")
Back to Journals » Clinical Ophthalmology » Volume 19
Stratified Phacoemulsification Technique to Enhance Safety in Posterior Polar Cataracts
Authors Parkash RO, Parkash TO, Sharma T , Vajpayee RB
Received 21 November 2024
Accepted for publication 12 February 2025
Published 18 February 2025 Volume 2025:19 Pages 571—576
DOI https://doi.org/10.2147/OPTH.S507772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Stratified Phacoemulsification technique in posterior polar cataracts – Video abstract [507772]
Views: 208
Rohit Om Parkash,1 Tushya Om Parkash,1 Trupti Sharma,2 Rasik B Vajpayee3
1Department of Cataract Surgery, Dr Om Parkash Eye Institute, Amritsar, India; 2Department of Cataract Surgery, Dr Om Parkash Eye Institute, Pathankot, India; 3Vision Eye Institute Melbourne, Victoria, Australia; Royal Victorian Eye and Ear Hospital, University of Melbourne, Melbourne, Victoria, Australia
Correspondence: Tushya Om Parkash, Email [email protected]
Purpose: To describe a new technique of stratified phacoemulsification of the nucleus to protect the vulnerable posterior capsule in posterior polar cataracts.
Setting: Dr Om Parkash Eye Institute, Amritsar, India.
Design: Prospective interventional study.
Methods: Twenty-six eyes of twenty-two patients with posterior polar cataracts and nuclear sclerosis of Grade 2 and above, undergoing phacoemulsification surgery, were included in the study. No hydro procedures were performed intentionally to prevent the pressure build-up within the bag or the occurrence of accidental hydrodissection in any of the eyes. Stratified separation was used to separate the nucleus from the surrounding epinucleus mass along natural separational planes in moderate to hard nuclei. Nuclear fragment was emulsified, leaving the epinucleus shell intact. This process of stratified separation and emulsification was repeated for all nuclear fragments without disrupting the epinucleus shell. The epinuclear shell acted as a scaffold and prevented fluidic turbulence and mechanical forces transmission to the fragile posterior capsule. Finally, the epinucleus shell and cortical lens matter were aspirated, and an intraocular lens was implanted.
Results: Our technique of stratified phacoemulsification, which entails chopper-assisted manual delineation of the nucleus, yielded excellent outcomes. Our study included Twenty-six eyes of twenty-two patients with posterior polar cataract and nuclear sclerosis grade 2 or higher. Posterior capsular rupture occurred in one case, which showed pre-existing dehiscence with a moth-eaten appearance on Anterior Segment Optical Coherence Tomography. The pre-existing posterior capsular rent did not result in any intraoperative complications.
Conclusion: The technique of stratified phacoemulsification can achieve safe and successful cataract surgery in posterior polar cataracts with Grade 2 or higher nuclear sclerosis, without the use of hydro maneuvers or expensive femtosecond lasers. The technique entails using standard instruments to form an epinuclear shell that protects the posterior capsule during nuclear emulsification.
Keywords: posterior polar cataract, cataract surgery, phacoemulsification, stratified phacoemulsification, femtodelineation, hydrodelineation
Introduction
Phacoemulsification surgery in posterior polar cataracts is challenging because of the high incidence of posterior capsular dehiscence and associated complications.1 Earlier studies reported posterior capsule rupture rates as high as 36%, underscoring the inherent challenges of posterior polar cataract management.2 However, recent advancements have significantly reduced posterior capsule rupture rates, with contemporary studies reporting incidences as low as 6–7%.3
Improved techniques and technologies have been developed to protect the inherently fragile posterior capsule, adhering to the principles of a closed-chamber technique with stable chamber settings. These methods aim to prevent fluctuations in the anterior chamber, prevent fast hydraulic pressure buildup within the capsular bag, and form a mechanical cushion over the weak capsule.4
Most of these techniques advocate avoiding hydro dissection and performing either conventional hydro delineation or inside-out hydro delineation to prevent a posterior capsule blowout.5 Hydro delineation separates the central nucleus from the epinucleus and prevents fluid from entering the peri cortical space. The separated epinucleus acts as a cushion during nuclear emulsification and minimizes the effects of fluidic and mechanical turbulence on the vulnerable posterior capsule. However, there is no controlling mechanism for fluid used for hydrodelineation, and any excess fluid may enter the pericortical space, resulting in inadvertent hydro dissection. Inside-out hydro delineation provides safe delineation with a minimal predisposition to inadvertent hydro dissection.
