")
Back to Journals » Clinical Ophthalmology » Volume 19
Sub-Tenon’s versus Topical Anesthesia for Effectiveness of Analgesia During Cataract Surgery: A Systematic Review with Meta-Analysis
Authors Valizadeh G , Duong E, Thang C, White LD
Received 18 January 2025
Accepted for publication 11 April 2025
Published 2 May 2025 Volume 2025:19 Pages 1475—1487
DOI https://doi.org/10.2147/OPTH.S512750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ghazal Valizadeh,1,2 Elliot Duong,3 Christopher Thang,2– 4 Leigh D White3,4
1Department of Ophthalmology, Princess Alexandra Hospital, Woolloongabba, Queensland, Australia; 2Faculty of Medicine, University of Queensland, Herston, Queensland, Australia; 3Department of Anesthesia and Perioperative Medicine, Sunshine Coast University Hospital, Birtinya, Queensland, Australia; 4School of Medicine, Griffith University, Birtinya, Queensland, Australia
Correspondence: Ghazal Valizadeh, Department of Ophthalmology, Princess Alexandra Hospital, Woolloongabba, Queensland, Australia, Email [email protected]
Background: Sub-Tenon’s and topical anesthesia are the most common anesthetic techniques employed for cataract surgery. The objectives were to compare the effectiveness of intraoperative analgesia between the two techniques.
Methods: A systematic review was performed of three databases (MEDLINE, EMBASE, CENTRAL) from inception until August 2023. Included were adult patients undergoing routine cataract surgery with sub-Tenon’s or topical anesthesia. Excluded were studies using systemic medications and complicated surgeries. The primary outcome was intraoperative analgesia assessed by patient reported pain scores. Secondary outcomes were post-operative pain at 30 minutes and 24 hours, patient satisfaction, surgeon satisfaction and complications. Risk of bias was evaluated using the revised Cochrane risk-of-bias tool for randomized trials (RoB 2). Outcomes were statistically assessed with meta-analyses where able.
Results: Twelve studies with 1370 patients were included in the meta-analysis. Sub-Tenon’s block provided better intraoperative analgesia with lower pain scores (SMD − 0.53, 95% CI − 0.70 to − 0.36; p < 0.001) which remained significant on subgroup analysis of six studies with uniform pain scales (MD − 0.84, 95% CI − 1.22 to − 0.47; p < 0.001). Instances of severe intraoperative discomfort requiring rescue regional anesthesia were reported with topical anesthesia. While there was no difference in pain scores at 30 minutes or 24 hours post-operatively, higher patient and surgeon satisfaction was found with sub-Tenon’s anesthesia. Serious complications were rare, with a higher reported rate of posterior capsule rupture with topical anesthesia. Only two of fourteen studies were considered an overall low risk-of-bias.
Conclusion: Sub-Tenon’s block provides marginally better intraoperative analgesia during cataract surgery over topical anesthesia. Both can be considered effective for uncomplicated cataract surgery.
Keywords: sub-Tenon’s, topical anesthesia, regional anesthesia, cataract surgery
Background
Cataract surgery is usually performed under local anesthesia with or without sedation in the ambulatory setting.1 A cataract is a clouding of the eye’s natural lens and is the leading cause of blindness worldwide.2 With the advent of minimally invasive surgical techniques, there has been a notable shift in anesthetic practice away from traditional peribulbar and retrobulbar blocks, towards sub-Tenon’s blocks and topical anesthesia drops.3 This has perceived advantages in avoiding risks associated with “needle” techniques near the orbit which include potentially sight and life-threatening complications. The choice of anesthesia for cataract surgery is variable, depending on patient factors including cooperation and medical comorbidities, surgeon preference and resource availability.1,3 Regardless of the local anesthetic technique employed, maintaining adequate analgesia and optimizing surgical conditions while minimizing complications is fundamental.
The sub-Tenon’s technique uses a blunt, angulated needle to access and deposit local anesthetic in the potential space deep to Tenon’s fascia.4 Topical anesthesia involves non-invasive application of local anesthetic, in drop or gel form, on the surface of the eye and may have benefits over sub-Tenon’s anesthesia due to faster administration time and reduced pain during administration.1 Topical anesthesia may be augmented intraoperatively with intracameral anesthesia, consisting of injection of local anesthetic into the anterior chamber of the eye with a blunt needle through a corneal incision.1 The use of topical anesthesia however may be associated with increased pain intra-operatively.1 The preference for topical or sub-Tenon’s anesthesia varies internationally, with a recent review of the European Registry of Quality Outcomes for Cataract and Refractive surgery noting a trend towards increasing topical anesthesia use (from 30% to 76%) and decreasing sub-Tenon’s anesthesia use (from 27% to 16%) across 1.3 million patients over 11 years.5 Conversely, in North America the use of sub-Tenon’s anesthesia increased from 31% in 2010 to 61% in 2018.6 Controversy remains regarding the safety profiles of each technique. Although sub-Tenon’s block uses a blunt needle, surface dissection is required to access the sub-Tenon’s space, leading to the potential risk of infection and orbital hemorrhage.5 In comparison, the lack of akinesia associated with topical anesthesia may increase the risk of patient movement and iatrogenic surgical injury, however this has not been shown on meta-analysis.7
There have been two systematic reviews comparing topical anesthesia with sub-Tenon’s block. The most recent systematic review published by Guay et al in 2015 found that sub-Tenon’s block provided better intraoperative analgesia, measured by a difference in pain scores of 1.1 on a 0–10 visual analogue scale (VAS).1,8 The results of this review were limited by the quality of included trials, consisting of only seven randomized controlled trials (RCTs). On subgroup analysis of low risk of bias, three RCTs demonstrated an analgesic benefit with sub-Tenon’s block over topical drops with a standardized mean difference (SMD) of 0.47, 95% CI 0.29 to 0.66.1 Furthermore, there were limited studies investigating patient or surgical satisfaction and not enough evidence to compare complication risk profiles.
