")
Back to Journals » Clinical Ophthalmology » Volume 19
Short-Term Outcomes Using a Novel Femtosecond Laser-Assisted Keratotomy Nomogram to Manage Corneal Astigmatism During Phacoemulsification
Authors Truong N, Ernst B, Mishra G, Seeger C, Sun A, Longenecker A, Lehman E, Pantanelli SM
Received 23 October 2024
Accepted for publication 23 October 2024
Published 27 February 2025 Volume 2025:19 Pages 721—731
DOI https://doi.org/10.2147/OPTH.S500884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Nguyen Truong,1 Brett Ernst,2 Gautam Mishra,2 Catherine Seeger,3 Ashley Sun,1 Amy Longenecker,1 Erik Lehman,4 Seth M Pantanelli1
1Department of Ophthalmology, Penn State College of Medicine, Hershey, PA, USA; 2Schein Ernst Mishra Eye, Harrisburg, PA, USA; 3Department of Ophthalmology, Jacobs School of Medicine & Biomedical Sciences, Buffalo, NY, USA; 4Department of Public Health Sciences, Penn State College of Medicine, Hershey, PA, USA
Correspondence: Seth M Pantanelli, Department of Ophthalmology, Penn State College of Medicine, 500 University Drive, HU19, Hershey, PA, 17033-0850, USA, Tel +1717-531-8783, Fax +1717-531-5475, Email [email protected]
Purpose: To evaluate the efficacy of a femtosecond laser assisted astigmatic keratotomy (AK) nomogram (FemtoAK.com) for correction of astigmatism during cataract surgery.
Patients and Methods: Consecutive patients underwent cataract extraction with AKs and insertion of a non-toric intraocular lens. Eyes with greater than 0.5 D of against-the-rule (ATR) or 1.0 D of with-the-rule (WTR) or oblique (OBL) astigmatism were treated in accordance with the nomogram. Optical biometry and manifest refraction were checked pre- and one-month post-operatively. Outcome measures included correction index (CI), index of success (IOS), and proportion of eyes with less than 0.5 and 1.0 D of astigmatism.
Results: Ninety-five eyes from 69 patients were included, of which 41 had ATR, 35 had WTR, and 19 had OBL astigmatism. Corneal CI (ATR = 0.86, WTR = 0.27) indicated a small and large under-correction of ATR and WTR astigmatism, respectively, while refractive CI revealed a near-ideal correction of WTR (ATR = 0.87, WTR = 1.02). The proportion of eyes with less than 0.5 and 1.0 D of refractive astigmatism increased from 28% and 54% pre-operatively to 56% and 92% post-operatively, respectively.
Conclusion: The FemtoAK nomogram is effective at reducing corneal astigmatism at the time of cataract surgery. Astigmatic correction was more precise when evaluated by refractive rather than corneal measures.
Keywords: arcuate incisions, astigmatism, FemtoAK, femtosecond laser, keratotomy
Introduction
Modern cataract surgery not only aims to replace the cloudy lens with an artificial one but additionally seeks to minimize postoperative refractive error. In fact, astigmatism (not myopia or hyperopia) is the most common refractive error, with 40–60% of eyes having ≥0.5 D.1,2 Two methods can be used to correct astigmatism at the time of surgery: toric intraocular lenses (IOLs) and astigmatic keratotomies (AKs). While toric IOLs are considered the most accurate, they have limitations, including being relatively contraindicated in cases of zonulopathy, having the risk of misalignment and need for re-operation, and being available in specified step sizes that begin as low as 1.25 D in the United States.3,4
Historically, manual AKs were used for treatment of all astigmatisms. However, manual AKs may be associated with complications such as corneal perforation and induction of irregular astigmatism.5 To the contrary, femtosecond laser assisted keratotomies (FLAKs) create incisions of precise position, size, length, and depth and are most often indicated nowadays for treatment of low-to-moderate astigmatism.6
With FLAKs, surgeons rely on nomograms that advise on the positioning, length, and depth of the incisions. Even though femtosecond lasers have been available for more than a decade, most current nomograms are still derived from modified versions of the old nomograms developed for manual AKs. One previous study by Wendelstein and Hoffman et al assessed the Castrop nomogram for low-to-moderate astigmatism correction in 43 eyes but had a relatively small sample size and did not differentiate treatment of ATR, WTR, and OBL astigmatisms, which are known to be variably impacted by the posterior cornea.7 Another study by Wortz et al evaluated outcomes of astigmatism management in 224 patients with low corneal astigmatism (< 1.0 D). However, their nomogram has several constraints – namely that it requires the cataract surgeon’s main incision to be located temporally and does not offer recommendations for levels of astigmatism >1.25 D.
The purpose of this study was to prospectively evaluate the efficacy of a new FLAKs nomogram (FemtoAK.com) for the correction of astigmatism at the time of cataract surgery.