Posterior polar cataracts combined with nuclear sclerosis present an even greater challenge because, during hydro delineation, the likelihood of unintentional hydro dissection and posterior capsule rupture is high.6 Therefore, the propensity for posterior capsule dehiscence in such cataracts remains higher.
Femtosecond laser has been used differently to provide an epinuclear shield to protect the posterior capsule by avoiding both hydrodissection and hydro delineation.7,8 Despite providing safe outcomes in posterior polar cataracts, femtosecond laser usage is limited due to its unavailability to all surgeons and the expensive nature of the treatment.
In the present study, we evaluated the technique of stratified phacoemulsification of nucleus in eyes that had posterior polar cataract with significant nuclear sclerosis.
Materials and Methods
Patients with posterior polar cataract as diagnosed on slit lamp evaluation and AS-OCT and with nuclear sclerosis of grade 2 or more undergoing phacoemulsification cataract surgery were enrolled for this prospective interventional study. The institutional review board of Dr Om Parkash Eye Institute approved this study and Informed consent was taken from all patients before the surgery. All the procedures followed ethical standards and principles outlined in the revised Helsinki Declaration of 1983.
Every case underwent a comprehensive ophthalmological evaluation including record of medical history, visual acuity assessment, estimation of intraocular pressure and anterior and posterior segment evaluation. The nucleus grading was done as per LOCS-III classification and retina was examined under dilatation with 78 D lens as well as Indirect Ophthalmoscopy. Other tests that were performed in each eye included, ocular ultrasound, macular OCT, Corneal specular microscopy, Optical Biometry using Zeiss IOL master 700 (Carl Zeiss Meditec AG, Jena, Germany) and Anterion Anterior Segment Optical Coherence Tomography (Heidelberg Engineering GmbH, Heidelberg, Germany).
Morphology of posterior polar cataract was studied on AS- OCT and integrity of the posterior capsule was noted.
Patients with Soft cataracts with nuclear sclerosis of grade 0 and 1, pupil size less than 5.5 mm, corneal pathologies, Endothelial Cell Count less than 1500 cells/mm, ocular co-morbidities like amblyopia, pre-existing glaucoma, pseudoexfoliation syndrome, and retinal diseases like proliferative diabetic retinopathy, macular pathologies, and history of previous ocular surgeries were excluded from the study.
All surgeries were done by a single surgeon (ROP).
Surgery was performed under topical anesthesia using proparacaine eye drops and with complete aseptic precautions. Following the creation of the temporal limbal incision, a side port incision calibrated to the side port instruments was formed to provide stable chamber settings. An anterior capsulorhexis was created using capsulorhexis forceps.9 Hydroxypropyl methylcellulose (Aurolab, Madurai, Tamil Nadu, India) was used as the ophthalmic viscosurgical device (OVD). The Centurion phacoemulsification system (Alcon, Fort Worth, TX, USA) was used with a balanced tip for the surgery. The machine settings were as follows: during sculpting, Intraocular pressure (IOP) was set to 24 mmHg, vacuum to 180 mmHg, aspiration flow rate to 23 cc/min, and torsional ultrasonic mode linear from 20% to 65% with intelligent phaco (IP) off; during quadrant removal, IOP was set to 24 mm Hg, vacuum to 500 mm Hg panel mode, aspiration flow rate to 40 cc/min, and ultrasonic power from 15% to 70% torsional with IP on at 90% occlusion. No hydro procedure were performed in any of the eyes.
