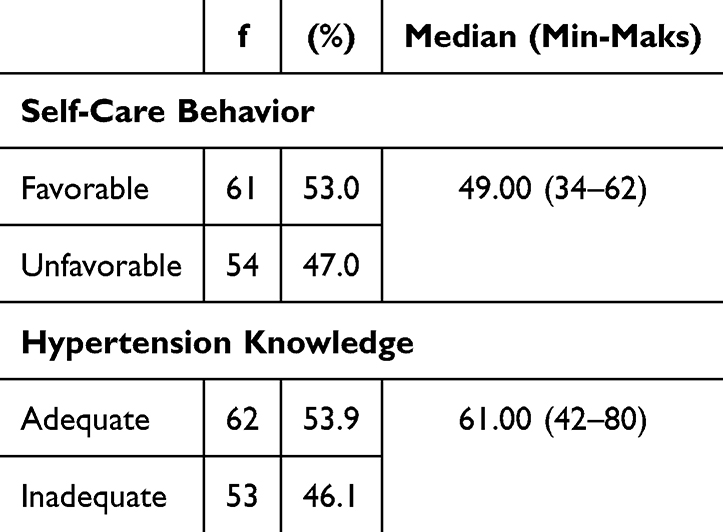 |
Table 2 Frequency, Percentage Level, and Median of Self-Care Behavior and Hypertension Knowledge Among Patients with Hypertension (n=115) |
 |
Table 3 Self-Care Behavior and Hypertension Knowledge According to Characteristics of Patients with Hypertension (n=115) |
Knowledge of Hypertension
The findings indicated that patients had a thorough understanding of hypertension. Most participants have adequate knowledge about hypertension (53.9%), with a median knowledge score of 61 (range 42–80) (Table 2). Adequate knowledge was found in men, aged 45–54 years, with secondary school education, family history of hypertension, diagnosis of hypertension for 6–10 years, and classification as stage 1 hypertension (Table 3).
Relationship Between Self-Care Behavior and Knowledge of Hypertension
In this study, participants had favorable behavior towards self-care (53%), and adequate knowledge about hypertension (53.9%) (Table 2). More than half of the participants with adequate hypertension knowledge were more likely to practice favorable self-care (52.5%). However, there was no significant association between knowledge and self-care behavior (p = 0.099, r = 0.155) (Table 4). Although most patients exhibited favorable behavior and had adequate knowledge, many still had stage 2 hypertension, indicating that self-care practices and disease management may need improvement. In particular, comprehensive education on both self-care practices and the rationale behind them is crucial to improving health outcomes.
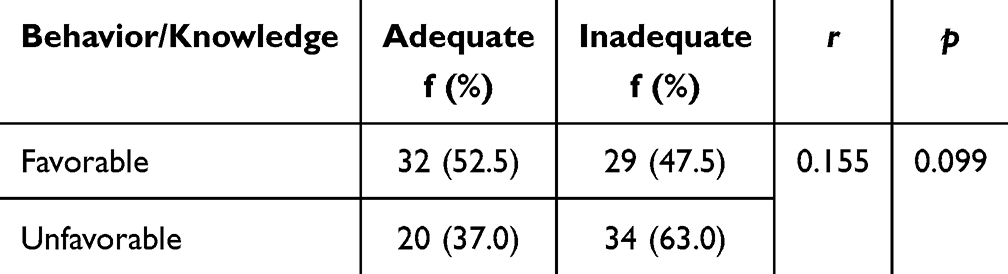 |
Table 4 Relationship Between Self-Care Behavior and Hypertension Knowledge of Patients with Hypertension (n=115) |
Discussion
In this study, more than half of the participants exhibited favorable behavior toward hypertension. This outcome surpasses previous research in the field.23 This favorable behavior was found in older people, and the duration of hypertension was over 6 years. These characteristics are similar to previous studies.24–27 Older patients tend to exhibit better self-care behavior, so they may be more conscious of the importance of managing their conditions and have more experience with self-care practices. A longer period of hypertension may have enhanced self-care abilities and a better understanding of their condition, which may influence their self-care behavior.25 Patients with a family history of hypertension also tend to have higher levels of self-care behavior,20 potentially due to prior knowledge and skills in managing the condition.28
Favorable behavior is also seen in individuals who frequently replace high-salt foods, limit their use of high-salt spices, consume less than 1 teaspoon of salt daily, limit their consumption of fat-containing foods, swap out high-fat foods for low-fat ones, limit their total calorie intake, refrain from smoking, consistently remember to take their medications and fill prescriptions, often maintain their weight, and avoid excessive stress. Unfavorable behavior can be seen from never exercising regularly, never reading nutritional labels to check salt and fat content, not controlling regularly, sometimes consuming fruits and vegetables daily, sometimes preferring frying over grilling or steaming, sometimes limiting the consumption of foods and drinks that contain alcohol, and never checking blood pressure outside the scheduled controls at the