The primary objective of this review was to compare topical anesthesia with sub-Tenon’s anesthesia in providing analgesia during cataract surgery. We also reviewed post-operative pain scores at defined time intervals, surgeon satisfaction and rates of associated complications.
Methods
Electronic Searches
This systematic review was prospectively registered on Prospero (CRD 42023543968). A search was performed through the MEDLINE (EBSCOHost), EMBASE and Cochrane Central Register of Controlled Trials (CENTRAL) electronic databases using the key concepts cataract surgery, sub-Tenon’s block and topical anesthesia (Appendices 1–3). The databases were searched from inception until the 14th of August 2023 using controlled vocabulary for each database where relevant. The Cochrane Highly Sensitive RCT filter9 was used for MEDLINE and the adapted Cochrane EMBASE RCT filter10 was used for the Embase.com interface. There were no restrictions on language or publication status. A manual citation search was performed of all included studies. Grey literature was searched through Open Grey as well as Google Scholar. Two authors independently performed title and abstract screening, with full-text copies obtained and assessed where required, and any disagreements were resolved through consensus or assessment by a third reviewer at each stage.
Eligibility Criteria
Two reviewers independently assessed studies for inclusion against eligibility criteria. Eligible studies were prospective RCTs comparing intraoperative analgesia in sub-Tenon’s anesthesia versus topical anesthesia (with or without intracameral injection) for adults undergoing cataract surgery. This included any combination of topical anesthetic drops or gel, local anesthetics with or without hyaluronic acid and whether the block was performed by the anesthetist or surgeon. Where there was disagreement between reviewers, they were resolved by a third reviewer.
Exclusion Criteria
Retrospective, case control and cohort trials were excluded. Studies where systemic sedation or anesthesia was provided were excluded given the inability to accurately assess intraoperative patient analgesia. We also excluded any studies assessing secondary or revision cataract surgeries and pediatric or animal populations.
Outcomes
The primary outcome assessed was intraoperative analgesia during cataract surgery which was measured using a pain score. Intraoperative pain scores were collected both during the procedure and immediately following the conclusion of the operation, depending on the included study. Secondary outcomes included pain during administration of local anesthesia, pain scores at 30 minutes and 24 hours post-operatively, patient satisfaction, surgeon satisfaction and patient compliance, operating time and complications that occurred as defined by study authors.
Data Collection and Extraction
Two reviewers independently extracted data from each study which met the inclusion criteria. Collected data was assessed for homogeneity and any discrepancies were reviewed. The original authors of eligible studies were contacted where required to obtain additional information. Data extracted from each study included patient demographics, type of local anesthesia used, study methodology, intraoperative pain scores, post-operative pain scores at defined intervals, surgeon satisfaction, patient compliance, operating time and complications.
Risk of Bias
Studies were assessed for risk of bias and methodological quality using the revised Cochrane Collaboration’s tool for assessing risk of bias (RoB 2).11,12 Two review authors independently assessed risk of bias for each study and any disagreements were resolved via a third author.
Statistical Analysis
Statistical analysis was performed using RevMan 5.3 (The Nordic Cochrane Centre, Copenhagen, Denmark). Statistical heterogeneity was quantified using the I2 statistic as either low (I2 < 25%), moderate (I2 = 25–74%) or high (I2 ≥ 75%). For continuous data, an inverse variance random-effects model was used for comparisons with moderate or high heterogeneity as quantified by the I2 statistic, while a fixed-effects model was used for comparisons with low heterogeneity. For dichotomous outcomes, the Mantel–Haenszel fixed effect method was used. Results for continuous data using different pain scales were assessed using standardized mean difference (SMD) summary statistics (Cohen’s d). A SMD of 0.2 was considered a small effect size, 0.5 was considered a medium effect size and ≥0.8 considered a large effect size.13 A sensitivity analysis was performed for studies using a 0–10 pain scale to assess for any difference in effect. Studies which did not provide a standard deviation were estimated using the formula set out by Hozo et al or calculated from raw data sets provided by study authors.14
Results
Electronic searches identified 5320 citations and a further one study was identified through grey literature searches. No ongoing clinical trials were found. After title and abstract screening a total of 22 full manuscripts were reviewed, of which 14 were eligible for inclusion. The PRISMA flow diagram for this review (Figure 1) demonstrates the studies identified, included, excluded and reasons for exclusion.15 In total, 14 studies with 1493 patients were included which are summarized in Table 1.16–29 Two RCTs comparing topical and sub-Tenon’s anesthesia were excluded due to the adjunctive use of systemic sedation. Details of the excluded studies are available in Supplement 1.
