")
Back to Journals » Clinical Ophthalmology » Volume 18
Slanted and Standard Lateral Rectus Recession Procedures for Convergence Insufficiency-Type Intermittent Exotropia in Children: A Retrospective Cohort Study
Authors Suzuki Y , Aoki T , Tomita A , Mitsukawa T , Hama Y, Yamada M
Received 28 March 2024
Accepted for publication 19 August 2024
Published 30 August 2024 Volume 2024:18 Pages 2453—2460
DOI https://doi.org/10.2147/OPTH.S471172
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yumi Suzuki, Takafumi Aoki, Akane Tomita, Tadahiro Mitsukawa, Yukiko Hama, Masakazu Yamada
Department of Ophthalmology, Kyorin University School of Medicine, Mitaka, Tokyo, Japan
Correspondence: Yumi Suzuki, Email [email protected]
Purpose: To evaluate the efficacy and safety of slanted bilateral lateral rectus recession (BLR-rec) for treating convergence insufficiency-type intermittent exotropia (CI-IXT) in children.
Methods: In this retrospective cohort study, 26 patients aged < 16 years with CI-IXT who underwent BLR-rec between August 2016 and July 2021 with six months of follow-up data post-surgery were classified into slanted BLR-rec group (n = 14) and standard BLR-rec group (n = 12; equal-length recession of the upper and lower horns of the LR muscle). Surgical outcomes were compared between the groups.
Results: In the slanted and standard groups, the preoperative distance exodeviation was 27.9 ± 5.5 and 30.8 ± 10.0 prism diopter (PD) (p = 0.63), near exodeviation was 41.1 ± 5.6 and 42.9 ± 9.2 PD (p = 0.75), and difference between near and distance deviation (N-D deviation difference) was 13.2 ± 3.2 and 12.1 ± 3.3 PD (p = 0.30), respectively. The ratio of postoperative and preoperative N-D deviation difference was compared between the slanted BLR and standard BLR groups at six months postoperatively. The results revealed that the ratio for slanted-BLR was 0.44 ± 0.19, and for standard-BLR was 0.84 ± 0.24. In the standard group, stereoacuity remained unchanged post-surgery compared to that pre-surgery, while the slanted group showed significant improvement (p < 0.05, Wilcoxon signed-rank test).
Conclusion: Compared with the standard BLR-rec procedure, the slanted BLR-rec procedure reduced N-D deviation differences in CI-IXT, positively impacting gross stereopsis.
Keywords: bilateral lateral rectus recession, convergence insufficiency-type intermittent exotropia, postoperative diplopia, consecutive esotropia, stereopsis
Introduction
The convergence-insufficiency type of intermittent exotropia (CI-IXT) is characterized by a greater exodeviation at near fixation compared to distance by ≥10 prism diopters (PD).1–3 Patients with CI-IXT may experience symptoms including headache, brow ague, diplopia, blurred vision, fatigue of the eye, and reading difficulty, which can significantly impact their work and lifestyle.4–6 CI-IXT is associated with weak fusional convergence amplitudes, reduced accommodative amplitudes, or a low accommodative convergence to accommodation (AC/A).3,4,7 In mild cases, symptoms may be amenable to non-surgical treatment like orthoptic treatment and base-in prism reading glasses.8–10 However, some patients do not respond to non-surgical treatment and cannot maintain phoria for near vision due to large exodeviations, necessitating surgical treatment.