health center. Previous research aligns with these findings, showing that the lowest self-care score is for blood pressure monitoring,29 and that many never monitor their blood pressure at home.26,28 Contrary to this study, prior research indicates that the majority of patients with hypertension regularly use blood pressure monitors.30 Almost all participants who exhibited unfavorable behavior were women and had stage 2 hypertension. The majority had an education level above high school and were over 55 years old. Nearly half had been diagnosed with hypertension for 2 to 5 years.
More than half of the participants had adequate knowledge in this study; these results are consistent with previous studies.11,19,20,23 However, a study by Bacha and Abera found that patients with hypertension had inadequate knowledge about hypertension.23 In this study, patients under the age of 55 exhibited adequate knowledge, indicating they can easily process information at that age. This aligns with previous research showing poor knowledge in participants over 50 years old and excellent knowledge in those aged 36 to 45.19,23 Patients with a family history of hypertension already have experience with the condition. The study also highlights that the longer a patient has been diagnosed with hypertension, the more information they receive, with a substantial correlation between disease duration and knowledge.19 Higher education levels help patients easily receive information about hypertension. This study found that participants with high school and college education levels had sufficient knowledge about hypertension, consistent with previous research indicating that higher education levels correlate with better knowledge about hypertension.19,23
Patients have excellent knowledge about the importance of regular control for hypertension, including additional blood pressure measurements beyond the health center’s schedule. They understand that hypertension can cause complications, and smoking and drinking alcohol are risk factors. Patients are also well-informed about the benefits of exercise in reducing blood pressure and appropriate diets for hypertension. However, many remain unaware of whether their blood pressure is normal or rising. Knowledge is critical in shaping behavior. Beneficial knowledge leads to beneficial behavior. Previous studies showed that a significant relationship between knowledge and self-care behavior, possibly due to respondents having a thorough understanding of their illness.20 Higher education levels correlate with improved self-management and health-related quality of life.7,11,18,31 In contrast with this study, participants with adequate hypertension knowledge exhibited more positive self-care behaviors, although the knowledge variable did not have a statistically significant impact on self-care behavior. Similar to the previous study, patients who had good knowledge had a favorable attitude toward self-care32 and no significant relationship between knowledge and self-care behavior.20 This result may be due to the participants’ adequate knowledge of hypertension and self-care, as well as differences in the sociodemographic characteristics of the participants, the sample size, and the tools used. Despite the patients’ excellent knowledge and favorable behavior, many still had grade 2 hypertension, even while on medication, indicating suboptimal disease control.