 |
Table 1 Characteristics of Included Studies |
 |
Figure 1 PRISMA flow diagram. |
Primary Outcome
Twelve studies, including a total of 1370 participants, assessed the primary outcome of analgesia intraoperatively.16–23,26–28 Sub-Tenon’s block provided better intraoperative analgesia compared to topical anesthesia demonstrated by lower pain scores (SMD −0.53, 95% CI −0.70 to −0.36; p < 0.001; I2 = 51%; medium effect size) (Figure 2). This equated to a mean difference of 1.18 on a 0–10 scale when standardized to a high-quality study (Srinivasan et al).26 Six of these studies17,19–21,26,28 assessed intraoperative analgesia using a pain scale from 0 to 10 while the remainder used a variety of alternative scales.16,18,22,23,27,29
 |
Figure 2 Forest plot of sub-Tenon’s versus topical anesthesia in providing intraoperative analgesia for all included studies using SMD. |
One study could not be included in the meta-analysis due to data unavailability.25 This study assessed pain outcomes during routine cataract surgery in 100 patients randomized to receiving either xylocaine jelly and intracameral lignocaine or one quadrant of sub-Tenon’s infiltration with 2mL of lignocaine 2%. It is of note that the cataract surgeries in this study were performed through a 6 mm sclero-corneal incision which has largely been replaced by clear corneal incisions. The median overall subjective pain score measured used a VAS immediately post-operatively, was significantly higher in the topical group compared to the sub-Tenon’s group (p < 0.001).
A sensitivity analysis was performed using six studies, consisting of 657 patients, with the same 0–10 pain scale.17,19–21,26,28 Again, Sub-Tenon’s anesthesia provided better analgesia intraoperatively (mean deviation (MD) −0.84, 95% CI −1.22 to −0.47; p < 0.001; I2 = 58%) (Figure 3). One study which reported a 0–10 pain scale could not be included in this sensitivity analysis as unpublished data subsequently obtained from the authors showed a pain scale of 1–10 was used rather than the reported 0–10 scale.27
 |
Figure 3 Forest plot of sub-Tenon’s versus topical anesthesia in providing intraoperative analgesia for all studies using a 0–10 pain scale. |
A sensitivity analysis for the type of surgical technique was also performed. Sub-Tenon’s anesthesia was found to provide better intraoperative analgesia regardless of whether a scleral tunnel incision (three studies including 135 patients; SMD −0.91, 95% CI −1.26 to −0.55; p < 0.001) or clear corneal incision (six studies including 856 patients; SMD −0.44, 95% CI −0.58 to −0.30; p < 0.001) was used.
In Sekundo et al’s study, there was a particularly high attrition rate from the topical anesthetic group, with 5 patients (10%) reporting unbearable intraoperative pain requiring additional sub-Tenon’s block to complete the surgery (notably via a sclero-corneal incision).25 In another study, one patient out of thirteen (7.7%) in the topical anesthetic group expressed severe pain requiring conversion to intravenous sedation (midazolam) and administration of a peribulbar block.24
Secondary Outcomes
Pain During Administration of Local Anesthetic
Six studies, including 1002 participants, investigated pain during the administration of local anesthetic.16,20,23,26–28 There was no significant difference in pain during administration of anesthesia (SMD 0.57, 95% CI −0.04 to 1.18; p = 0.06; I2 = 95%), although there was a trend towards reduced pain during administration of topical anesthesia (Figure 4).
 |
Figure 4 Forest plot of pain during administration of sub-Tenon’s versus topical anesthesia in cataract surgery. |
Although Nielsen et al reported outcomes on pain during local anesthetic administration, it could not be included in this meta-analyses due to insufficient data.22 In their study, they reported a higher mean pain score in the sub-Tenon’s group (1.48) compared to the topical anesthetic group (0.14) on a scale of 0–10.22
Post-Operative Pain at 30 minutes and 24 hours
Four studies which included 728 participants investigated pain post-operatively at 30 minutes.23,26–28 Meta-analysis revealed a trend towards enhanced analgesia with sub-Tenon’s block at 30 minutes, however this result was not statistically significant (SMD −0.40, 95% CI −0.85 to 0.06; p = 0.09; I2 = 89%) (Figure 5).
 |
Figure 5 Forest plot of post-operative pain at 30 minutes for sub-Tenon’s versus topical anesthesia in cataract surgery. |
Only one study investigated post-operative pain at 24 hours. In this study of 200 patients, the mean pain score on a scale of 0–10 was greater in the sub-Tenon’s group (pain score of 0.23 ± 0.40) compared to the topical anesthesia group (pain score of 0; p < 0.01).28
Patient Satisfaction
Five studies including 331 participants reported outcomes on patient satisfaction.19,22,24,27,29 Due to the variations in methodology used to assess and report patient satisfaction, meta-analysis was not performed. Three studies showed an increase in patient satisfaction with sub-Tenon’s anesthesia while the remaining two studies found no difference.