Patients and Methods
This was a prospective, single-center, assessor-masked clinical trial. The protocol and study specific informed consent was approved by the Penn State College of Medicine Institutional Review Board before enrollment of any subjects. The study was registered on clinicaltrails.gov (NCT04676451) and was performed in compliance with the tenets of the Declaration of Helsinki. Consecutive patients who underwent cataract evaluation between April 2019 and September 2023 at Schein Ernst Mishra Eye (Harrisburg, PA) and met inclusion/exclusion criteria were offered enrollment in the study at the time of initial cataract evaluation. Due to the pandemic and post-pandemic related staffing shortages, no patients were enrolled between June 2021 and January 2023.
Eligible subjects included patients 22 years or older, net keratometric astigmatism equal to or greater than 0.5 D of against-the-rule (ATR; 0–30° or 150–180°) or 1.0 D of with-the-rule (WTR; 60–120°) or oblique (OBL; 30–60° or 120–150°) astigmatism as measured by an optical biometer (IOLMaster 700, Carl Zeiss Meditec, Jena, GERMANY), at least one eye for which cataract extraction with monofocal or non-toric multifocal posterior chamber IOL implantation and FLAKs were planned, an anticipated post-operative BCDVA of 20/40 or better, and a calculated spherical equivalent power targeted for emmetropia. Soft and rigid gas-permeable (RGP) contact lens wearers were required to discontinue lens wear for a minimum of 2 or 3 weeks, respectively, or until biometry was stable. Exclusion criteria included mature cataract anticipated to prolong the surgical procedure, abnormal corneal topography (ie keratoconus, pellucid marginal degeneration, or irregular astigmatism), significant anterior segment pathology (ie chronic uveitis, iritis, aniridia, rubeosis iridis), history of severe dry eye that would impair the ability to obtain reliable study measurements, corneal disease (ie herpes simplex, herpes zoster keratitis, Fuchs corneal dystrophy), history of intraocular or corneal surgery, history of clinically significant retinal pathology that would limit the patient’s ability to obtain a postoperative BCDVA of 20/40, or uncontrolled glaucoma in the study eye. Patients planned to undergo other concomitant ocular procedures (ie MIGS, endothelial keratoplasty) were also excluded. If both eyes from one patient met these criteria, then both eyes were considered study eyes.
Enrolled subjects received optical biometry (IOLMaster 700; Carl Zeiss Meditec AG, Jena, Germany), topography (Galilei G4; Ziemer Ophthalmic Systems AG, Port, Switzerland), and pre-operative manifest refraction. Surgeries were performed by one of two right-handed surgeons (B.E. or G.M.). The femtosecond laser used was the Victus (SW v3.3 SP03, Bausch & Lomb Surgical, Bridgewater, New Jersey). A laser-assisted 2.5 mm clear corneal incision was created 20 degrees inferotemporal/superotemporal to the horizontal meridian in right/left eyes, respectively. Surgically induced astigmatism of 0.2 D was assumed for all main incisions.8 The laser was also used to complete a 5.2 mm capsulotomy and nuclear fragmentation. All arcuate incisions were made at a 9.0 mm diameter and depth of 80% as measured by the OCT corneal depth measurement on the laser. Other pertinent arcuate incision parameters included a side cut angle of 90°, line spacing of 2.0 µm, spot spacing of 5.0 µm, and energy of 1.7 µJ. Arcuate incisions were not further manipulated or opened by the surgeon intraoperatively or at any point post-operatively. Standard coaxial phacoemulsification techniques were used for nucleus disassembly. There were no complications noted in any of the surgeries for enrolled subjects. One month post-operatively, uncorrected and corrected distance visual acuity, optical biometry (IOLMaster 700), and manifest refraction were collected by experienced clinical staff masked to the treatment plan.
The FemtoAK nomogram (FemtoAK.com) is a freely accessible femtosecond-laser assisted arcuate incision planning-tool for treating astigmatism at the time of cataract surgery. It will make recommendations in eyes with ≥0.5 D of ATR or ≥1.0 D of WTR or OBL astigmatism, but ≤2.25 D. The nomogram is optimized for incisions of 80% depth and 9 mm diameter. It allows the surgeon to customize placement and effect (surgically induced astigmatism) of the main wound. In the case where a single arc with arc length greater than 45 degrees is recommended, the nomogram will automatically truncate that single arc to be no larger than 45 degrees to minimize the risk of inducing irregular astigmatism (and will display a warning message to this effect). The nomogram is an adaptation of another nomogram previously published by Baharozian et al9 with modifications to WTR astigmatism treatments, since they reported 24% of eyes in this sub-group had a flipped-axis post-operatively.