Various surgical modalities have been reported for patients with CI-IXT.3,4,11–14 In cases of intractable convergence insufficiency, surgeons have employed medial rectus (MR) strengthening procedures and MR resections with adjustable sutures to minimize the disparity between near and distance deviations (N-D deviation difference).4,11,12
Furthermore, unilateral lateral rectus (LR) recession combined with MR resection (R&R) has been utilized for CI-IXT treatment.3,13,14 Despite the range of surgical methods available, they often struggle to address the N-D deviation difference effectively. Conventional recession/resection surgeries targeting near deviation may result in postoperative overcorrection at a distance, while those targeting distance deviation may lead to under-correction at near deviation. Consequently, slant surgery has emerged as a method aimed at improving the N-D deviation difference.6,7,15–18
In 1999, Snir et al proposed a novel slanted LR recession procedure for CI-IXT, wherein the upper horn of the LR muscle was recessed based on distance exodeviation, and the lower horn was recessed based on near exodeviation.7 They reported a success rate of 80–90% in achieving an N-D deviation difference of ≤8 PD one year after slanted LR recession for convergence insufficiency. This study aimed to evaluate the efficacy and safety of the slanted bilateral LR recession procedure (slanted BLR-rec) for the treatment of CI-IXT in children compared with those of the standard bilateral LR recession procedure (standard BLR-rec). We evaluated improvements in near stereopsis and N-D deviation difference per 1 mm. The primary outcome measured the ratio of postoperative to preoperative N-D deviation difference.
Materials and Methods
Patients
The study was approved by the institutional review board of Kyorin University Hospital (project R-01-115, approval number 1380) and adhered to the Declaration of Helsinki for the protection of human subjects. Informed consent was obtained from parents or guardians of patients (<16 years) before surgery.
This single-institution retrospective cohort study was conducted at Kyorin University Hospital. It included patients aged six to 15 years with CI-IXT who underwent BLR-rec between August 2016 and July 2021, with at least six months of post-surgery follow-up, were recruited from our medical records. Inclusion criteria were CI-IXT with ≥10 PD greater exodeviation at near fixation than at a distance, best-corrected visual acuity (VA) in the worse eye of 20/25 or better, and ≤1-line interocular difference in VA on the Landolt Optotype. Both eyes’ spherical equivalent values based on cycloplegic refraction fell within −7.0 D and +4.0 D. Exclusion criteria included: A-V pattern of strabismus, vertical deviation ≥5 PD, torsional strabismus, nystagmus, previous ocular/strabismus surgery, other ocular/neurologic conditions, and systemic disease. Preoperatively, none of the patients underwent occlusion therapy or received a prescription for prism eyeglasses. Patients were divided into two groups based on surgical procedures: Standard BLR-rec was performed on eligible patients from 2016 to 2018, while slanted BLR-rec was conducted from 2019 to 2021. Standard BLR-rec served as a historical control.
Examination
Patients underwent comprehensive ophthalmologic and orthoptic evaluations, including best-corrected visual acuity, cycloplegic refraction (1% cyclopentolate hydrochloride, administered twice), fundus examination, and ocular motility assessment. Distance (5 m) and near (1/3 m) deviations were measured using the alternating prism cover test (APCT) using accommodative targets, with patients wearing their best optical correction. Monocular occlusion was performed for 45 minutes to avoid fusion, followed by a prism adaptation test (PAT); maximum deviations were determined near and at a distance. In other words, the maximum angle of deviation was obtained using PAT to determine the surgical amount for both groups. Surgical doses for LR recession in both groups were calculated using Park’s surgical dosage table.19
Our routine post-operative follow-up schedule included assessments at one day, one week, four weeks, and six months.
Objective torsion was measured using a major amblyoscope to detect cyclotropia. Stereopsis was evaluated using the Titmus stereo test (Stereo Optical, Chicago, IL, USA) and the TNO stereo test (HAAG-STREIT UK) (Table 1). Titmus and TNO stereo tests were used to evaluate pre- and post-operative binocular vision function. For numerical comparison of these stereoscopic results, we scored the stereopsis such that the binocular disparity log values were approximately equal. Table 1 presents the stereopsis scoring of the results of the TNO and Titmus stereo tests on an interval scale. The eight points of the scale are defined as follows: score 0: none; score 1: 3000 seconds (sec); score 2: 800 sec; score 3: 480 sec; score 4: 240 sec; score 5: 120 sec; score 6: 60 sec; score 7: <60 sec.
