")
Back to Journals » Journal of Inflammation Research » Volume 17
Sepsis-Induced Coagulopathy Score is Associated with an Increased Risk of New-Onset Atrial Fibrillation in Septic Patients: A Two-Centered Retrospective Study
Authors Li J, Wang S, Ma C, Ning N, Huang Y, Jiao M, Zhang J, Sun W , Li J, Zhao B, Mao E, Che Z, Gao C
Received 3 May 2024
Accepted for publication 19 August 2024
Published 30 August 2024 Volume 2024:17 Pages 5889—5899
DOI https://doi.org/10.2147/JIR.S467424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Juan Li,1,* Shu Wang,2,* Chaoping Ma,1,* Ning Ning,3,* Yingying Huang,1,4,* Min Jiao,1 Jiyuan Zhang,1 Wenwu Sun,3 Jiaoyan Li,3 Bing Zhao,3 Enqiang Mao,3 Zaiqian Che,3 Chengjin Gao1
1Department of Emergency, Xinhua Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200025, People’s Republic of China; 2Department of Intensive Care Medicine, Chongqing University Central Hospital, Chongqing Emergency Medical Center, Chongqing, 400016, People’s Republic of China; 3Departments of Emergency, Ruijin Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 200025, People’s Republic of China; 4Dementia Research Center, Macquarie University, Sydney, Australia
*These authors contributed equally to this work
Correspondence: Chengjin Gao, Department of Emergency, Xinhua Hospital, Shanghai Jiao Tong University School of Medicine, 1665 Kongjiang Road, Shanghai, People’s Republic of China, Email [email protected] Zaiqian Che, Departments of Emergency, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200025, People’s Republic of China, Email [email protected]
Purpose: New-onset atrial fibrillation (NOAF) and sepsis-induced coagulopathy (SIC) are severe complications in septic patients. However, the relationship between NOAF and SIC score has not been clearly defined. This study aims to investigate the association between SIC score and NOAF, as well as their effect on mortality in sepsis.
Patients and Methods: This study was a two-center retrospective analysis. Medical data were collected from patients diagnosed with sepsis. The patients were divided into NOAF and non-NOAF groups, and the SIC score was calculated for each group. Univariable and multivariable logistic regression analyses were performed to explore the relationship between the SIC score and NOAF, as well as their effects on mortality. The Kaplan-Meier curve was used to assess the survival rate.
Results: A total of 2,280 septic patients were included, with 132 (5.7%) suffering from NOAF. Multivariable logistic regression analyses indicated that age, gender, the Acute Physiology and Chronic Health Evaluation II score (APACHE II), heart rate, renal failure, stroke, chronic obstructive pulmonary disease (COPD), and the SIC score were independent risk factors for NOAF in sepsis. Moreover, NOAF was associated with an increased risk of in-hospital mortality, 28-day mortality, and 90-day mortality. These results were consistent across subgroup analyses.
Conclusion: The SIC score was an independent risk factor for NOAF in septic patients, and NOAF was an independent risk factor for predicting mortality.
Keywords: sepsis, sepsis-induced coagulopathy, new-onset atrial fibrillation, association, mortality
Introduction
New-onset atrial fibrillation (NOAF) is a commonly occurred arrhythmia in sepsis,1 with an incidence rate of nearly 10%.2 Several studies have suggested that NOAF in patients with severe sepsis contributes to severe complications, higher mortality, and longer hospitalization.3,4 Sepsis often triggers elevated inflammatory and coagulatory responses, which can subsequently lead to atrial fibrillation.5,6 Patients with atrial fibrillation have a higher risk of ischemic stroke due to coagulopathy, especially in severe sepsis.7
Coagulopathy is a relatively common complication of sepsis, leading to a poor prognosis.8,9 Septic patients with coagulopathy are more likely to suffer unfavorable prognosis. Therefore it is crucial to identify early coagulopathy in sepsis.10 The newly proposed sepsis-induced coagulopathy (SIC) score has been applied to diagnose sepsis coagulation dysfunction at an early stage.11 One study found that higher International Normalized Ratio (INR) is a risk factor for the occurrence of AF in critical patients.12 Research has shown that coagulopathy within 24 hours of ICU admission in sepsis is an independent risk factor for atrial fibrillation morbidity. The impact of atrial fibrillation on 90-day mortality varies with the severity of early coagulopathy.13 However the connection between NOAF and SIC score remains vaguely defined. The aim of this study was to explore the association between the SIC score and NOAF, and their effect on mortality in patients with sepsis. Thus, providing guidance for anticoagulant therapy in patients with new-onset atrial fibrillation associated with sepsis.