Nuclear emulsification was performed using the stop-and-chop technique with low IOP settings.10 After creating a central trench, the nucleus was divided along its entire length into two hemispheres. Subsequently, the nuclear fragment adjacent to the division at the 6 o’clock position relative to the primary incision was cross-chopped, followed by separating the nuclear piece from the epinucleus shell using a blunt chopper (Figure 1).11
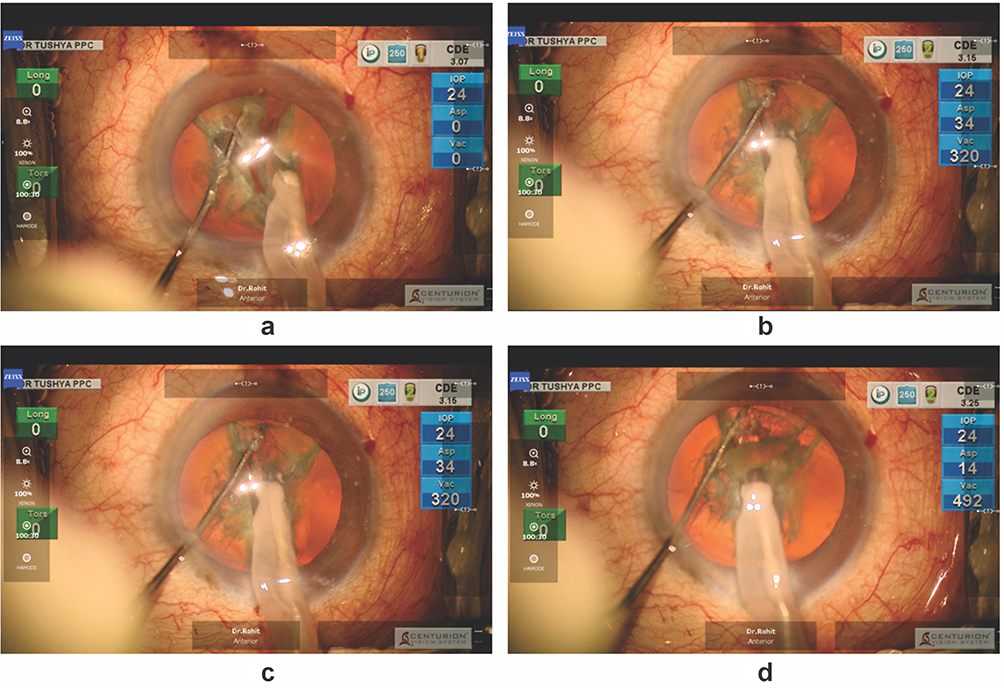 |
Figure 1 (a) Cross chopping done. (b) Nucleus held in the inner harder region and chopper positioned superficially to immobilize the epinucleus. (c) Inner harder nucleus pulled centrally, and chopper superficially immobilizes epinucleus causing initiation of stratified separation. (d) Stratified separation achieved with epinucleus left behind. |
Stratified separation was used for the first time on nuclei of all hardness grades that could be firmly held with the phaco tip. A standard chopper was used to effectively separate the nucleus from the surrounding epinucleus mass. Stratified separation of the nucleus and epinucleus was achieved through two simultaneous maneuvers: the central movement of the firmly held inner nuclear fragment by the phaco tip and the stabilization of the epinucleus by the superficially embedded chopper. This resulted in the effortless splitting of the nuclear-epinuclear mass into the nucleus and epinucleus. Once separated, the nuclear fragment was emulsified, leaving behind the corresponding epinucleus (Figures 1 and 2).
 |
Figure 2 (a) Chopper placed superficially, and nucleus impaled by the phaco tip. (b) stratified separation initiated by two separational forces. (c) Nucleus being emulsified and epinucleus left behind. |
A similar stratified separation was performed on the opposite side adjacent to the division at the 6 o’clock position relative to the primary incision. The nuclear fragment was emulsified, leaving the epinucleus intact. The nuclear-epinuclear masses positioned proximally on both sides were manually delineated in a similar manner, and the separated nuclear fragments were emulsified. At the end of the emulsification of all nuclear fragments, only the epinuclear fragments remained, spread out in all quadrants.
This was followed by aspiration/emulsification of the total epinuclear shell and OVD was injected through the side port to maintain stable chamber settings before removing the phaco handpiece. During irrigation and aspiration, low IOP settings were continued. After completion of aspiration of cortical lens matter, OVD was injected through the side port before removing the IA handpiece to keep the anterior chamber stable A foldable, single-piece IOL was implanted in the bag, and the wounds were sealed stromal hydration.
Results
Twenty-six eyes of twenty-two patients were enrolled for this study. In our series, 22 patients underwent surgery in only one eye. In the Indian context, patients often take time to decide on the timing of surgical intervention for the second eye, leading to delays and progression of nuclear sclerosis in untreated eye. Of these 13 patients were males and 9 were females. The Mean age of the patients was 53.92 years ± 5.7 years with an age range of 43 years to 64 years.
In all eyes, successful phacoemulsification surgery was performed. Except for one case, none of the eyes experienced the complication of an intraoperative posterior capsular rent. The eye that did have a posterior capsular rupture showed a moth-eaten morphology of the posterior capsule during Anterior Segment Optical Coherence Tomography (AS-OCT) examination, indicating the presence of pre-existing posterior capsular dehiscence.12 However, there was no vitreous loss, and Sensar AR40 3-piece IOL was implanted successfully in the sulcus with optic capture in this eye.