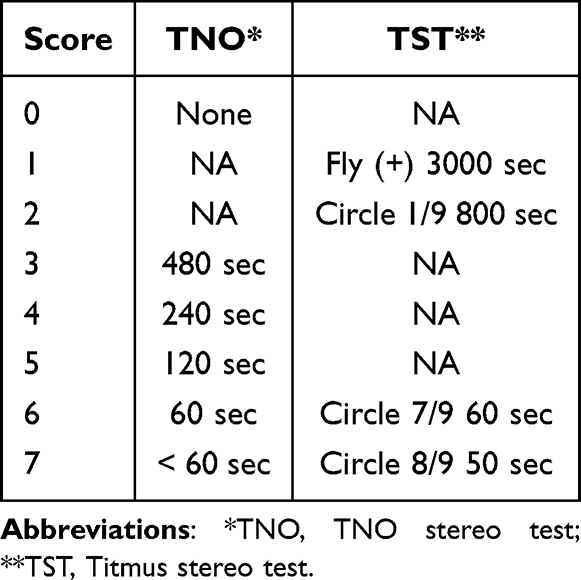 |
Table 1 Stereopsis Scoring |
Surgical Procedure
Both standard and slanted BLR-rec procedures were conducted via temporal limbal peritomy under general anesthesia in all cases. The LR was recessed and sutured directly to the globe. The amount of slanted BLR-rec was determined according to the Park’s surgical dosage table.19 The upper and lower horns of the LR were recessed based on the distance and near exodeviations, respectively. The slanted LR recession was performed obliquely compared with the original insertion (Figure 1). The lower horn was recessed more than the upper horn owing to greater exodeviation at near than at distance. In standard LR recession, without any risk of consecutive esotropia at distance, both upper and lower horns were equally recessed based on the maximum exodeviation angle at a distance determined by Park’s surgical dosage tables.19
 |
Figure 1 The slanted BLR-rec procedure (surgeon’s view). The lower horn was recessed according to the near exodeviation. The upper horn was recessed according to the distance exodeviation. The lower horn of the muscle was more recessed than the upper horn in the new insertion. The physiological mechanism of the slanted BLR-rec for CI-IXT considered that it was based on Scott’s investigation. Abbreviations: BLR-rec, bilateral lateral rectus recession; CI-IXT, convergence insufficiency-type intermittent exotropia. |
Postoperative evaluations included assessment of the difference between distance and near exodeviation as well as the presence of diplopia due to consecutive esotropia, torsion, and the A-V pattern of strabismus. The impact of the slanted recession on deviation collapse was defined as per Snir et al.7 The impact of the slanted recession on the collapse of the angle of deviation was calculated as follows: the mean reduction in the N-D deviation difference in exodeviation after slanted surgery was divided by the mean amount of slanted insertion, which was the mean difference between the new upper and lower horns of the slanted muscle from the original insertion. All surgeries were performed by two surgeons.
Successful surgical alignment was defined as <+5.0 PD esodeviation (esophoria/tropia) and <-8.0 PD exodeviation (exophoria/tropia) in the primary gaze while viewing distant or near targets, with an N-D deviation difference ≤8 PD.
Statistical Analysis
The Statistical Package for the Social Sciences (version 27.0, IBM Armonk, NY, USA) was used for all statistical analyses. Mann–Whitney U-test, Wilcoxon signed-rank test, and Fisher’s exact test were used to perform comparisons.
Results
In total, 26 patients aged six to 15 years with CI-IXT were included in the study, with 14 and 12 patients in the slanted BLR-rec and standard BLR-rec groups, respectively. Table 2 displays participants’ characteristics, revealing no significant differences between groups in preoperative factors such as average age at surgery (p = 0.38), preoperative follow-up duration (p = 0.76), and spherical equivalent of the right and left eyes (p = 0.90, and p = 0.68, respectively).