Ruschen et al investigated patient satisfaction using an Iowa Satisfaction with Anesthesia Scale (ISAS), giving an overall score of −3 (totally dissatisfied) to +3 (completely satisfied) comparing sub-Tenons block with topical anesthesia drops in 28 patients.24 The analysis showed a significant difference in patient satisfaction (p < 0.0085), with higher scores obtained with the sub-Tenon’s block group (median score 2.77; IQR 2.45 to 3) compared to topical anesthesia (median score 2.04; IQR 1.54 to 2.50).
Vielpeau et al had a unique method of assessing patient satisfaction.29 This study was restricted to patients undergoing bilateral cataract surgery who received sub-Tenon’s anesthesia in one eye followed by topical anesthesia in the contralateral eye. Patient satisfaction was then measured by asking which method of anesthesia was preferred. Sixty-four percent of patients indicated a preference for sub-Tenon’s block compared to 8% of patients who favored topical anesthesia, while 28% did not express a preference.29
In a study by Nielsen et al, patients undergoing bilateral cataract surgery received either topical anesthesia, sub-Tenon’s or a peribulbar block.22 Sixteen percent (7/44) of patients stated they would not have a sub-Tenon’s block again compared to 19% (8/43) of patients who would not have topical anesthesia again. Reduced intraoperative awareness of surgery was the main reason stated by patients for this preference of sub-Tenon’s over topical anesthesia.22
In Teh et al’s study, extra unpublished data provided from the authors showed that all 118 patients receiving either sub-Tenon’s or topical anesthesia would keep the same “choice of anesthesia during the next operation”.27 Likewise, in the study by Manners et al, all patients were reported to have been satisfied with their mode of anesthesia.19
Surgeon Satisfaction and Patient Compliance
One study addressed surgeon satisfaction directly, while two studies examined the rates of patient compliance or non-compliance. In a study of 200 participants, Zafirakis et al assessed surgeon satisfaction directly through surgeon ratings of patient cooperation on a scale of 2.5 to 10, with 2.5 being poor and 10 being excellent.28 They found a significant difference favoring cooperation in the sub-Tenon’s group (9.63 ± 0.96) over the topical anesthetic group (8.93 ± 1.78; p < 0.01). In comparison, Nielsen et al described a surgeon-reported patient non-compliance rate of 18% in both the sub-Tenon’s and topical anesthetic groups in a study of 86 participants.22 Similarly, the operating surgeon in Rashmi et al’s study reported that the majority of patients in both local anesthetic groups (77% for sub-Tenon’s anesthesia and 79% for topical anesthesia) were significantly co‐operative.23
Operating Time
Five studies reported on mean operating time for cataract surgery after sub-Tenon’s or topical anesthesia was administered.18,19,22,24,28 Meta-analysis of these studies was performed to investigate procedural time and where standard deviation was unavailable, the standard deviation was calculated from ranges or imputed based on the average standard deviation of the other studies (Supplements 2 and 3). The mean procedural time was shorter in the topical group when compared to the sub-Tenon’s group (MD 1.02 min, 95% CI 1.02 to 5.42; p = 0.01; I2 = 21%). The average weighted procedural time for cataract surgery was 12.96 minutes in the topical anesthesia group and 13.97 minutes in the sub-Tenon’s group, equating to a 7.2% reduction in operating time.