Participants in this study ranged in age (the youngest was 39 years old and the oldest was 83 years old), making the results representative of all age groups. However, the range in age in this study might influence the relationship between knowledge and self-care. Older patients may face unique challenges in accessing and understanding health information,24 while younger patients may have different lifestyle habits and preferences for educational materials.18 Additionally, the effectiveness of self-care strategies, such as physical activity or dietary changes, may vary depending on age-related factors like physical limitations or metabolic differences. Therefore, assessing the challenges in performing self-care is necessary. Furthermore, comprehensive and repeated health education (which addresses both knowledge and practical self-care and is tailored to patients’ needs) and family support are needed to enhance understanding and improve self-care behavior.18,24,33
However, generalizing the findings has limitations. This study took place only in a primary care setting with a high rate of hypertension, which may not accurately represent all patients with hypertension. Additionally, the sample selection process may have introduced biases as patients with acute conditions or those unable to complete the questionnaire were excluded. Despite these limitations, the study provides valuable insights into the relationship between self-care behavior and hypertension knowledge among patients in this specific setting.
Conclusion
Although most participants demonstrated favorable attitudes toward self-care and possessed adequate knowledge, a significant association between these two factors was not established. This indicates that, although knowledge is significant, it may not be the single factor influencing self-care behavior in patients with hypertension. Further research is required to understand the complex factors influencing self-care adherence and develop effective interventions such as targeted educational programs, especially for those with inadequate knowledge.
Acknowledgments
We would like to acknowledge Universitas Padjadjaran for the financial support provided through the Universitas Padjadjaran Internal Research Grant program, under grant number 1093/UN6.L/PL/2018. Additionally, we would like to acknowledge the valuable contributions of the participants who took part in this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kemenkes RI. Hipertensi Si Pembunuh Senyap. InfoDATIN (Pusat Data dan Informasi Kementerian Kesehatan RI). Indonesian. 2019;1–5. Available from: https://pusdatin.kemkes.go.id/resources/download/pusdatin/infodatin/infodatin-hipertensi-si-pembunuh-senyap.pdf.
2. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–237. doi:10.1038/s41581-019-0244-2
3. Unger T, Borghi C, Charchar F, et al. 2020 international society of hypertension global hypertension practice guidelines. Hypertension. 2020;75(6):1334–1357. doi:10.1161/HYPERTENSIONAHA.120.15026
4. Ketata N, Ben Ayed H, Ben Hmida M, et al. Prevalence and predictors of hypertension self-care practice in primary health-care facilities in Southern Tunisia. JMV-J de Med Vasculaire. 2021;46(2):72–79. doi:10.1016/j.jdmv.2021.01.005
5. Niriayo YL, Ibrahim S, Kassa TD, et al. Practice and predictors of self-care behaviors among ambulatory patients with hypertension in Ethiopia. PLoS One. 2019;14(6):e0218947. doi:10.1371/journal.pone.0218947
6. Labata BG, Ahmed MB, Mekonen GF, Daba FB. Prevalence and predictors of self care practices among hypertensive patients at Jimma University Specialized Hospital, Southwest Ethiopia: cross-sectional study. BMC Res Notes. 2019;12(1). doi:10.1186/s13104-019-4125-3
7. Lee EJ, Park E. Self-care behavior and related factors in older patients with uncontrolled hypertension. Contemp Nurse. 2017;53(6):607–621. doi:10.1080/10376178.2017.1368401
8. Salim H, Lee PY, Sazlina SG, et al. The self-care profiles and its determinants among adults with hypertension in primary health care clinics in Selangor, Malaysia. PLoS One. 2019;14(11):1–14. doi:10.1371/journal.pone.0224649
9. Richard AA, Shea K. Delineation of self-care and associated concepts. J Nurs Scholarsh. 2011;43(3):255–264. doi:10.1111/j.1547-5069.2011.01404.x
10. Han HR, Lee H, Commodore-Mensah Y, Kim M. Development and validation of the hypertension self-care profile: a practical tool to measure hypertension self-care. J Cardiovasc Nurs. 2014;29(3):1–16.