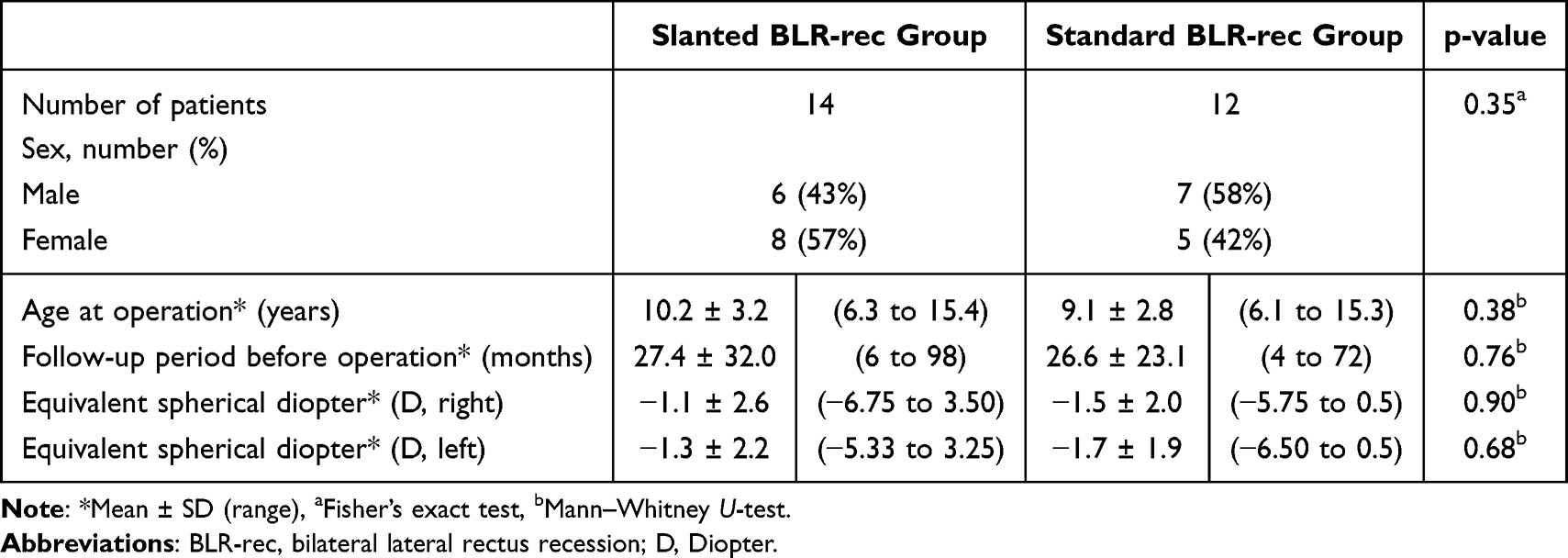 |
Table 2 Preoperative Patient Characteristics |
Table 3 presents angles of deviation at near fixation, far fixation, N-D deviation difference, and the ratio of postoperative N-D deviation difference/preoperative N-D deviation difference in the preoperative period and six months post-surgery. No significant differences were observed between slanted and standard groups in the preoperative angle of deviation at near and distant, as well as the N-D deviation difference (p = 0.63, p = 0.75, and p = 0.30, respectively).
 |
Table 3 Pre-and Post-Operative Exotropia Deviation Results |
However, the angle of deviation at six months post-surgery for the slanted and standard groups was 5.7 ± 6.0 PD and 13.6 ± 10.9 PD (p = 0.04) for distance and 8.7 ± 8.7 PD and 23.4 ± 10.2 PD (p < 0.01) for near, respectively. Postoperative distance deviation (p < 0.05) and near deviation (p < 0.01) were significantly smaller in the slanted group compared to the standard group. The N-D deviation difference of the slanted group (5.9 ± 3.1 PD) was significantly smaller than that of the standard group (9.8 ± 2.7 PD). The results showed that the ratio of postoperative N-D deviation difference/preoperative N-D deviation difference for slanted BLR-rec was 0.44 ± 0.19, whereas for standard BLR-rec was 0.84 ± 0.24. The slanted BLR-rec was able to reduce the N-D deviation difference by an average of 56%, while the standard BLR-rec was only able to reduce the N-D deviation difference by an average of 16%.