All patients achieved excellent visual outcomes with a best corrected visual acuity of 6/6 at 1 month post-operatively. The mean preoperative endothelial cell count was 2402 ± 245.75 cells/mm², while the mean postoperative count was 2310 ± 229.74 cells/mm². The percentage of endothelial cell loss observed at 1 month postoperatively was 3.76% ± 2.31%.
Discussion
Posterior polar cataracts pose a unique challenge to cataract surgeons for their morphological feature of posterior capsular abnormality with a predilection for causing an intra-surgical posterior capsule rupture. Cataract surgeons from various parts of the world have endeavored to develop optimal techniques and surgical protocols to make surgery safe in posterior polar cataracts. Preoperative confirmation of the type of posterior polar cataract and planning with enhanced image quality with AS-OCT, improved techniques of slow motion phacoemulsification using low IOP, creating appropriate capsulorhexis size and shape, avoidance of hydrodissection, escape route, use of stable chamber settings, and improved technology of the use of Femtosecond Laser have been pivotal in reduction of posterior capsular dehiscence and limiting the extent of tears in pre-existing posterior capsular rents.13
One of the critical considerations in posterior polar cataract surgery is the avoidance of hydro dissection, a technique that can lead to hydraulic rupture of the posterior capsule and increase the risk of nucleus drop. Vasavada et al have described hydrodissection as a contraindication in posterior polar cataracts. To mitigate these risks, various alternative techniques of using only hydro delineation of the nucleus have been developed and refined. The enveloping epinucleus following the hydro delineation procedure provides cushion to the posterior capsule, which aids in preventing build-up of hydro pressure in peri cortical space anterior to the posterior capsule, thereby minimizing the occurrence of a posterior capsule rupture in cases of posterior polar cataracts. Furthermore, the epinucleus keeps the bag stretched, thereby decreasing the predisposition of the forward movement of the bag and inadvertent posterior capsule rupture.
Vajpayee et al showcased layer-by-layer hydro delineation to protect the posterior capsule.14 Layer-by-layer hydro delineation provides multiple-layer cushioning and provides protection to the posterior capsule. As compared to the conventional hydro delineation, inside-out hydro delineation technique described by Vasavada et al reduces the risk of inadvertent hydro dissection and undue pressure on the posterior capsule.
Moreover, in posterior polar cataracts with associated significant nuclear sclerosis, hydro delineation may not be completely successful, and multiple attempts to inject fluid into the mass of the nucleus can cause accidental hydro dissection.
To eliminate the possibility of accidental hydro dissection, Femtosecond Laser has been used by different authors to create different layers of the nucleus. The outer epinuclear/nuclear layers provide protection to the vulnerable posterior capsule, thereby decreasing the incidence of posterior capsule dehiscence. Additionally, femtodelineation cushioning has decreased the propensity for posterior capsule rupture enlargement, vitreous loss, and associated complications. However, access to femtosecond lasers may be limited to cataract surgeons in developing countries and is expensive.
The stratified technique of separating the nucleus from the epinucleus, a concept developed by Chee, is straightforward to perform and does not require any additional instruments beyond a phaco needle and a chopper.15 Given that most surgeons are familiar with standard phaco chop procedures, our technique is easy to adopt, reproducible, and involves a minimal learning curve, primarily requiring the phaco tip to be impaled at a slightly deeper plane within the nucleus. The simultaneous central pulling of the nucleus by the phaco tip, combined with the immobilization effort of the superficially embedded chopper, generates forces that effectively separate the epinucleus from the nucleus.
Our stratified phacoemulsification technique is different to the mechanical separation of nuclear lamellae in hard cataracts described by Chee. While her technique is limited to hard cataracts, our study demonstrates that mechanical delineation can also be successfully applied in cases of posterior polar cataracts with moderate nuclear sclerosis. Our simplified technique uses a standard chopper, eliminating the need for a sharp tip and significantly reducing the risk of collateral damage to the capsular rim. Our approach involves a single, straightforward maneuver, embedding the chopper superficially to immobilize the nuclear and epinuclear mass. The separation forces generated by stabilizing the epinucleus and centrally pulling the firmly held nucleus effectively divide the nucleus from the epinucleus.
Recently, Singhal et al have described an innovative manual delineation and dissection technique for posterior polar cataracts.16 Our technique of stratified nuclear emulsification uses the separational forces along the natural cleavage plane to delineate the nucleus into central nucleus and enveloping epinucleus.
To summarize, the stratified phacoemulsification technique of nucleus in posterior polar cataracts with associated nucleus can be used where firm holding of nucleus is possible. Our approach is safe and eliminates the need for hydro maneuvers that can create of undue pressure on the posterior capsule. The innovative simple step of placing a blunt chopper anteriorly to provide immobilization of the epinucleus does not cause any damage to the capsulorhexis edge or other surrounding tissues.