Data and Statistical Analysis
We set as a benchmark for success a goal of obtaining ≤0.5 D of astigmatism in 50% of eyes post-operatively, based on a Cochrane Database Systematic Review on the performance of other limbal relaxing incision nomograms.10 Assuming 0% of patients had ≤0.5 D of astigmatism pre-operatively (inclusion criteria for entry into the study) and setting a benchmark of 50% with ≤0.5 D post-operatively, 16 eyes would be needed to achieve a power of 80% and a two-sided significance of 5%.11
Astigmatism analyses were performed using the Alpins method considering 3 vectors: target-induced astigmatism (TIA), surgically induced astigmatism (SIA), and difference vector (DV).12 TIA is defined as the keratometric magnitude and direction of astigmatic correction that the surgery intends. The SIA is the actual magnitude and direction of astigmatic treatment from surgery. The DV measures the magnitude and orientation of the astigmatism needed to achieve the intended targeted correction (SIA minus TIA). Additionally, we created a new astigmatic index, net effective astigmatism (NEA). The NEA is the FemtoAK nomogram’s proprietary estimation of the refractive astigmatism an eye has, after accounting for the 0.2 D of astigmatism induced by the main incision. As a general rule, the NEA is greater than the TIA in eyes with ATR and less than the TIA in eyes with WTR astigmatism.
Main outcome measures included magnitude of error (ME), angle of error (AE), correction index (CI), index of success (IOS), and proportion of eyes with ≤0.5 and 1.0 D of astigmatism. ME is the difference in magnitude between SIA and TIA, with positive values indicating over-correction and negative values indicating under-correction. AE is the difference in axis between SIA and TIA, with positive values representing a counterclockwise treatment application and negative representing a clockwise application. CI is the ratio of SIA to TIA, with an ideal value being 1.0. IOS measures the ratio of DV to the TIA and has an inverse relationship to the relative surgical success (smaller IOS is equivalent to greater success). While the TIA value is based on the corneal plane value of the actual treatment, SIA and all other parameters are subdivided into keratometric and refractive analyses, which will be reported as such. The corneal SIA was compared against TIA for the keratometric analysis, whereas the refractive SIA was compared against the NEA for the refractive analysis.
Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) was used for data collection, vector analysis, and graphical representation. Baseline demographic characteristics were summarized using descriptive statistics including frequencies, means, and standard deviations. Pre- to post-operative univariate comparisons were made using the paired t-test, while vector analyses required conversion of polar vectors to cartesian coordinates and application of Hotelling’s T-squared test.13 SAS software version 9.4 (SAS Institute, Cary, NC) was used to evaluate centroid data. P-values less than 0.05 were considered statistically significant.
Results
Ninety-four patients were recruited between April 2019 and September 2023. Of these, 13 patients were lost to follow up and 12 patients withdrew from the study after signing consent but before their final follow-up. As a result, 95 eyes of 69 patients received surgery between May 2019 and November 2023. Twenty-two patients had eligible right eyes, another 21 patients had eligible left eyes, and 26 patients had both eyes that were eligible. The demographics of study eyes are shown in Table 1. The patient population ranged from 39 to 80 years old. There were 48 (51%) right eyes and 47 (49%) left eyes. The orientation, as measured by the optical biometer, included 41 (43.2%), 35 (36.8%), and 19 (20.0%) eyes with ATR, WTR, and OBL astigmatism, respectively.
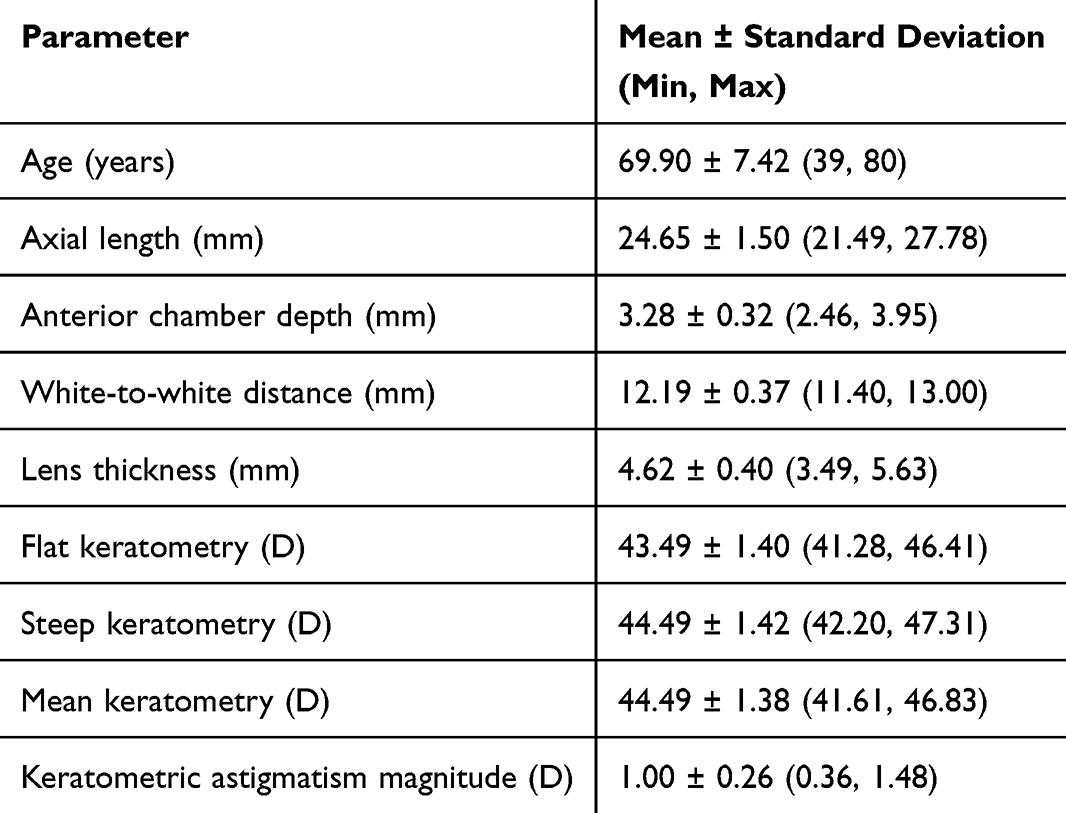 |
Table 1 Eye Demographics |
Keratometric Efficacy Analysis
Postoperative outcomes, based on keratometric indices, are displayed in Table 2 and Figure 1A. Overall, the mean corneal astigmatism was significantly reduced from 1.00 D ± 0.26 D (range [0.36, 1.48]) to 0.83 D ± 0.49 D (range [0, 3.10]) (p < 0.001). The mean absolute astigmatism magnitude was less than 1.00 D for all three orientation sub-groups. Overall, 26% and 66% of eyes achieved corneal astigmatism ≤0.50 and 1.00 D. Seventy-eight, 46%, and 79% of ATR, WTR, and OBL eyes, respectively, achieved less than 1.0 diopter (D).