In 11 of the 14 cases (79%) in the slanted group and five of the 12 cases (42%) in the standard group, the N-D deviation difference showed improvement to ≤8 PD. In addition, with regard to the angle of near deviation 6 months after surgery, eight of 14 patients (57%) in the slanted group and 0 of 12 patients (0%) in the standard group exhibited successful surgical alignment (Figure 2). In the slanted group, the amount of recession was 6.5 ± 1.0 mm (range: 4.5–8.0 mm) and 8.0 ± 0.7 mm (range: 7.0–9.5 mm) at the upper and lower horns of the LR muscle, respectively. Conversely, the amount of recession in the standard group was 6.9 ± 1.1 mm. The difference between the lower and upper horns of the LR muscle (the difference in the amount of recession) was 1.5 ± 0.5 mm (range 1.0–2.5 mm). Each millimeter of difference between the upper and lower horns of the slanted recessed LR muscle was associated with an improvement of 8.6 PD in the N-D deviation difference for children. No A-V pattern misalignment was observed preoperatively or postoperatively. No patient in either group had an overcorrection (esotropia) of ≥10 PD, torsional effect, or postoperative diplopia six months post-surgery. TNO and Titmus stereo test results, expressed on an interval scale by stereopsis scoring (Table 1), compared pre- and postoperative stereopsis in the slanted and standard groups, respectively. The slanted group had a stereopsis score of 3.9 ± 2.3 preoperatively and 4.7 ± 1.8 postoperatively (p < 0.05) (Table 4). The standard group scored 4.8 ± 1.8 preoperatively and 5.0 ± 1.1 postoperatively. In the standard group, there was no change in stereoacuity pre- and post-operatively, while in the slanted group, stereoacuity was significantly improved compared to that before surgery (p < 0.05, Wilcoxon signed-rank test). Until the last follow-up, none of the patients demonstrated restricted abduction of the eyes, A-V pattern misalignment, torsional diplopia, or consecutive esotropia.
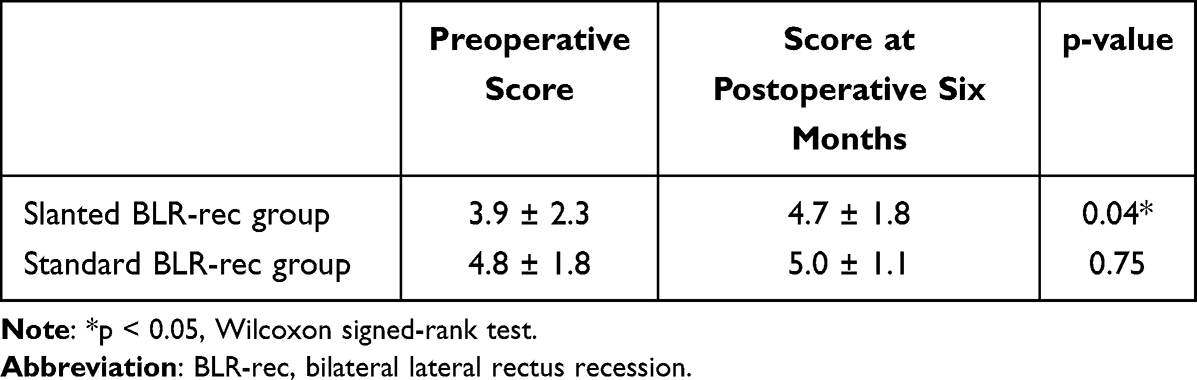 |
Table 4 Stereopsis at Pre- and Post-Operation |
 |
Figure 2 Scatter plot of pre- and postoperative angle deviations. A successful surgical alignment was defined as an exodeviation (exophoria/tropia) of −8.0 PD or less and esodeviation (esophoria/tropia) of +5.0 PD or less in primary gaze while viewing distance or near targets, with an N-D deviation difference ≤ 8 PD. In terms of the angle of near deviation 6 months after surgery, the surgical success rate was 57% (8/14) in the slanted BLR-rec group and 0% (0/12) in the standard BLR-rec group. Abbreviations: BLR-rec, bilateral lateral rectus recession; N-D, near and distance deviation; PD, prism diopter. |
Discussion
Surgery for CI-IXT is less common compared to other exodeviation patterns,3 yet CI-IXT, particularly when associated with reading difficulties and blurred near vision, significantly impacts quality of life. Recognizing the importance of reducing the N-D deviation difference to alleviate these symptoms, we compared slanted BLR-rec surgery with standard BLR-rec. surgery. The results indicate that slanted BLR-rec surgery reduced the N-D deviation difference in CI-IXT, as shown by the comparison of the ratio of the postoperative to preoperative N-D deviation difference with that of the standard BLR-rec surgery (Table 3), making it easier to maintain the phoria at near vision, potentially leading to an improvement in binocular function. In other words, the N-D deviation difference in CI-IXT poses challenges in surgical techniques. Various surgical approaches have been explored to address this issue.3,4,11–14 In 1990, Nemet et al20 performed three patient-biased MR muscle resections, whereby the upper and lower horns of the MR were resected according to the distance and near deviations, respectively, based on Scott’s principle. In 1975, Scott reported that the fibers of the upper and lower horns of the LR muscle were of equal length in the primary ocular position; however, in the downward near gaze (30°) position and at the near position, the upper muscle fibers were lengthened from 40.0 to 41.5 mm, while the lower muscle fibers were reduced from 40.0 to 37.1 mm.21