Complications
Subconjunctival hemorrhage and chemosis were reported in five studies (Table 2).19,22,23,28,29 Five studies did not comment on complications.16–18,20,27 Srinivasan et al reported posterior capsular tear at a rate of 2.1% for sub-Tenon’s anesthesia (2/136) and 4.3% for topical anesthesia (3/65).26 They also reported one case (0.5%) of iris prolapse in the sub-Tenon’s group (1/136) and none in the topical anesthesia group. Nghiem-Buffet et al also reported one incident of capsular rupture in the topical anesthesia group (2.3%).21
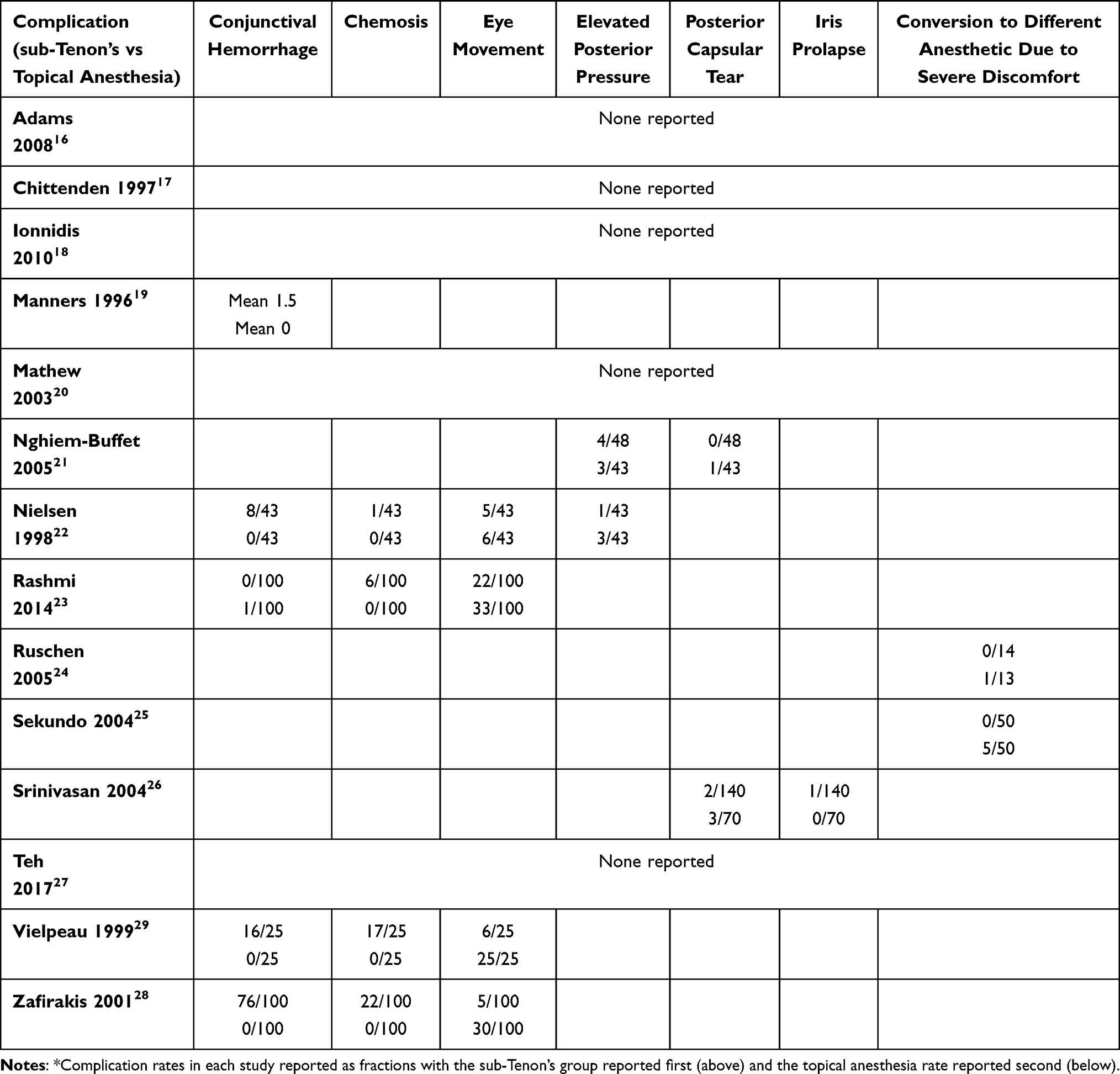 |
Table 2 Documented Complications for Sub-Tenon’s versus Topical Anesthesia |
Risk of Bias
The risk of bias and methodological quality for the included studies was assessed using the Cochrane Collaboration’s Tool for risk of bias (RoB 2) (Figures 6 and 7).12 Two studies (Rashmi et al and Srinivasan et al) were assessed to have an overall low risk of bias.23,26
 |
Figure 6 Summary of risk of bias domains presented as percentages across all included studies. |
 |
Figure 7 Summary of each risk of bias item for all included studies. |
Discussion
This systematic review included 14 RCTs comparing intraoperative analgesia with sub-Tenon’s versus topical anesthesia in routine cataract surgery. Twelve of these studies were included for meta-analyses of the primary outcome of intraoperative analgesia. The results suggest that sub-Tenon’s blocks provide better intraoperative analgesia compared to topical anesthesia for cataract surgery. This finding was found to be statistically significant (SMD −0.53, 95% CI −0.70 to −0.36; p < 0.001; I2 = 51%), representing a VAS reduction of 1.18 (on a scale of 0–10) when standardized to the one high-quality study which used a VAS 0–10 pain scale.26 To assess for robustness in this finding, a sensitivity analysis was performed with studies using a 0–10 VAS, which also showed a significant analgesic benefit with sub-Tenon’s anesthesia (MD −0.84, 95% CI −1.22 to −0.47; p < 0.001; I2 = 58%).