 |
Table 2 Corneal Astigmatism Measurements and Alpins’ Indices of Astigmatism Correction Efficacy |
 |
Figure 1 (A) Proportion of eyes with corneal astigmatism within target. (B) Proportion of eyes with refractive astigmatism within target. |
The standard single-angle plots ascribed to the Alpins method of analysis are displayed in Figure 2. The mean TIA (0.26 D @ 32° ± 1.08 D, range [0.5, 1.58]) was lower than the mean keratometric SIA (0.28 D @ 103° ± 0.92 D, range [0.04, 4.41]). The mean keratometric DV was 0.51 D @ 22° ± 0.92 D, range [0, 3.09]. Since a general rule of thumb is to aggressively treat ATR astigmatism and undertreat WTR astigmatism, one would expect the CI to be highest for ATR and lowest for WTR eyes; likewise, the IOS should be lowest for ATR eyes and highest for WTR eyes. In our study, the keratometric CI was 0.86 and 0.27 for ATR and WTR eyes, respectively. The keratometric IOS was also lowest for ATR (0.14 ± 0.63) and highest for WTR (0.83 ± 0.28).
 |
Figure 2 Standard single-angle plots for target-induced astigmatism (TIA), surgically induced astigmatism (SIA), difference vector, correction index, SIA magnitude vs TIA magnitude, and corneal angle of error. |
Figure 3A denotes the double-angle plots for pre- and postoperative corneal astigmatism. There was a significant change from pre- to post-operative centroid values (p = 0.045), with the net effect moving toward a more WTR orientation (0.10 D @ 125° to 0.36 D @ 108°). This is an expected result for a nomogram that has the intention of over-correcting ATR eyes and under-correcting WTR eyes.
 |
Figure 3 (A) Double-angle plot for preoperative and postoperative corneal astigmatism. (B) Double-angle plot for preoperative and postoperative refractive astigmatism. |
Refractive Efficacy Analysis
Postoperative outcomes, based on refractive indices, are displayed in Table 3 and Figure 1B. Overall, the mean refractive astigmatism was significantly reduced from 1.04 D ± 0.62 D (range [0, 3.25]) to 0.58 D ± 0.45 D (range [0, 2.50]) (p < 0.001). The mean absolute astigmatism magnitude was less than 0.75 D for all three orientation sub-groups. Overall, 56% and 92% of eyes achieved refractive astigmatism ≤0.50 and 1.00 D. Ninety, 94%, and 89% of ATR, WTR, and OBL eyes, respectively, achieved less than 1.0 diopter (D).