11. Worku Kassahun C, Asasahegn A, Hagos D, et al. Knowledge on hypertension and self-care practice among adult hypertensive patients at University of Gondar Comprehensive Specialized Hospital, Ethiopia, 2019. Int J Hypertens. 2020;2020:1–7. doi:10.1155/2020/5649165
12. Navidian A, Yaghoubinia F, Ganjali A, Khoshsimaee S. The effect of self-care education on the awareness, attitude, and adherence to self- care behaviors in hospitalized patients due to heart failure with and without depression. PLoS One. 2015;10:1–13.
13. Dasgupta A, Sembiah S, Paul B, Ghosh A, Biswas B, Mallick N. Assessment of self-care practices among hypertensive patients: a clinic based study in rural area of Singur, West Bengal. Int J Community Med Public Health. 2017;5(1):262. doi:10.18203/2394-6040.ijcmph20175794
14. Eslamimehr F, Hosseini Z, Aghamolaei T, Nikparvar M, Ghanbarnejad A. Predictors of self-care behaviors in patients with hypertension: the integrated model of theories of “planned behavior” and “protection motivation. J Educ Health Promot. 2024;13(1). doi:10.4103/jehp.jehp_592_23
15. Dwi Kurnia A, Hariyati S, Melizza N, et al. Personal factors related to self-care management among people with hypertension at primary health care: a cross-sectional study OPEN ACCESS. Jurnal Keperawatan Padjadjaran. 2023;11(3):203–213. doi:10.24198/jkp.v11i3.2340
16. Sarfika R, Sulistiawati Afriyanti E, Yanuar Saifudin IMM, Saifudin IMMY. Self-care behavior among adult patients with hypertension in Padang, West Sumatra, Indonesia: a cross-sectional study. Belitung Nurs J. 2023;9(6):595–602. doi:10.33546/bnj.2915
17. Huy TQ, Nguyet NT, Nguyet NM, Van Truong P. Self-care behavior mediates the relationship between health literacy and blood pressure in older adults with hypertension. Bangladesh J Med Sci. 2024;23(2):476–483. doi:10.3329/bjms.v23i2.72176
18. Roxo MI, Guerra MM, Pepe B, et al. Arterial hypertension: do self-care and knowledge of the disease matter? 2024. Available from: https://academic.oup.com/ndt/article/39/Supplement_1/gfae069-1083-2869/7677537.
19. Bakhsh LA, Adas AA, Murad MA, et al. Awareness and knowledge on hypertension and its self- care practices among hypertensive patients in Saudi Arabia. Ann Int Med Dental Res. 2017;2(5). doi:10.21276/aimdr.2017.3.5.ME13
20. Pahria T, Nugroho C, Yani DI. Factors influencing self-care behaviors in hypertension patients with complications. Vasc Health Risk Manag. 2022;18:463–471. doi:10.2147/VHRM.S366811
21. Eugene V, Bourne P. Hypertensive patients: knowledge, Self-care management practices and challenges. J Behav Health. 2013;2(3):259. doi:10.5455/jbh.20130217103511
22. Sari EA, Pratiwi SH. Laporan aktivitas perawatan diri pasien hipertensi di kota bandung [Reports of self-care activities of patient’s with hypertension in Bandung City]. Malahayati Nurs J. 2022;5(2):300–307. doi:10.33024/mnj.v5i2.5885
23. Bacha D, Abera H. Knowledge, attitude and self-care practice towards control of hypertension among hypertensive patients on follow-up at st. paul’s hospital, Addis Ababa. Ethiop J Health Sci. 2019;29(4):421–430. doi:10.4314/ejhs.v29i4.2
24. Gusty R, Effendi N, Abdullah KL, Syafrita Y. Association between knowledge and self-care adherence among elderly hypertensive patient in dwelling community. Open Access Maced J Med Sci. 2022;10(E):206–212. doi:10.3889/oamjms.2022.8342