The findings of the primary outcome in this study are consistent with previous systematic reviews.1,8 A systematic review by Guay et al which analyzed six studies for the outcome of intraoperative analgesia, found a statistically significant reduction in pain scores favoring sub-Tenon’s anesthesia (SMD 0.64, 95% CI 0.43 to 0.84; I2 = 36%).1 Although the observed difference was statistically significant in this review, the clinical relevance was not obvious. Our review found an additional six studies for inclusion in the primary outcome, thereby enhancing the statistical power of our findings. Notably, we found a clinically meaningful incidence of severe pain (7–10%) in the topical anesthesia group across two studies, requiring conversion to a regional block technique and the administration of systemic sedation.
This review also investigated several secondary outcomes including reduction in pain scores at 30 minutes and 24 hours, as well as patient satisfaction. On meta-analysis of four studies, there was no significant difference in pain scores between the two groups at 30 minutes, although sub-Tenon’s block was favored. Additional marginal benefits associated with sub-Tenon’s anesthesia were increases in patient and surgeon satisfaction, however there was an inadequate number of studies to run a meta-analysis on these outcomes.
Of the studies that reported rates of minor complications such as chemosis and subconjunctival hemorrhage, a higher incidence was found in the sub-Tenon’s group compared to the topical anesthesia group. Expectedly, this result is due to tissue damage during surface dissection in sub-Tenon’s blocks in order to access the sub-Tenon’s space. In contrast, in all four studies that commented on intraoperative motor blockade of the eye, there was a higher rate of eye movement during surgery with topical anesthesia, leading to a theoretically higher rate of serious complications such as posterior capsular rupture.22,23,28,29
Major complications were rare with eight studies reporting no major complications. Two studies reported incidences of posterior capsular rupture and in both studies the rate was higher in the topical anesthetic group.21,26 Supporting these findings, a recent retrospective cross-sectional register-based study of 1,354,036 cataract surgeries showed an increased risk of posterior capsular rupture, with or without dropped nucleus, with topical anesthesia compared to sub-Tenon’s anesthesia (odds ratio (OR) 0.74, 95% CI 0.71 to 0.78; p < 0.001).5 Associated was a statistically significant increase in the rate of endophthalmitis for topical compared to regional anesthesia techniques (peribulbar or retrobulbar blocks) (OR 0.60, 95% CI 0.44 to 0.82; p = 0.001), however statistical significance was not maintained when compared to sub-Tenon’s anesthesia (OR 0.81, 95% CI 0.62 to 1.06; p = 0.126).5 In this systematic review, while cases of posterior capsular rupture were reported at a higher rate in the topical anesthesia group, there were no reported cases of endophthalmitis. Given posterior capsular rupture is a notable risk factor of endophthalmitis, future prospective RCTs are required to investigate this risk in topical versus sub-Tenon’s anesthesia.5
There were six trials in our review which assessed patient pain during administration of anesthesia.16,20,23,26–28 Although there was a trend towards increased pain with sub-Tenon’s compared to topical anesthesia, this did not reach statistical significance. It is worth noting that as part of the inclusion criteria, all blocks were done in the absence of intravenous sedation or systemic analgesia. The use of systemic sedation or analgesia is commonplace in many countries and use of these medications in clinical practice may help alleviate the discomfort experienced by patients’ during the administration of anesthesia.5 Any potential increase in pain during anesthetic administration needs to be weighed against the higher rate of severe intraoperative discomfort requiring conversion to another anesthetic technique or administration of intravenous medications in the topical group as reported by both Ruschen et al and Sekundo et al24,25 Notably, there was no difference in the number of patients reporting that they would not have a sub-Tenon’s block compared to topical drops again.
Our review found a minor decrease in operating time of 1.02 minutes with the use of topical anesthesia compared to sub-Tenon’s anesthesia, which was found to be statistically significant on meta-analysis (MD 1.02 min, 95% CI 1.02 to 5.42; p = 0.01; I2 = 21%). The clinical significance of this amount of time reduction, however, is likely limited. Cataract surgery is one of the most common surgical procedures in the world with more than 26 million cataract surgeries performed annually and a cost-effectiveness similar to knee arthroplasties.30 Further studies and an in-depth economic analysis would need to be undertaken to establish any economic benefit for use of topical anesthesia over sub-Tenon’s blockade.30
Studies show a multitude of different factors influence a patient’s perception of pain intraoperatively which are distinct from the surgery and type of anesthetic itself. A systematic review by Obuchowska et al found that appropriate patient selection and pre-operative counselling was found to decrease rates of peri-operative anxiety.31 Further to this, an observational masked study by Socea et al found that pre-operative anxiety levels are a significant predictor of intraoperative pain for cataract surgery.32 Obuchowska et al reported that non-pharmacological methods such as hand-massage and music were effective in reducing intraoperative anxiety and pain sensations, respectively, highlighting the importance of a holistic approach to reducing pain perception.31
Limitations
The strengths and weaknesses of each included study is summarized in Figure 7. In total, two studies were deemed to have an overall low risk of bias as measured by the Cochrane risk of bias tool.23,26,27 Srinivasan et al was set as the reference high-quality study to which our findings were scaled, as it was the only high-quality study using a 0–10 VAS scale. Major limitations amongst the remainder of included studies were a lack of blinding through use of a placebo as well as incomplete descriptions of randomization. Teh et al was initially assessed to have an overall low risk of bias, however, after obtaining additional unpublished data from the authors, it was found that pain scores were reported on a 1–10 pain scale instead of the 0–10 pain scale published in their study.27 As a result, their overall risk of bias was downgraded from low to some concerns for risk of bias.