In our study, we performed slanted BLR-rec in children with CI-IXT, a technique introduced by Snir et al7 based on Scott’s principle.21 Snir et al7 performed bilateral or unilateral slanted surgery on 12 subjects aged 4 to 50 years in 1999 and compared them with a standard surgery group, consisting of six patients aged 6–22 years, who underwent equal-length recession of the upper and lower horns of the LR muscle. Their comparison revealed that slanted LR recession outperformed standard LR recession in reducing both distance and near exodeviation, as well as the N-D deviation difference. Subsequent retrospective clinical studies on the slanted BLR-rec procedure, following Snir et al's6,15,17 work, have consistently demonstrated a reduction in the N-D deviation difference to <8 PD with a 70–80% success rate. Similar to the procedure in previous studies6,7,15,17,18 that involved slanted BLR-rec, the procedure in our study successfully reduced the N-D deviation difference to <8 PD. Because this study was designed as a retrospective cohort study, we confirmed the absence of significant differences in the age at surgery, sex ratio, preoperative follow-up period, and equivalent spherical values between the slanted and standard BLR-rec groups, and the fact that we compared the two groups will contribute to evaluations of the efficacy of slanted BLR-rec.
In addition, in our study, 11 of 14 cases (79%) in the slanted BLR-rec group showed an improved N-D deviation difference of ≤8 PD. This result was in contrast to those of Choi et al,22 who performed slanted bilateral MR resections in 10 patients with CI-IXT and found an N-D deviation difference of <10 PD in only half the patients. This suggests that slanted BLR-rec may be more effective than slanted bilateral MR resection in reducing N-D deviation.
Farid et al16 conducted a prospective study in 2018, where 67 CI-IXT patients were categorized into three groups, and the effects of three surgical methods were compared, including Slanted BLR-rec; New R&R, in which unilateral MR was based on near exodeviation while LR recession was based on the distance exodeviation; and augmented bilateral LR recession (A-BLR), in which LR recession was augmented to the near exodeviation. However, they reported no significant differences among the three groups in terms of distance deviation, near deviation, or N-D deviation difference one year after surgery. Furthermore, they reported that the Slanted BLR-rec group had a vertical pattern of strabismus (A and V pattern), while the New R&R and A-BLR groups had many instances of postoperative overcorrection and under-correction. They considered the cause of the AV phenomenon as a complication of the Slanted BLR-rec procedure. This complication could be attributed to the large N-D deviation difference in the cases recruited in their series. In their study, the following surgical approach was performed: the upper horn of the muscle was recessed based on the distant exodeviation (range: 4 −7.5 mm) and the lower horn of the muscle was recessed according to the near deviation (range: 6–11 mm).