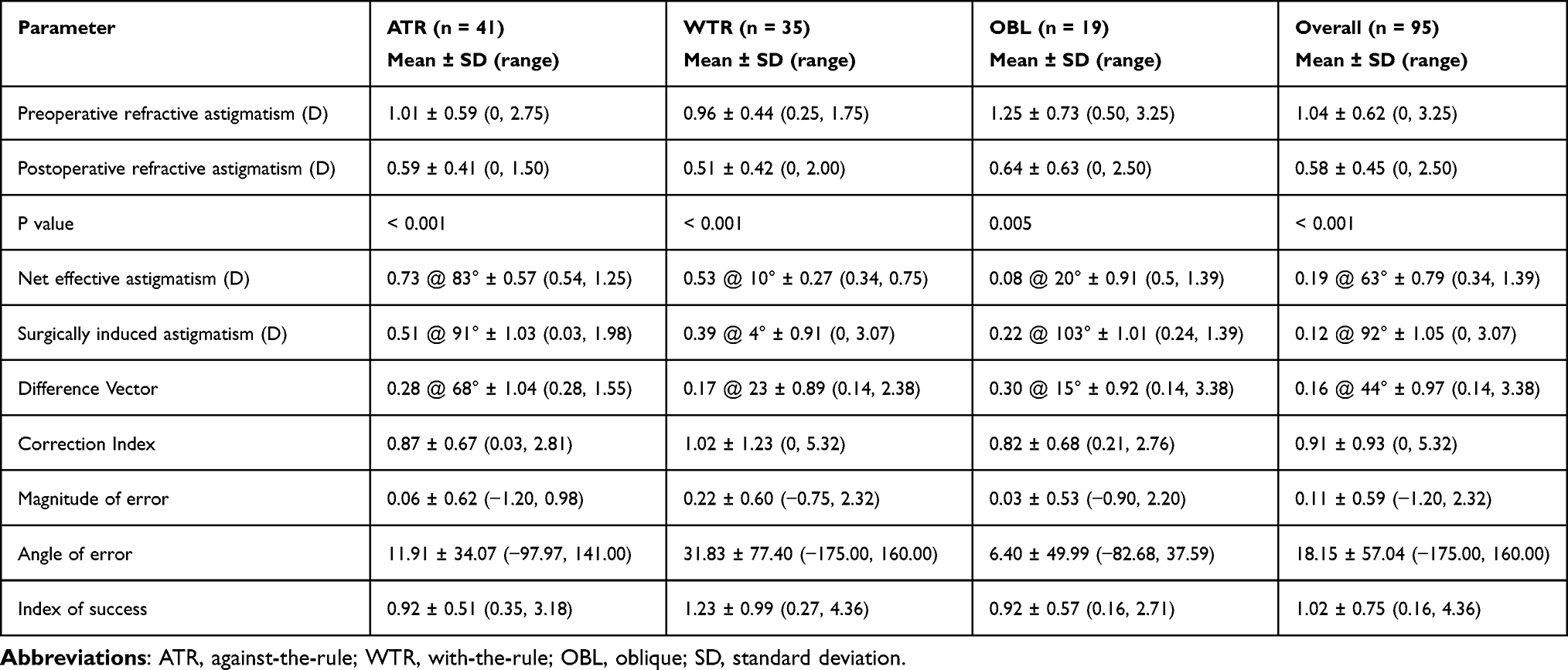 |
Table 3 Refractive Astigmatism Measurements and Alpins’ Indices of Astigmatism Correction Efficacy |
Refractive SIA was calculated as the difference between post- and preoperative refractive astigmatism. The mean NEA (0.19 D @ 63° ± 0.79 D, range [0.34, 1.39]) was higher than the mean refractive SIA (0.12 D @ 92° ± 1.05 D, range [0, 3.07]). The refractive DV was 0.16 D @ 44° ± 0.97 D (range [0.14, 3.38]). Since a general rule of thumb is to aggressively treat ATR astigmatism and under-treat WTR astigmatism, one would expect the CI to be highest for ATR and lowest for WTR eyes; likewise, the IOS should be lowest for ATR eyes and highest for WTR eyes. In our study, the refractive CI was 0.87 and 1.02 for ATR and WTR eyes, respectively. The refractive IOS was also lowest for ATR (0.92 ± 0.51) and highest for WTR (1.23 ± 0.99).
Figure 3B denotes the double-angle plot for pre- and postoperative refractive astigmatism. Of note, cataracts can make preoperative refractive astigmatism measurements unreliable; this may explain the presence of multiple outliers compared to the preoperative astigmatism measurements shown in Figure 3A. There was no statistical significance between pre- and postoperative centroid values (p = 0.56), with the net effect moving towards a more WTR orientation (0.29 D @ 175° to 0.17 D @ 171°). This is an expected result for a nomogram that has the intention of over-correcting ATR eyes and under-correcting WTR eyes.
Flipped Axes
The number and proportion of eyes that experienced a flipped axis of astigmatism (ATR to WTR or WTR to ATR) is enumerated in Table 4. Even though 17% of ATR eyes experienced a flipped axis of astigmatism by keratometric measures, this only translated to a 7% incidence by refraction. Conversely, despite only 3% of WTR eyes experiencing a flipped axis by keratometric measures, this translated to a 34% incidence by refraction. Overall, 8% and 16% of ATR or WTR eyes experienced a flipped axis of astigmatism by corneal or refractive measures, respectively.