Assessment of the secondary outcome of patient satisfaction was limited by the lack of uniform assessment methods across the different studies. As such, meta-analysis and statistical analysis proved difficult. Despite this, three of the studies showed a patient preference for sub-Tenon’s over topical anesthesia. Overall, there was a wide range of different medications used for both the topical application of anesthesia as well as within the sub-Tenons’ blocks. Only one study included in the meta-analysis used intracameral anesthesia in combination with topical anesthesia.18 In clinical practice, supplementation of topical anesthesia with intracameral medication is commonplace and further studies are required to compare analgesic outcomes of topical anesthesia with and without intracameral anesthesia with sub-Tenon’s blocks.5 For the purposes of this review, we assumed that all doses and types of local anesthetics used were suitable for their intended purpose of intraoperative analgesia for cataract surgery. There was no mention of inadequate dosing for local anesthetics used in any of the studies included in this review. Comparison of the effectiveness of the different types of local anesthetics used was outside the scope of this review.
Conclusions
This systematic review found a statistically significant reduction in patient reported pain scores with sub-Tenon’s anesthesia compared to topical anesthesia in routine cataract surgery, equating to a difference of 1.18 on a VAS pain scale of 0–10. While statistically significant, the clinical relevance of these scores in isolation may not be large enough to warrant a complete change in practice and therefore, both techniques can be considered effective for use in cataract surgery. Notably, however, there were several instances of intraoperative discomfort requiring rescue regional anesthesia in the topical group. There was a trend towards higher patient and surgeon satisfaction in the sub-Tenon’s group, as well as decreased rates of serious complications, however variations in methodology between studies did now allow meta-analyses of these outcomes and these outcomes did not reach statistical significance. The findings from this review show that sub-Tenon’s anesthesia has a modest intraoperative analgesic benefit in clinical practice when compared to topical anesthesia for use in routine cataract surgery.
Acknowledgments
The review was registered prospectively on Prospero (CRD 42023543968). The authors declare that aspects of this study have been presented at the 2024 Royal Australian and New Zealand College of Ophthalmologists annual conference.
Funding
None to declare. There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Guay J, Sales K. Sub-tenon’s anesthesia versus topical anesthesia for cataract surgery. Cochrane Database Syst Rev. 2015;2015(8):CD006291. doi:10.1002/14651858.CD006291.pub3
2. Fang R, Yu YF, Li EJ, et al. Global, regional, national burden and gender disparity of cataract: findings from the global burden of disease study 2019. BMC Public Health. 2022;22(1):2068. doi:10.1186/s12889-022-14491-0
3. Guise P. Sub-tenon’s anesthesia: an update. Local Reg Anesth. 2012;5:35–46. doi:10.2147/LRA.S16314
4. Stevens JD. A new local anesthesia technique for cataract extraction by one quadrant sub-tenon’s infiltration. Br J Ophthalmol. 1992;76(11):670–674. doi:10.1136/bjo.76.11.670
5. Segers MHM, Rosen P, van den Biggelaar F, et al. Anesthesia techniques and the risk of complications as reflected in the European Registry of Quality Outcomes for Cataract and Refractive Surgery. J Cataract Refract Surg. 2022;48(12):1403–1407. doi:10.1097/j.jcrs.0000000000001009
6. Chua MJ, Lersch F, Chua AWY, Kumar CM, Eke T. Sub-tenon’s anesthesia for modern eye surgery-clinicians’ perspective, 30 years after re-introduction. Eye. 2021;35(5):1295–1304. doi:10.1038/s41433-021-01412-5
7. Lee RMH, Foot B, Eke T. Posterior capsule rupture rate with akinetic and kinetic block anesthetic techniques. J Cataract Refract Surg. 2013;39(1):128–131. doi:10.1016/j.jcrs.2012.11.002
8. Davison M, Padroni S, Bunce C, Rüschen H. Sub-tenon’s anesthesia versus topical anesthesia for cataract surgery. Cochrane Database Syst Rev. 2007;3:CD006291. doi:10.1002/14651858.CD006291.pub2
9. Lefebvre C, Manheimer E, Glanville J. Chapeter 6: searching for studies. In: Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration; 2011.