Materials and Methods
Patients
Adult septic patients were enrolled in this study. Exclusion criteria were individuals with congenital coagulation disorders, congenital heart diseases, valvular heart diseases, cardiac pacemaker implantation, coronary heart diseases, and hospitalization or died less than 72 hours from admission. Coagulation function and SIC scores were detected within 24 h after admission into the ICU. Patients with atrial fibrillation earlier than SIC score evaluation were excluded. NOAF was defined as atrial fibrillation that occurred during the hospital stay, excluding cases with a history of atrial fibrillation. Sepsis was diagnosed in accordance with the Third International Consensus Definitions for sepsis and septic shock: SOFA score ≥2 points consequent to the infection (Sepsis 3.0). Patients with septic shock were identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and serum lactate level greater than 2 mmol/L (>18 mg/dL) in the absence of hypovolemia within 24 h after admission to the ICU. The SIC score was evaluated with the factors of platelet count, prothrombin time, and SOFA score according to the International Thrombosis and Hemostasis Association (ISTH) Recommendations and Guidelines in 2019. The detailed scoring rules are shown in Table 1.
 |
Table 1 SIC Scoring Criteria |
Study Design
The data for this retrospective study were acquired from patients with sepsis admitted to the Emergency ward and ICU department of Xinhua Hospital and Ruijin hospital, affiliated with the Shanghai Jiao Tong University School of Medicine. All data were recorded by two authors in each center, one author was responsible for collating the data, and the other author was in charge of checking the data.
Statistical Analysis
Variables were classified as categorical or continuous. Categorical variables were described as frequencies with percentages and were tested with the Wilcoxon rank sum test or chi-squared test. Continuous variables with a normal distribution were expressed as the mean ± standard deviation (mean ± SD), while skewed distribution variables were expressed as medians with interquartile ranges (IQR). The independent samples t-test was applied in normal distribution data, and a nonparametric Wilcoxon rank sum test was applied to skewed distribution data. Univariable and multivariable logistic regression analyses were used to evaluate the independent risk factors for NOAF in sepsis and to evaluate the association between NOAF and the SIC score on mortality. Kaplan-Meier curves with Log rank tests were used to evaluate the survival rate. The statistical analyses were performed using SPSS version 26.0 and R statistical software version 3.2.4. A p-value of < 0.05 was considered statistically significant.
Results
Baseline Characteristics of Patients on Admission
In Figure 1, a total of 2280 patients with sepsis were included in this study, among whom 132(5.7%) had NOAF. In Table 2, the mean age of all the patients was 71 years old, and 62.6% were male. Patients in the NOAF group were older [80(72, 85) vs 70(61, 81); p<0.001], more likely to have congestive heart failure (23.5 vs 8.8%; p<0.001), septic shock (26.5 vs 12%; p<0.001), stroke (37.9 vs 18.9%; p<0.001), renal failure (39.4% vs 17.9%; p<0.001), and Chronic obstructive pulmonary disease (COPD) (12.1 vs 5.6%; p=0.002). Patients in the NOAF group have higher APACHE-II score [15(12, 21) vs 12(9, 17); p<0.001], higher SOFA score [5(3.25, 8) vs 5(3, 8); p=0.031], and higher SIC scores [3(3, 4) vs 3(2,4), p=0.006]. The in-hospital mortality (36.4 vs 21.1%, p<0.001), 28-day mortality (25.8 vs 14.4%, p<0.001) and 90-day mortality rates (33.3 vs 19.4%, p<0.001) was significantly higher in the NOAF group. In Table 3, a comparison was made between the hospital survival group and non-survival group of NOAF patients, and the results showed the latter showed a higher severity of illness with higher SOFA [5(3, 6) vs 8(6,11), p<0.001] and APACHE-II score [14(12, 20) vs 16(14, 26), p=0.008]. The results showed that age, respiratory rate (RR), Congestive heart failure, Liver failure, Septic shock, C-reactive protein (CRP), procalcitonin (PCT), prothrombin time (PT), fibrinogen (FIB) were associated with in hospital mortality in NOAF patients. And the SIC score in the non-survival patients were higher than the survival patients in NOAF patients [5(4, 6) vs 4(3, 5), p=0.023].