25. Azmiardi A, Widiyanto A, Atmojo JT, Anasulfalah H, Mubarok AS, Iswahyuni S. Hypertension self-care behavior and its associated factors among patients with hypertension. Indonesian J Med. 2023;8(3):249–257. doi:10.26911/theijmed.2023.08.03.02
26. AlHadlaq R, Swarelzahab M, AlSaad S, et al. Factors affecting self-management of hypertensive patients attending family medicine clinics in Riyadh, Saudi Arabia. J Family Med Prim Care. 2019;8(12):4003. doi:10.4103/jfmpc.jfmpc_752_19
27. Lee JE, Han HR, Song H, et al. Correlates of self-care behaviors for managing hypertension among Korean Americans: a questionnaire survey. Int J Nurs Stud. 2010;47(4):411–417. doi:10.1016/j.ijnurstu.2009.09.011
28. Hu H, Li G, Arao T. Prevalence rates of self-care behaviors and related factors in a rural hypertension population: a questionnaire survey. Int J Hypertens. 2013;2013:1–8. doi:10.1155/2013/526949
29. Kholisoh PN, Wati P, Nursiswati N, Sari EA. Self-care profile pada pasien hipertensi. Jurnal Keperawatan’Aisyiyah. Indonesian. 2024;11:23–24.
30. Chudek A, Owczarek AJ, Ficek J, Almgren-Rachtan A, Chudek J. Lower utilization of home blood pressure monitoring in younger, poorly educated hypertensive males–real-life data. Blood Press. 2020;29(2):95–102. doi:10.1080/08037051.2019.1684818
31. Harisa A, Arfan AF, Ramadhani WA, Pahruddin MNS, Yodang Y. Determinant of self-management in chronic non-communicable disease among elderly. J Holistic Nurs Sci. 2022;9(2):51–57. doi:10.31603/nursing.v9i2.7081
32. Tekle Gebreyohannes L, Dabi Wake A. Hypertension recommended self-care knowledge, attitude, practice and its predictors among hypertensive patients in Ethiopia: a cross-sectional study. J Cardiol Curr Res. 2024;17(4):92–100.
33. Sarrafzadegan N, Mansourian M, Alikhassi H, et al. Self-care behaviours and determinants associated with hypertension control in elderly patients. J Pat Care. 2021;7(3):1–8.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Self-Care in Patients with Non-Optimal Diabetes Management in Brazilian Rural Areas: A Mixed-Methods Study
Macedo JCL, Soares DA, de Carvalho VCHS, Cortes TBA, Mistro S, Kochergin CN, Rumel D, Oliveira MG
Patient Preference and Adherence 2022, 16:1831-1842
Published Date: 27 July 2022
Public Knowledge, Attitudes, and Practices Regarding the Use of Over-The-Counter (OTC) Analgesics in Indonesia: A Cross-Sectional Study
Sinuraya RK, Wulandari C, Amalia R, Puspitasari IM
Patient Preference and Adherence 2023, 17:2569-2578
Published Date: 17 October 2023
Understanding Public Knowledge and Behavior Regarding Antibiotic Use in Indonesia
Sinuraya RK, Wulandari C, Amalia R, Puspitasari IM
Infection and Drug Resistance 2023, 16:6833-6842
Published Date: 26 October 2023
Comprehensive Knowledge, Attitudes, Behaviors, and Associated Factors of HIV/AIDS in Gondar City Public Health Facilities Among HIV Testing and Counselling Service Users, Northwest Ethiopia, 2022; an Ordinal Logistic Regression Analysis
Terefe B, Techane MA, Assimamaw NT
HIV/AIDS - Research and Palliative Care 2023, 15:713-726
Published Date: 7 December 2023
Adherence Behaviors and Related Factors Among Elderly Hypertensive Patients in China: Evidence from the China Health and Retirement Longitudinal Study
Liu F, Chang H, Liu X
Patient Preference and Adherence 2023, 17:3539-3553
Published Date: 23 December 2023