10. Glanville J, Foxlee R, Wisniewski S, Noel-Storr A, Edwards M, Dooley G. Translating the Cochrane Embase RCT filter from the Ovid interface to Embase.com: a case study. Health Info Libr J. 2019;36(3):264–277. doi:10.1111/hir.12269
11. Higgins J, Green S, Altman G. Chapter 6: searching for studies. In: Cochrane Handbook for Systematic Reviews of Interventions Version. 2021; Vol. 5.
12. Sterne JAC, Savovic J, Page MJ, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
13. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
14. Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:13. doi:10.1186/1471-2288-5-13
15. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269. doi:10.7326/0003-4819-151-4-200908180-00135
16. Adams W, Vaideanu D, Fraser S, Bell R. Comparison of anesthetic methods for phacoemulsification using the McGill pain questionnaire. Invest Ophthalmol Vis Sci. 2008;49(13):5670.
17. Chittenden HB, Meacock WR, Govan JA. Topical anesthesia with oxybuprocaine versus sub-tenon’s infiltration with 2% lignocaine for small incision cataract surgery. Br J Ophthalmol. 1997;81(4):288–290. doi:10.1136/bjo.81.4.288
18. Ioannidis AS, Papageorgiou K, Alexandraki KI, Massaoutis P, Sinha AJ, Andreou PS. Light sensitivity and pain sensation during cataract surgery. A comparative study of two modes of anesthesia. Int Ophthalmol. 2010;30(6):703–707. doi:10.1007/s10792-010-9344-5
19. Manners TD, Burton RL. Randomised trial of topical versus sub-tenon’s local anesthesia for small-incision cataract surgery. Eye. 1996;10(3):367–370. doi:10.1038/eye.1996.75
20. Mathew MR, Williams A, Esakowitz L, Webb LA, Murray SB, Bennett HG. Patient comfort during clear corneal phacoemulsification with sub-tenon’s local anesthesia. J Cataract Refract Surg. 2003;29(6):
21. Nghiem-Buffet MH, Sonigo B, Fajnkuchen F, Chaine G. Topical versus sub-tenon’s anesthesia without sedation in clear corneal cataract surgery. Invest Ophthalmol Vis Sci. 2005;46:
22. Nielsen PJ, Allerod CW. Evaluation of local anesthesia techniques for small incision cataract surgery. J Cataract Refract Surg. 1998;24(8):1136–1144. doi:10.1016/S0886-3350(98)80110-7
23. Rashmi S, Akshaya KM, Mahesha S. Comparison of topical versus sub-tenon’s anesthesia in phacoemulsification at a tertiary care eye hospital. J Ophthalmic Vis Res. 2014;9(3):329–333. doi:10.4103/2008-322X.143370
24. Rüschen H, Celaschi D, Bunce C, Carr C. Randomised controlled trial of sub-tenon’s block versus topical anesthesia for cataract surgery: a comparison of patient satisfaction. Br J Ophthalmol. 2005;89(3):291–293. doi:10.1136/bjo.2004.052167
25. Sekundo W, Dick HB, Schmidt JC. Lidocaine-assisted xylocaine jelly anesthesia versus one quadrant sub-tenon infiltration for self-sealing sclerocorneal incision routine phacoemulsification. Eur J Ophthalmol. 2004;14(2):111–116. doi:10.1177/112067210401400205
26. Srinivasan S, Fern AI, Selvaraj S, Hasan S. Randomized double-blind clinical trial comparing topical and sub-tenon’s anesthesia in routine cataract surgery. Br J Anaesth. 2004;93(5):683–686. doi:10.1093/bja/aeh254
27. Teh S, Abdul Ghani N, Subrayan V. The ideal surgical anesthesia: a comparison of pain experience in subjects undergoing cataract surgery under topical versus subtenon anesthesia. Ann Clin Lab Res. 2017;5(3):181.
28. Zafirakis P, Voudouri A, Rowe S, et al. Topical versus sub-tenon’s anesthesia without sedation in cataract surgery. J Cataract Refract Surg. 2001;27(6):873–879. doi:10.1016/S0886-3350(00)00703-3
29. Vielpeau I, Billotte C, Kreidie J, Lecoq P. Comparative study between topical anesthesia and subtenon anesthesia for cataract surgery. J Fr Ophtalmol. 1999;22(1):48–51.
30. Lansingh VC, Carter MJ, Martens M. Global cost-effectiveness of cataract surgery. Ophthalmology. 2007;114(9):1670–1678. doi:10.1016/j.ophtha.2006.12.013
31. Obuchowska I, Konopinska J. Fear and anxiety associated with cataract surgery under local anesthesia in adults: a systematic review. Psychol Res Behav Manag. 2021;14:781–793. doi:10.2147/PRBM.S314214
32. Socea SD, Abualhasan H, Magen O, et al. Preoperative anxiety levels and pain during cataract surgery. Curr Eye Res. 2020;45(4):471–476. doi:10.1080/02713683.2019.1666996
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.