 |
Table 2 Baseline Characteristics of NOAF and Non-NOAF Group Patients |
 |
Table 3 Baseline Characteristics of the Survivors and Non-Survivors in NOAF Group Patients |
 |
Figure 1 Flow diagram of study patients. From January 2013 to October 2021, septic patients were assessed and 2280 patients were enrolled in the final analysis. |
Association Between the SIC Score and NOAF
In Supplementary Table 1, following factors with p value < 0.1 were included in the multiple logistic regression model: age, male, APACHEII score, heart rate, congestive heart failure, liver failure, renal failure, stroke, COPD, platelets, and SIC score. In Table 4, after adjusted for confounders, the results of multivariate logistic regression indicated that the SIC score (OR=1.211; 95% CI: 1.040–1.411; p=0.014) was an independent risk factor for NOAF. And some other factors included age (adjusted OR=1.051; 95% CI: 1.033–1.069; p<0.001), gender(adjusted OR=1.569; 95% CI: 1.040–2.367; p=0.032), APACHEII score (adjusted OR=1.030; 95% CI: 1.000–1.060; p=0.048), heart rate (adjusted OR=1.011; 95% CI: 1.002–1.021; p=0.019), renal failure (OR=2.242; 95% CI: 1.506–3.339; p<0.001), stroke (OR=1.669; 95% CI: 1.123–2.478; p=0.011), and COPD (OR=1.852; 95% CI: 1.029–3.333; p=0.040) were also associated with NOAF morbidity. The results revealed that the SIC score was an independent risk factor for NOAF morbidity. We performed univariable and multivariable logistic regression analysis of SIC score on mortality in new-onset atrial fibrillation patients (Supplementary Table 2). Results indicated that there is no significant correlation between SIC and mortality in NOAF patients.
 |
Table 4 Association of SIC Score and New-Onset Atrial Fibrillation(NOAF) in Univariable and Multivariable Logistic Regression Analysis |
Association Between NOAF and Mortality in Septic Patients
In Figure 2A and B, the Kaplan-Meier curve suggested that the 28-day and 90-day mortality in the NOAF group was remarkably higher than that in the non-NOAF group. In Table 5, after adjusted for confounders, the multivariable logistic regression analysis indicated that NOAF was an independent risk factor for in-hospital mortality (adjusted OR=1.646; 1.116–2.428; p=0.012), 28-day mortality (adjusted OR=1.605; 1.047–2.460; p=0.030) and 90-day mortality (adjusted OR=1.595; 1.071–2.376; p=0.022). In addition, to further testify the relationship between NOAF and in-hospital mortality, subgroup analyses were conducted based on age, gender, APACHEII score, SOFA score, septic shock, congestive heart failure, renal failure, hypertension, diabetes and stroke. In Figure 3, There is a significant relationship between NOAF and in-hospital mortality for both septic shock (OR = 1.716, 95% CI 1.041–2.828) and non-septic shock patients (OR=2.775, 95% CI 1.596–4.824), as well as for patients with hypertension and those without hypertension. The effect of NOAF on the in-hospital mortality was consistent in each subgroup. There was no significant interaction effect between NOAF and each stratification factor.