However, stratified phacoemulsification technique has limitations as it cannot be performed in soft cataracts where firm holding of the inner nucleus is difficult.
Conclusion
In conclusion, stratified phacoemulsification in posterior polar cataracts with moderate to hard nuclear sclerosis offers a viable method for delineating the nucleus and creating an epinucleus shield to protect the delicate posterior capsule without the use of hydro procedures and femtosecond laser.
Ethics and Consent Statements
The Ethics Committee of Dr. Om Parkash Eye Institute approved the study before its initiation. The patient’s written informed consent was obtained, and the tenets of the Declaration of Helsinki were followed.
Funding
There was no funding for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Osher RH, Yu BC-Y, Koch DD. Posterior polar cataracts: a pre-disposition to intraoperative posterior capsule rupture. J Cataract Refract Surg. 1990;16:157–162. doi:10.1016/S0886-3350(13)80724-9
2. Vasavada A, Singh R. Phacoemulsification in eyes with posterior polar cataract. J Cataract Refract Surg. 1999;25:238–245. doi:10.1016/S0886-3350(99)80133-3
3. Hayashi K, Hayashi H, Nakao F, Hayashi F. Outcomes of surgery for posterior polar cataract. J Cataract Refract Surg. 2003;29:45–49. doi:10.1016/S0886-3350(02)01692-9
4. Vasavada AR, Vasavada V, Vasavada S, Srivastava S, Vasavada V, Raj S. Femtodelineation to enhance safety in posterior polar cataracts. J Cataract Refract Surg. 2015;41(4):702–707. doi:10.1016/j.jcrs.2015.02.021
5. Vasavada AR, Raj SM. Inside-out delineation. J Cataract Refract Surg. 2004;30:1167–1169. doi:10.1016/j.jcrs.2003.10.034
6. Vasavada AR, Vasavada VA. Managing the posterior polar cataract: an update. Indian J Ophthalmol. 2017;65(12):1350–1358. doi:10.4103/ijo.IJO_707_17
7. Titiyal JS, Kaur M, Sharma N. Femtosecond laser-assisted cataract surgery technique to enhance safety in posterior polar cataract. J Refract Surg. 2015;31:826–828. doi:10.3928/1081597X-20150824-01
8. Sachdev MS, Malik R, Gupta H, Sachdev R, Sachdev GS. Femtosecond laser-integrated anterior segment optical coherence tomography to detect preexisting posterior capsular dehiscence and increase safety in posterior polar cataracts. J Cataract Refract Surg. 2020;46:235–240. doi:10.1097/j.jcrs.0000000000000048
9. Singh KMS, Mittal VMS, Kaur HMS. Oval capsulorhexis for phacoemulsification in posterior polar cataract with preexisting posterior capsule rupture. J Cataract Refract Surg. 2011;37(7):1183–1188. doi:10.1016/j.jcrs.2011.04.017
10. Osher RH. Slow motion phacoemulsification approach [letter]. J Cataract Refract Surg. 1993;195:667. doi:10.1016/S0886-3350(13)80025-9
11. Yeoh R. Cross-chop to the rescue, IIIC symposium APAO symposium ‘The perfect save’.
12. Pujari A, Yadav S, Sharma N, et al. Study 1: evaluation of the signs of deficient posterior capsule in posterior polar cataracts using anterior segment optical coherence tomography. J Cataract Refract Surg. 2020;46(9):1260–1265. doi:10.1097/j.jcrs.0000000000000246
13. Osher RH, Amaral HL. The escape route: novel surgical technique for the posterior polar cataract. J Cataract Refract Surg. 2022;48(11):1233–1234. doi:10.1097/j.jcrs.0000000000001004
14. Vajpayee RB, Sinha R, Singhvi A, Sharma N, Titiyal JS, Tandon R. ‘Layer by layer’ phacoemulsification in posterior polar cataract with pre-existing posterior capsular rent. Eye. 2008;22:1008–1010. doi:10.1038/sj.eye.6702795
15. Chee SP. Management of the hard posterior polar cataract. J Cataract Refract Surg. 2007;33(9):1509–1514. doi:10.1016/j.jcrs.2007.05.027
16. Singhal L, Sood G. Manual-delineation and hydrodissection technique for posterior polar cataract. JCRS Online Case Rep. 2024;12(4):e00123. doi:10.1097/j.jcro.0000000000000123
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.