Our series and previous reports6,7,16,18 showed no cases of vertical-pattern strabismus (A and V pattern) postoperative complications. This is because the difference in the amount of recession in our study was 1.5 ± 0.5 mm, and the amount of slant stated by Kwon and Lee17 was 1.7 mm (range, 1–3 mm). We also speculated that the following factors are likely to cause the AV phenomenon as a postoperative complication. If the N-D deviation difference is large, the difference in the recession will inevitably increase, leading to the AV phenomenon.
In contrast, slant BLR-rec is also indicated as a treatment for A and V pattern strabismus without superior and inferior oblique muscle overaction23,24 In the case of A and V pattern strabismus, the difference in the amount of recession was >3–4 mm.24 Therefore, in the treatment of CI-IXT, we assume that the amount of slant should be within 3 mm to avoid postoperative vertical deviation.
We investigated the effect of reducing the N-D deviation difference per 1 mm of the difference in the amount of recession at the lower and upper horns of the LR muscle. In our study, the difference in the amount of recession per 1 mm shortened the N-D deviation difference by 8.6 PD. Similarly, the improvement associated with the difference in the amount of recession on the LR was reported as follows: Snir et al7 4.6 PD/mm; Chun and Kyung,15 8.7 PD/mm; and Ren et al6 5.7 PD/mm. This is because Snir et al and Ren et al included adult cases in the study, whereas Chun and Kyung targeted patients under 12. In comparison, in this study, pediatric patients <15 years were included, which means that the effect of the difference in the amount of recession may differ according to age. In other words, the effect of the difference in the amount of recession may be larger for children than for adults.
This study has some limitations. The sample size was small, with slanted and standard groups including 14 and 12 patients, respectively. In addition, the postoperative follow-up period was short, with six months postoperatively. This study was conducted as a retrospective cohort study, potentially introducing bias through case selection and unmasked outcome examination. Further studies should be conducted to determine the utility of slanted BLR-rec.
Conclusions
In conclusion, the slanted BLR-rec procedure for CI-IXT in children might successfully reduce the N-D deviation difference compared to the standard BLR-rec procedure, without risk of postoperative diplopia. It is possible that the postoperative stereopsis score observed in the slanted BLR-rec group was better than that of the standard BLR-rec group because of the improved N-D deviation difference within this group. This technique may have a positive impact on gross stereopsis.
Abbreviations
CI-IXT, convergence-insufficiency type of intermittent exotropia; PD, prism diopters; MR, medial rectus; ULR, unilateral lateral rectus; APCT, alternating prism cover test; PAT, prism adaptation test.
Data Sharing Statement
All data relevant to the study are included in the article.
Acknowledgments
We would like to extend our special thanks to Ms. Yuko Sasatani at Medical Library, Kyorin University for her invaluable assistance in sourcing and organizing the references essential for this manuscript. Her expertise and support in accessing the necessary literature have greatly contributed to the quality of this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Prof. Dr. Masakazu Yamada reports personal fees from Santen Pharmaceutical Co., Senju Pharmaceutical Co., and Johnson & Johnson Vision Care Company, outside the submitted work. The authors have no other competing interests, including relevant financial interests, activities, and affiliations in this work.
References
1. Burian HM, Spivey BE. The surgical management of exodeviations. Am J Ophthalmol. 1965;59:603–620. doi:10.1016/0002-9394(65)93991-7
2. Burian HM. Exodeviations: their classification, diagnosis and treatment. Am J Ophthalmol. 1966;62(6):1161–1166. doi:10.1016/0002-9394(66)92570-0
3. Kraft SP, Levin AV, Enzenauer RW. Unilateral surgery for exotropia with convergence weakness. J Pediatr Ophthalmol Strabismus. 1995;32(3):183–187. doi:10.3928/0191-3913-19950501-12
4. von Noorden GK. Resection of both medial rectus muscles in organic convergence insufficiency. Am J Ophthalmol. 1976;81(2):223–226. doi:10.1016/0002-9394(76)90735-2
5. Daum KM. Characteristics of convergence insufficiency. Am J Optom Physiol Opt. 1988;65(6):426–438. doi:10.1097/00006324-198806000-00002
6. Ren M, Wang Q, Wang L. Slanted bilateral lateral rectus recession for convergence insufficiency-type intermittent exotropia: a retrospective study. BMC Ophthalmol. 2020;20(1):287. doi:10.1186/s12886-020-01562-2
7. Snir M, Axer-Siegel R, Shalev B, Sherf I, Yassur Y. Slanted lateral rectus recession for exotropia with convergence weakness. Ophthalmology. 1999;106(5):992–996. doi:10.1016/S0161-6420(99)00522-9
8. Birnbaum MH, Soden R, Cohen AH. Efficacy of vision therapy for convergence insufficiency in an adult male population. J Am Optom Assoc. 1999;70(4):225–232.