 |
Table 5 Univariable and Multivariable Logistic Regression Analysis of New-Onset Atrial Fibrillation (NOAF) on Mortality in Septic Patients |
 |
Figure 2 Kaplan–Meier curve of survival analysis in NOAF group and non-NOAF group. (A) Kaplan–Meier curve of 28-day survival analysis in NOAF group and non-NOAF group. (B) Kaplan–Meier curve of 90-day survival analysis in NOAF group and non-NOAF group. P value < 0.05 was considered statistically significant. |
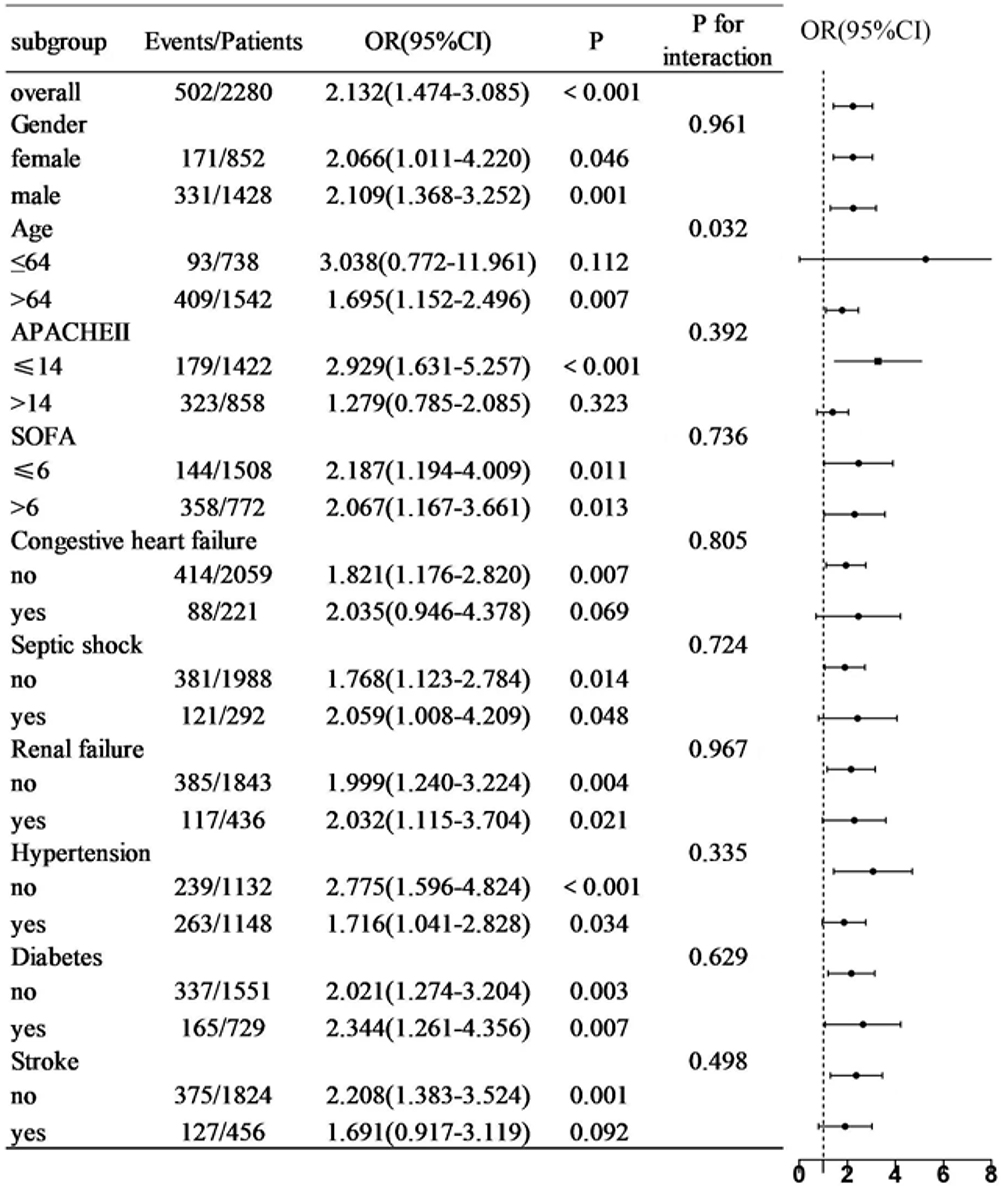 |
Figure 3 Subgroup analysis for the association of NOAF with in-hospital mortality. |
Discussion
This study is the first to report an association between the SIC score and NOAF, as well as their impact on mortality in sepsis. The major findings are that the SIC score is an independent risk factor for NOAF in septic patients, and NOAF is an independent risk factor to predict the in-hospital, 28-day and 90-day mortality.