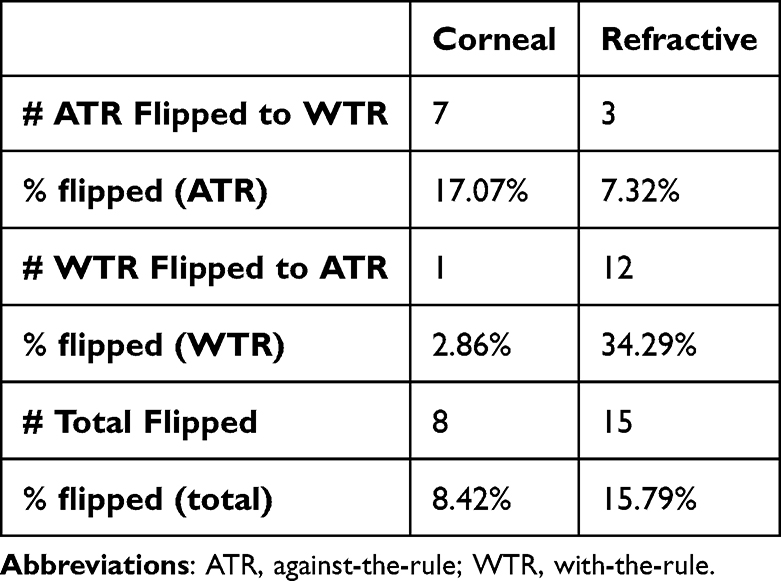 |
Table 4 Number and Proportion of Eyes Flipped from ATR to WTR or WTR to ATR |
Discussion
Persistent astigmatism following cataract surgery heightens reliance on corrective lenses and can reduce patient satisfaction. Correction of astigmatism can be accomplished either through an incisional technique, such as arcuate keratotomies, or by implanting a toric intraocular lens.14 LRIs and FLAKs aim to reduce postoperative astigmatism, where FLAKs can reduce confounding influence of manual imprecisions to the keratotomies.15 The FemtoAK nomogram was created to guide surgical plans in the creation of femtosecond-laser assisted arcuate keratotomies. It is accessible at FemtoAK.com, is open-access, accepts a large range of treatable astigmatism magnitudes, and incorporates the effect of the main surgical incision. We hope that this lowers barriers for surgeons who are interested in incorporating FLAKs into their practice.
Herein, we present the first prospective case series completed using the FemtoAK nomogram, and analyze the efficacy in treating eyes with low to moderate astigmatism. We found a significant reduction in refractive astigmatism from 1.04 ± 0.62 D to 0.58 ± 0.45 D. Fifty-six and 92% of eyes had ≤0.50 D and 1.00 D, respectively, of residual refractive astigmatism one month after surgery. Of note, we set a benchmark against which success is measured of 50% of eyes with ≤0.5 D of astigmatism post-operatively. Although we did not achieve this benchmark by keratometric outcome measures (26%), we did so by refractive criteria (56%). Since the goal of refractive surgery is not neutralization of corneal astigmatism, but rather manifest refractive astigmatism (what the patient experiences), we can say that the FemtoAK nomogram is efficacious in its correction of astigmatism when performed at the time of cataract surgery.
Our results compared favorably to previously published literature on outcomes of femtosecond arcuate incisions. A study by Yoo et al on 23 patients with preoperative refractive astigmatism ranging from 1.0 to 3.0 D found that the postoperative refractive astigmatism was 0.79 ± 0.11 D at the one-month follow-up,16 and Chan et al reported 33% of eyes with ≤0.5 D.17 Baharozian et al reported a decrease in keratometric astigmatism from 0.856 ± 0.318 to 0.626 ± 0.417 D, and a resultant postoperative refractive astigmatism of 0.495 ± 0.400 D.9 Our study observed similar reduction with keratometric astigmatism decreasing from 1.00 ± 0.26 D to 0.83 ± 0.49 D and refractive astigmatism decreasing from 1.04 ± 0.62 D to 0.58 ± 0.45 D. On the other hand, we reported higher postoperative keratometric (0.83 ± 0.49 D) and refractive (0.58 ± 0.45 D) cylinders when compared to the Castrop nomogram from the Wendelstein study (0.65 ± 0.40 and 0.39 ± 0.25 D, respectively).7 The magnitude of correction in our study was also excellent, with an overall CI of 0.91 ± 0.93 D. This result was comparable to the Castrop nomogram by Wendelstein et al (0.92 ± 0.21 D),7 and was better than the Chan et al nomogram (0.86 ± 0.52 D).17 Differences in the results between previous studies and ours could be due to varying demographics, distributions of the corrected astigmatism, or differences in the nomograms themselves.
We also investigated the proportion of eyes with flipped axes following treatment with the FemtoAK nomogram. By keratometric measures, we observed a higher rate of axis flipping from ATR to WTR than the reverse. However, by refractive measures, a greater proportion flipped from WTR to ATR. It is well established that, independent of cataract surgery, the corneal axis tends to shift towards ATR as we age.18 To this end, the FemtoAK nomogram was designed to over-correct ATR eyes and under-correct WTR eyes. Further updates to the nomogram might be needed for those with preoperative WTR astigmatism.
This study has many strengths, including the study design (prospective interventional clinical trial) and proper analysis of astigmatism outcomes. Our opinion is that the Alpins method provides a comprehensive display that answers all the questions related to astigmatism correction. It utilizes both univariate and bivariate analysis. We also included double-angle plots to emphasize the nomograms focus on minimizing refractive, rather than keratometric, astigmatism.