9. Daum KM. Convergence insufficiency. Am J Optom Physiol Opt. 1984;61(1):16–22. doi:10.1097/00006324-198401000-00003
10. Stavis M, Murray M, Jenkins P, Wood R, Brenham B, Jass J. Objective improvement from base-in prisms for reading discomfort associated with mini-convergence insufficiency type exophoria in school children. Binocul Vis Strabismus Q. 2002;17(2):135–142.
11. Hermann JS. Surgical therapy of convergence insufficiency. J Pediatr Ophthalmol Strabismus. 1981;18(1):28–31. doi:10.3928/0191-3913-19810101-08
12. Choi DG, Rosenbaum AL. Medial rectus resection(s) with adjustable suture for intermittent exotropia of the convergence insufficiency type. J AAPOS. 2001;5(1):13–17. doi:10.1067/mpa.2001.111137
13. Choi MY, Hyung S-M, Hwang J-M. Unilateral recession-resection in children with exotropia of the convergence insufficiency type. Eye (Lond). 2007;21(3):344–347. doi:10.1038/sj.eye.6702197
14. Wang B, Wang L, Wang Q, Ren M. Comparison of different surgery procedures for convergence insufficiency-type intermittent exotropia in children. Br J Ophthalmol. 2014;98(10):1409–1413. doi:10.1136/bjophthalmol-2013-304442
15. Chun B, Kang K. Early results of slanted recession of the lateral rectus muscle for intermittent exotropia with convergence insufficiency. J Ophthalmol. 2015;2015:380467. doi:10.1155/2015/380467
16. Farid MF, Abdelbaset EA. Surgical outcomes of three different surgical techniques for treatment of convergence insufficiency intermittent exotropia. Eye (Lond). 2018;32(4):693–700. doi:10.1038/eye.2017.259
17. Kwon JM, Lee SJ. Long-term results of slanted recession of bilateral lateral rectus muscle for intermittent exotropia with convergence insufficiency. Korean J Ophthalmol. 2019;33(4):353–358. doi:10.3341/kjo.2019.0031
18. Li Y, Lin H. Slanted recession on bilateral lateral rectus for the treatment of intermittent Exotropia with convergence insufficiency. BMC Ophthalmol. 2022;22(1):134. doi:10.1186/s12886-022-02367-1
19. Parks MM. Ocular Motility and Strabismus. Hagerstown: Md. Harper & Row; 1975:99–111.
20. Nemet P, Stolovich C. Biased resection of the medial recti: a new surgical approach to convergence insufficiency. Binocul Vis. 1990;5(4):213–216.
21. Scott AB. Strabismus muscle forces and innervation. In:
22. Choi MY, Hwang J-M. The long-term result of slanted medial rectus resection in exotropia of the convergence insufficiency type. Eye (Lond). 2006;20(11):1279–1283. doi:10.1038/sj.eye.6702095
23. Boyd TA, Leitch GT, Budd GE. A new treatment for ‘A’ and ‘V’ patterns in strabismus by slanting muscle insertions. A preliminary report. Can J Ophthalmol. 1971;6(3):170–177.
24. Ohba M, Nakagawa T. Treatment for “A” and “V” exotropia by slanting muscle insertions. Jpn J Ophthalmol. 2000;44(4):433–438. doi:10.1016/s0021-5155(00)00182-9
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.