Septic patients complicated with NOAF had worse prognosis, which has been reported in several previous studies.2,14 A multicenter retrospective cohort study found that sepsis with NOAF resulted in a longer ICU stay.14 Mik et al suggested that sepsis with NOAF is associated with adverse prognosis and higher mortality.2 Therefore, NOAF is a likely contributor to severe complications and a risk factor for mortality in sepsis. Our research confirmed that NOAF is an independent risk factor for in-hospital mortality, 28-day mortality and 90-day mortality. Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Recent studies have indicated that systemic inflammation is associated with a prothrombotic tendency by activating platelets and accelerating endothelial injury, which may contribute to atrial fibrillation.15 Inflammatory mediators are thought to promote arrhythmogenesis due to structural and contractile remodeling of the atria and endocardium.16 Consequently, sepsis induced atrial fibrosis creates an inflammatory substrate that trigger new-onset atrial fibrillation.17,18 Additionally, sepsis can lead to hypovolemia, which disrupts normal electrical conduction and initiates atrial fibrillation.5 Furthermore, atrial fibrillation often results in decreased cardiac output and congestive heart failure, further increasing mortality risk.19
Atrial fibrillation is associated with a hypercoagulable state, which can lead to thrombosis.20 However, it remains unclear if coagulopathy independently increases the risk of new-onset fibrillation in sepsis patients. Research shows that sepsis often leads to early coagulopathy, such as thrombocytopenia and prolonged clotting time.21 Activation of the coagulation system and subsequent thrombogenesis are common.22 The International Thrombosis and Hemostasis Association (ISTH) updated the SIC score to better identify coagulopathy in sepsis early by incorporating the SOFA score.11 Leukocyte accumulation, platelet activation, vascular endothelial cell injury, and coagulation factor activation play key roles in the mechanism of SIC.23 Vascular endothelial damage and fibrinolysis disorders are major causes of SIC, resulting in microvascular thrombosis, tissue ischemia, and hemorrhage, which contribute to hemodynamic disorders.24,25 Hemodynamic changes act as a substrate for the occurrence of sepsis. Therefore, the SIC score is associated with NOAF and our study finds that the SIC score is an independent risk factor for NOAF morbidity. However, our research indicates that there is no significant correlation between SIC and mortality in NOAF patients. This result may be due to the limited number of sepsis induced NOAF cases. Excessive inflammation activation and immune dysregulation contribute to SIC development, activating and consuming platelets and clotting factors, which can lead to microvascular thrombosis and bleeding.26 This disorder in microcirculation may cause multiple organ dysfunction, and studies suggest that coagulation processes are remarkably more active in atrial fibrillation patients.27 Therefore coagulation abnormalities are linked to atrial fibrillation in sepsis. Potential mechanisms include increased thrombin generation, changes in endothelial function, and inflammatory responses affecting cardiac tissue and rhythm.28–30
Disseminated intravascular coagulation is a severe complication of sepsis associated with high mortality.10 Therefore, early identification of coagulopathy in sepsis is crucial. In 2019, the International Society on Thrombosis and Hemostasis introduced new diagnostic systems to define SIC.11 To diagnose SIC, factors such as platelet count, PT ratio, and SOFA score should be considered. Several studies have explored the role of the SIC score in predicting sepsis mortality, assessing coagulation function in sepsis, and determining the optimal timing for anticoagulant therapy. However, no studies have investigated the utility of the SIC score in predicting the occurrence of NOAF in sepsis or its impact on mortality. Our study suggests that a higher the SIC score is associated with an increased risk of NOAF.
Currently, few models exist to forecast the occurrence of NOAF in sepsis. However, our study suggests that the SIC score may serve as a potential indicator for predicting NOAF, alongside other prediction indicators. Therefore, evaluating the SIC score could be crucial for the early identification of septic patients with NOAF, aiding in prompt diagnosis and treatment. Since both SIC and atrial fibrillation involve anticoagulant therapy, our research further elucidates the relationship between the SIC score and atrial fibrillation, offering guidance for anticoagulant therapy in sepsis patients.
This study has several limitations. First, this was a retrospective study that collected data from nine years. During this time, the definition and regulation of sepsis varied considerably and thus would be a confounding factor in sepsis mortality. Second, as this was a retrospective study, a certain degree of internal bias is inevitable Finally, this study was a two-center study, and the data is limited. A further multicenter prospective study will be needed to explore the association between the SIC score and new-onset atrial fibrillation and further evaluate the clinical efficacy of anticoagulant therapy in septic patients complicated with NOAF.
Conclusions
The SIC score was an independent risk factor for NOAF in patients with sepsis, and NOAF was an independent risk factor to predict the in-hospital, 28-day and 90-day mortality.
Data Sharing Statement
Data supporting the conclusions of this paper can be obtained from the article and its Supplementary Materials. Due to ethical restrictions, the raw data in this article cannot be made freely available, but scientific data (excluding individual data) supporting the findings of this study are available to be requested.