On the other hand, this study is not without limitations. First, recruitment was significantly impacted by the COVID-19 pandemic, which forced many patients who signed consent and/or completed surgery to be lost to follow-up. Second, the final follow-up was short at 1 month. While some literature has shown that these corrections remain stable after the first postoperative month,19–22 others suggest that the effects of AKs may regress over time, and our study did not allow us to evaluate this. Third, while AKs applied in this study were epi-penetrating (versus intra-stromal), no attempts were made to open any of the incisions intra- or postoperatively. Giving the surgeon discretion to open incisions postoperatively at the slit lamp in patients that present with under-corrections might have translated to improved outcomes. Last, in cases in which the side-port (1.0 mm) incision would have interacted with the AK incision, its position was manually adjusted. Yet, our study did not evaluate the impact the position of the side port incision had on surgically induced astigmatism. Lastly, our nomogram is restrained in its recommendation of arcuates with a depth of 80% and diameter of 9.0 mm. The 9.0 mm diameter might be too large for some eyes, or might interact obtrusively with the main incision. To compensate for this, surgeons might consider adjusting the diameter down to 8.5 mm during treatment, but must then consider the increased effect of planned arcuate incisions.23
The FemtoAK nomogram is a useful tool in the management of astigmatism, but more work is needed to further improve its accuracy. The results from this study, specifically the keratometric and refractive CI’s, might be used to further refine the nomogram. Since CI’s were less than 1.0 on average, we suggest, as a first step, that surgeons evaluate their outcomes after opening the arcuate incisions, which was not done in this study. In addition, future incorporation of additional biometric variables, such as measured posterior corneal curvature or corneal hysteresis, might further improve nomogram accuracy. Allowing customization of the incision depth and diameter within the same nomogram, as a function of corneal pachymetry and white-to-white, might also be useful. Further sub-group analysis might also allow us to better refine the nomograms proprietary calculation of NEA, which in turn could lead to even better accuracy. Last, even though femtosecond technology offers the advantage of smoother interfaces and reproducible cuts, variability in the wound healing process is an inherent limitation when working with this treatment modality;24 future work might also entail modulating this healing response postoperatively to make it more uniform.
Abbreviations
IOLs, intraocular lenses; AKs, astigmatic keratotomies; FLAKs, femtosecond laser assisted keratotomies; BCDVA, best corrected distant visual acuity; RGP, rigid gas-permeable; OCT, optical coherence tomography; ATR, against-the-rule; WTR, with-the-rule; OBL, oblique; TIA, target-induced astigmatism; NEA, net effective astigmatism; SIA, surgically induced astigmatism; DV, difference vector; ME, magnitude of error; AE, angle of error; CI, correction index; IOS, index of success.
Data Sharing Statement
The de-identified data may be made available for three years by contacting the corresponding author, Seth Pantanelli.
Ethics Approval and Informed Consent
The Penn State College of Medicine Institutional Review Board reviewed and approved the study protocol (IRB STUDY00008058). All enrolled subjects completed a written informed consent before enrollment. All patient data was kept anonymous and confidential.
Funding
The project was supported by the Pennsylvania Lions Sight Conservation and Eye Research Foundation and by the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1 TR002014. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Disclosure
S.P. receives research support from Bausch & Lomb and Carl Zeiss Meditec, unrelated to the present work. He is also a consultant for Bausch & Lomb and Carl Zeiss Meditec, also unrelated to the present work. The remaining authors have no proprietary interest or financial relationships to disclose.
References
1. Hashemi H, Fotouhi A, Yekta A, Pakzad R, Ostadimoghaddam H, Khabazkhoob M. Global and regional estimates of prevalence of refractive errors: systematic review and meta-analysis. J Curr Ophthalmol. 2017;30(1):3–22. doi:10.1016/j.joco.2017.08.009
2. Wasser LM, Tsessler M, Weill Y, Zadok D, Abulafia A. Ocular biometric characteristics measured by swept-source optical coherence tomography in individuals undergoing cataract surgery. Am J Ophthalmol. 2022;233:38–47. doi:10.1016/j.ajo.2021.06.032
3. Müller-Kassner A, Sartory T, Müller M, et al. Refractive and visual outcome of misaligned toric intraocular lens after operative realignment. Am J Ophthalmol. 2021;224:150–157. doi:10.1016/j.ajo.2020.11.024
4. Oshika T, Nakano S, Inamura M, et al. Extensive misalignment of plate-haptic rotationally asymmetric multifocal toric intraocular lens. Jpn J Ophthalmol. 2023;67(5):560–564. doi:10.1007/s10384-023-01001-x
5. Cleary C, Tang M, Ahmed H, Fox M, Huang D. Beveled femtosecond laser astigmatic keratotomy for the treatment of high astigmatism post–penetrating keratoplasty. Cornea. 2013;32(1):54–62. doi:10.1097/ICO.0b013e31825ea2e6
6. Noh H, Yoo YS, Shin KY, Lim DH, Chung TY. Comparison of penetrating femtosecond laser-assisted astigmatic keratotomy and toric intraocular lens implantation for correction of astigmatism in cataract surgery. Sci Rep. 2021;11(1):7340. doi:10.1038/s41598-021-86763-5
7. Wendelstein JA, Hoffmann PC, Mariacher S, et al. Precision and refractive predictability of a new nomogram for femtosecond laser‐assisted corneal arcuate incisions. Acta Ophthalmol. 2021;99(8):e1297–e1306. doi:10.1111/aos.14837
8. Langenbucher A, Szentmáry N, Cayless A, et al. Surgically induced astigmatism after cataract surgery—a vector analysis. Curr Eye Res. 2022;47(9):1279–1287. doi:10.1080/02713683.2022.2052108
9. Baharozian CJ, Song C, Hatch KM, Talamo JH. A novel nomogram for the treatment of astigmatism with femtosecond-laser arcuate incisions at the time of cataract surgery. Clin Ophthalmol. 2017;11:1841–1848. doi:10.2147/OPTH.S141255
10. Mukhija R, Fonseca A, Borkum S, Frattaroli P, Barbon E, Nanavaty MA. Toric intraocular lens versus peripheral corneal relaxing incisions for astigmatism between 0.75 and 2.5 diopters: 5-years outcomes. Curr Eye Res. 2024;49(1):46–52. doi:10.1080/02713683.2023.2260961
11. Dhand NK, Khatkar MS. Statulator: an online statistical calculator. Sample size calculator for comparing two paired proportions. 2014. Available from: https://statulator.com/SampleSize/ss2PP.html.