Ethics Statement
The protocol was approved by the institutional ethics board of Xinhua Hospital, Shanghai Jiao Tong University School of Medicine and Ruijin Hospital, Shanghai Jiao Tong University School of Medicine. The informed consent was waived because of the non-interventional, retrospective design of the study. Data analysis was performed in accordance with the 1964 Helsinki Declaration and its later amendments.
Acknowledgments
The authors would like to thank all the participants for their assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Medical Innovation Research Project of Shanghai Science and Technology Commission (No. 23Y31900102); Key Supporting Subject Researching Project of Shanghai Municipal Health Commission (No. 2023ZDFC0106); National Natural Science Foundation of China (No. 82172138) and Innovation Research Project of Shanghai Science and Technology Commission (No. 21Y11902400).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Aibar J, Schulman S. New-Onset Atrial Fibrillation in Sepsis: a Narrative Review. Semin Thromb Hemost. 2021;47(1):18–25. doi:10.1055/s-0040-1714400
2. Wetterslev M, Haase N, Hassager C, et al. New-onset atrial fibrillation in adult critically ill patients: a scoping review. Intens Care Med. 2019;45(7):928–938. doi:10.1007/s00134-019-05633-x
3. Moss TJ, Calland JF, Enfield KB, et al. New-Onset Atrial Fibrillation in the Critically Ill. Crit Care Med. 2017;45(5):790–797. doi:10.1097/CCM.0000000000002325
4. Kuipers S, Klein Klouwenberg PM, Cremer OL. Incidence, risk factors and outcomes of new-onset atrial fibrillation in patients with sepsis: a systematic review. Crit Care. 2014;18(6):688. doi:10.1186/s13054-014-0688-5
5. Bosch NA, Cimini J, Walkey AJ. Atrial Fibrillation in the ICU. Chest. 2018;154(6):1424–1434. doi:10.1016/j.chest.2018.03.040
6. Ruiz LA, Serrano L, España PP, et al. New-onset atrial fibrillation in patients with pneumococcal pneumonia. Impact of timing and duration on short- and medium-term mortality. J Infect. 2021;82(1):67–75. doi:10.1016/j.jinf.2020.11.005
7. Walkey AJ, Wiener RS, Ghobrial JM, Curtis LH, Benjamin EJ. Incident stroke and mortality associated with new-onset atrial fibrillation in patients hospitalized with severe sepsis. JAMA. 2011;306(20):2248–2254. doi:10.1001/jama.2011.1615
8. Jacobi J. The pathophysiology of sepsis-2021 update: part 1, immunology and coagulopathy leading to endothelial injury. Am J Health Syst Pharm. 2022;79(5):329–337. doi:10.1093/ajhp/zxab380
9. Giustozzi M, Ehrlinder H, Bongiovanni D, et al. Coagulopathy and sepsis: pathophysiology, clinical manifestations and treatment. Blood Rev. 2021;50:100864. doi:10.1016/j.blre.2021.100864
10. Iba T, Connors JM, Nagaoka I, Levy JH. Recent advances in the research and management of sepsis-associated DIC. Int J Hematol. 2021;113(1):24–33. doi:10.1007/s12185-020-03053-y
11. Iba T, Levy JH, Warkentin TE, Thachil J, van der Poll T, Levi M. Diagnosis and management of sepsis-induced coagulopathy and disseminated intravascular coagulation. J Thromb Haemost. 2019;17(11):1989–1994. doi:10.1111/jth.14578
12. Ortega-Martorell S, Olier I, Johnston BW, Welters ID. Sepsis-induced coagulopathy is associated with new episodes of atrial fibrillation in patients admitted to critical care in sinus rhythm. Front Med. 2023;10:1230854. doi:10.3389/fmed.2023.1230854
13. Long Y, Tong Y, Miao R, et al. Early Coagulation Disorder Is Associated With an Increased Risk of Atrial Fibrillation in Septic Patients. Front Cardiovasc Med. 2021;8:724942. doi:10.3389/fcvm.2021.724942
14. Fernando SM, Mathew R, Hibbert B, et al. New-onset atrial fibrillation and associated outcomes and resource use among critically ill adults-a multicenter retrospective cohort study. Crit Care. 2020;24(1):15. doi:10.1186/s13054-020-2730-0
15. Polovina MM, Lip GY, Potpara TS. Endothelial (dys)function in lone atrial fibrillation. Curr Pharm Des. 2015;21(5):622–645. doi:10.2174/1381612820666140825143028
16. Yang C, Wang X, Guo Y, et al. Beneficial Effect of Edoxaban on Preventing Atrial Fibrillation and Coagulation by Reducing Inflammation via HBG1/HBD Biomarkers. Front Pharmacol. 2022;13:904317. doi:10.3389/fphar.2022.904317
17. Guo Y, Lip GY, Apostolakis S. Inflammation in atrial fibrillation. J Am Coll Cardiol. 2012;60(22):2263–2270. doi:10.1016/j.jacc.2012.04.063
18. Hu YF, Chen YJ, Lin YJ, Chen SA. Inflammation and the pathogenesis of atrial fibrillation. Nat Rev Cardiol. 2015;12(4):230–243. doi:10.1038/nrcardio.2015.2
19. Reddy YNV, Obokata M, Verbrugge FH, Lin G, Borlaug BA. Atrial Dysfunction in Patients With Heart Failure With Preserved Ejection Fraction and Atrial Fibrillation. J Am Coll Cardiol. 2020;76(9):1051–1064. doi:10.1016/j.jacc.2020.07.009
20. Khan AA, Lip GYH. The prothrombotic state in atrial fibrillation: pathophysiological and management implications. Cardiovasc Res. 2019;115(1):31–45. doi:10.1093/cvr/cvy272
21. Lyons PG, Micek ST, Hampton N, Kollef MH. Sepsis-Associated Coagulopathy Severity Predicts Hospital Mortality. Crit Care Med. 2018;46(5):736–742. doi:10.1097/CCM.0000000000002997
22. Kato Y, Nishida O, Kuriyama N, et al. Effects of Thrombomodulin in Reducing Lethality and Suppressing Neutrophil Extracellular Trap Formation in the Lungs and Liver in a Lipopolysaccharide-Induced Murine Septic Shock Model. Int J Mol Sci. 2021;22(9):4933. doi:10.3390/ijms22094933
23. McDonald B, Davis RP, Kim SJ, et al. Platelets and neutrophil extracellular traps collaborate to promote intravascular coagulation during sepsis in mice. Blood. 2017;129(10):1357–1367. doi:10.1182/blood-2016-09-741298
24. Gando S. Role of fibrinolysis in sepsis. Semin Thromb Hemost. 2013;39(4):392–399. doi:10.1055/s-0033-1334140
25. Adelborg K, Larsen JB, Hvas AM. Disseminated intravascular coagulation: epidemiology, biomarkers, and management. Br J Haematol. 2021;192(5):803–818. doi:10.1111/bjh.17172
26. Bao W, Xing H, Cao S, et al. Neutrophils restrain sepsis associated coagulopathy via extracellular vesicles carrying superoxide dismutase 2 in a murine model of lipopolysaccharide induced sepsis. Nat Commun. 2022;13(1):4583. doi:10.1038/s41467-022-32325-w
27. Weymann A, Sabashnikov A, Ali-Hasan-Al-Saegh S, et al. Predictive Role of Coagulation, Fibrinolytic, and Endothelial Markers in Patients with Atrial Fibrillation, Stroke, and Thromboembolism: a Meta-Analysis, Meta-Regression, and Systematic Review. Med Sci Monit Basic Res. 2017;23:97–140. doi:10.12659/MSMBR.902558
28. Elias A, Khoury Y, Shehadeh F, et al. Elevated thrombin generation levels in the left atrial appendage in patients with atrial fibrillation. Res Pract Thromb Haemost. 2023;7(2):100127. doi:10.1016/j.rpth.2023.100127
29. Black N, Mohammad F, Saraf K, Morris G. Endothelial function and atrial fibrillation: a missing piece of the puzzle? J Cardiovasc Electrophysiol. 2022;33(1):109–116. doi:10.1111/jce.15277
30. Yao C, Veleva T, Scott L Jr, et al. Enhanced Cardiomyocyte NLRP3 Inflammasome Signaling Promotes Atrial Fibrillation. Circulation. 2018;138(20):2227–2242. doi:10.1161/CIRCULATIONAHA.118.035202
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.