12. Alpins N. Comment on: rethinking the optimal methods for vector analysis of astigmatism. J Cataract Refract Surg. 2021;47(1):138. doi:10.1097/j.jcrs.0000000000000521
13. Karslioglu MZ, Kesim C, Tas AY, Hasanreisoglu M, Muftuoglu O, Sahin A. Comparison of postoperative corneal astigmatism induced by two different corneal incisions during microincisional cataract surgery. Beyoglu Eye J. 2021;7(1):1–8. doi:10.14744/bej.2021.17362
14. Amesbury EC, Miller KM. Correction of astigmatism at the time of cataract surgery. Curr Opin Ophthalmol. 2009;20(1):19–24. doi:10.1097/ICU.0b013e328319c27a
15. Roberts HW, Wagh VK, Sullivan DL, Archer TJ, O’Brart DPS. Refractive outcomes after limbal relaxing incisions or femtosecond laser arcuate keratotomy to manage corneal astigmatism at the time of cataract surgery. J Cataract Refract Surg. 2018;44(8):955–963. doi:10.1016/j.jcrs.2018.05.027
16. Yoo A, Yun S, Kim JY, Kim MJ, Tchah H. Femtosecond laser-assisted arcuate keratotomy versus toric IOL implantation for correcting astigmatism. J Refract Surg. 2015;31(9):574–578. doi:10.3928/1081597X-20150820-01
17. Chan TCY, Cheng GPM, Wang Z, Tham CCY, Woo VCP, Jhanji V. Vector analysis of corneal astigmatism after combined femtosecond-assisted phacoemulsification and arcuate keratotomy. Am J Ophthalmol. 2015;160(2):250–255.e2. doi:10.1016/j.ajo.2015.05.004
18. Hayashi K, Manabe SI, Hirata A, Yoshimura K. Changes in corneal astigmatism during 20 years after cataract surgery. J Cataract Refract Surg. 2017;43(5):615–621. doi:10.1016/j.jcrs.2017.02.028
19. Lim R, Borasio E, Ilari L. Long-term stability of keratometric astigmatism after limbal relaxing incisions. J Cataract Refract Surg. 2014;40(10):1676–1681. doi:10.1016/j.jcrs.2014.01.045
20. Day AC, Stevens JD. Stability of keratometric astigmatism after non-penetrating femtosecond laser intrastromal astigmatic keratotomy performed during laser cataract surgery. J Refract Surg. 2016;32(3):152–155. doi:10.3928/1081597X-20160204-01
21. Chan TCY, Ng ALK, Cheng GPM, Wang Z, Woo VCP, Jhanji V. Corneal astigmatism and aberrations after combined femtosecond-assisted phacoemulsification and arcuate keratotomy: two-year results. Am J Ophthalmol. 2016;170:83–90. doi:10.1016/j.ajo.2016.07.022
22. Byun YS, Kim S, Lazo MZ, et al. Astigmatic correction by intrastromal astigmatic keratotomy during femtosecond laser-assisted cataract surgery: factors in outcomes. J Cataract Refract Surg. 2018;44(2):202–208. doi:10.1016/j.jcrs.2017.11.018
23. Oshika T, Shimazaki J, Yoshitomi F, et al. Arcuate keratotomy to treat corneal astigmatism after cataract surgery: a prospective evaluation of predictability and effectiveness. Ophthalmology. 1998;105(11):2012–2016. doi:10.1016/S0161-6420(98)91117-4
24. Sarayba MA, Ignacio TS, Binder PS, Tran DB. Comparative study of stromal bed quality by using mechanical, IntraLase femtosecond laser 15- and 30-kHz microkeratomes. Cornea. 2007;26(4):446–451. doi:10.1097/ICO.0b013e318033e7cc
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.